1. Introduction
Statistics revealed that 2% of the world’s population lives with intellectual disabilities (ID) [
1]. Most individuals with ID demonstrate problems in learning and motor control [
2]. Consequently, they usually have difficulties in activities that require movement coordination, such as standing, walking, and stair climbing [
3,
4,
5,
6].
To monitor the physical performance of these children, regular gross motor evaluation is vital. Among the frequently used tests, tests of walking ability, especially straight-line level walking, are the most pivotal for measuring mobility [
3,
7,
8,
9,
10,
11,
12]. However, Iosa et al. (2014) [
7] showed that unless the adolescents have multiple disabilities, such as cognitive or physical problems, no significant differences can be found between adolescents with ID and typically developed (TD) adolescents in a straight-line level walking test. This is reasonable because, compared with other complicated tasks, such as obstacle crossing, straight-line level walking is less challenging and generally requires less lower extremity muscle control and strength [
13,
14]. The obstacle crossing test is a standardized criterion-based evaluation that is often used in numerous motor performance tests. However, this test is not adequate when used for participants with ID because it typically requires the subject’s attention and active participation, which most participants with ID lack. Moreover, if the motion being evaluated is not a familiar task, most of the participants with ID experience difficulty in following the testing instructions. Consequently, tracking the motor performance of these participants presents a great challenge.
Another mobility test, stair-walking, is also a crucial functional motor evaluation for children and adolescents with ID [
14,
15,
16,
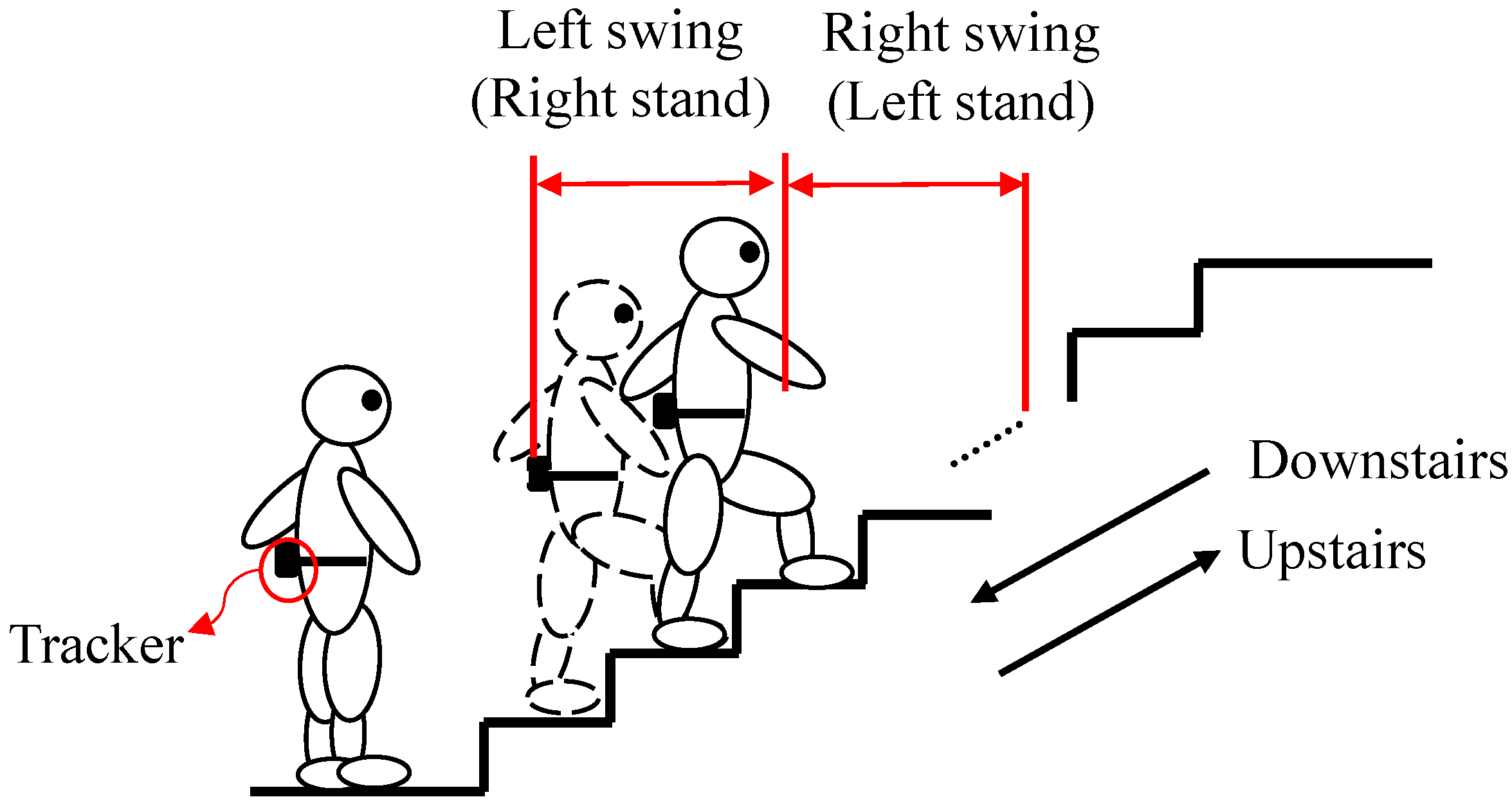
17]. Like normal gait walking, stair-walking comprises stance phases (weight acceptance, forward continuance, and controlled lowering) and swing phases (leg pull-through and preparation of foot placement) alternatively performed by the lower limbs [
15,
16], as shown in
