
The Effects of Endoplasmic Reticulum Stress via Intratracheal Instillation of Water-Soluble Acrylic Acid Polymer on the Lungs of Rats

 , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Results
2.1. Characterization of PAA
2.2. Relative Lung Weights
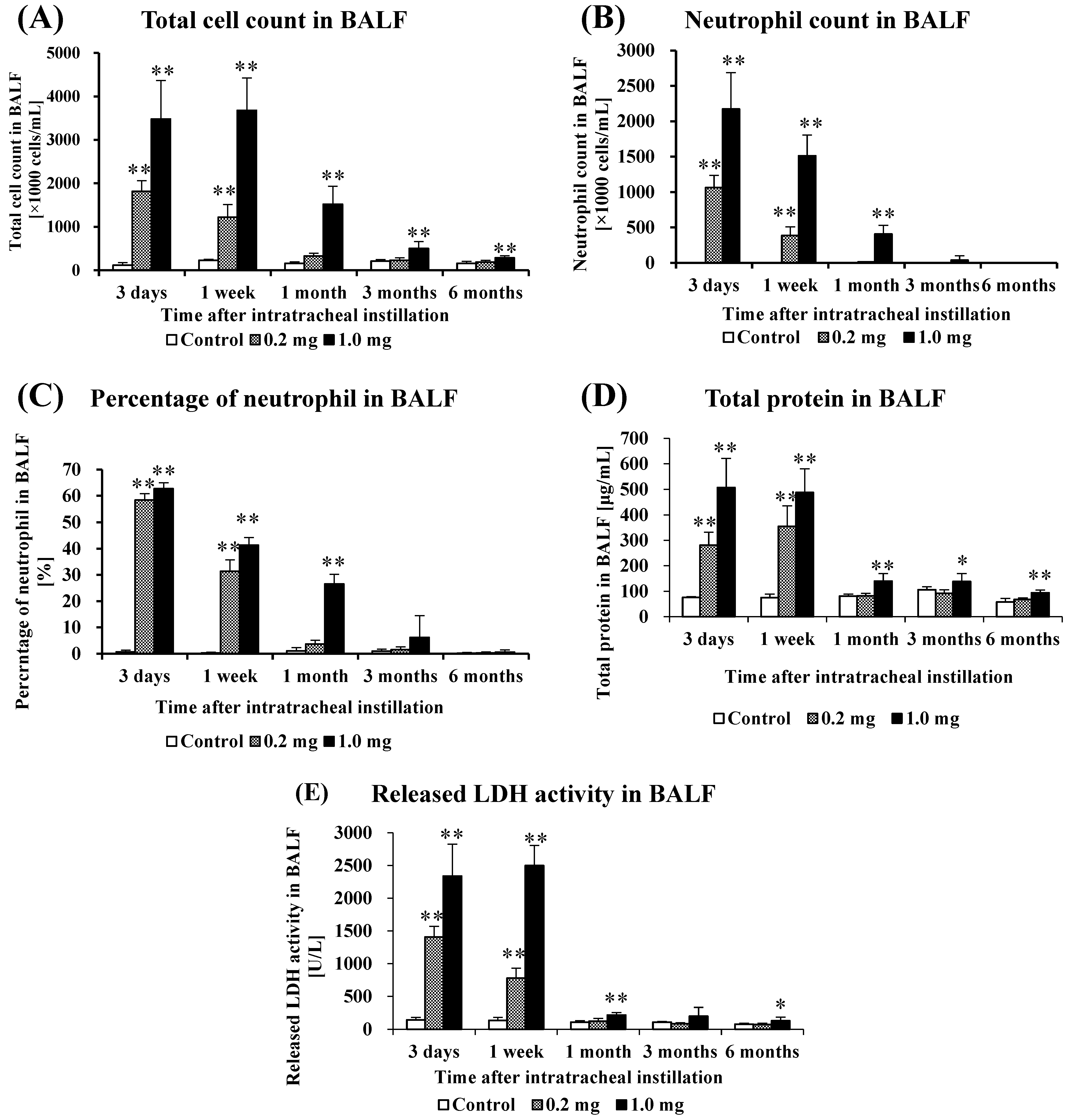
2.3. Cell Analysis and Lactate Dehydrogenase (LDH) Activity in Bronchoalveolar Lavage Fluid (BALF)
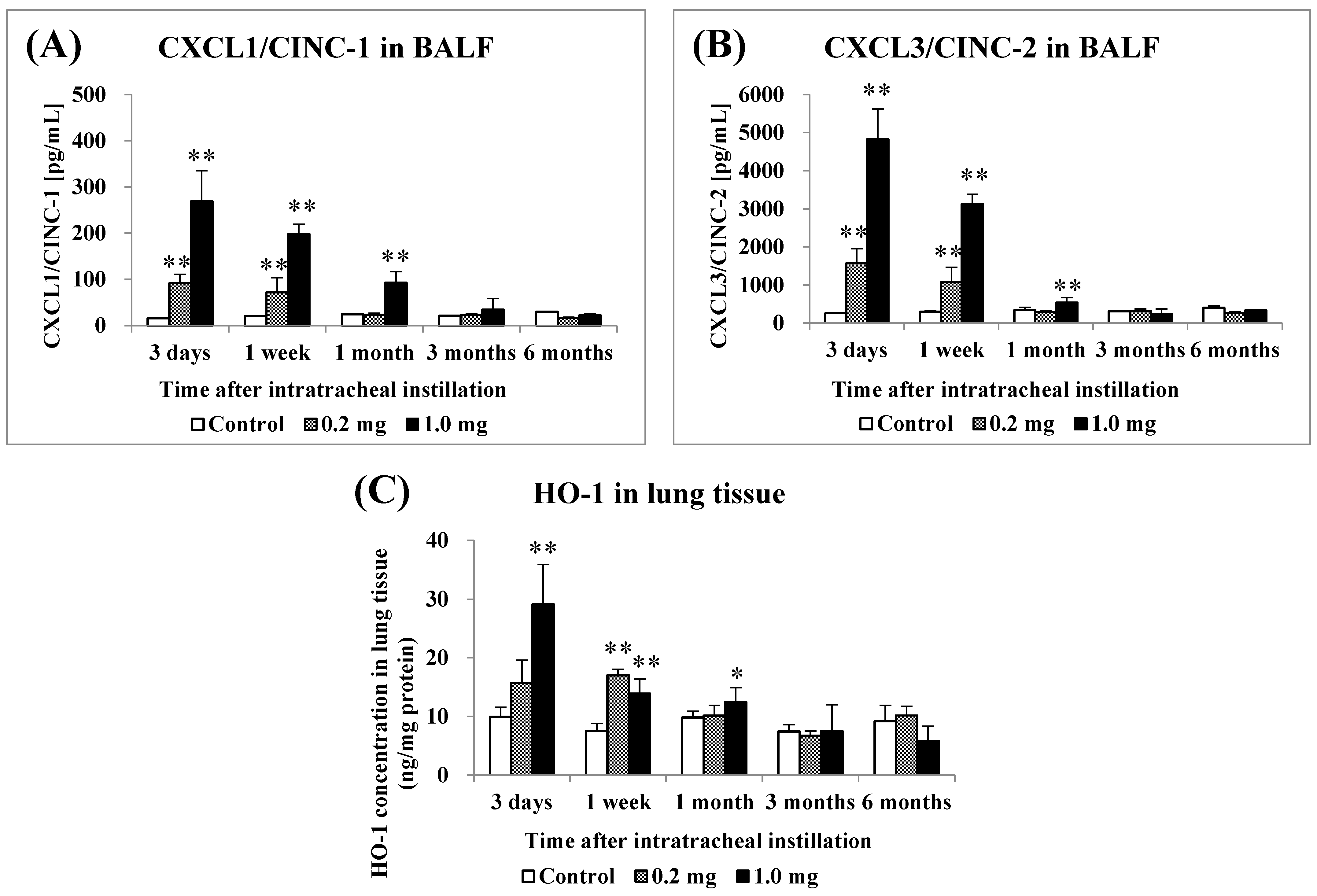
2.4. Concentration of CINC in BALF and Concentration of HO-1 in Lung Tissue
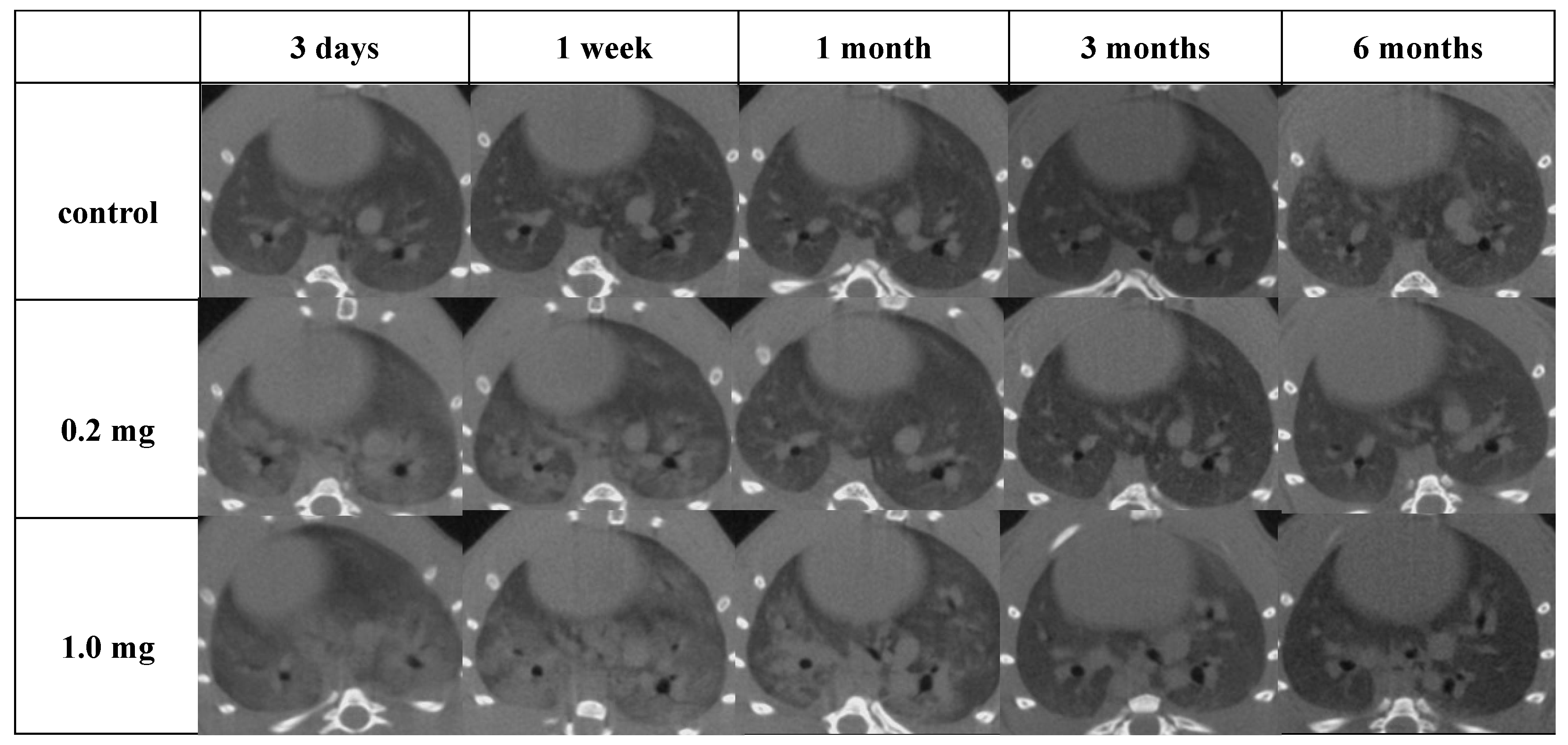
2.5. Micro-CT Imaging
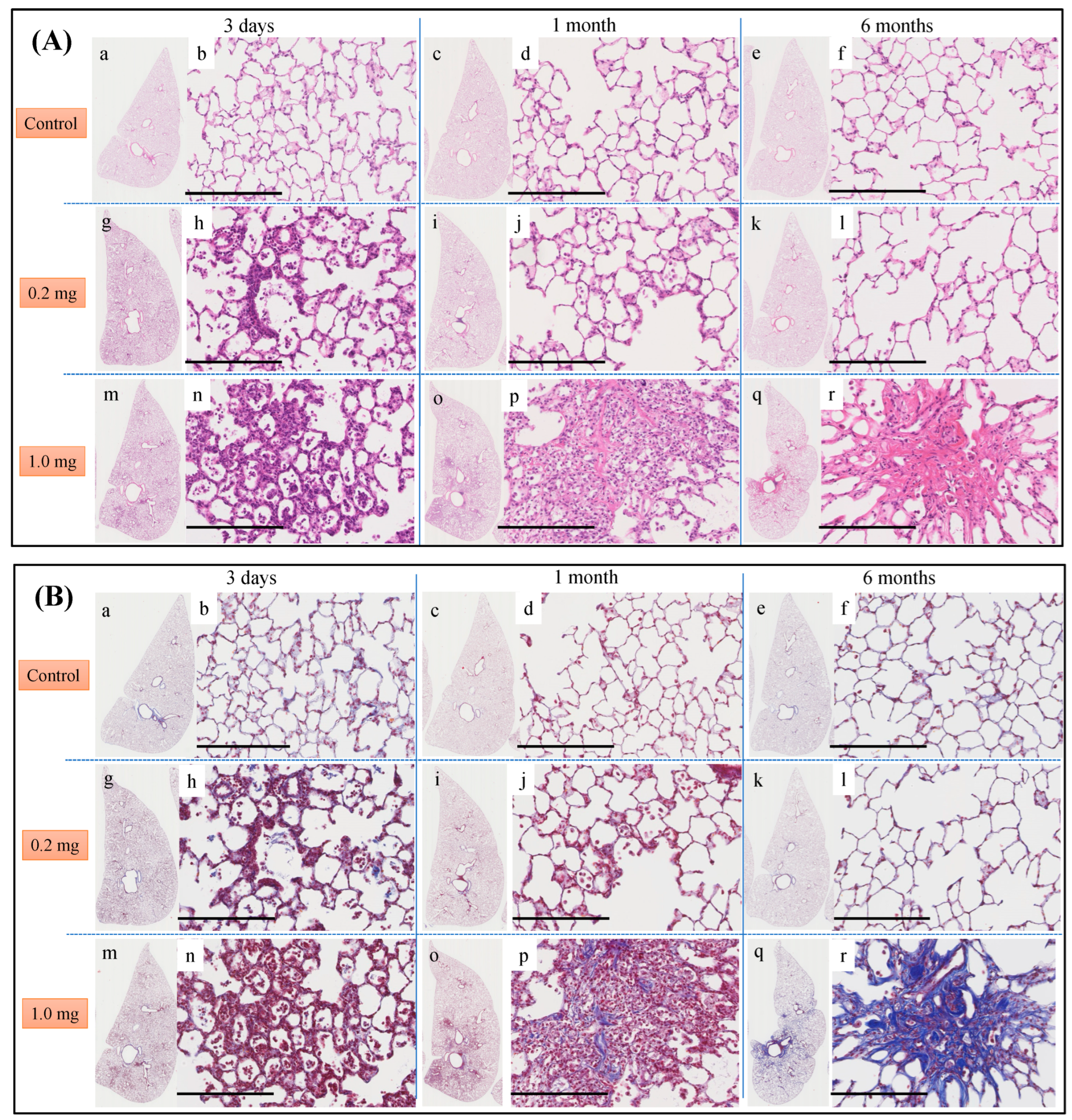
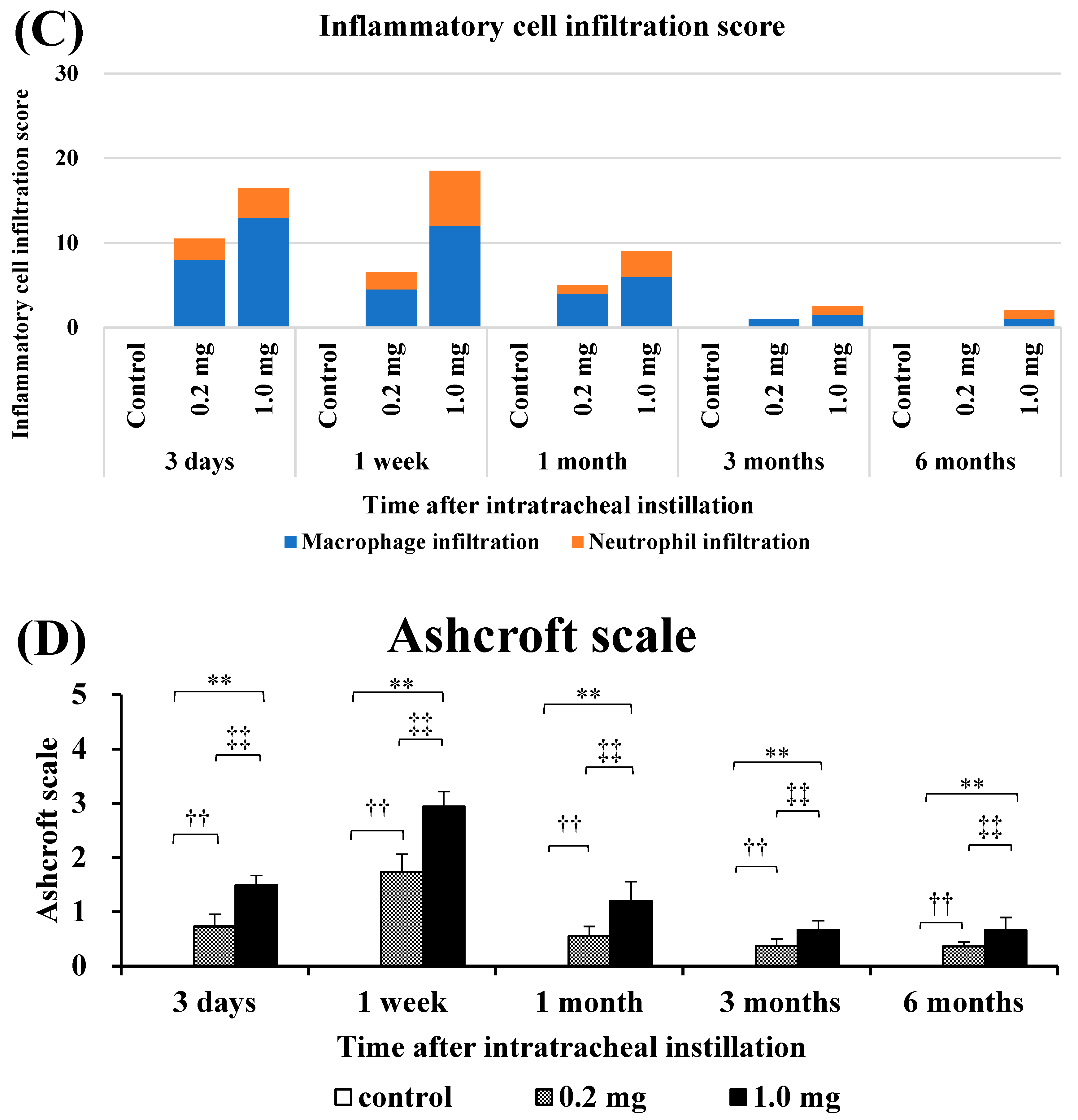
2.6. Histopathological Features in the Lung
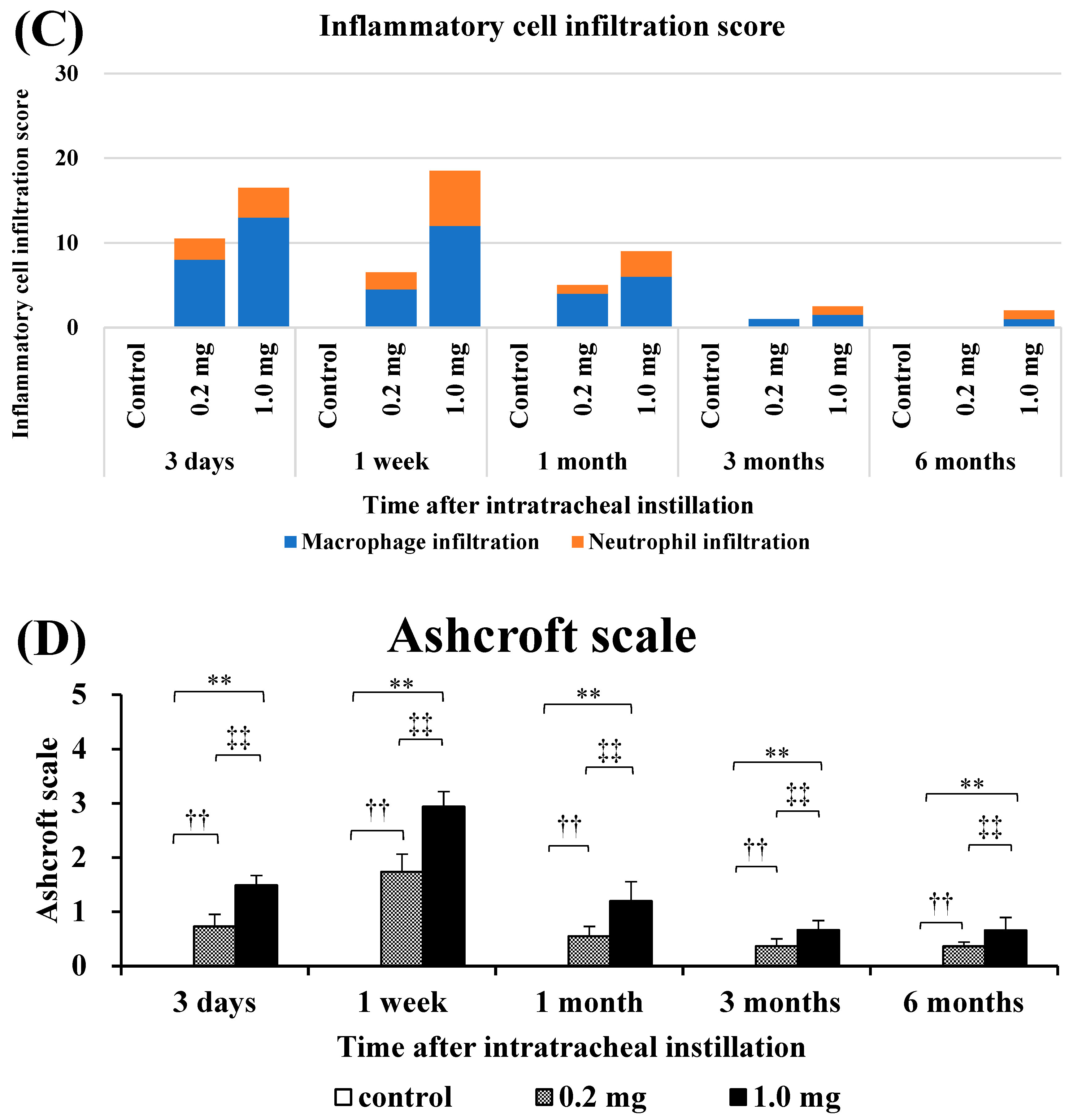
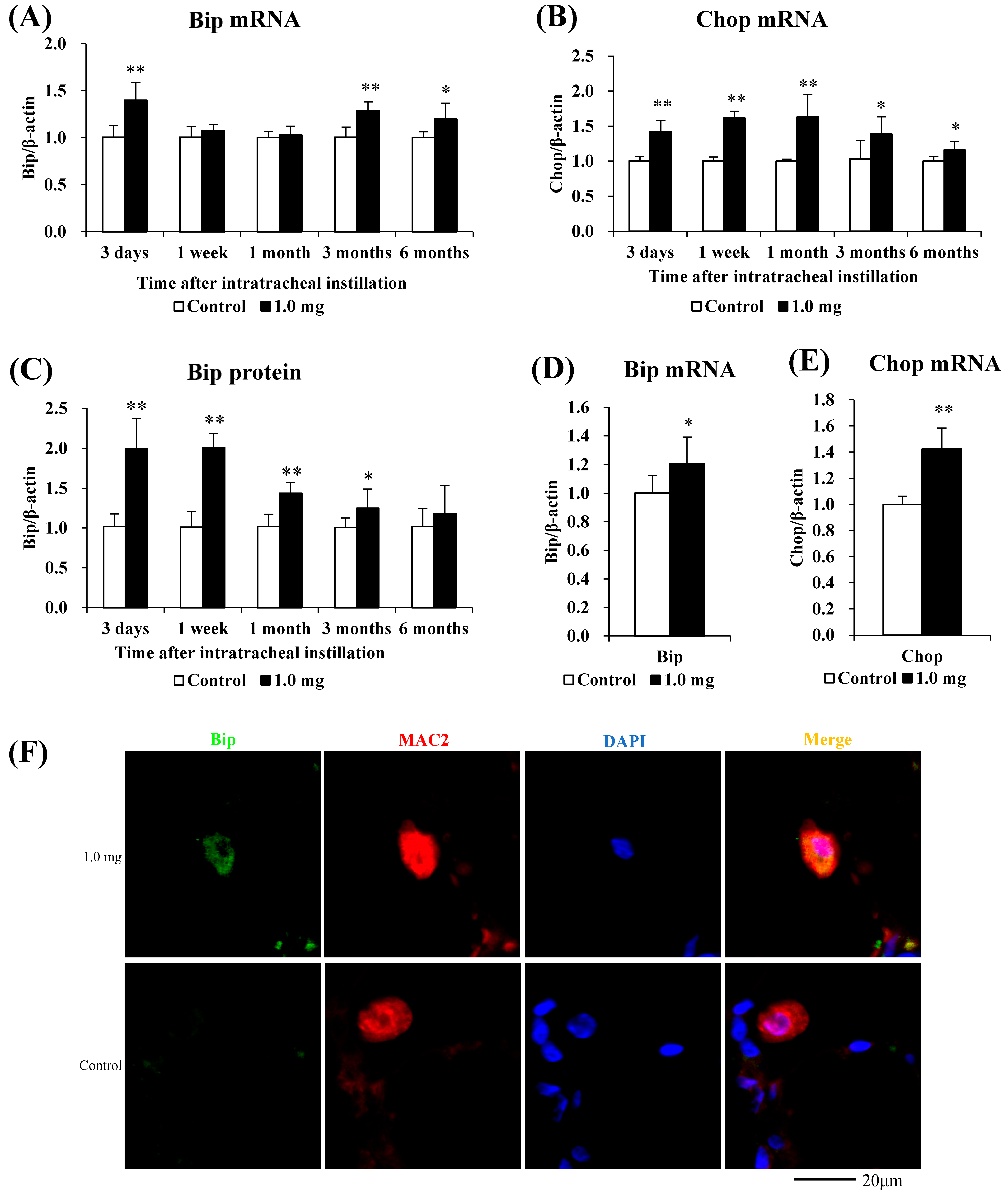
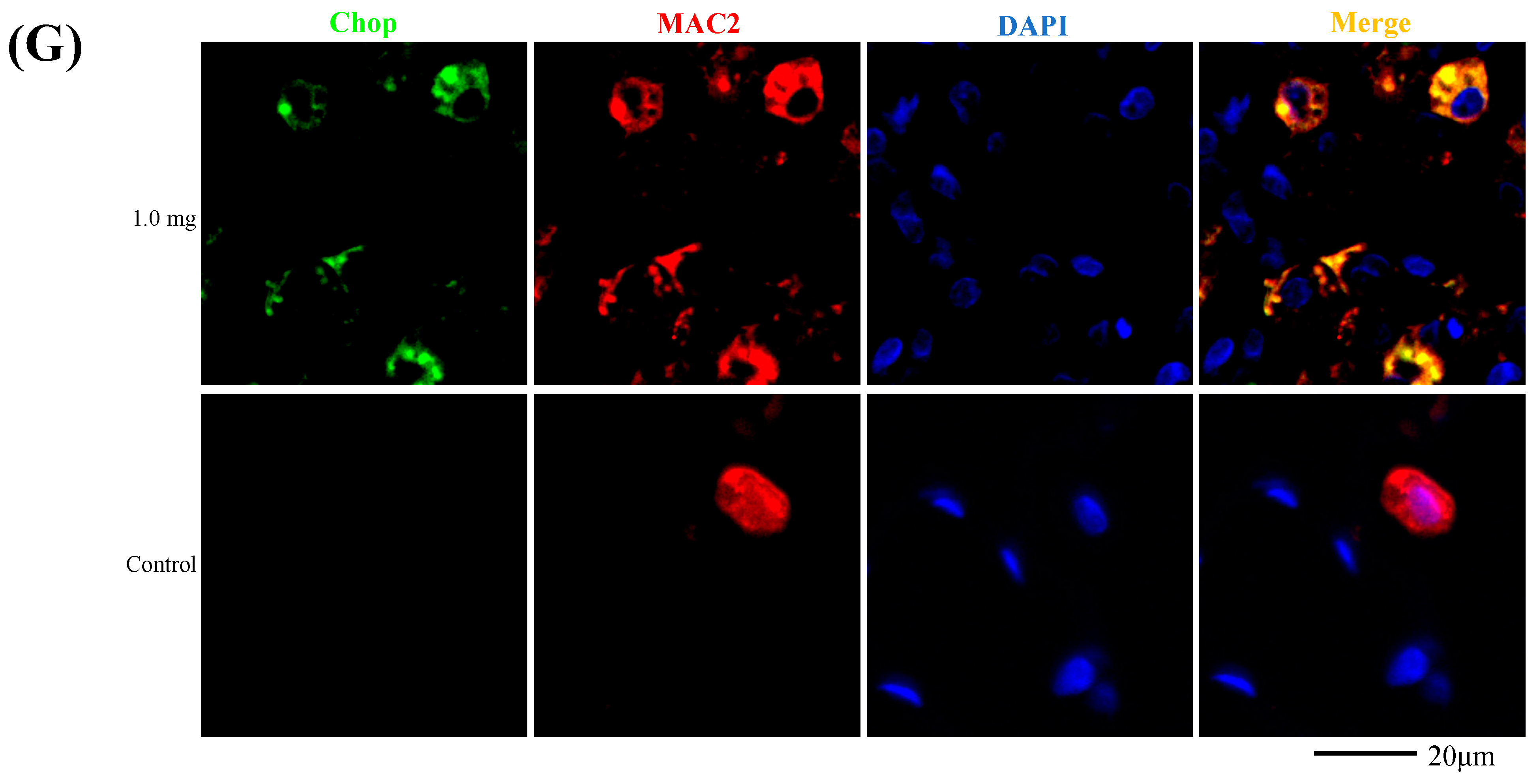
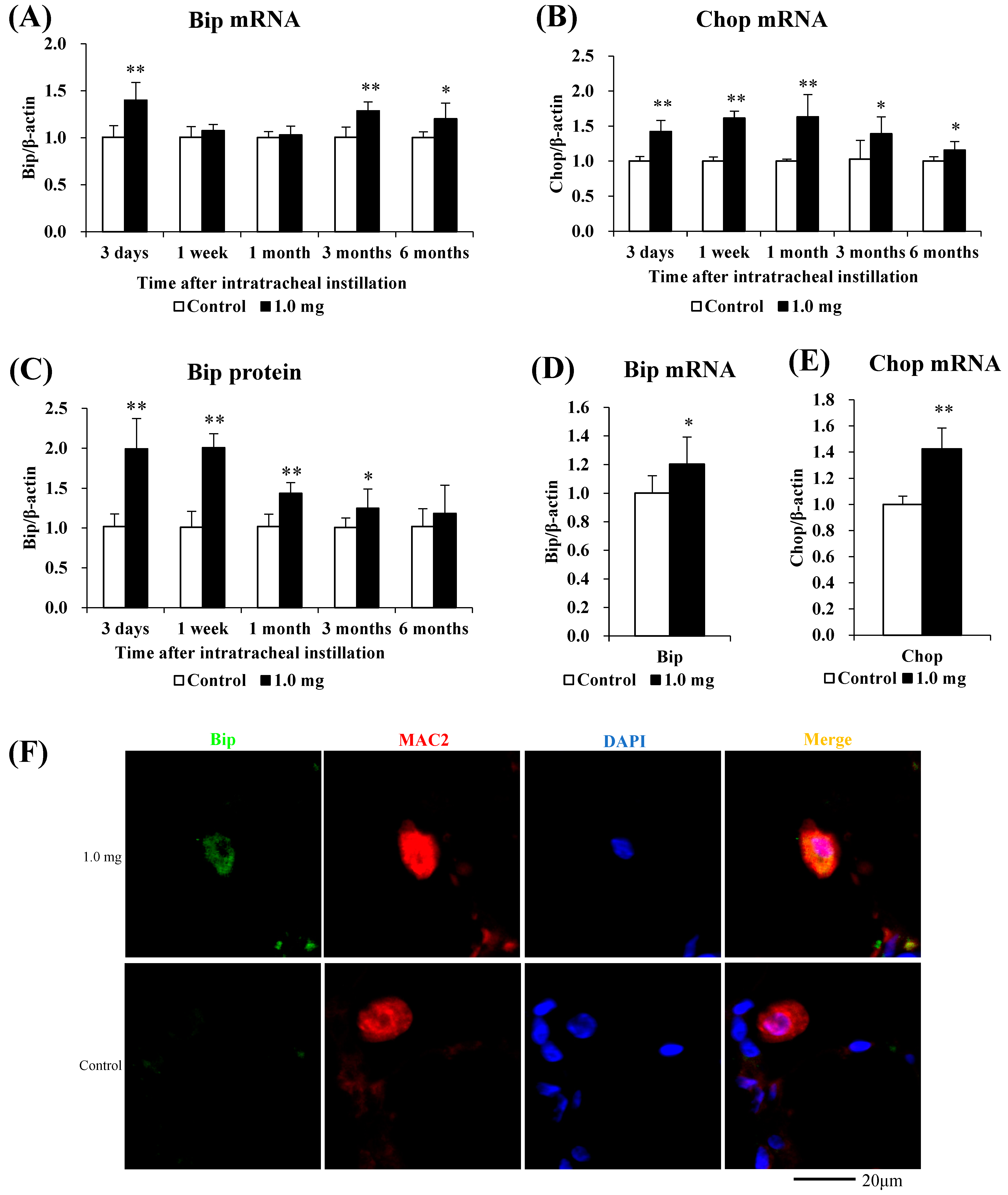
2.7. The Relationship between PAA and Endoplasmic Reticulum Stress
3. Discussion
4. Materials and Methods
4.1. Sample Polymer
4.2. Animals
4.3. Intratracheal Instillation
4.4. Animals Following Intratracheal Instillation
4.5. Preparation of Alveolar Macrophages from BALF
4.6. Cytospin Analysis of Inflammatory Cells and Measurement of LDH in BALF
4.7. Measurement of Chemokines in BALF and Heme Oxygenase (HO)-1 in Lung Tissue
4.8. SDS-PAGE and Western Blotting
4.9. Three-Dimensional Micro-CT Imaging
4.10. Quantitative Real-Time Polymerase Chain Reaction
4.11. Histopathology
4.12. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Observation Point | Group | vs. Control |
|---|---|---|
| Relative Lung Weight | ||
| 3 days | 0.2 mg | p < 0.01 |
| 1.0 mg | p < 0.01 | |
| 1 week | 0.2 mg | p < 0.01 |
| 1.0 mg | p < 0.01 | |
| 1 month | 0.2 mg | p = 0.034 |
| 1.0 mg | p < 0.01 | |
| 3 months | 0.2 mg | p = 0.084 |
| 1.0 mg | p < 0.01 | |
| 6 months | 0.2 mg | p = 0.667 |
| 1.0 mg | p = 0.021 |
| Observation Point | Group | vs. Control | ||||
|---|---|---|---|---|---|---|
| Total Cell Count | Neutrophil Count | Percentage of Neutrophil | Total Protein | Released LDH Activity | ||
| 3 days | 0.2 mg | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 |
| 1.0 mg | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | |
| 1 week | 0.2 mg | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 |
