
Free and Bioavailable Vitamin D Are Correlated with Disease Severity in Acute Pancreatitis: A Single-Center, Prospective Study
 , , , , ,
, , , , ,
Abstract

1. Introduction
2. Results
3. Discussion
Comparing Healthy Individuals
4. Materials and Methods
4.1. Patients
4.2. Blood Analyses
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hribar, M.; Hristov, H.; Gregorič, M.; Blaznik, U.; Zaletel, K.; Oblak, A.; Osredkar, J.; Kušar, A.; Žmitek, K.; Rogelj, I.; et al. Nutrihealth Study: Seasonal Variation in Vitamin D Status Among the Slovenian Adult and Elderly Population. Nutrients 2020, 12, 1838. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Naughton, D.P. Vitamin D in health and disease: Current perspectives. Nutr. J. 2010, 9, 65. [Google Scholar] [CrossRef] [PubMed]
- Delrue, C.; Speeckaert, M.M. Vitamin D and Vitamin D-Binding Protein in Health and Disease. Int. J. Mol. Sci. 2023, 24, 4642. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Holleczek, B.; Schöttker, B. Vitamin D Insufficiency and Deficiency and Mortality from Respiratory Diseases in a Cohort of Older Adults: Potential for Limiting the Death Toll during and beyond the COVID-19 Pandemic? Int. J. Environ. Res. Public. Health 2023, 20, 2488. [Google Scholar] [CrossRef]
- Bouillon, R.; Schuit, F.; Antonio, L.; Rastinejad, F. Vitamin D Binding Protein: A Historic Overview. Front. Endocrinol. 2020, 11, 317. [Google Scholar] [CrossRef]
- Bikle, D.D.; Schwartz, J. Vitamin D Binding Protein, Total and Free Vitamin D Levels in Different Physiological and Pathophysiological Conditions. Front. Endocrinol. 2019, 10, 317. [Google Scholar] [CrossRef]
- Zhu, A.; Kuznia, S.; Boakye, D.; Schöttker, B.; Brenner, H. Vitamin D-Binding Protein, Bioavailable, and Free 25(OH)D, and Mortality: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 3894. [Google Scholar] [CrossRef]
- Wöbke, T.K.; Sorg, B.L.; Steinhilber, D. Vitamin D in inflammatory diseases. Front. Physiol. 2014, 5, 244. [Google Scholar] [CrossRef]
- Martens, P.-J.; Gysemans, C.; Verstuyf, A.; Mathieu, C. Vitamin D’s Effect on Immune Function. Nutrients 2020, 12, 1248. [Google Scholar] [CrossRef]
