
.jpg)

Increased Leptin Levels in Plasma and Serum in Patients with Metabolic Disorders: A Systematic Review and Meta-Analysis

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Quality Appraisal
2.5. Statistical Analyses
3. Results
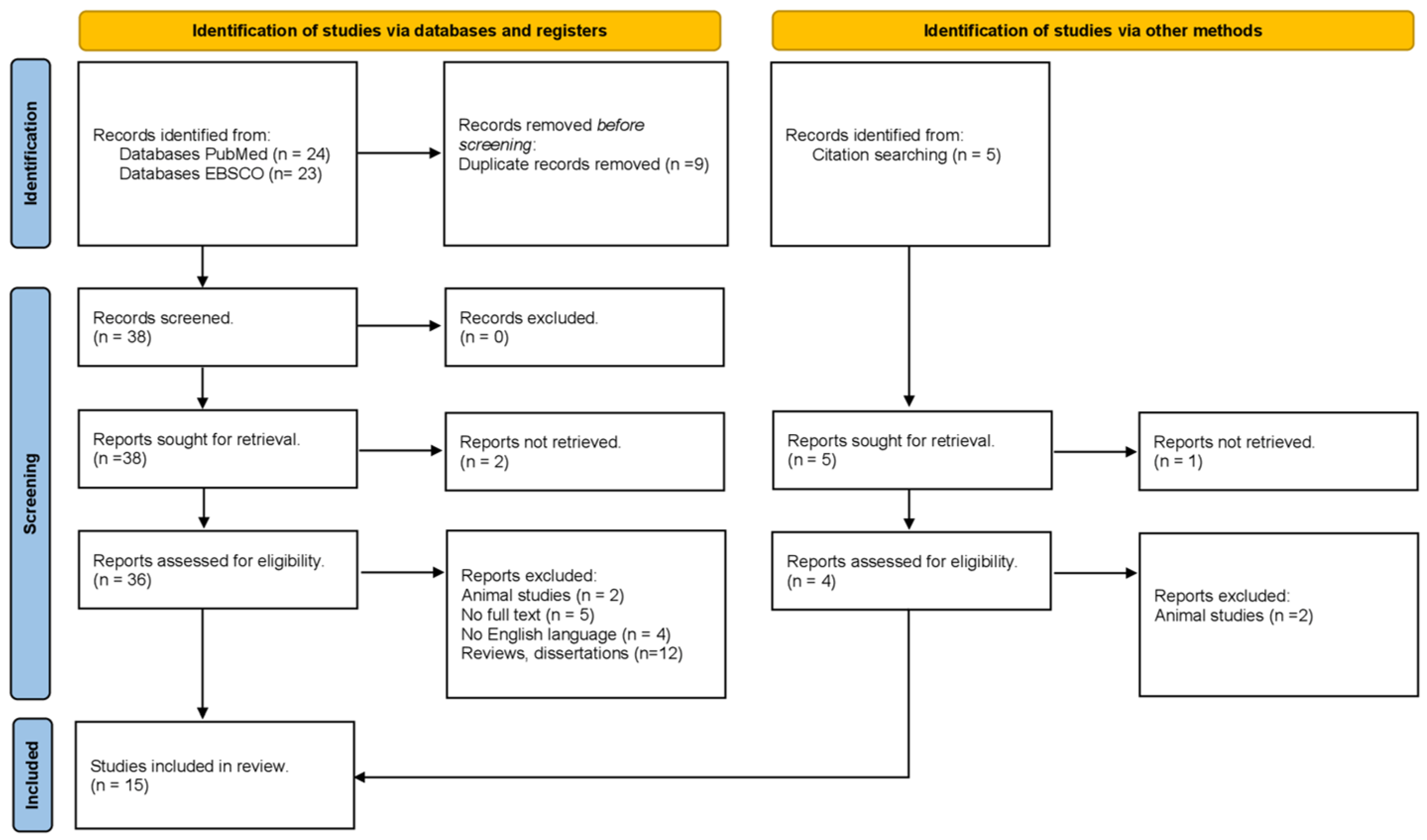
3.1. Literature Screening Process and Results
3.2. Methodological Characteristics of the Studies
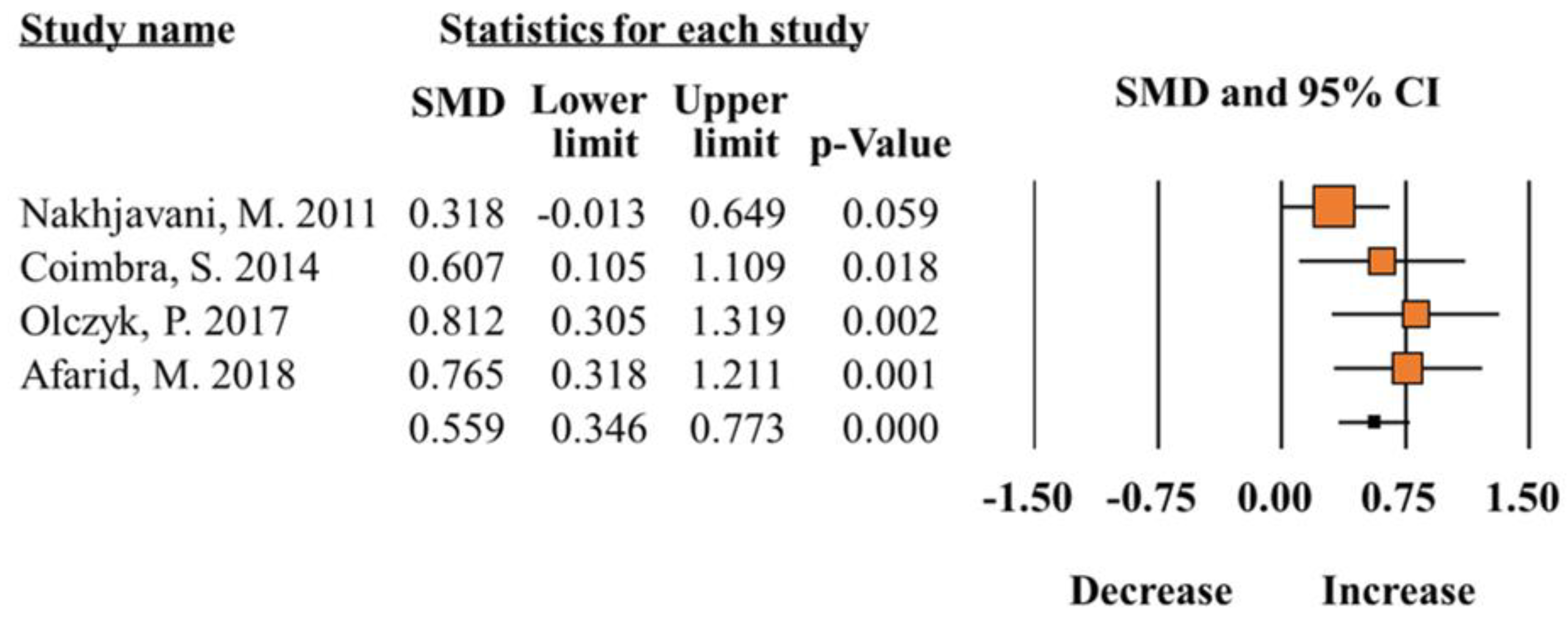
3.3. Meta-Analysis of Leptin Levels in Individuals with Diabetes vs. Controls
3.4. Meta-Analysis of Total Leptin Levels in Individual with Obesity vs. Controls
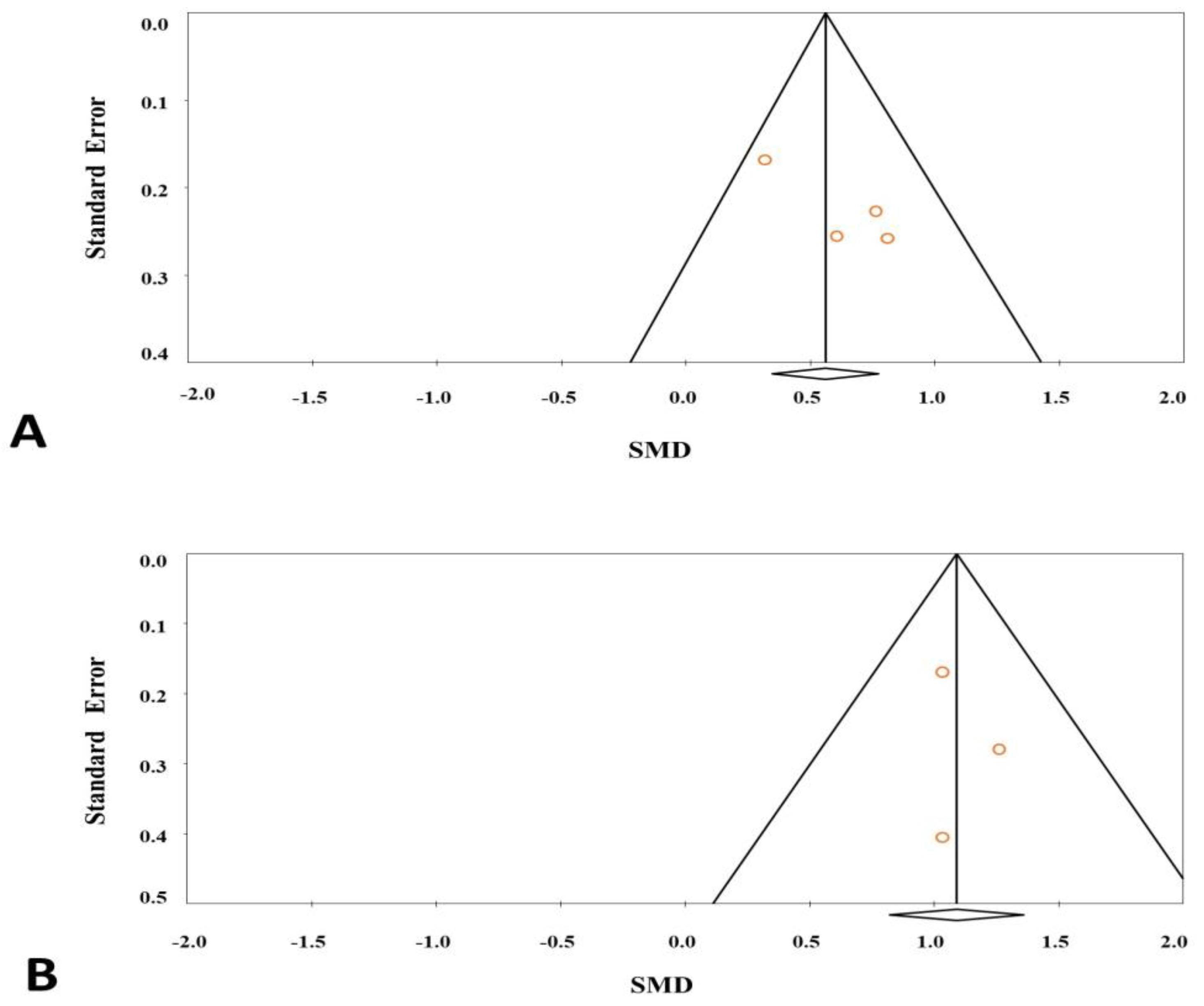
3.5. Evaluation of Publication Bias
3.6. Meta-Regression and Sensitivity Analysis
3.7. Quality Appraisal
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liao, Y.C.; Lim, Y.S.; Chu, P.W.; Chen, S.K. Inflammatory Milieu Induces Mitochondrial Alterations and Neuronal Activations in Hypothalamic POMC Neurons in a Time-Dependent Manner. Mol. Neurobiol. 2022, 60, 1164–1178. [Google Scholar] [CrossRef]
- Ayo-Martin, O.; García-García, J.; Hernández-Fernández, F.; Gómez-Hontanilla, M.; Gómez-Fernández, I.; Andrés-Fernández, C.; Lamas, C.; Alfaro-Martínez, J.J.; Botella, F.; Segura, T. Cerebral hemodynamics in obesity: Relationship with sex, age, and adipokines in a cohort-based study. GeroScience 2021, 43, 1465–1479. [Google Scholar] [CrossRef]
- Farooqi, I.S.; O’Rahilly, S. Leptin: A pivotal regulator of human energy homeostasis. Am. J. Clin. Nutr. 2009, 89, 980S–984S. [Google Scholar] [CrossRef]
- Obradovic, M.; Sudar-Milovanovic, E.; Soskic, S.; Essack, M.; Arya, S.; Stewart, A.J.; Gojobori, T.; Isenovic, E.R. Leptin and Obesity: Role and Clinical Implication. Front. Endocrinol. 2021, 12, 585887. [Google Scholar] [CrossRef]
- Huang, J.; Peng, X.; Dong, K.; Tao, J.; Yang, Y. The Association Between Insulin Resistance, Leptin, and Resistin and Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients with Different Body Mass Indexes. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 2357–2365. [Google Scholar] [CrossRef]