| 1.0 mg | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | |
| 1 month | 0.2 mg | p = 0.240 | p = 0.571 | p = 0.099 | p = 0.658 | p = 0.362 |
| 1.0 mg | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | |
| 3 months | 0.2 mg | p = 0.526 | p = 0.649 | p = 0.601 | p = 0.939 | p = 0.821 |
| 1.0 mg | p < 0.01 | p = 0.113 | p = 0.100 | p = 0.027 | p = 0.076 | |
| 6 months | 0.2 mg | p = 0.268 | p = 0.617 | p = 0.558 | p = 0.157 | p = 0.721 |
| 1.0 mg | p < 0.01 | p = 0.149 | p = 0.249 | p < 0.01 | p = 0.032 | |
| Observation Point | Group | vs. Control | ||
|---|---|---|---|---|
| CXCL1/CINC-1 in BALF | CXCL3/CINC-2 in BALF | HO-1 in Lung Tissue | ||
| 3 days | 0.2 mg | p < 0.01 | p < 0.01 | p = 0.062 |
| 1.0 mg | p < 0.01 | p < 0.01 | p < 0.01 | |
| 1 week | 0.2 mg | p < 0.01 | p < 0.01 | p < 0.01 |
| 1.0 mg | p < 0.01 | p < 0.01 | p < 0.01 | |
| 1 month | 0.2 mg | p = 0.711 | p = 0.933 | p = 0.564 |
| 1.0 mg | p < 0.01 | p < 0.01 | p = 0.043 | |
| 3 months | 0.2 mg | p = 0.595 | p = 0.618 | p = 0.808 |
| 1.0 mg | p = 0.134 | p = 0.951 | p = 0.640 | |
| 6 months | 0.2 mg | p = 1.000 | p = 1.000 | p = 0.388 |
| 1.0 mg | p = 0.996 | p = 0.998 | p = 0.995 | |
| Observation Point | Group | vs. the Same Point | ||
|---|---|---|---|---|
| Control | 0.2 mg | 1.0 mg | ||
| 3 days | Control | - | p < 0.01 | p < 0.01 |
| 0.2 mg | p < 0.01 | - | p < 0.01 | |
| 1.0 mg | p < 0.01 | p < 0.01 | - | |
| 1 week | Control | - | p < 0.01 | p < 0.01 |
| 0.2 mg | p < 0.01 | - | p < 0.01 | |
| 1.0 mg | p < 0.01 | p < 0.01 | - | |
| 1 month | Control | - | p < 0.01 | p < 0.01 |
| 0.2 mg | p < 0.01 | - | p < 0.01 | |
| 1.0 mg | p < 0.01 | p < 0.01 | - | |
| 3 months | Control | - | p < 0.01 | p < 0.01 |
| 0.2 mg | p < 0.01 | - | p < 0.01 | |
| 1.0 mg | p < 0.01 | p < 0.01 | - | |
| 6 months | Control | - | p < 0.01 | p < 0.01 |
| 0.2 mg | p < 0.01 | - | p < 0.01 | |
| 1.0 mg | p < 0.01 | p < 0.01 | - | |
| Observation Point | Group | vs. Control (Lung Tissue) | vs. Control (BALF) | |||
|---|---|---|---|---|---|---|
| Bip mRNA | Chop mRNA | Bip protein | Bip mRNA | Chop mRNA | ||
| 3 days | 1.0 mg | p < 0.01 | p < 0.01 | p < 0.01 | p = 0.043 | p < 0.01 |
| 1 week | 1.0 mg | p = 0.138 | p < 0.01 | p < 0.01 | - | - |
