
Vitamin D Inadequacy Affects Skeletal Muscle Index and Physical Performance in Lumbar Disc Degeneration


Abstract
1. Introduction
2. Results
2.1. Characteristics of Participants with Vitamin D Sufficiency and Insufficiency
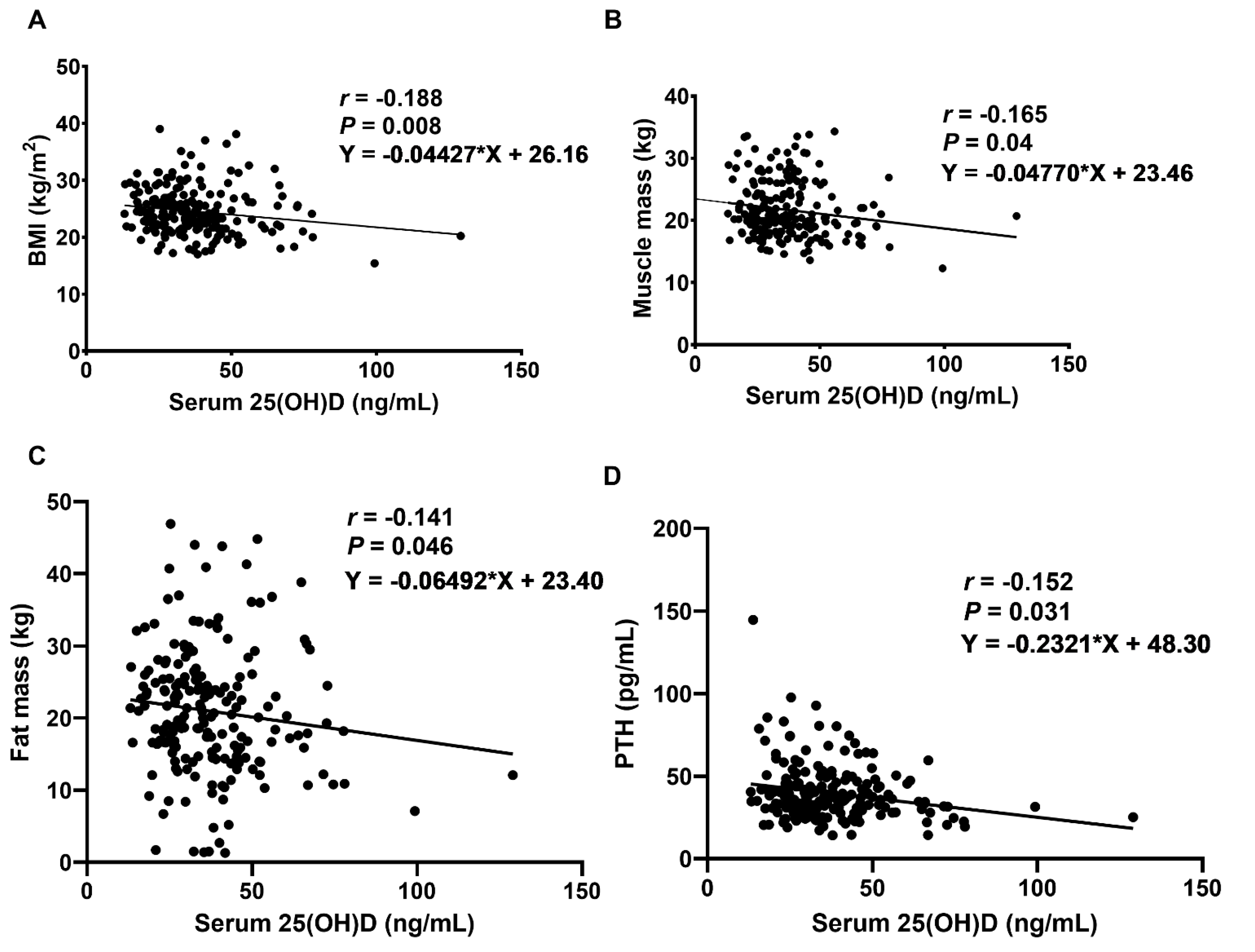
2.2. Relationship between Vitamin D Levels, Body Compositions, and PTH in LDD Patients
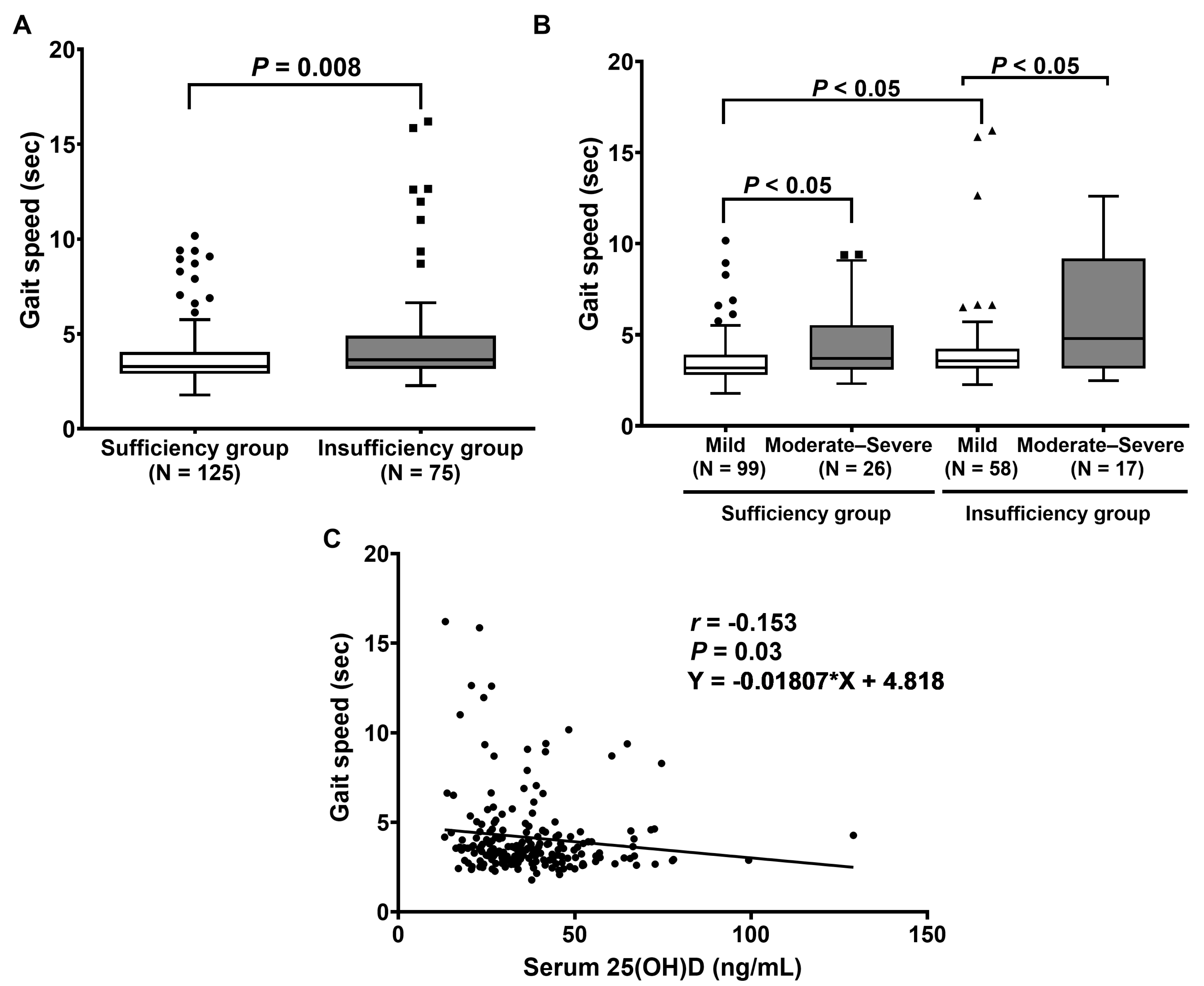
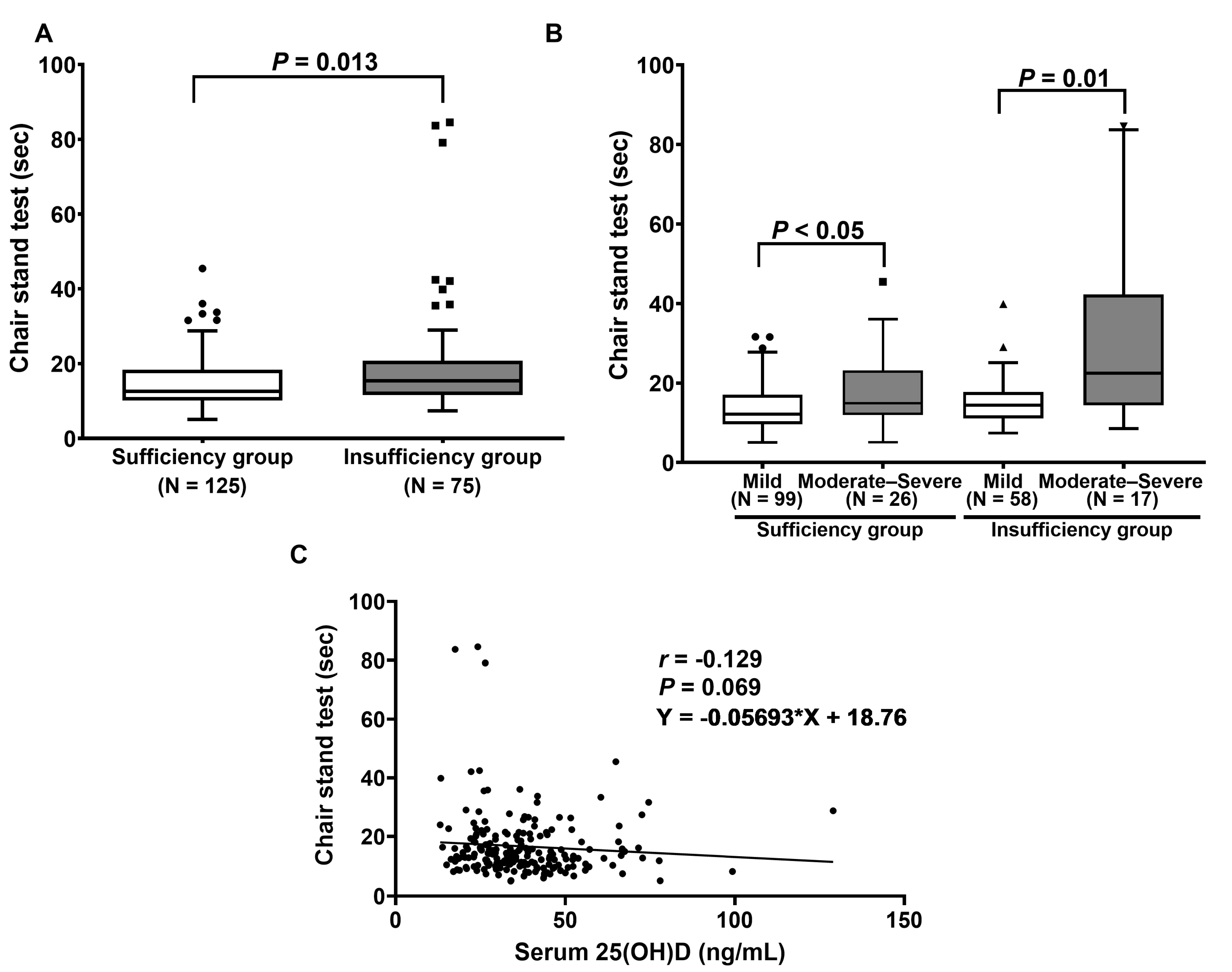
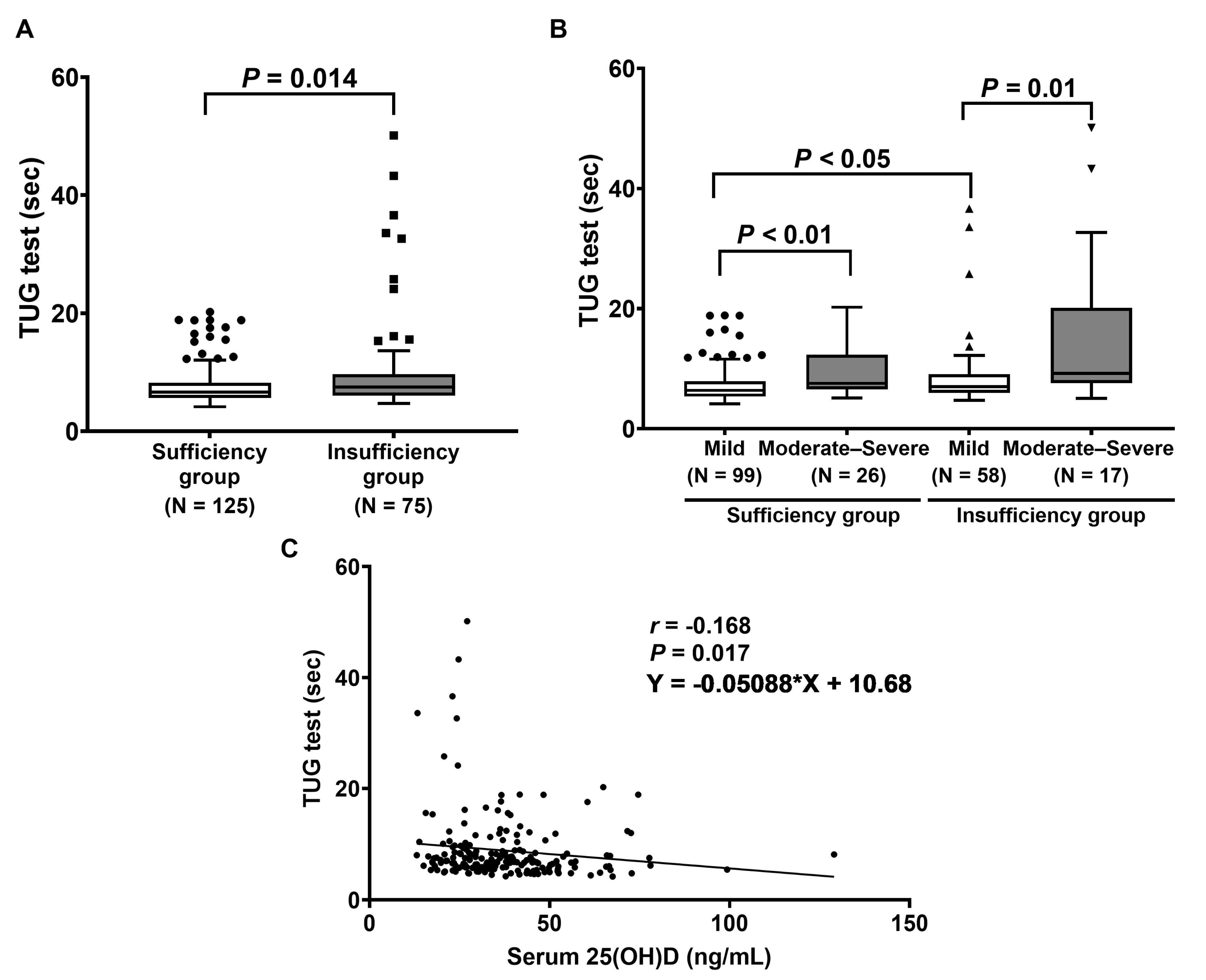
2.3. Effect of Vitamin D Levels on Muscle Strength and Physical Performance
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Visual Analog Scale and Oswestry Disability Index Assessment
4.3. Anthropometric and Body Composition Measurements
4.4. Muscle Strength and Physical Performance
4.5. Serum and Plasma Preparation
4.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 25(OH)D | 25-hydroxyvitamin D |
| 1,25(OH)D | 1,25-dihydroxyvitamin D |
| ASM | Appendicular skeletal mass |
| BIA | Bioelectrical impedance analysis |
| BMI | Body mass index |
| EQ-5D-5L | EuroQol-5 dimensions-5 level |
| IQR | Interquartile range |
| LDD | Lumbar disc degeneration |
| ODI | Oswestry Disability Index |
| PTH | Parathyroid hormone |
| SMI | Skeletal muscle index |
| SPPB | Short physical performance battery |
| SPSS | Statistical Package for the Social Sciences |
| TUG | Timed Up and Go |
| VAS | Visual analog scale |
| VDR | Vitamin D receptor |
| WC | Waist circumference |
References
- Vlaeyen, J.W.S.; Maher, C.G.; Wiech, K.; Van Zundert, J.; Meloto, C.B.; Diatchenko, L.; Battié, M.C.; Goossens, M.; Koes, B.; Linton, S.J. Low back pain. Nat. Rev. Dis. Prim. 2018, 4, 52. [Google Scholar] [CrossRef]
