
Oral Infection, Oral Pathology and Salivary Diagnostics of Mpox Disease: Relevance in Dentistry and OMICs Perspectives
 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Study Design and Search Strategy
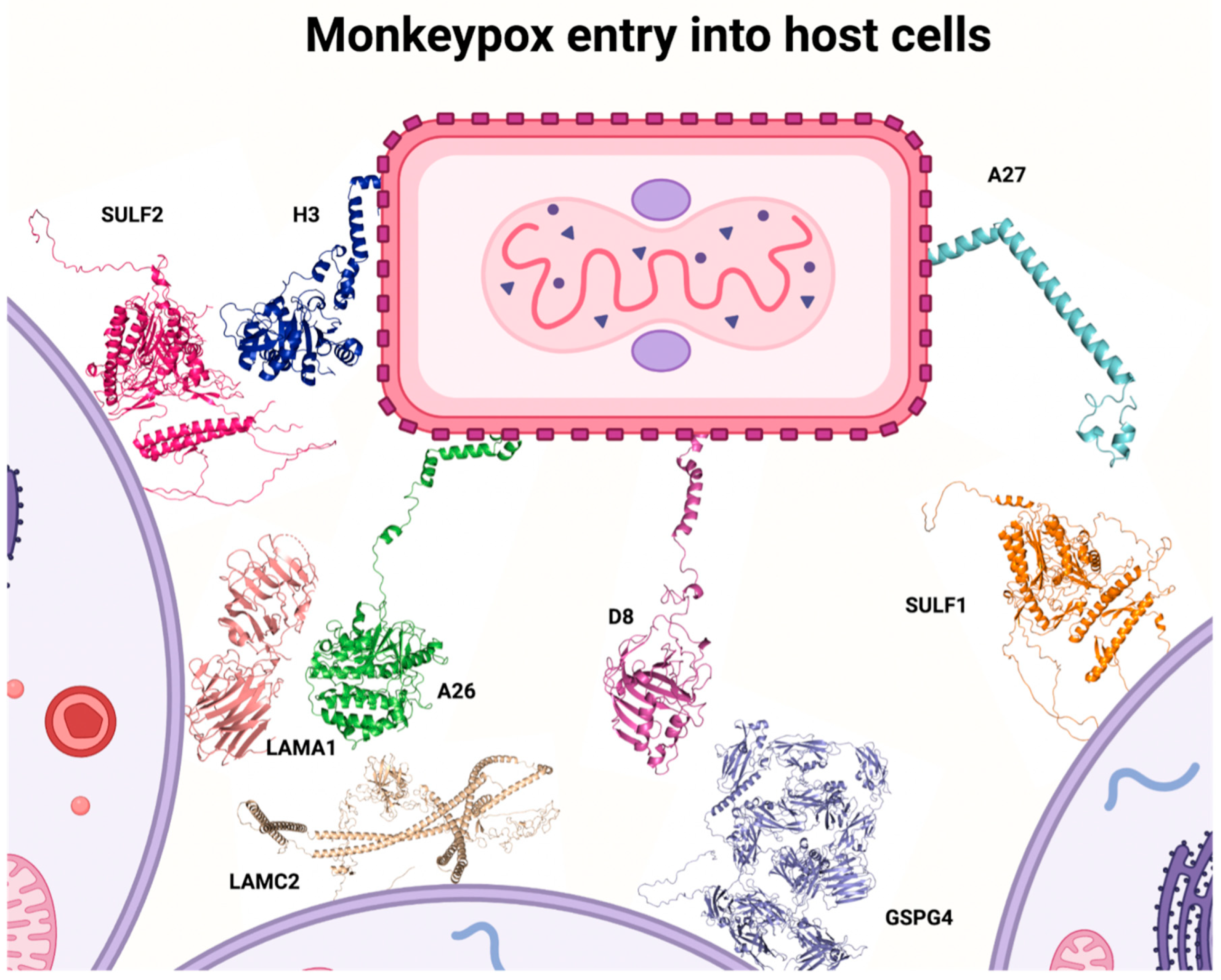
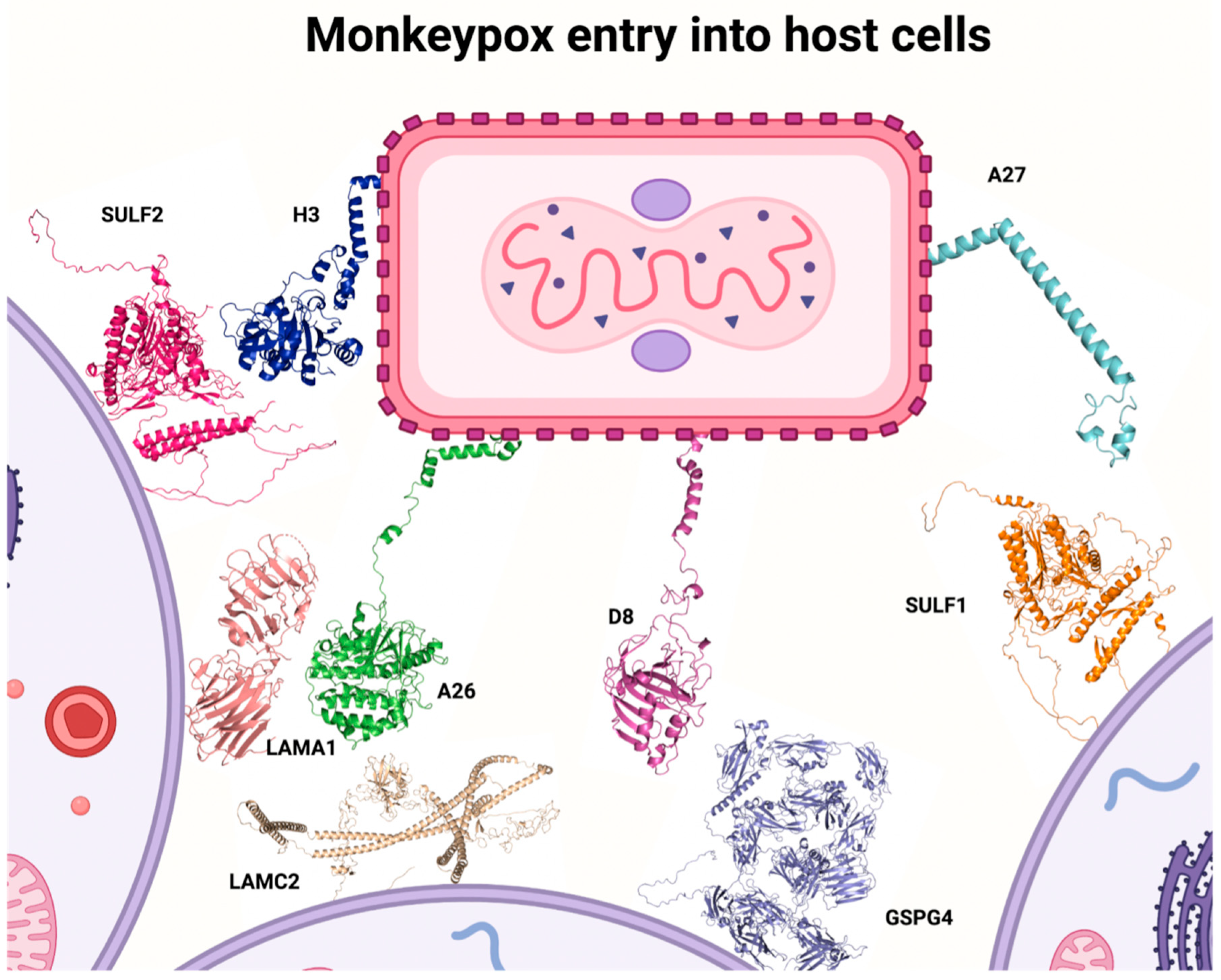
3. Viral Structure, MPXV Entry into Host Cells, and MPXV Replicative Cycle