| 1 month | 1.0 mg | p = 0.299 | p < 0.01 | p < 0.01 | - | - |
| 3 months | 1.0 mg | p < 0.01 | p = 0.28 | p = 0.042 | - | - |
| 6 months | 1.0 mg | p = 0.19 | p = 0.18 | p = 0.203 | - | - |
References
- Park, D.U.; Ryu, S.H.; Lim, H.K.; Kim, S.K.; Choi, Y.Y.; Ahn, J.J.; Lee, E.; Hong, S.B.; Do, K.H.; Cho, J.L.; et al. Types of Household Humidifier Disinfectant and Associated Risk of Lung Injury (HDLI) in South Korea. Sci. Total Environ. 2017, 596–597, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.H.; Park, D.U.; Lee, E.; Park, S.; Lee, S.Y.; Jung, S.; Hong, S.B.; Park, J.; Hong, S.J. Humidifier Disinfectant and Use Characteristics Associated with Lung Injury in Korea. Indoor Air 2019, 29, 735–747. [Google Scholar] [CrossRef] [PubMed]
- McCauley, L.; Markin, C.; Hosmer, D. An Unexpected Consequence of Electronic Cigarette Use. Chest 2012, 141, 1110–1113. [Google Scholar] [CrossRef] [PubMed]
- Thota, D.; Latham, E. Case Report of Electronic Cigarettes Possibly Associated with Eosinophilic Pneumonitis in a Previously Healthy Active-Duty Sailor. J. Emerg. Med. 2014, 47, 15–17. [Google Scholar] [CrossRef]
- Kishimoto, T.; Okamoto, K.; Koda, S.; Ono, M.; Umeda, Y.; Yamano, S.; Takeda, T.; Rai, K.; Kato, K.; Nishimura, Y.; et al. Respiratory Disease in Workers Handling Cross-Linked Water-Soluble Acrylic Acid Polymer. PLoS ONE 2023, 18, e0284837. [Google Scholar] [CrossRef] [PubMed]
- Nishida, C.; Tomonaga, T.; Izumi, H.; Wang, K.Y.; Higashi, H.; Ishidao, T.; Takeshita, J.-i.; Ono, R.; Sumiya, K.; Fujii, S.; et al. Inflammogenic Effect of Polyacrylic Acid in Rat Lung Following Intratracheal Instillation. Part. Fibre Toxicol. 2022, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Yamano, S.; Goto, Y.; Hirai, S.; Furukawa, Y.; Kikuchi, Y.; Misumi, K.; Suzuki, M.; Takanobu, K.; Senoh, H.; et al. Dose–Response Relationship of Pulmonary Disorders by Inhalation Exposure to Cross-Linked Water-Soluble Acrylic Acid Polymers in F344 Rats. Part. Fibre Toxicol. 2022, 19, 27. [Google Scholar] [CrossRef]
- Mun, E.A.; Hannell, C.; Rogers, S.E.; Hole, P.; Williams, A.C.; Khutoryanskiy, V.V. On the Role of Specific Interactions in the Diffusion of Nanoparticles in Aqueous Polymer Solutions. Langmuir 2014, 30, 308–317. [Google Scholar] [CrossRef]