- Dechsupa, S.; Singhatanadgige, W.; Limthongkul, W.; Yingsakmongkol, W.; Ittipanichpong, T.; Honsawek, S. Alterations of relative telomere length and mitochondrial DNA copy number from ligamentum flavum-derived cells in lumbar spinal stenosis: Pilot study. Chula. Med. J. 2017, 61, 497–509. [Google Scholar]
- Jitjumnong, M.; Chalermkitpanit, P.; Suantawee, T.; Dechsupa, S.; Vajarintarangoon, L.; Honsawek, S. Telomere Short-ening and Increased Oxidative Stress in Lumbar Disc Degeneration. Int. J. Mol. Sci. 2022, 23, 10125. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-H.; Yoon, J.Y.; Lee, B.H.; Jung, H.-S.; Park, M.S.; Park, J.-O.; Moon, E.-S.; Kim, H.-S.; Lee, H.-M.; Moon, S.-H. Changes in Vitamin D Status After Surgery in Female Patients with Lumbar Spinal Stenosis and Its Clinical Significance. Spine 2012, 37, E1326–E1330. [Google Scholar] [CrossRef] [PubMed]
- Çalık, Y.; Aygün, Ü. Evaluation of vitamin D levels in patients with chronic low back-leg pain. Acta Orthop. et Traumatol. Turc. 2017, 51, 243–247. [Google Scholar] [CrossRef]
- Fernandes, M.R.; Barreto, W.D.R.J. Association between physical activity and vitamin D: A narrative literature review. Rev. Assoc. Med. Bras. 2017, 63, 550–556. [Google Scholar] [CrossRef]
- Dzik, K.P.; Grzywacz, T.; Łuszczyk, M.; Kujach, S.; Flis, D.J.; Kaczor, J.J. Single bout of exercise triggers the increase of vitamin D blood concentration in adolescent trained boys: A pilot study. Sci. Rep. 2022, 12, 1825. [Google Scholar] [CrossRef]
- Lips, P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: Consequences for bone loss and fractures and therapeutic implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar] [CrossRef]