- Yin, H.; Tian, S.; Huang, R.; Cai, R.; Guo, D.; Lin, H.; Wang, J.; Wang, S. Low Plasma Leptin and High Soluble Leptin Receptor Levels Are Associated With Mild Cognitive Impairment in Type 2 Diabetic Patients. Front. Aging Neurosci. 2018, 10, 132. [Google Scholar] [CrossRef]
- Flier, J.S.; Ahima, R.S. Leptin physiology and pathophysiology: Knowns and unknowns 30 years after its discovery. J. Clin. Investig. 2024, 134, 1. [Google Scholar] [CrossRef]
- Hanaki, K.; Becker, D.J.; Arslanian, S.A. Leptin before and after insulin therapy in children with new-onset type 1 diabetes. J. Clin. Endocrinol. Metab. 1999, 84, 1524–1526. [Google Scholar] [CrossRef]
- Tatti, P.; Masselli, L.; Buonanno, A.; Di Mauro, P.; Strollo, F. Leptin levels in diabetic and nondiabetic subjects. Endocrine 2001, 15, 305–308. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Attas, O.S.; Al-Rubeaan, K.; Mohieldin, M.; Al-Katari, M.; Jones, A.F.; Kumar, S. Serum leptin and its relation to anthropometric measures of obesity in pre-diabetic Saudis. Cardiovasc. Diabetol. 2007, 6, 18. [Google Scholar] [CrossRef]
- Ozkan, Y.; Aydin, S.; Donder, E.; Koca, S.S.; Aydin, S.; Ozkan, B.; Sahin, I. Effect of orlistat on the total ghrelin and leptin levels in obese patients. J. Physiol. Biochem. 2009, 65, 215–223. [Google Scholar] [CrossRef]
- Nakhjavani, M.; Esteghamati, A.; Tarafdari, A.M.; Nikzamir, A.; Ashraf, H.; Abbasi, M. Association of plasma leptin levels and insulin resistance in diabetic women: A cross-sectional analysis in an Iranian population with different results in men and women. Gynecol. Endocrinol. 2011, 27, 14–19. [Google Scholar] [CrossRef]
- Morteza, A.; Nakhjavani, M.; Asgarani, F.; Ghaneei, A.; Esteghamati, A.; Mirmiranpour, H. The lost correlation between leptin and CRP in type 2 diabetes. Eur. Cytokine Netw. 2013, 24, 53–59. [Google Scholar] [CrossRef]
- Al-Hamodi, Z.; Al-Habori, M.; Al-Meeri, A.; Saif-Ali, R. Association of adipokines, leptin/adiponectin ratio and C-reactive protein with obesity and type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2014, 6, 99. [Google Scholar] [CrossRef]
- Coimbra, S.; Brandão Proença, J.; Santos-Silva, A.; Neuparth, M.J. Adiponectin, leptin, and chemerin in elderly patients with type 2 diabetes mellitus: A close linkage with obesity and length of the disease. BioMed Res. Int. 2014, 2014, 701915. [Google Scholar] [CrossRef]