- Garg, S.; Makhija, N. A Study on Effect of Vitamin D Supplementation in Vitamin D Deficient Females With Polycystic Ovarian Syndrome. Int. J. Reprod. Contracept. Obs. Gynecol. 2022, 11, 2398–2405. [Google Scholar] [CrossRef]
- Kolosovych, I.; Hanol, I.; Bystrytska, M.; Uzun, H. Changes in Vitamin D and Calcium-Phosphorus Metabolism in Patients with Severe Acute Pancreatitis. Turk. J. Surg. 2022, 38, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Ocal, S.; Cerci, K.; Buldukoglu, O.C.; Atar, G.E.; Harmandar, F.A.; Cekin, A.H. Effect of Serum Vitamin D Levels on the Severity of Acute Pancreatitis: A Prospective Study. Pancreatology 2024, 24, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Kim, J.W.; Lee, K.J. Vitamin D Deficiency Predicts Severe Acute Pancreatitis. United Eur. Gastroenterol. J. 2019, 7, 90–95. [Google Scholar] [CrossRef]
- Vieth, R.; Holick, M.F. The IOM—Endocrine Society Controversy on Recommended Vitamin D Targets in Support of the Endocrine Society Position. In Vitamin D, 4th ed.; Feldman, D., Ed.; Academic Press: Cambridge, MA, USA, 2018; Chapter 57B; pp. 1091–1107. [Google Scholar]
- Malheiro, A.P.G.; Gianfrancesco, L.; Nogueira, R.J.N.; Grotta, M.B.; Morcillo, A.M.; Ribeiro, J.D.; Toro, A.A.D.C. Association between serum Vitamin D levels and asthma severity and control in children and adolescents. Lung 2023, 201, 181–187. [Google Scholar] [CrossRef]
- Cai, F.; Hu, C.; Chen, C.J.; Han, Y.P.; Lin, Z.Q.; Deng, L.H.; Xia, Q. Vitamin D and Pancreatitis: A Narrative Review of Current Evidence. Nutrients 2022, 14, 2113. [Google Scholar] [CrossRef]
- Ghaseminejad-Raeini, A.; Ghaderi, A.; Sharafi, A.; Nematollahi-Sani, B.; Moossavi, M.; Derakhshani, A.; Sarab, G.A. Immunomodulatory Actions of Vitamin D in Various Immune-Related Disorders: A Comprehensive Review. Front. Immunol. 2023, 14, 950465. [Google Scholar] [CrossRef]
- Li, X.Y.; He, C.; Zhu, Y.; Lu, N.H. Role of Gut Microbiota on Intestinal Barrier Function in Acute Pancreatitis. World J. Gastroenterol. 2020, 26, 2187–2193. [Google Scholar] [CrossRef]