- Keyimu, K.; Zhou, X.-H.; Miao, H.-J.; Zou, T. Relationship between vitamin D receptor gene polymorphism and mild cognitive impairment in elderly Uygur people. Int. J. Clin. Exp. Med. 2014, 7, 5282–5288. [Google Scholar]
- Kim, T.-H.; Lee, B.H.; Lee, H.-M.; Lee, S.-H.; Park, J.-O.; Kim, H.-S.; Kim, S.W.; Moon, S.-H. Prevalence of vitamin D deficiency in patients with lumbar spinal stenosis and its relationship with pain. Pain Physician 2013, 16, 165–176. [Google Scholar]
- Tieland, M.; Brouwer-Brolsma, E.M.; Nienaber-Rousseau, C.; van Loon, L.J.; De Groot, L.C. Low vitamin D status is associated with reduced muscle mass and impaired physical performance in frail elderly people. Eur. J. Clin. Nutr. 2013, 67, 1050–1055. [Google Scholar] [CrossRef]
- Olsson, K.; Saini, A.; Strömberg, A.; Alam, S.; Lilja, M.; Rullman, E.; Gustafsson, T. Evidence for Vitamin D Receptor Expression and Direct Effects of 1alpha,25(OH)2D3 in Human Skeletal Muscle Precursor Cells. Endocrinology 2016, 157, 98–111. [Google Scholar] [CrossRef]
- Colombini, A.; Lanteri, P.; Lombardi, G.; Grasso, D.; Recordati, C.; Lovi, A.; Banfi, G.; Bassani, R.; Brayda-Bruno, M. Metabolic effects of vitamin D active metabolites in monolayer and micromass cultures of nucleus pulposus and annulus fibrosus cells isolated from human intervertebral disc. Int. J. Biochem. Cell Biol. 2012, 44, 1019–1030. [Google Scholar] [CrossRef]
- Abboud, M.; Rybchyn, M.; Ning, Y.; Brennan-Speranza, T.; Girgis, C.; Gunton, J.; Fraser, D.; Mason, R. 1,25-Dihydroxycholecalciferol (calcitriol) modifies uptake and release of 25-hydroxycholecalciferol in skeletal muscle cells in culture. J. Steroid Biochem. Mol. Biol. 2018, 177, 109–115. [Google Scholar] [CrossRef]