- Olczyk, P.; Koprowski, R.; Komosinska-Vassev, K.; Jura-Półtorak, A.; Winsz-Szczotka, K.; Kuźnik-Trocha, K.; Mencner, Ł.; Telega, A.; Ivanova, D.; Olczyk, K. Adiponectin, Leptin, and Leptin Receptor in Obese Patients with Type 2 Diabetes Treated with Insulin Detemir. Molecules 2017, 22, 1274. [Google Scholar] [CrossRef]
- Afarid, M.; Attarzadeh, A.; Farvardin, M.; Ashraf, H. The Association of Serum Leptin Level and Anthropometric Measures With the Severity of Diabetic Retinopathy in Type 2 Diabetes Mellitus. Med. Hypothesis Discov. Innov. Ophthalmol. J. 2018, 7, 156–162. [Google Scholar]
- Bidulescu, A.; Dinh, P.C., Jr.; Sarwary, S.; Forsyth, E.; Luetke, M.C.; King, D.B.; Liu, J.; Davis, S.K.; Correa, A. Associations of leptin and adiponectin with incident type 2 diabetes and interactions among African Americans: The Jackson heart study. BMC Endocr. Disord. 2020, 20, 31. [Google Scholar] [CrossRef]
- Katsogiannos, P.; Kamble, P.G.; Pereira, M.J.; Sundbom, M.; Carlsson, P.O.; Eriksson, J.W.; Espes, D. Changes in Circulating Cytokines and Adipokines After RYGB in Patients with and without Type 2 Diabetes. Obesity 2021, 29, 535–542. [Google Scholar] [CrossRef]
- Sitar-Tǎut, A.V.; Cozma, A.; Fodor, A.; Coste, S.C.; Orasan, O.H.; Negrean, V.; Pop, D.; Sitar-Tǎut, D.A. New Insights on the Relationship between Leptin, Ghrelin, and Leptin/Ghrelin Ratio Enforced by Body Mass Index in Obesity and Diabetes. Biomedicines 2021, 9, 1657. [Google Scholar] [CrossRef]
- Grasso, P. Harnessing the Power of Leptin: The Biochemical Link Connecting Obesity, Diabetes, and Cognitive Decline. Front. Aging Neurosci. 2022, 14, 861350. [Google Scholar] [CrossRef]
- Li, Y.; Chen, X.; Gong, X.; Yao, J.; He, D.; Du, W. Effect of Gender on Serum Leptin in Type 2 Diabetes Mellitus: A System Review and Meta-Analysis. Comput. Math. Methods Med. 2022, 2022, 4875799. [Google Scholar] [CrossRef]
- Kim, D.W.; Glendining, K.A.; Grattan, D.R.; Jasoni, C.L. Maternal Obesity in the Mouse Compromises the Blood-Brain Barrier in the Arcuate Nucleus of Offspring. Endocrinology 2016, 157, 2229–2242. [Google Scholar] [CrossRef]