- Borm, P.J.A.; Driscoll, K. Particles, Inflammation and Respiratory Tract Carcinogenesis. Toxicol. Lett. 1996, 88, 109–113. [Google Scholar] [CrossRef]
- Shacter, E.; Weitzman, S.A. Chronic Inflammation and Cancer. Oncology 2002, 16, 217–226. [Google Scholar] [PubMed]
- Bellmann, B.; Muhle, H.; Creutzenberg, O.; Ernst, H.; Müller, M.; Bernstein, D.M.; Sintes, J.M.R. Calibration Study on Subchronic Inhalation Toxicity of Man-Made Vitreous Fibers in Rats. Inhal. Toxicol. 2003, 15, 1147–1177. [Google Scholar] [CrossRef] [PubMed]
- Kamstrup, O.; Ellehauge, A.; Chevalier, J.; Davis, J.M.G.; McConnell, E.E.; Thévenaz, P. Chronic Inhalation Studies of Two Types of Stone Wool Fibers in Rats. Inhal. Toxicol. 2001, 13, 603–621. [Google Scholar] [CrossRef] [PubMed]
- Pott, F.; Ziem, U.; Reiffer, F.J.; Huth, F.; Ernst, H.; Mohr, U. Carcinogenicity Studies on Fibres, Metal Compounds, and Some Other Dusts in Rats. Exp. Pathol. 1987, 32, 129–152. [Google Scholar] [CrossRef] [PubMed]
- MUHLE, H. Pulmonary Response to Toner upon Chronic Inhalation Exposure in Rats. Fundam. Appl. Toxicol. 1991, 17, 280–299. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.G.; Cowie, H.A. The Relationship between Fibrosis and Cancer in Experimental Animals Exposed to Asbestos and Other Fibers. Environ. Health Perspect. 1990, 88, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Oakes, S.A.; Papa, F.R. The Role of Endoplasmic Reticulum Stress in Human Pathology. Annu. Rev. Pathol. Mech. Dis. 2015, 10, 173–194. [Google Scholar] [CrossRef]
- Groenendyk, J.; Agellon, L.B.; Michalak, M. Calcium Signaling and Endoplasmic Reticulum Stress. Int. Rev. Cell Mol. Biol. 2021, 363, 1–20. [Google Scholar] [CrossRef]
- Spencer, B.G.; Finnie, J.W. The Role of Endoplasmic Reticulum Stress in Cell Survival and Death. J. Comp. Pathol. 2020, 181, 86–91. [Google Scholar] [CrossRef]
- Jiang, M.; Li, Z.; Zhu, G. The Role of Endoplasmic Reticulum Stress in the Pathophysiology of Periodontal Disease. J. Periodontal Res. 2022, 57, 915–932. [Google Scholar] [CrossRef]
- Cybulsky, A.V. Endoplasmic Reticulum Stress, the Unfolded Protein Response and Autophagy in Kidney Diseases. Nat. Rev. Nephrol. 2017, 13, 681–696. [Google Scholar] [CrossRef]