- Amphansap, T.; Wongthanakitcharoen, P.; Stitkitti, N.; Chaiyosburana, W.; Therdyothin, A. Prevalence and risk factors of vitamin D indequacy among Thai elderly patients with osteoporotic hip fracture. J. Southeast Asian Med. Res. 2022, 6, e011. [Google Scholar] [CrossRef]
- Visser, M.; Deeg, D.J.H.; Lips, P. Low Vitamin D and High Parathyroid Hormone Levels as Determinants of Loss of Muscle Strength and Muscle Mass (Sarcopenia): The Longitudinal Aging Study Amsterdam. J. Clin. Endocrinol. Metab. 2003, 88, 5766–5772. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Bhat, M.; Kalam, R.; Qadri, S.S.; Madabushi, S.; Ismail, A. Vitamin D Deficiency-Induced Muscle Wasting Occurs through the Ubiquitin Proteasome Pathway and Is Partially Corrected by Calcium in Male Rats. Endocrinology 2013, 154, 4018–4029. [Google Scholar] [CrossRef] [PubMed]
- Manoy, P.; Yuktanandana, P.; Tanavalee, A.; Anomasiri, W.; Ngarmukos, S.; Tanpowpong, T.; Honsawek, S. Vitamin D Supple-mentation Improves Quality of Life and Physical Performance in Osteoarthritis Patients. Nutrients 2017, 9, 799. [Google Scholar] [CrossRef] [PubMed]
- Dzik, K.; Skrobot, W.; Flis, D.J.; Karnia, M.; Libionka, W.; Kloc, W.; Kaczor, J.J. Vitamin D supplementation attenuates oxidative stress in paraspinal skeletal muscles in patients with low back pain. Eur. J. Appl. Physiol. 2017, 118, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Ghai, B.; Bansal, D.; Kapil, G.; Kanukula, R.; Lavudiya, S.; Sachdeva, N. High Prevalence of Hypovitaminosis D in Indian Chronic Low Back Patients. Pain Physician 2015, 18, E853–E862. [Google Scholar]