- Tran, L.T.; Park, S.; Kim, S.K.; Lee, J.S.; Kim, K.W.; Kwon, O. Hypothalamic control of energy expenditure and thermogenesis. Exp. Mol. Med. 2022, 54, 358–369. [Google Scholar] [CrossRef]
- Amorim, M.R.; Aung, O.; Mokhlesi, B.; Polotsky, V.Y. Leptin-mediated neural targets in obesity hypoventilation syndrome. Sleep 2022, 45, zsac153. [Google Scholar] [CrossRef]
- Tacad, D.K.M.; Tovar, A.P.; Richardson, C.E.; Horn, W.F.; Krishnan, G.P.; Keim, N.L.; Krishnan, S. Satiety Associated with Calorie Restriction and Time-Restricted Feeding: Peripheral Hormones. Adv. Nutr. 2022, 13, 792–820. [Google Scholar] [CrossRef]
- Milek, M.; Moulla, Y.; Kern, M.; Stroh, C.; Dietrich, A.; Schön, M.R.; Gärtner, D.; Lohmann, T.; Dressler, M.; Kovacs, P.; et al. Adipsin Serum Concentrations and Adipose Tissue Expression in People with Obesity and Type 2 Diabetes. Int. J. Mol. Sci. 2022, 23, 2222. [Google Scholar] [CrossRef]
- Jiménez-Cortegana, C.; Hontecillas-Prieto, L.; García-Domínguez, D.J.; Zapata, F.; Palazón-Carrión, N.; Sánchez-León, M.L.; Tami, M.; Pérez-Pérez, A.; Sánchez-Jiménez, F.; Vilariño-García, T.; et al. Obesity and Risk for Lymphoma: Possible Role of Leptin. Int. J. Mol. Sci. 2022, 23, 15530. [Google Scholar] [CrossRef]
- Pan, W.H.; Flegal, K.M.; Chang, H.Y.; Yeh, W.T.; Yeh, C.J.; Lee, W.C. Body mass index and obesity-related metabolic disorders in Taiwanese and US whites and blacks: Implications for definitions of overweight and obesity for Asians. Am. J. Clin. Nutr. 2004, 79, 31–39. [Google Scholar] [CrossRef]
- Colin Bell, A.; Adair, L.S.; Popkin, B.M. Ethnic differences in the association between body mass index and hypertension. Am. J. Epidemiol. 2002, 155, 346–353. [Google Scholar] [CrossRef]
- Gaillard, T.; Osei, K. Ethnic differences in serum lipids and lipoproteins in overweight/obese African-American and white American women with pre-diabetes: Significance of NMR-derived lipoprotein particle concentrations and sizes. BMJ Open Diabetes Res. Care 2016, 4, e000246. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Year | Population | Main Results | |||||
|---|---|---|---|---|---|---|---|---|---|