- Li, J.; Zhou, R.; Zhang, J.; Li, Z.F. Calcium Signaling of Pancreatic Acinar Cells in the Pathogenesis of Pancreatitis. World J. Gastroenterol. 2014, 20, 16146–16152. [Google Scholar] [CrossRef]
- Gerasimenko, J.V.; Gerasimenko, O.V.; Petersen, O.H. The Role of Ca2+ in the Pathophysiology of Pancreatitis. J. Physiol. 2014, 592, 269–280. [Google Scholar] [CrossRef]
- Gallerani, M.; Boari, B.; Salmi, R.; Manfredini, R. Seasonal variation in the onset of acute pancreatitis. World J. Gastroenterol. 2004, 10, 3328–3331. [Google Scholar] [CrossRef]
- Zerwekh, J.E. Blood biomarkers of vitamin D status. Am. J. Clin. Nutr. 2008, 87, 1087S–1091S. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, U.; Hirche, F.; Stangl, G.I.; Hinz, K.; Westphal, S.; Dierkes, J. Bioavailability of Vitamin D₂ and D₃ in healthy volunteers: A randomized placebo-controlled trial. J. Clin. Endocrinol. Metab. 2013, 98, 4339–4345. [Google Scholar] [CrossRef] [PubMed]
- Bertoldo, F.; Cianferotti, L.; Di Monaco, M.; Falchetti, A.; Fassio, A.; Gatti, D.; Gennari, L.; Giannini, S.; Girasole, G.; Gonnelli, S.; et al. Definition, Assessment, and Management of Vitamin D Inadequacy: Suggestions, Recommendations, and Warnings from the Italian Society for Osteoporosis, Mineral Metabolism and Bone Diseases (SIOMMMS). Nutrients 2022, 14, 4148. [Google Scholar] [CrossRef] [PubMed]
- Parrish, C.R.; DiBaise, J.K. Vitamin D deficiency in patients with pancreatitis: Is vitamin D replacement required? J. Nutr. Disord. Ther. 2015, 5, 3. [Google Scholar]
- Margulies, S.L.; Kurian, D.; Elliott, M.S.; Han, Z. Vitamin D deficiency in patients with intestinal malabsorption syndromes—Think in and outside the gut. J. Dig. Dis. 2015, 16, 617–633. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Suh, H.W.; Kim, J.K.; Kim, T.S.; Jo, E.K. New insights into vitamin D and autophagy in inflammatory bowel diseases. Curr. Med. Chem. 2017, 24, 898–910. [Google Scholar] [CrossRef]
- Bhutia, S.K. Vitamin D in autophagy signaling for health and diseases: Insights on potential mechanisms and future perspectives. J. Nutr. Biochem. 2022, 99, 108841. [Google Scholar] [CrossRef]