4. Transmission
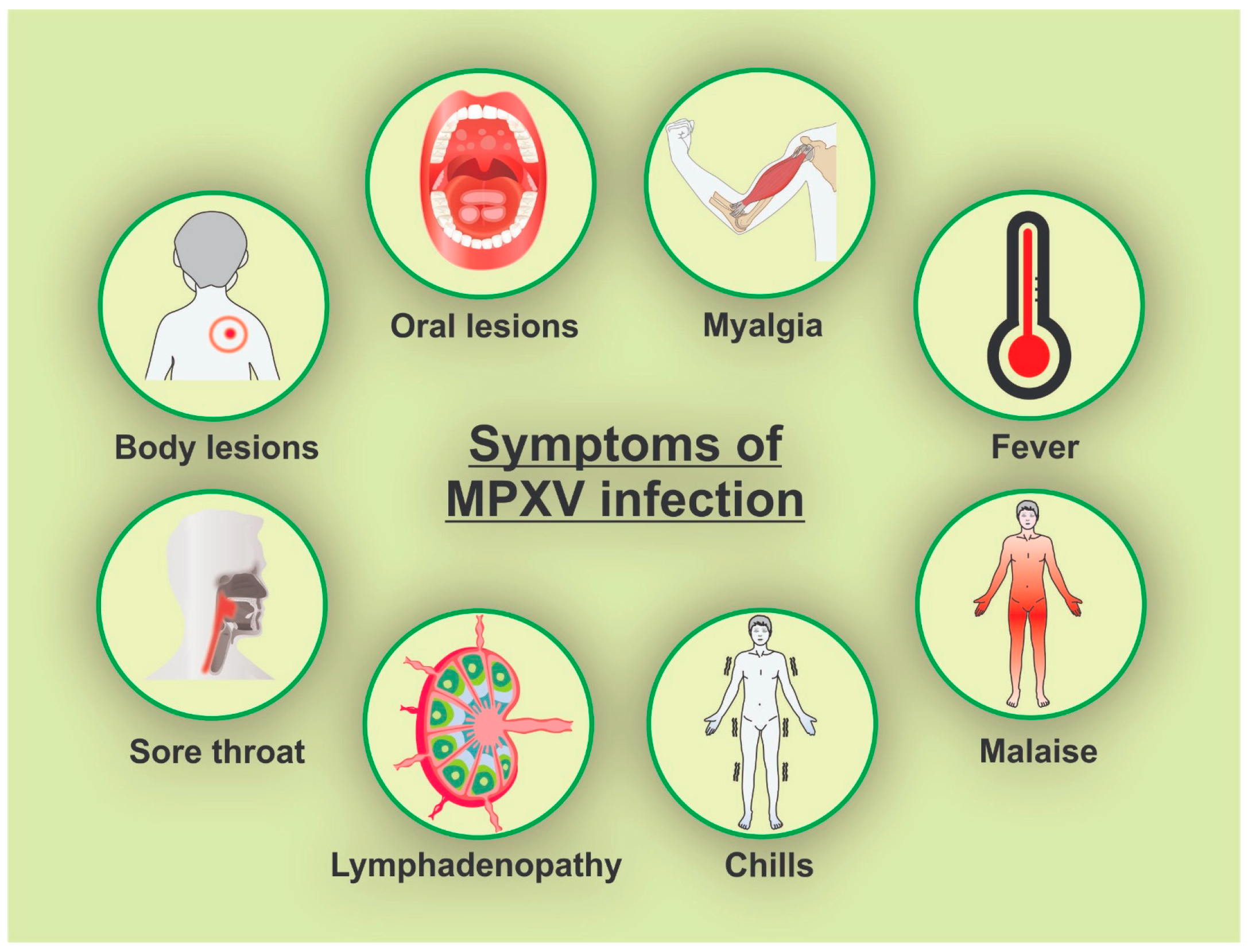
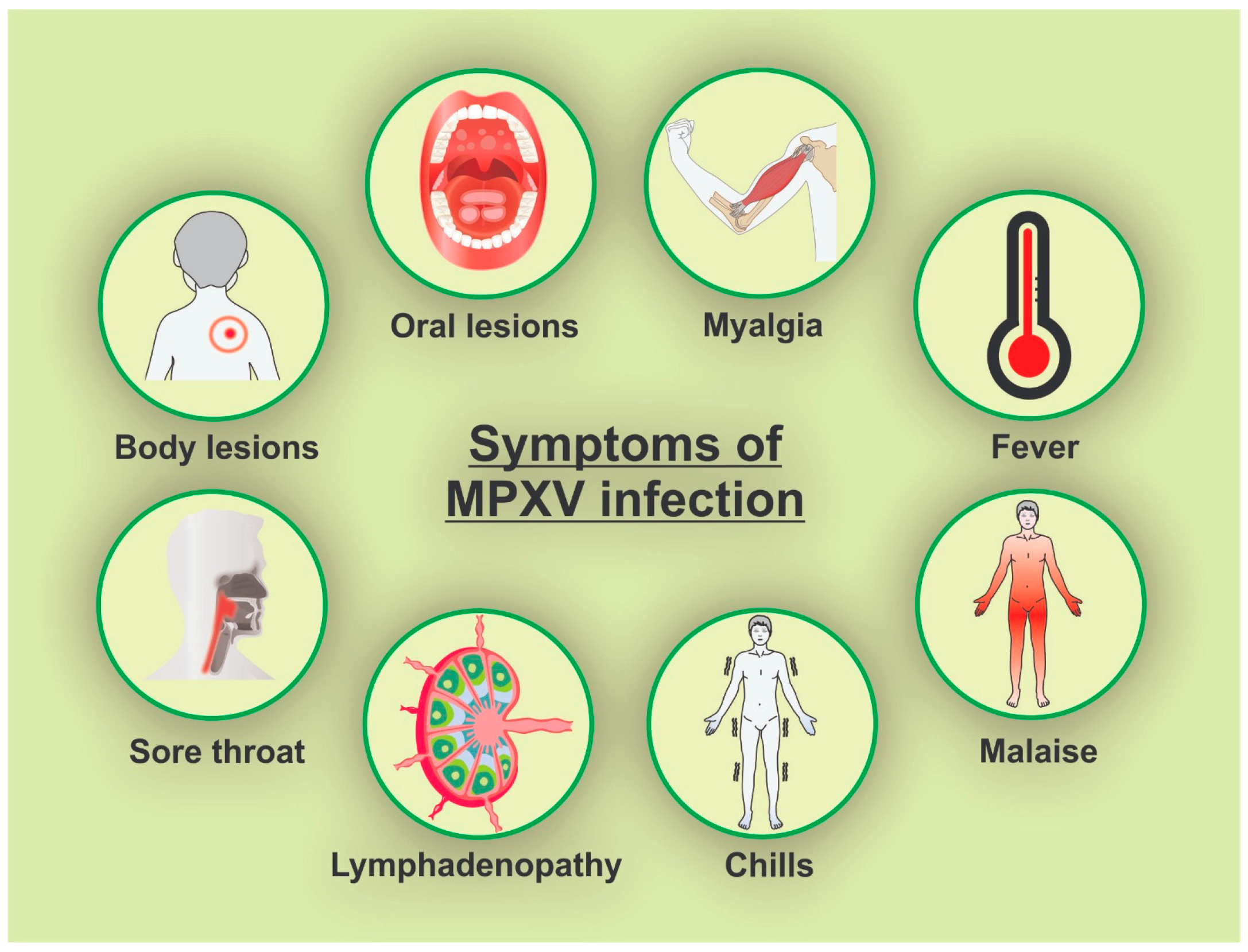
5. Oral, Perioral, and Body Symptoms
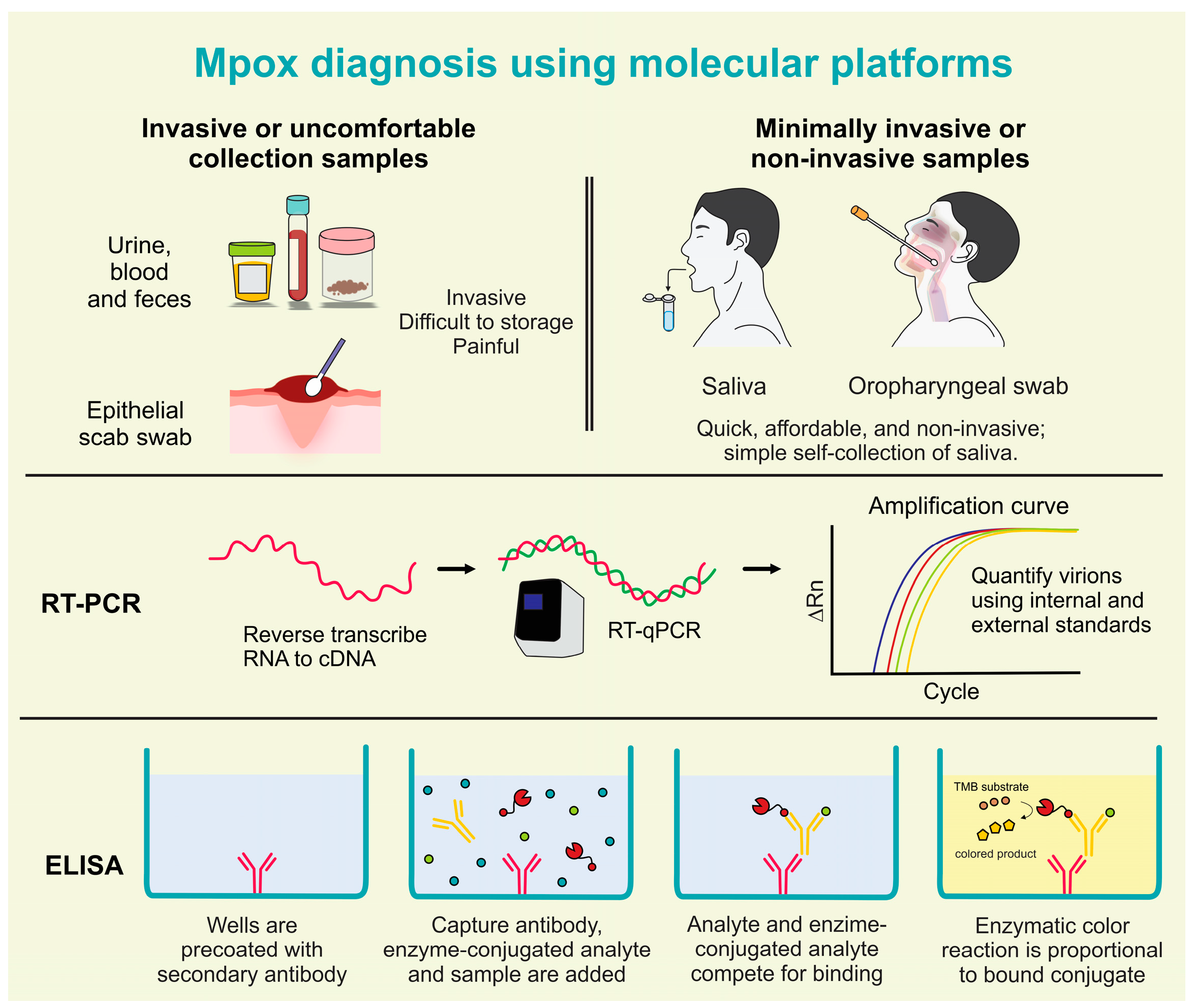