| Sample | Ethnicity | Total | Control | Case | Study | ||||
| Hanaki et al. [8] | USA | 1999 | Serum | Caucasian | 38 | 19 | 19 | Diabetes | The results of this study demonstrate that patients with new-onset type 1 diabetes have low leptin levels. |
| Tatti et al. [9] | Italy | 2001 | Plasma | Caucasian | 300 | 160 | 140 | Diabetes | The leptin levels were lower in the diabetic population only when both sexes were combined, and were higher in the females of both groups. |
| Al-Daghri et al. [10] | Asia | 2007 | Serum | Afro-American | 222 | 80 | 142 | Diabetes | Leptin is associated with measures of adiposity (hip circumference, in particular) in the non-diabetic state among Saudi subjects. |
| Ozkan et al. [11] | Turkey | 2009 | Serum | Caucasian | 31 | 10 | 21 | Obesity | Leptin levels were lower in controls than in obese subjects. |
| Nakhjavani et al. [12] | Iran | 2011 | Plasma | Middle East | 142 | 71 | 71 | Diabetes | Leptin concentration correlated with obesity in female, but not male, diabetic subjects. |
| Morteza et al. [13] | Iran | 2013 | Serum | Middle East | 85 | 41 | 44 | Diabetes | A positive correlation between leptin levels in patients with T2DM was reported. |
| Al-Hamodi et al. [14] | Republic of Yemen | 2014 | Plasma | Caucasian | 92 | 46 | 46 | Diabetes and obesity | Leptin levels were higher in both obese subjects and non-obese T2DM patients. |
| Coimbra et al. [15] | Portugal | 2014 | Serum | Portuguese | 93 | 20 | 73 | Diabetes | Leptin levels in elderly patients with T2DM seem to be closely linked to obesity and to length of the disease. |
| Olczyk et al. [16] | Poland | 2017 | Plasma | Yemeni | 67 | 27 | 40 | Diabetes | Leptin values were significantly higher in patients with untreated T2DM. |
| Yin et al. [6] | USA | 2018 | Plasma | Caucasian | 124 | 63 | 61 | Diabetes | This study showed that a high level of leptin is associated with improved cognitive function in T2DM patients and more significantly in female individuals. |
| Afarid et al. [17] | Iran | 2018 | Serum | Middle East | 83 | 39 | 44 | Diabetes | Increased serum levels of leptin were associated with advanced stages of diabetic retinopathy in subjects with T2DM. |