- Yin, K.; Agrawal, D.K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar]
- Del Pinto, R.; Pietropaoli, D.; Chandar, A.K.; Ferri, C.; Cominelli, F. Association between inflammatory bowel disease and vitamin D deficiency: A systematic review and meta-analysis. Inflamm. Bowel Dis. 2015, 21, 2708–2717. [Google Scholar] [CrossRef]
- Raman, M.; Milestone, A.N.; Walters, J.R.; Hart, A.L.; Ghosh, S. Vitamin D and gastrointestinal diseases: Inflammatory bowel disease and colorectal cancer. Ther. Adv. Gastroenterol. 2011, 4, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.; Cooper, S.C.; Ghosh, S.; Hewison, M. The role of vitamin D in inflammatory bowel disease: Mechanism to management. Nutrients 2019, 11, 1019. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Sanguankeo, A.; Permpalung, N. Significant association between vitamin D deficiency and sepsis: A systematic review and meta-analysis. BMC Anesth. 2015, 15, 84. [Google Scholar] [CrossRef] [PubMed]
- Kempker, J.A.; Han, J.E.; Tangpricha, V.; Ziegler, T.R.; Martin, G.S. Vitamin D and sepsis: An emerging relationship. Dermato-endocrinology 2012, 4, 101–108. [Google Scholar] [CrossRef]
- Vičič, V.; Kukec, A.; Kugler, S.; Geršak, K.; Osredkar, J.; Pandel Mikuš, R. Correction: Vičič et al. Assessment of Vitamin D Status in Slovenian Premenopausal and Postmenopausal Women, Using Total, Free, and Bioavailable 25-Hydroxyvitamin D (25(OH)D). Nutrients 2022, 14, 5349. Nutrients 2023, 15, 2103. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| All Patients (N = 80) | |
|---|---|
| Age [years] | 58.8 ± 16.1 |
| Gender | |
| Male/female | 45/35 |
| BMI | 28.3 ± 5.4 |
| VDBP [mg/mL] | 146.5 ± 82.6 |
| 25(OH)D3 [nmol/L] | 45.7 ± 25.3 |
| Vit D deficiency | |
| Severe deficient < 30 nmol/L | 22 (27.5%) |
| Deficient 30–50 nmol/L | 25 (31.3%) |
| Insufficient 50–75 nmol/L | 26 (32.5%) |
| Optimal > 75 nmol/L | 7 (8.8%) |
| Free 25(OH)D3 | 28.5 ± 22.8 |
| Bioavailable 25(OH)D3 | 9.3 ± 7.8 |
| Supplementation of vitamin D | 28 (35.0%) |
| Etiology | |
| Biliar | 38 (47.5%) |
| Alcoholic | 19 (23.8%) |
| Hyperlipemic | 4 (5.0%) |