- Ajoolabady, A.; Kaplowitz, N.; Lebeaupin, C.; Kroemer, G.; Kaufman, R.J.; Malhi, H.; Ren, J. Endoplasmic Reticulum Stress in Liver Diseases. Hepatology 2023, 77, 619–639. [Google Scholar] [CrossRef] [PubMed]
- Burman, A.; Tanjore, H.; Blackwell, T.S. Endoplasmic Reticulum Stress in Pulmonary Fibrosis. Matrix Biol. 2018, 68–69, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.C.H.; Burr, L.; McGuckin, M.A. Oxidative and Endoplasmic Reticulum Stress in Respiratory Disease. Clin. Transl. Immunol. 2018, 7, e1019. [Google Scholar] [CrossRef] [PubMed]
- Samarelli, A.V.; Masciale, V.; Aramini, B.; Coló, G.P.; Tonelli, R.; Marchioni, A.; Bruzzi, G.; Gozzi, F.; Andrisani, D.; Castaniere, I.; et al. Molecular Mechanisms and Cellular Contribution from Lung Fibrosis to Lung Cancer Development. Int. J. Mol. Sci. 2021, 22, 12179. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, S.J. Endoplasmic Reticulum Stress in Lung Disease. Eur. Respir. Rev. 2017, 26, 170018. [Google Scholar] [CrossRef] [PubMed]
- Baek, H.A.; Kim, D.S.; Park, H.S.; Jang, K.Y.; Kang, M.J.; Lee, D.G.; Moon, W.S.; Chae, H.J.; Chung, M.J. Involvement of Endoplasmic Reticulum Stress in Myofibroblastic Differentiation of Lung Fibroblasts. Am. J. Respir. Cell Mol. Biol. 2012, 46, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.S.; Liu, C.C.; Lin, J.H.; Hsu, T.W.; Hsu, J.W.; Su, K.; Hung, S.C. Involvement of ER Stress, PI3K/AKT Activation, and Lung Fibroblast Proliferation in Bleomycin-Induced Pulmonary Fibrosis. Sci. Rep. 2017, 7, 14272. [Google Scholar] [CrossRef]
- Morimoto, Y.; Izumi, H.; Yoshiura, Y.; Tomonaga, T.; Lee, B.W.; Okada, T.; Oyabu, T.; Myojo, T.; Kawai, K.; Yatera, K.; et al. Comparison of Pulmonary Inflammatory Responses Following Intratracheal Instillation and Inhalation of Nanoparticles. Nanotoxicology 2016, 10, 607–618. [Google Scholar] [CrossRef]
- Morimoto, Y.; Izumi, H.; Yoshiura, Y.; Tomonaga, T.; Oyabu, T.; Myojo, T.; Kawai, K.; Yatera, K.; Shimada, M.; Kubo, M.; et al. Evaluation of Pulmonary Toxicity of Zinc Oxide Nanoparticles Following Inhalation and Intratracheal Instillation. Int. J. Mol. Sci. 2016, 17, 1241. [Google Scholar] [CrossRef]