Figure 1. To ascend or descend stairs safely, a person must resist the force of gravity by contracting the rectus femoris, vastus lateralis, soleus, and medial gastrocnemius during two phases [
16]. Stair-walking is an everyday skill for children and adolescents with ID and the objective is clearly understood [
17]. Such a test presents numerous challenges to participants with ID [
8,
14,
15] because stair-walking is associated with factors including lower extremity strength, cardiopulmonary endurance, vision, balance, and fear of falling. Limited ability in those factors is one of the most crucial markers for participants with ID [
15]. To prevent postural instability or falls during stair-walking, children with ID often develop unusual motion patterns, such as tap-stepping and forward leaning [
16].
Currently, studies on stair-walking tests for children and adolescents with ID are limited. Most studies can be partitioned into two approaches. The first approach is to evaluate stair ability through expert scoring, an example of which is the Dynamic Gait Index (DGI) [
18]. The final testing item of the DGI concerns stair-climbing performance, and the score is determined according to a therapist’s observation, ranging from 0–3 points. However, the score represents only an overall description of stair-climbing performance (e.g., walking with or without a rail). Pattern changes and movement details cannot be measured objectively through expert scoring. Therefore, numerous other studies have adopted the second approach, that is, using a motion capture system (i.e., based on optical cameras) and force plates to measure the gait; this has been considered the gold standard in the industry and at most hospitals [
3,
4,
5,
6,
7,
8,
9]. Such systems can detect comprehensive temporal and spatial gait features. However, this approach has time and space limitations in stair-walking testing. For most participants with ID, even though a motion capture system can measure gait completely, the less limiting approach is to develop an easy-to-use, wearable, and portable tool that can be applied in daily or unrestricted-distance measurement for eliciting awareness of gait abnormalities throughout childhood and adulthood [
10].