| Other | 15 (18.8%) |
| Missing data | 4 (5.0%) |
| Smoking | 30 (37.5%) |
| Number of packs/year | 11.7 ± 16.2 |
| Alcohol consumption | |
| No | 29 (36.3%) |
| 1 to 7×/week (low) | 22 (27.5%) |
| 8–14×/week (moderate) | 7 (8.6%) |
| 14–20/week (high) | 9 (11.3%) |
| >20×/week (severe) | 4 (5.0%) |
| Missing data | 9 (11.3%) |
| Vit D Deficiency | |||||
|---|---|---|---|---|---|
| Severely Deficient (n = 22) | Deficient (n = 25) | Insufficient (n = 26) | Optimal (n = 7) | p-Value | |
| Age | 53.8 ± 14.0 | 55.6 ± 15.0 | 62.9 ± 17.1 | 71.2 ± 15.2 | 0.028 |
| Gender | |||||
| Male/female | 12/10 | 16/9 | 13/13 | 4/3 | 0.789 |
| 25(OH)D3 [nmol/L] | 19.0 ± 5.1 | 38.0 ± 6.4 | 61.3 ± 6.3 | 99.3 ± 26.9 | <0.001 |
| Free 25(OH)D3 [pmol/L] | 9.9 ± 4.4 | 24.5 ± 16.3 | 36.9 ± 17.3 | 69.7 ± 28.9 | <0.001 |
| Bioavailable 25(OH)D3 [nmol/L] | 3.1 ± 1.5 | 7.9 ± 5.1 | 11.8 ± 5.6 | 25.0 ± 9.8 | <0.001 |
| Pts with Ranson after 48 h ≥3 | 0 | 1 (4.0%) | 0 | 0 | 0.509 |
| CRP [mg/L] | 80.7 ± 123.4 | 50.6 ± 62.5 | 54.5 ± 70.3 | 28.0 ± 49.0 | 0.493 |
| Admission to ICU | 6 (27.3%) | 1 (4.0%) | 0 | 0 | 0.007 |
| Hospitalization duration [days] | 14.6 ± 15.2 | 9.7 ± 9.3 | 6.9 ± 3.8 | 8.0 ± 5.5 | 0.018 |
| Type of AP | |||||
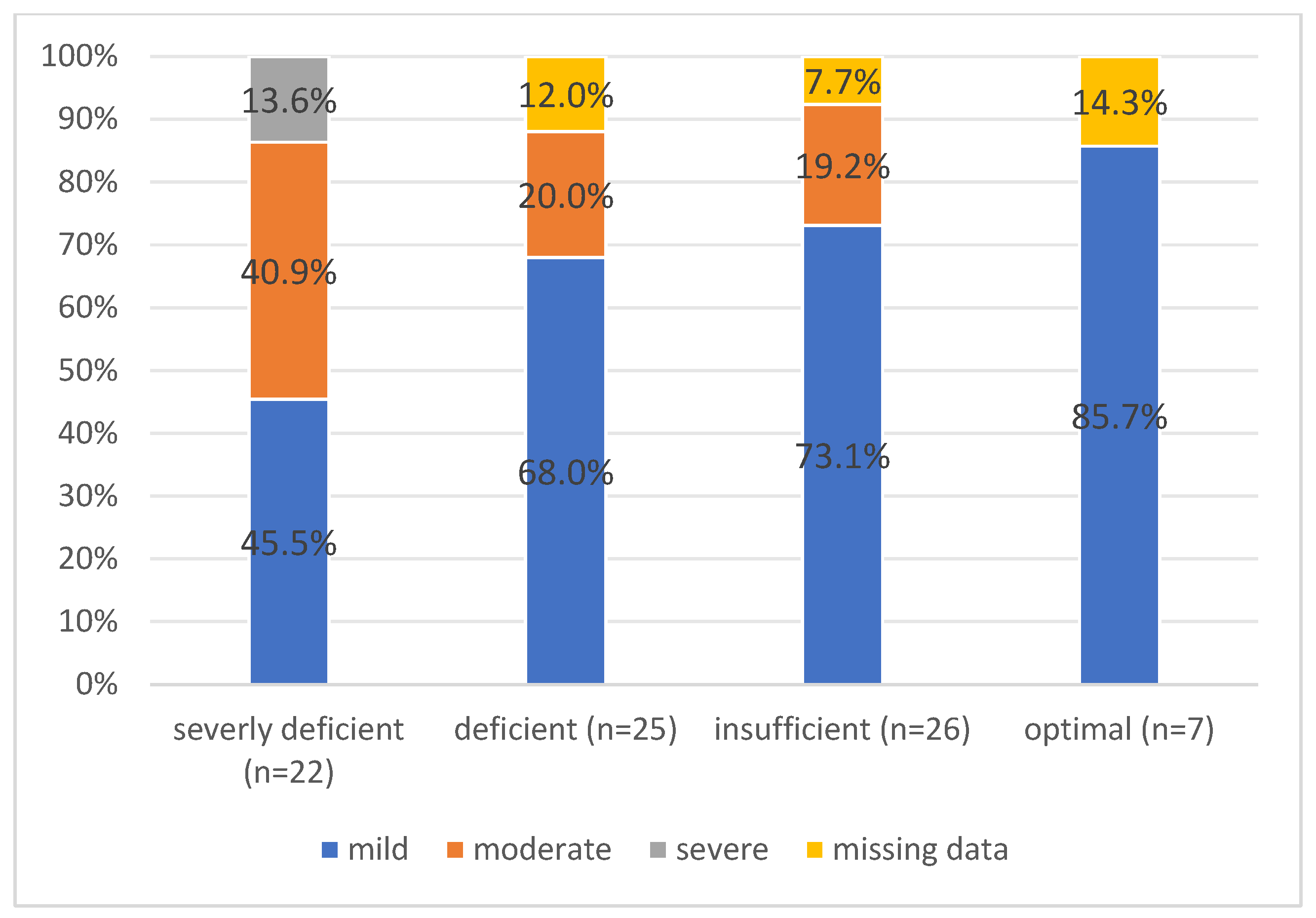
| Class of AP (Atlanta) | 0.029 | ||||
| Mild | 10 (45.5%) | 17 (68.0%) | 19 (73.1%) | 6 (85.7%) | |
| Moderate | 9 (40.9%) | 5 (20.0%) | 5 (19.2%) | 0 | |
| Severe | 3 (13.6%) | 0 | 0 | 0 | |
| Missing data | 0 | 3 (12.0%) | 2 (7.7%) | 1 (14.3%) | |
| CT finding of AP | 0.013 | ||||
| Interstitial | 10 (45.5%) | 18 (72.0%) | 19 (73.1%) | 6 (85.7%) | |
| Necrotizing | 12 (54.5%) | 5 (20.0%) | 5 (19.2%) | 0 | |
| Missing data | 0 | 2 (8.0%) | 2 (7.7%) | 1 (14.3%) | |
| CT score; CTSI | 2.7 ± 3.2 | 1.8 ± 3.2 | 1.5 ± 3.2 | 0 | 0.191 |
| CTSI > 3 | 10 (45.5%) | 6 (24.0%) | 4 (15.4%) | 0 | 0.087 |
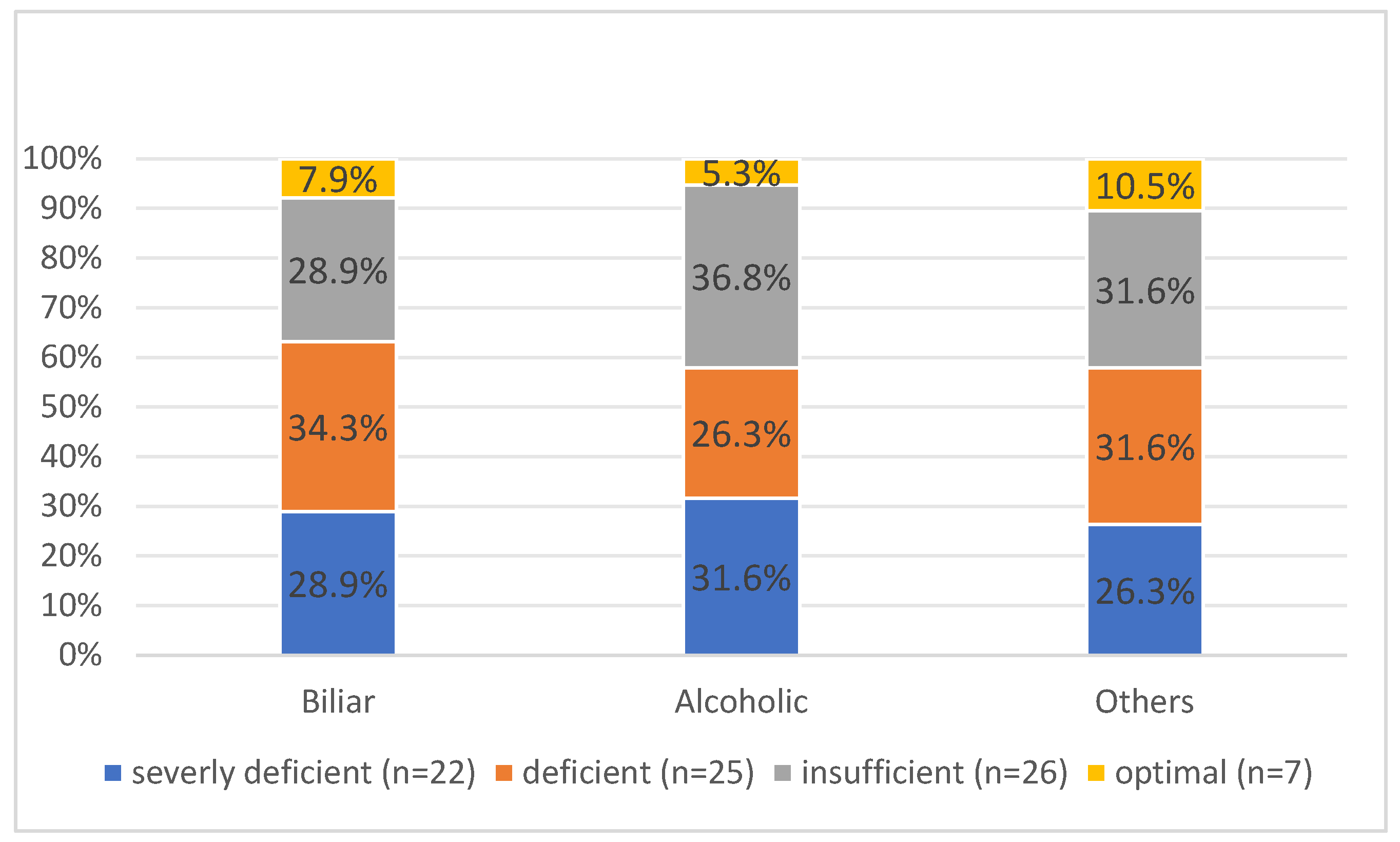
| Etiology of AP | 0.988 | ||||
| Biliar | 11 (50.0%) | 13 (52.0%) | 11 (42.3%) | 3 (42.9%) | |
| Alcoholic | 6 (27.3%) | 5 (20.0%) | 7 (26.9%) | 1 (14.3%) | |
| Other | 5 (22.7%) | 6 (24.0%) | 6 (23.1%) | 2 (28.6%) | |