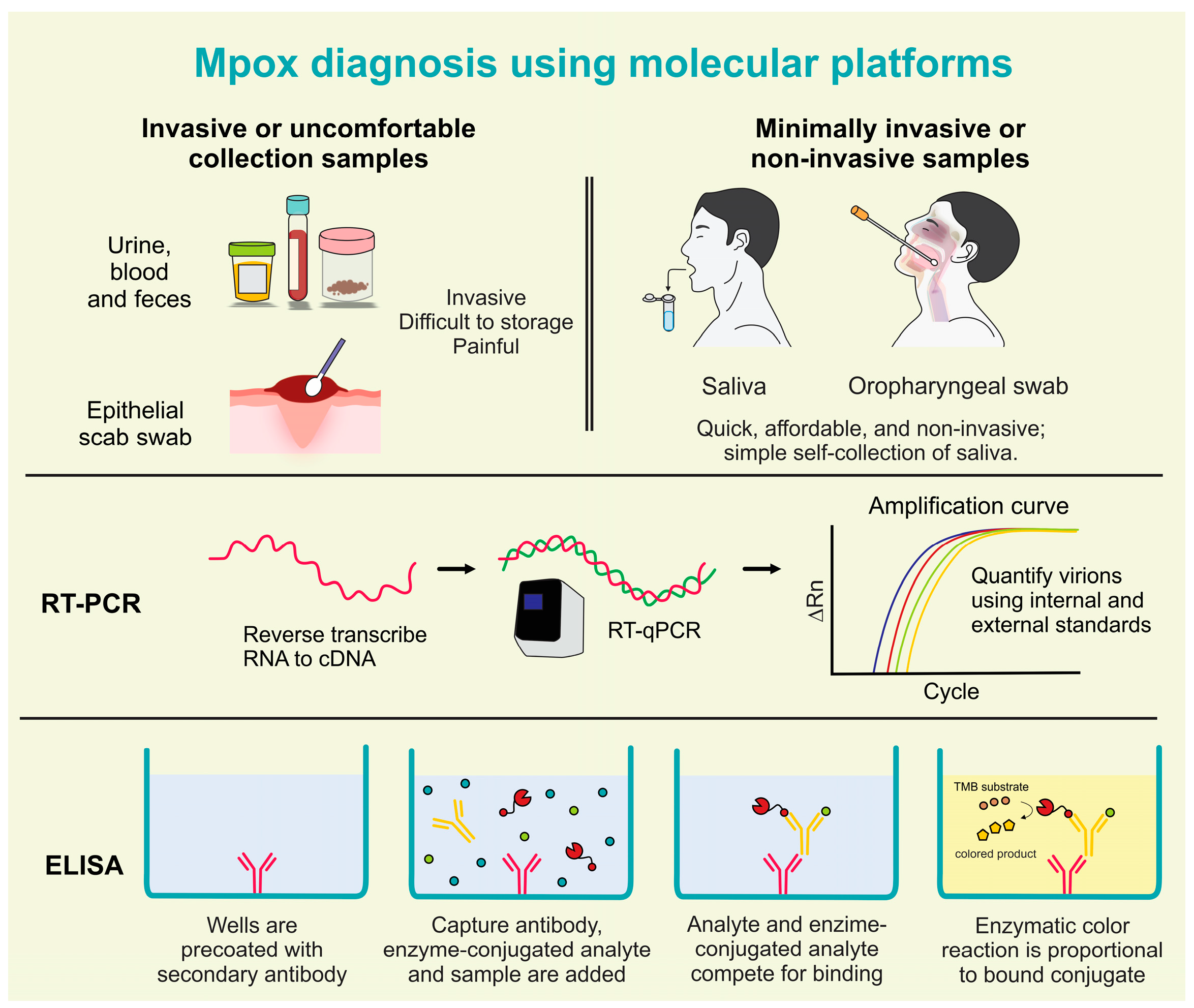
6. Mpox Diagnosis Using Molecular Platforms
7. Mpox Salivary Diagnostics and Omics Perspectives on Mpox Research
8. Measures to Dentists and Frontline Healthcare Workers
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Recommends New Name for Monkeypox Disease [Internet]; World Health Organization (WHO): Geneva, Switzerland, 2022; Available online: https://www.who.int/news/item/28-11-2022-who-recommends-new-name-for-monkeypox-disease (accessed on 31 July 2023).