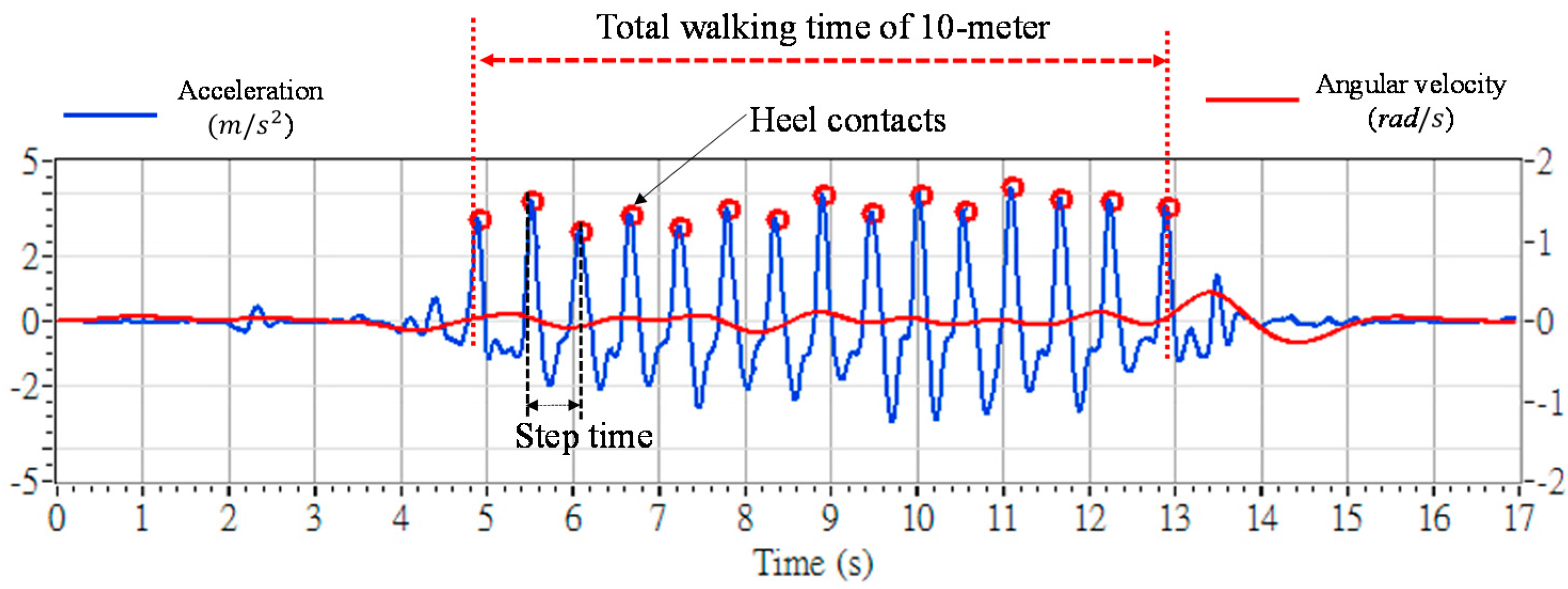
With the rapid development of the inertial sensor technology, numerous researchers have applied sensors based on microelectromechanical systems (MEMS) to measure gait motions [
11,
12,
15,
19,
20,
21,
22]. The most widely used inertial sensors are accelerometers and gyroscopes. Accelerometers can be used to measure the acceleration of an object along its movement trajectory [
11], and gyroscopes can be used to measure an object’s rotational angular velocity around three-dimensional axes (i.e., roll, pitch, and yaw) [
12]. Both of them can be mounted on the limbs or the trunk to measure motions without undue restrictions of space or time. However, inertial sensors encounter accumulated drift effects [
23,
24] and gravity interventions [
10]. These problems render the measurements inaccurate, which inherently limits the sensors’ applications. Therefore, most studies that use inertial sensors focus on measuring the temporal gait parameters, and use those parameters to explore various abnormalities prior to formal assessment, or investigate physical activity levels in children and youth with ID [
25].