| B | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| Gender male | 0.370 | 1.448 | 0.521–4.030 | 0.478 |
| Age [years] | −0.02 | 0.98 | 0.95–1.01 | 0.266 |
| BMI | −0.07 | 0.93 | 0.84–1.03 | 0.167 |
| 25(OH)D3 [nmol/L] | −0.04 | 0.96 | 0.93–0.99 | 0.006 |
| Free 25(OH)D3 [pmol/L] | −0.07 | 0.93 | 0.89–0.98 | 0.003 |
| Bioavailable 25(OH)D3 [nmol/L] | −0.24 | 0.79 | 0.67–0.92 | 0.002 |
| Albumin | −0.106 | 0.899 | 0.807–1.002 | 0.055 |
| Etiology—alcoholic | 1.405 | 4.074 | 1.351–12.286 | 0.013 |
| CT—Necrotizing | 6.996 | 1092 | 65.236–18,279.158 | <0.001 |
| CTSI score | 0.791 | 2.206 | 1.581–3.077 | <0.001 |
| B | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| Gender male | 0.680 | 1.974 | 0.358–10.893 | 0.435 |
| Age [years] | −0.02 | 0.98 | 0.94–1.03 | 0.468 |
| BMI | 0.03 | 1.03 | 0.89–1.19 | 0.712 |
| 25(OH)D3 [nmol/L] | −0.14 | 0.87 | 0.78–0.97 | 0.014 |
| Free 25(OH)D3 [pmol/L] | −0.39 | 0.68 | 0.47–0.97 | 0.036 |
| Bioavailable 25(OH)D3 [nmol/L] | −1.04 | 0.35 | 0.13–0.98 | 0.046 |
| Albumin | −0.061 | 0.941 | 0.801–1.104 | 0.456 |
| Etiology—alcoholic | 0.891 | 2.437 | 0.493–12.053 | 0.275 |
| CT—Necrotizing | 20.441 | 753,888 | 0.000 | 0.997 |
| CTSI score | 0.541 | 1.718 | 1.224–2.411 | 0.002 |
| Unstandardized B | Standardized Beta Correlation | t | 95% CI for B | p-Value | |
|---|---|---|---|---|---|
| Gender, male | −0.257 | −0.132 | −1.169 | −0.695–0.181 | 0.246 |
| Age | 0.033 | 0.551 | 5.792 | 0.022–0.045 | <0.001 |
| BMI | −0.019 | −0.108 | −0.921 | −0.061–0.022 | 0.360 |
| 25(OH)D3 [nmol/L] | 0.01 | 0.08 | 0.70 | 0.01–0.01 | 0.485 |
| Free 25(OH)D3 [pmol/L] | 0.01 | 0.07 | 0.62 | −0.01–0.01 | 0.540 |
| Bioavailable 25(OH)D3 [nmol/L] | 0.01 | 0.03 | 0.24 | 0.03–0.03 | 0.808 |
| Albumin | −0.051 | −0.265 | −2.414 | −0.092–(−0.009) | 0.018 |
| Etiology—alcoholic | −0.193 | −0.084 | −0.724 | −0.724–0.338 | 0.471 |
| CT—Necrotizing | 0.215 | 0.103 | 0.875 | −0.275–0.705 | 0.384 |
| CTSI score | 0.016 | 0.052 | 0.433 | −0.058–0.091 | 0.666 |
| Unstandardized B | Standardized Beta Correlation | t | 95% CI for B | p-Value | |
|---|---|---|---|---|---|