- Lodh, M.; Goswami, B.; Mahajan, R.D.; Sen, D.; Jajodia, N.; Roy, A. Assessment of Vitamin D status In Patients of Chronic Low Back Pain of Unknown Etiology. Indian J. Clin. Biochem. 2014, 30, 174–179. [Google Scholar] [CrossRef]
- Bislev, L.S.; Langagergaard Rodbro, L.; Rolighed, L.; Sikjaer, T.; Rejnmark, L. Effects of Vitamin D3 Supplementation on Muscle Strength, Mass, and Physical Performance in Women with Vitamin D Insufficiency: A Randomized Place-bo-Controlled Trial. Calcif. Tissue Int. 2018, 103, 483–493. [Google Scholar] [CrossRef]
- Uchiyama, M.; Mizukami, S.; Arima, K.; Nishimura, T.; Tomita, Y.; Abe, Y.; Tanaka, N.; Honda, Y.; Goto, H.; Hasegawa, M.; et al. Association between serum 25-hydroxyvitamin D and physical performance measures in middle-aged and old Japanese men and women: The Unzen study. PLoS ONE 2021, 16, e0261639. [Google Scholar] [CrossRef]
- Montenegro, K.R.; Cruzat, V.; Carlessi, R.; Newsholme, P. Mechanisms of vitamin D action in skeletal muscle. Nutr. Res. Rev. 2019, 32, 192–204. [Google Scholar] [CrossRef]
- Girgis, C.M.; Mokbel, N.; Cha, K.M.; Houweling, P.J.; Abboud, M.; Fraser, D.R.; Mason, R.S.; Clifton-Bligh, R.J.; Gunton, J.E. The vitamin D receptor (VDR) is expressed in skeletal muscle of male mice and modulates 25-hydroxyvitamin D (25OHD) uptake in myofibers. Endocrinology 2014, 155, 3227–3237. [Google Scholar] [CrossRef]
- Iolascon, G.; Mauro, G.L.; Fiore, P.; Cisari, C.; Benedetti, M.G.; Panella, L.; De Sire, A.; Calafiore, D.; Moretti, A.; Gimigliano, F. Can vitamin D deficiency influence muscle performance in postmenopausal women? A multicentre retrospective study. Eur. J. Phys. Rehabil. Med. 2018, 54, 676–682. [Google Scholar] [CrossRef]