| Bidulescu et al. [18] | USA | 2020 | Plasma | Caucasian | 3363 | 2779 | 584 | Diabetes | The association of leptin with incident T2DM was mediated by insulin resistance. |
| Katsogiannos et al. [19] | Sweden | 2021 | Plasma | Swedish | 59 | 25 | 34 | Diabetes and obesity | Leptin values were higher in all patients with obesity compared with healthy controls. |
| Sitar-Taut et al. [20] | Romania | 2021 | Serum | Caucasian | 29 | 12 | 17 | Obesity | Leptin levels were significantly higher in obese and diabetic patients. |
| Huang et al. [5] | China | 2021 | Serum | Asian | 196 | 144 | 52 | Obesity | Leptin values were higher for diabetic nephropathy in the T2DM patients. |
| Subgroup Analysis | Pooled Data | Heterogeneity | Egger p-Value | ||||
|---|---|---|---|---|---|---|---|
| Point Estimate | Lower | Upper | Z p-Value | Q p-Value | I2 | ||
| Diabetic vs. Healthy | 0.559 | 0.346 | 0.773 | 0.000 | 0.280 | 21.727 | 0.10774 |
| Subgroup | |||||||
| Male | 0.340 | 0.172 | 0.509 | 0.000 | 0.225 | 31.236 | 0.63029 |
| Female | 0.348 | 0.160 | 0.537 | 0.000 | 0.311 | 14.378 | 0.56557 |
| Middle East | 0.477 | 0.211 | 0.743 | 0.000 | 0.0116 | 59.583 | 0.39321 |
| Caucasian | −0.763 | −0.953 | −0.574 | 0.000 | 1.185 | 0.553 | 0.33844 |
| Plasma | 0.466 | 0.189 | 0.743 | 0.001 | 0.110 | 60.788 | 0.65302 |
| Serum | 0.695 | 0.361 | 1.029 | 0.000 | 0.646 | 0.000 | 0.71815 |
| Obese vs. Healthy | 1.090 | 0.822 | 1.358 | 0.000 | 0.777 | 0.000 | 0.73765 |
| Subgroup | |||||||
| Serum | 1.036 | 0.728 | 1.343 | 0.000 | 1.000 | 0.000 | 1.000 |
| Author | NOS Category | Assessment | ||
|---|---|---|---|---|
| Selection | Comparability | Outcome | ||
| Hanaki K. [8] | ⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Tatti P. [9] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Al-Daghri N.M. [10] | ⋆⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Ozkan Y. [11] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Nakhjavani M. [12] | ⋆⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Morteza A. [13] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Al-Hamodi Z. [14] | ⋆⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Coimbra