- Chauhan, R.P.; Fogel, R.; Limson, J. Overview of Diagnostic Methods, Disease Prevalence and Transmission of Mpox (Formerly Monkeypox) in Humans and Animal Reservoirs. Microorganisms 2023, 11, 1186. [Google Scholar] [CrossRef] [PubMed]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A Human Infection Caused by Monkeypox Virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593. [Google Scholar] [PubMed]
- Srivastava, G.; Srivastava, G. Human Monkeypox Disease. Clin. Dermatol. 2022, 40, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Rimoin, A.W.; Mulembakani, P.M.; Johnston, S.C.; Lloyd Smith, J.O.; Kisalu, N.K.; Kinkela, T.L.; Blumberg, S.; Thomassen, H.A.; Pike, B.L.; Fair, J.N.; et al. Major Increase in Human Monkeypox Incidence 30 Years after Smallpox Vaccination Campaigns Cease in the Democratic Republic of Congo. Proc. Natl. Acad. Sci. USA 2010, 107, 16262–16267. [Google Scholar] [CrossRef]
- Xiang, Y.; White, A. Monkeypox Virus Emerges from the Shadow of Its More Infamous Cousin: Family Biology Matters. Emerg. Microbes Infect. 2022, 11, 1768–1777. [Google Scholar] [CrossRef]
- Guarner, J.; Johnson, B.J.; Paddock, C.D.; Shieh, W.J.; Goldsmith, C.S.; Reynolds, M.G.; Damon, I.K.; Regnery, R.L.; Zaki, S.R.; Greer, P.; et al. Monkeypox Transmission and Pathogenesis in Prairie Dogs. Emerg. Infect. Dis. 2004, 10, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Hobson, G.; Adamson, J.; Adler, H.; Firth, R.; Gould, S.; Houlihan, C.; Johnson, C.; Porter, D.; Rampling, T.; Ratcliffe, L.; et al. Family Cluster of Three Cases of Monkeypox Imported from Nigeria to the United Kingdom, May 2021. Eur. Surveill. 2021, 26, 2100745. [Google Scholar] [CrossRef]
- Mathieu, E.; Spooner, F.; Dattani, S.; Ritchie, H.; Roser, M. Mpox (Monkeypox) [Internet]. 2023. Available online: https://ourworldindata.org/monkeypox (accessed on 31 July 2023).
- Haider, N.; Guitian, J.; Simons, D.; Asogun, D.; Ansumana, R.; Honeyborne, I.; Velavan, T.P.; Ntoumi, F.; Valdoleiros, S.R.; Petersen, E.; et al. Increased Outbreaks of Monkeypox Highlight Gaps in Actual Disease Burden in Sub-Saharan Africa and in Animal Reservoirs. Int. J. Infect. Dis. 2022, 122, 107–111. [Google Scholar] [CrossRef]
- World Health Organization. Multi-Country Outbreak of Mpox, External Situation Report #27—14 August 2023 [Internet]. 2023. Available online: https://www.who.int/publications/m/item/multi-country-outbreak-of-mpox--external-situation-report--26---14-july-2023 (accessed on 15 August 2023).