- Ryan, Z.C.; Craig, T.A.; Folmes, C.D.; Wang, X.; Lanza, I.R.; Schaible, N.S.; Salisbury, J.L.; Nair, K.S.; Terzic, A.; Sieck, G.C.; et al. 1alpha,25-Dihydroxyvitamin D3 Regulates Mitochondrial Oxygen Consumption and Dynamics in Human Skeletal Muscle Cells. J. Biol. Chem. 2016, 291, 1514–1528. [Google Scholar] [CrossRef]
- Welford, A.E.; Darling, A.L.; Allison, S.J.; Lanham-New, S.A.; Greig, C.A. Lack of significant seasonal association between serum 25(OH)D concentration, muscle mass and strength in postmenopausal women from the D-FINES longitudinal study. J. Nutr. Sci. 2022, 11, e107. [Google Scholar] [CrossRef]
- Sanjaroensuttikul, N. The Oswestry low back pain disability questionnaire (version 1.0) Thai version. J. Med. Assoc. Thail. 2007, 90, 1417. [Google Scholar]
- Manoy, P.; Anomasiri, W.; Yuktanandana, P.; Tanavalee, A.; Ngarmukos, S.; Tanpowpong, T.; Honsawek, S. Elevated serum leptin levels are associated with low vitamin D, sarcopenic obesity, poor muscle strength, and physical performance in knee osteoarthritis. Biomarkers 2017, 22, 723–730. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Vitamin D Status | p-Value | |
|---|---|---|---|
| Sufficiency Group (n = 125) | Insufficiency Group (n = 75) | ||
| Age (years) | 66.1 ± 9.3 | 66.2 ± 9.6 | 0.366 b |
| Gender, n (%) Female Male | 98 (78.4) 27 (21.6) | 57 (76.0) 18 (24.0) | 0.728 a |
| Body composition BMI (kg/m2) Muscle mass (kg) Percentage of fat mass (%) Fat mass (kg) ASM (kg) SMI (%) | 24.2 ± 4.3 20.3 (22.4–20.7) 32.6 ± 11.0 20.5 ± 9.3 16.0 (17.2–16.3) 28.2 ± 4.3 | 25.0 ± 3.8 21.1 (22.9–20.9) 34.3 ± 8.9 21.7 ± 7.7 16.0 (17.4–16.3) 27.3 ± 3.3 | 0.388 b 0.424 c 0.034b 0.067 b 0.649 c 0.030b |