S. [15] | ⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Olczyk P. [16] | ⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Yin H. [6] | ⋆⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Afarid M. [17] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Bidulescu A. [18] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Katsogiannos P. [19] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Sitar-Taut A. V. [20] | ⋆⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
| Huang J. [5] | ⋆⋆⋆ | ⋆⋆ | ⋆⋆ | Good |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Díaz, Y.; de los Ángeles Ovando-Almeida, M.; Fresán, A.; Juárez-Rojop, I.E.; Genis-Mendoza, A.D.; Nicolini, H.; González-Castro, T.B.; Tovilla-Zárate, C.A.; López-Narváez, M.L. Increased Leptin Levels in Plasma and Serum in Patients with Metabolic Disorders: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2024, 25, 12668. https://doi.org/10.3390/ijms252312668
Hernández-Díaz Y, de los Ángeles Ovando-Almeida M, Fresán A, Juárez-Rojop IE, Genis-Mendoza AD, Nicolini H, González-Castro TB, Tovilla-Zárate CA, López-Narváez ML. Increased Leptin Levels in Plasma and Serum in Patients with Metabolic Disorders: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2024; 25(23):12668. https://doi.org/10.3390/ijms252312668
Chicago/Turabian StyleHernández-Díaz, Yazmín, María de los Ángeles Ovando-Almeida, Ana Fresán, Isela Esther Juárez-Rojop, Alma Delia Genis-Mendoza, Humberto Nicolini, Thelma Beatriz González-Castro, Carlos Alfonso Tovilla-Zárate, and María Lilia López-Narváez. 2024. "Increased Leptin Levels in Plasma and Serum in Patients with Metabolic Disorders: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 25, no. 23: 12668. https://doi.org/10.3390/ijms252312668
APA StyleHernández-Díaz, Y., de los Ángeles Ovando-Almeida, M., Fresán, A., Juárez-Rojop, I. E., Genis-Mendoza, A. D., Nicolini, H., González-Castro, T. B., Tovilla-Zárate, C. A., & López-Narváez, M. L. (2024). Increased Leptin Levels in Plasma and Serum in Patients with Metabolic Disorders: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences, 25(23), 12668. https://doi.org/10.3390/ijms252312668