| Gender, male | 1.639 | 0.079 | 0.675 | −3.202–6.479 | 0.502 |
| Age | 0.038 | 0.059 | 0.506 | −0.111–0.187 | 0.614 |
| BMI | −0.401 | −0.201 | −1.733 | −0.862–0.060 | 0.087 |
| 25(OH)D3 [nmol/L] | −0.11 | −0.27 | −2.42 | 0.20–(−0.02) | 0.018 |
| Free 25(OH)D3 [pmol/L] | −0.11 | −0.24 | −2.08 | −0.22–(−0.01) | 0.041 |
| Bioavailable 25(OH)D3 [nmol/L] | −0.35 | −0.25 | −2.19 | −0.66–(−0.03) | 0.032 |
| Albumin | −0.498 | −0.244 | −2.154 | −0.959–(−0.037) | 0.035 |
| Etiology—alcoholic | 4.249 | −0.176 | 0.524 | −1.308–9.805 | 0.132 |
| CT—Necrotizing | 11.599 | 0.503 | 4.941 | 6.920–16.279 | <0.001 |
| CTSI score | 1.569 | 0.459 | 4.324 | 0.845–2.293 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siuka, D.; Rakuša, M.; Vodenik, A.; Vodnik, L.; Štabuc, B.; Štubljar, D.; Drobne, D.; Jerin, A.; Matelič, H.; Osredkar, J. Free and Bioavailable Vitamin D Are Correlated with Disease Severity in Acute Pancreatitis: A Single-Center, Prospective Study. Int. J. Mol. Sci. 2025, 26, 5695. https://doi.org/10.3390/ijms26125695
Siuka D, Rakuša M, Vodenik A, Vodnik L, Štabuc B, Štubljar D, Drobne D, Jerin A, Matelič H, Osredkar J. Free and Bioavailable Vitamin D Are Correlated with Disease Severity in Acute Pancreatitis: A Single-Center, Prospective Study. International Journal of Molecular Sciences. 2025; 26(12):5695. https://doi.org/10.3390/ijms26125695
Chicago/Turabian StyleSiuka, Darko, Matej Rakuša, Aleš Vodenik, Lana Vodnik, Borut Štabuc, David Štubljar, David Drobne, Aleš Jerin, Helena Matelič, and Joško Osredkar. 2025. "Free and Bioavailable Vitamin D Are Correlated with Disease Severity in Acute Pancreatitis: A Single-Center, Prospective Study" International Journal of Molecular Sciences 26, no. 12: 5695. https://doi.org/10.3390/ijms26125695
APA StyleSiuka, D., Rakuša, M., Vodenik, A., Vodnik, L., Štabuc, B., Štubljar, D., Drobne, D., Jerin, A., Matelič, H., & Osredkar, J. (2025). Free and Bioavailable Vitamin D Are Correlated with Disease Severity in Acute Pancreatitis: A Single-Center, Prospective Study. International Journal of Molecular Sciences, 26(12), 5695. https://doi.org/10.3390/ijms26125695