| Serum 25(OH)D (ng/mL) | 41.2 (48.0–42.8) | 24.5 (24.7–22.7) | <0.0001c |
| PTH (pg/mL) | 37.5 ± 14.1 | 43.1 ± 20.5 | 0.027b |
| VAS (0–10) | 5.0 (6.0–5.0) | 6.0 (6.0–4.7) | 0.991 c |
| Oswestry Disability Index (ODI) | 30.3 ± 12.1 | 30.5 ± 14.2 | 0.147 b |
| Oswestry Disability Index (ODI) Mild disability, n (%) Moderate disability, n (%) Severe disability, n (%) | 99 (79.2) 25 (20.0) 1 (0.8) | 58 (77.3) 16 (21.3) 1 (1.3) | 0.907 a |
| EQ-5D-5L | 0.7 (0.7–0.6) | 0.7 (0.7–0.6) | 0.611 c |
| Variables | r | p-Value | 95% CI |
|---|---|---|---|
| Age (years) | 0.085 | 0.233 | (−0.060 to 0.236) |
| BMI (kg/m2) | −0.188 | 0.008 | (−0.332 to −0.048) |
| Muscle mass (kg) | −0.157 | 0.026 | (−0.281 to −0.008) |
| Percent of fat mass (%) | −0.056 | 0.429 | (−0.168 to 0.087) |
| Fat mass (kg) | −0.141 | 0.046 | (−0.263 to −0.008) |
| ASM (kg) | −0.115 | 0.105 | (−0.250 to 0.012) |
| SMI (%) | 0.131 | 0.065 | (−0.009 to 0.262) |
| VAS | 0.024 | 0.738 | (−0.119 to 0.165) |
| ODI | 0.013 | 0.853 | (−0.145 to 0.160) |
| EQ-5D-5L | 0.012 | 0.861 | (−0.131 to 0.154) |
| PTH (pg/mL) | −0.125 | 0.031 | (−0.315 to −0.007) |
| Grip strength (kg) | −0.058 | 0.417 | (−0.187 to 0.080) |
| Balance test (points) | 0.041 | 0.566 | (−0.089 to 0.180) |
| Gait speed (s) | −0.153 | 0.030 | (−0.013 to −0.287) |
| Chair stand test (s) | −0.129 | 0.069 | (−0.260 to 0.014) |
| Timed Up and Go test (s) | −0.168 | 0.017 | (−0.331 to −0.016) |
| Short physical performance battery (SPPB) (points) | 0.118 | 0.095 | (−0.022 to 0.271) |
| Variables | Vitamin D Status | p-Value | |
|---|---|---|---|
| Sufficiency Group (n = 125) | Insufficiency Group (n = 75) | ||