- Luo, Y.; Deng, J.; Cui, Y.; Li, T.; Bai, J.; Huang, L.; Sun, Y.; Dong, F.; Zhang, Q. Long-Term Instillation to Four Natural Representative Chrysotile of China Induce the Inactivation of P53 and P16 and the Activation of C-JUN and C-FOS in the Lung Tissues of Wistar Rats. Toxicol. Lett. 2020, 333, 140–149. [Google Scholar] [CrossRef]
- Cyphert, J.M.; McGee, M.A.; Nyska, A.; Schladweiler, M.C.; Kodavanti, U.P.; Gavett, S.H. Long-Term Toxicity of Naturally Occurring Asbestos in Male Fischer 344 Rats. J. Toxicol. Environ. Health A 2016, 79, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Nishida, C.; Izumi, H.; Tomonaga, T.; Wang, K.-Y.; Higashi, H.; Takeshita, J.-I.; Ono, R.; Sumiya, K.; Fujii, S.; Hata, Y.; et al. Effect of Different Molecular Weights of Polyacrylic Acid on Rat Lung Following Intratracheal Instillation. Int. J. Mol. Sci. 2022, 2022, 10345. [Google Scholar] [CrossRef]
- Kamp, D.W.; Liu, G.; Cheresh, P.; Kim, S.-J.; Mueller, A.; Lam, A.P.; Trejo, H.; Williams, D.; Tulasiram, S.; Baker, M.; et al. Asbestos-Induced Alveolar Epithelial Cell Apoptosis the Role of Endoplasmic Reticulum Stress Response. Am. J. Respir. Cell Mol. Biol. 2013, 49, 892–901. [Google Scholar] [CrossRef]
- Ryan, A.J.; Larson-Casey, J.L.; He, C.; Murthy, S.; Brent Carter, A. Asbestos-Induced Disruption of Calcium Homeostasis Induces Endoplasmic Reticulum Stress in Macrophages. J. Biol. Chem. 2014, 289, 33391–33403. [Google Scholar] [CrossRef] [PubMed]
- Korfei, M.; Ruppert, C.; Mahavadi, P.; Henneke, I.; Markart, P.; Koch, M.; Lang, G.; Fink, L.; Bohle, R.M.; Seeger, W.; et al. Epithelial Endoplasmic Reticulum Stress and Apoptosis in Sporadic Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2008, 178, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Ayaub, E.A.; Kolb, P.S.; Mohammed-Ali, Z.; Tat, V.; Murphy, J.; Bellaye, P.S.; Shimbori, C.; Boivin, F.J.; Lai, R.; Lynn, E.G.; et al. GRP78 and CHOP Modulate Macrophage Apoptosis and the Development of Bleomycin-Induced Pulmonary Fibrosis. J. Pathol. 2016, 239, 411–425. [Google Scholar] [CrossRef]
- Yao, Y.; Wang, Y.; Zhang, Z.; He, L.; Zhu, J.; Zhang, M.; He, X.; Cheng, Z.; Ao, Q.; Cao, Y.; et al. Chop Deficiency Protects Mice against Bleomycin-Induced Pulmonary Fibrosis by Attenuating M2 Macrophage Production. Mol. Ther. 2016, 24, 915–925. [Google Scholar] [CrossRef]