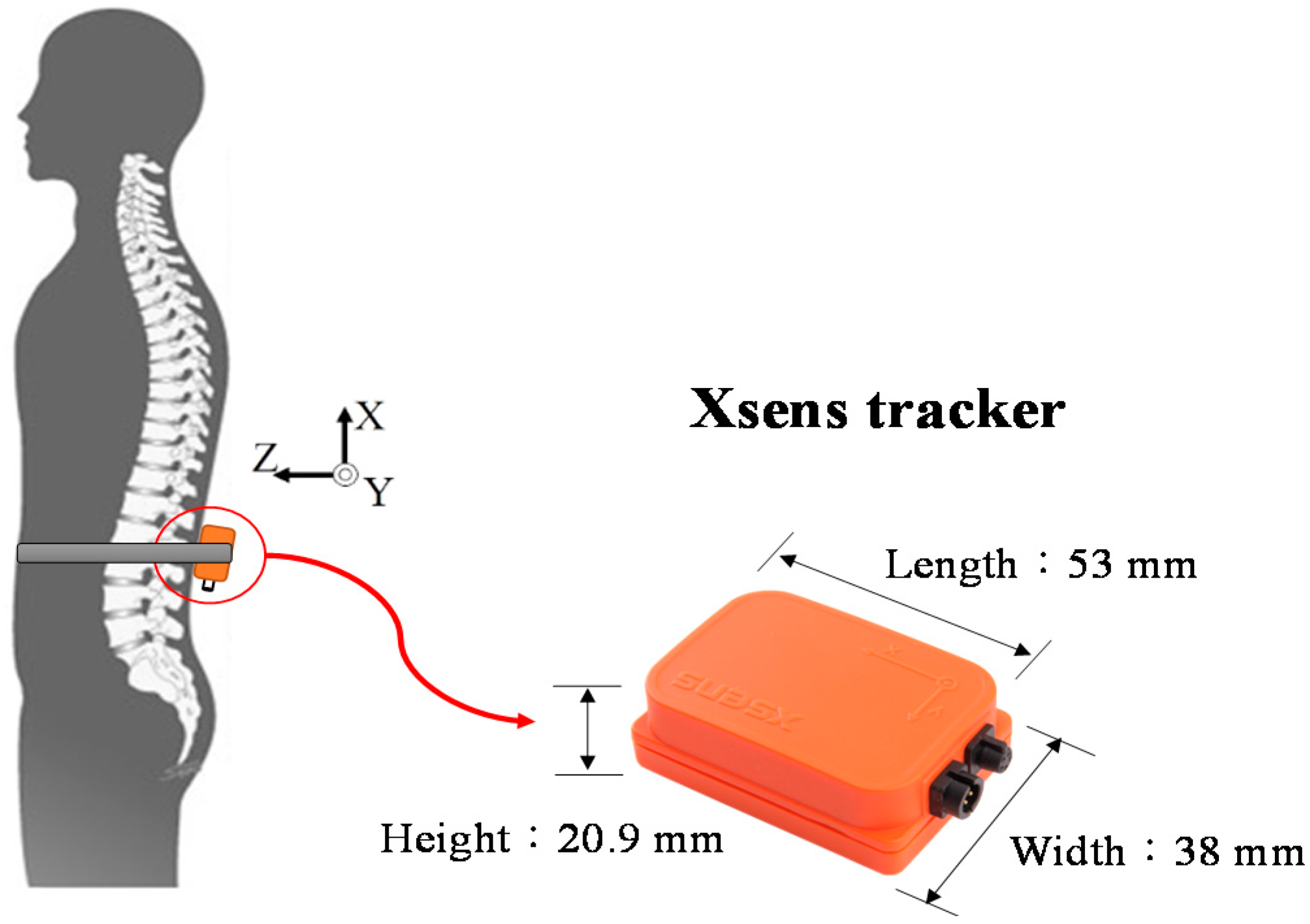
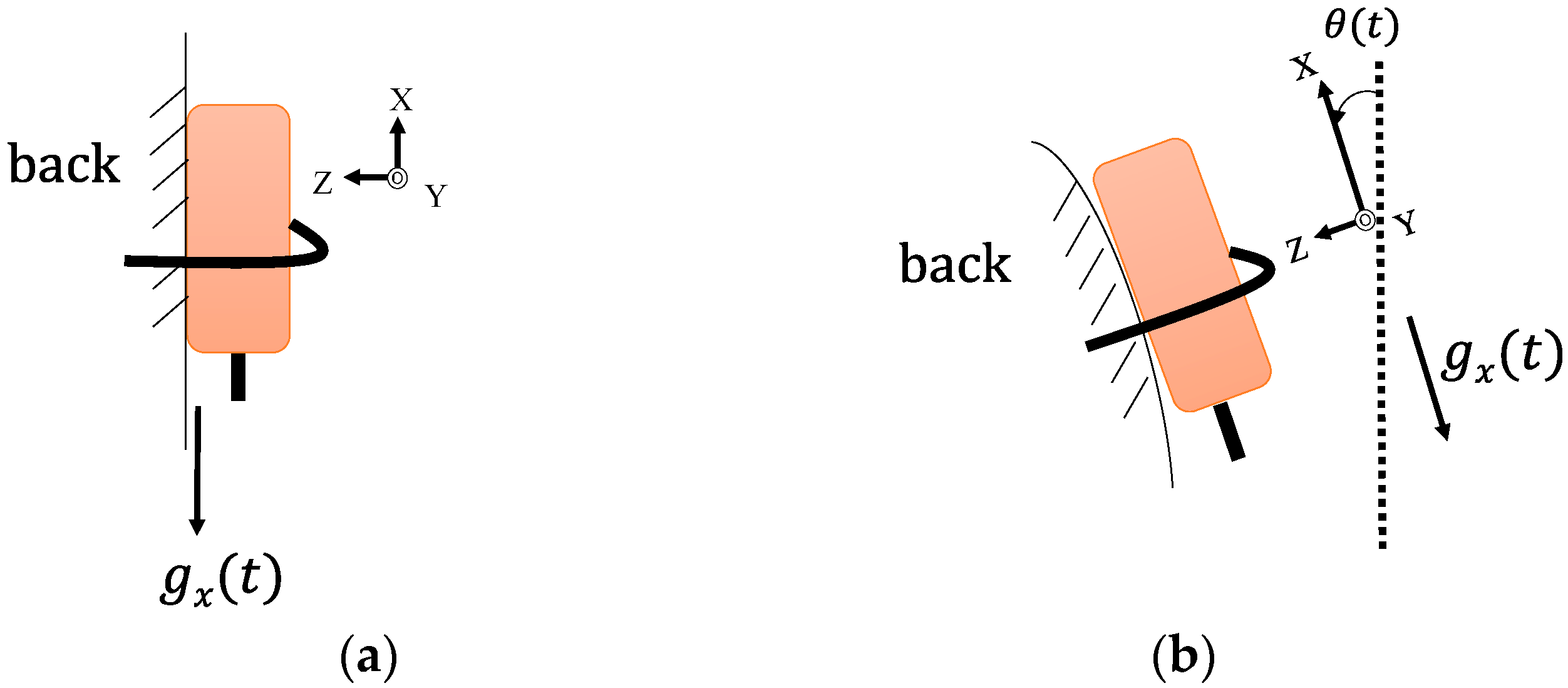
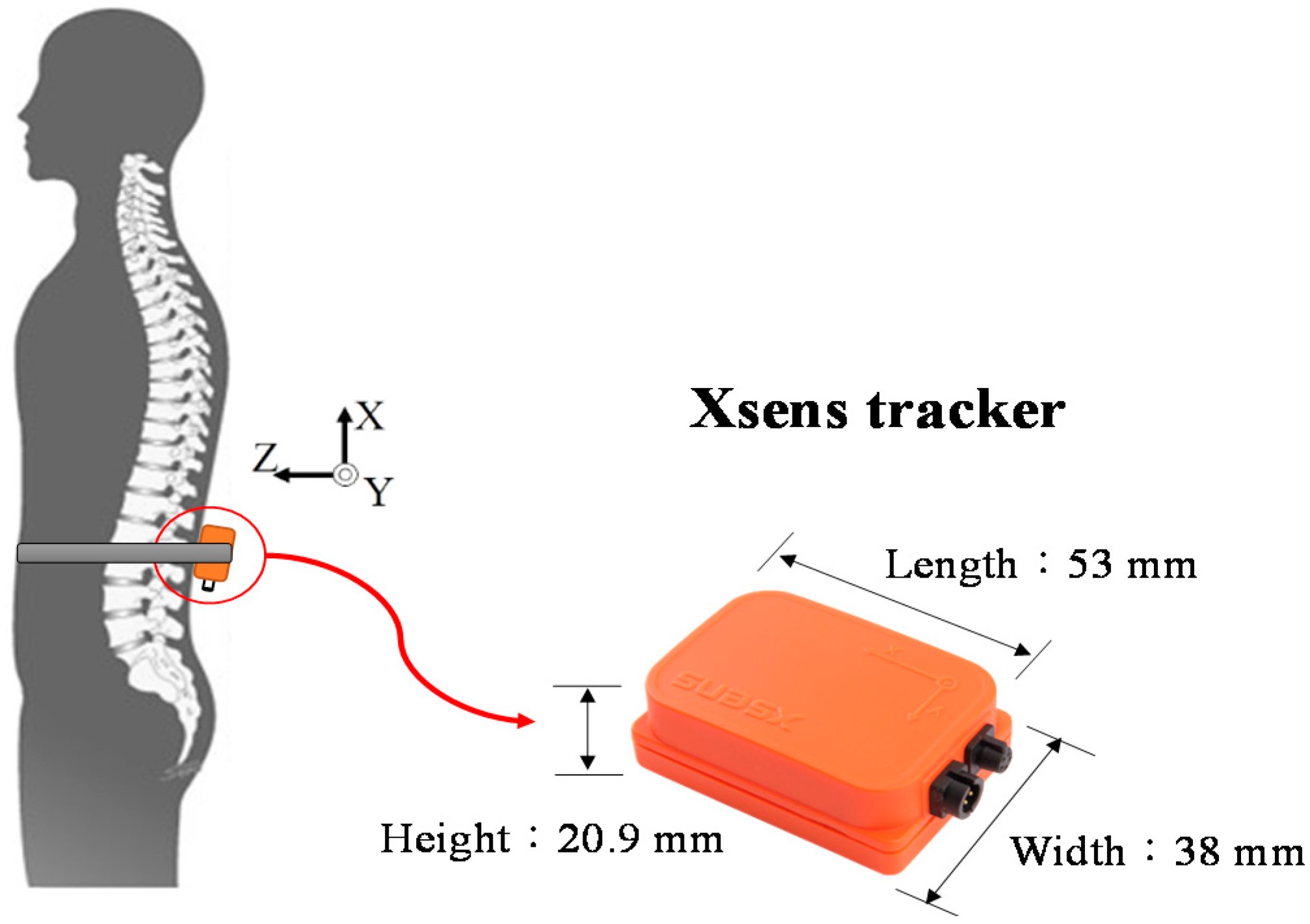
In this paper, we aim to propose an approach based on 3D accelerometers and gyroscopes for adolescents with ID to measure their stair-walking performance. In particular, we address the problem of sensor calibration to ensure accurate measurement. Rather than using only a straight-line level walking test, this study focused more on measuring the motor performance of children with ID through both upstairs and downstairs walking tests. We mounted an integrated sensor containing an accelerometer and a gyroscope on each participant’s lower back to measure their gait parameters. The testing protocol was approved by the Ethics Committee of Chang Gung Medical Foundation (Number: 103-7374B).
The remainder of this paper is organized as follows. In
Section 2, we explain the proposed method and the testing procedure. In
Section 3, we report and discuss the results. Finally, we present our conclusion in
Section 4.



 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}