| Grip strength Dominant (kg) | 18.9 (21.5–19.1) | 19.1 (22.2–18.8) | 0.829 |
| Physical performance Balance test (points) Gait speed (s) Chair stand test (s) Timed Up and Go test (s) | 4.0 (3.8–3.5) 3.3 (4.1–3.5) 13.4 (17.9–14.4) 6.6 (8.5–7.2) | 4.0 (3.6–3.0) 3.7 (5.9–4.1) 15.4 (22.9–16.0) 7.5 (12.4–8.3) | 0.056 0.008 0.013 0.014 |
| SPPB (points) | 10.0 (10.3–9.7) | 10.0 (9.6–8.3) | 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dechsupa, S.; Yingsakmongkol, W.; Limthongkul, W.; Singhatanadgige, W.; Jitjumnong, M.; Honsawek, S. Vitamin D Inadequacy Affects Skeletal Muscle Index and Physical Performance in Lumbar Disc Degeneration. Int. J. Mol. Sci. 2023, 24, 3152. https://doi.org/10.3390/ijms24043152
Dechsupa S, Yingsakmongkol W, Limthongkul W, Singhatanadgige W, Jitjumnong M, Honsawek S. Vitamin D Inadequacy Affects Skeletal Muscle Index and Physical Performance in Lumbar Disc Degeneration. International Journal of Molecular Sciences. 2023; 24(4):3152. https://doi.org/10.3390/ijms24043152
Chicago/Turabian StyleDechsupa, Sinsuda, Wicharn Yingsakmongkol, Worawat Limthongkul, Weerasak Singhatanadgige, Manassanan Jitjumnong, and Sittisak Honsawek. 2023. "Vitamin D Inadequacy Affects Skeletal Muscle Index and Physical Performance in Lumbar Disc Degeneration" International Journal of Molecular Sciences 24, no. 4: 3152. https://doi.org/10.3390/ijms24043152
APA StyleDechsupa, S., Yingsakmongkol, W., Limthongkul, W., Singhatanadgige, W., Jitjumnong, M., & Honsawek, S. (2023). Vitamin D Inadequacy Affects Skeletal Muscle Index and Physical Performance in Lumbar Disc Degeneration. International Journal of Molecular Sciences, 24(4), 3152. https://doi.org/10.3390/ijms24043152