- Tan, S.; Yang, S.; Chen, M.; Wang, Y.; Zhu, L.; Sun, Z.; Chen, S. Lipopolysaccharides Promote Pulmonary Fibrosis in Silicosis through the Aggravation of Apoptosis and Inflammation in Alveolar Macrophages. Open Life Sci. 2020, 15, 598–605. [Google Scholar] [CrossRef]
- Tomonaga, T.; Nishida, C.; Izumi, H.; Kawai, N.; Wang, K.Y.; Higashi, H.; Takeshita, J.I.; Ono, R.; Sumiya, K.; Fujii, S.; et al. Crosslinked Structure of Polyacrylic Acid Affects Pulmonary Fibrogenicity in Rats. Int. J. Mol. Sci. 2022, 23, 13870. [Google Scholar] [CrossRef]
- Oyabu, T.; Morimoto, Y.; Hirohashi, M.; Horie, M.; Kambara, T.; Lee, B.W.; Hashiba, M.; Mizuguchi, Y.; Myojo, T.; Kuroda, E. Dose-Dependent Pulmonary Response of Well-Dispersed Titanium Dioxide Nanoparticles Following Intratracheal Instillation. J. Nanoparticle Res. 2013, 15, 1600. [Google Scholar] [CrossRef]
- Morrow, P.E.; Muhle, H.; Mermelstein, R. Chronic Inhalation Study Findings as a Basis for Proposing a New Occupational Dust Exposure Limit. J. Am. Coll. Toxicol. 1991, 10, 279–290. [Google Scholar] [CrossRef]
- Bellmann, B.; Muhle, H.; Creutzenberg, O.; Mermelstein, R. Irreversible Pulmonary Changes Induced in Rat Lung by Dust Overload. Environ. Health Perspect. 1992, 97, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Ran, D.; Liang, X.; Zhao, K.; Zhang, Q.; Zhou, M.; He, P. Cigarette Smoke-Induced Lung Inflammation in COPD Mediated via LTB4/BLT1/SOCs1 Pathway. Int. J. COPD 2016, 11, 31–41. [Google Scholar] [CrossRef]
- Nishida, C.; Izumi, H.; Tomonaga, T.; Takeshita, J.I.; Wang, K.Y.; Yamasaki, K.; Yatera, K.; Morimoto, Y. Predictive Biomarkers for the Ranking of Pulmonary Toxicity of Nanomaterials. Nanomaterials 2020, 10, 2032. [Google Scholar] [CrossRef] [PubMed]
- Koi, C.; Izumi, H.; Kurita, T.; Nguyen, T.T.; Murakami, M.; Yoshiura, Y.; Hachisuga, T.; Morimoto, Y. Lovastatin Induced Kruppel like Factor 2 (KLF2), Kruppel like Factor 6 (KLF6) and Ras Homolog Family Member B (RHOB) Genes and Preferentially Led to Viability Reduction of Cisplatin-Resistant Cells. Oncotarget 2017, 8, 106429–106442. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, T.; Simpson, J.M.; Timbrell, V. Simple Method of Estimating Severity of Pulmonary Fibrosis on a Numerical Scale. J. Clin. Pathol. 1988, 41, 467–470. [Google Scholar] [CrossRef]
- Zhang, J.H.; Tasaki, T.; Tsukamoto, M.; Wang, K.Y.; Kubo, K.Y.; Azuma, K. Deletion of Wnt10a Is Implicated in Hippocampal Neurodegeneration in Mice. Biomedicines 2022, 10, 1500. [Google Scholar] [CrossRef]



| Physicochemical Characterization | |
|---|---|
| Structural formula |  |
| Weight average molecular weight (Mw) | 2.69 × 105 g/mol |
| Number average molecular weight (Mn) | 2.20 × 105 g/mol |
| Poly dispersity index (PDI) | 1.22 |
| Degree of cross-linking | None |
| Radius of gyration (Rg) | 49.8 nm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morimoto, T.; Izumi, H.; Tomonaga, T.; Nishida, C.; Kawai, N.; Higashi, Y.; Wang, K.-Y.; Ono, R.; Sumiya, K.; Sakurai, K.; et al. The Effects of Endoplasmic Reticulum Stress via Intratracheal Instillation of Water-Soluble Acrylic Acid Polymer on the Lungs of Rats. Int. J. Mol. Sci. 2024, 25, 3573. https://doi.org/10.3390/ijms25073573
Morimoto T, Izumi H, Tomonaga T, Nishida C, Kawai N, Higashi Y, Wang K-Y, Ono R, Sumiya K, Sakurai K, et al. The Effects of Endoplasmic Reticulum Stress via Intratracheal Instillation of Water-Soluble Acrylic Acid Polymer on the Lungs of Rats. International Journal of Molecular Sciences. 2024; 25(7):3573. https://doi.org/10.3390/ijms25073573
Chicago/Turabian StyleMorimoto, Toshiki, Hiroto Izumi, Taisuke Tomonaga, Chinatsu Nishida, Naoki Kawai, Yasuyuki Higashi, Ke-Yong Wang, Ryohei Ono, Kazuki Sumiya, Kazuo Sakurai, and et al. 2024. "The Effects of Endoplasmic Reticulum Stress via Intratracheal Instillation of Water-Soluble Acrylic Acid Polymer on the Lungs of Rats" International Journal of Molecular Sciences 25, no. 7: 3573. https://doi.org/10.3390/ijms25073573
APA StyleMorimoto, T., Izumi, H., Tomonaga, T., Nishida, C., Kawai, N., Higashi, Y., Wang, K.-Y., Ono, R., Sumiya, K., Sakurai, K., Moriyama, A., Takeshita, J.-i., Yamasaki, K., Yatera, K., & Morimoto, Y. (2024). The Effects of Endoplasmic Reticulum Stress via Intratracheal Instillation of Water-Soluble Acrylic Acid Polymer on the Lungs of Rats. International Journal of Molecular Sciences, 25(7), 3573. https://doi.org/10.3390/ijms25073573