- World Health Organization. Monkeypox: Experts Give Virus Variants New Names [Internet]. 2022. Available online: https://www.who.int/news/item/12-08-2022-monkeypox--experts-give-virus-variants-new-names (accessed on 14 October 2022).
- Isidro, J.; Borges, V.; Pinto, M.; Sobral, D.; Santos, J.D.; Nunes, A.; Mixão, V.; Ferreira, R.; Santos, D.; Duarte, S.; et al. Phylogenomic Characterization and Signs of Microevolution in the 2022 Multi-Country Outbreak of Monkeypox Virus. Nat. Med. 2022, 28, 1569–1572. [Google Scholar] [CrossRef]
- Wilson, M.E.; Hughes, J.M.; McCollum, A.M.; Damon, I.K. Human Monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar]
- Heskin, J.; Belfield, A.; Milne, C.; Brown, N.; Walters, Y.; Scott, C.; Bracchi, M.; Moore, L.S.; Mughal, N.; Rampling, T.; et al. Transmission of Monkeypox Virus through Sexual Contact—A Novel Route of Infection. J. Infect. 2022, 85, 334–363. [Google Scholar] [CrossRef]
- Lim, C.K.; Roberts, J.; Moso, M.; Liew, K.C.; Taouk, M.L.; Williams, E.; Tran, T.; Steinig, E.; Caly, L.; Williamson, D.A. Mpox Diagnostics: Review of Current and Emerging Technologies. J. Med. Virol. 2023, 95, e28429. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Saavedra, B.; Montes-Madariaga, E.S.; Cabanillas-Ramirez, C.; Alva, N.; Ricardo-Martínez, A.; León-Figueroa, D.A.; Barboza, J.J.; Mohanty, A.; Padhi, B.K.; Sah, R. Epidemiologic Situation of HIV and Monkeypox Coinfection: A Systematic Review. Vaccines 2023, 11, 246. [Google Scholar] [CrossRef] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The Changing Epidemiology of Human Monkeypox-A Potential Threat? A Systematic Review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- Likos, A.M.; Sammons, S.A.; Olson, V.A.; Frace, A.M.; Li, Y.; Olsen-Rasmussen, M.; Davidson, W.; Galloway, R.; Khristova, M.L.; Reynolds, M.G.; et al. A Tale of Two Clades: Monkeypox Viruses. J. Gen. Virol. 2005, 86, 2661–2672. [Google Scholar] [CrossRef]
- Pan, D.; Nazareth, J.; Sze, S.; Martin, C.A.; Decker, J.; Fletcher, E.; Hollingsworth, T.D.; Barer, M.R.; Pareek, M.; Tang, J.W. Transmission of Monkeypox/Mpox Virus: A Narrative Review of Environmental, Viral, Host, and Population Factors in Relation to the 2022 International Outbreak. J. Med. Virol. 2023, 95, e28534. [Google Scholar] [CrossRef]
- Manes, N.P.; Estep, R.D.; Mottaz, H.M.; Moore, R.J.; Clauss, T.R.W.; Monroe, M.E.; Du, X.; Adkins, J.N.; Wong, S.W.; Smith, R.D. Comparative Proteomics of Human Monkeypox and Vaccinia Intracellular Mature and Extracellular Enveloped Virions. J. Proteome Res. 2008, 7, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Meng, X.; Yan, B.; Crotty, S.; Deng, J.; Xiang, Y. An Epitope Conserved in Orthopoxvirus A13 Envelope Protein Is the Target of Neutralizing and Protective Antibodies. Virology 2011, 418, 67–73. [Google Scholar] [CrossRef]
- Moss, B. Poxvirus Cell Entry: How Many Proteins Does It Take? Viruses 2012, 4, 688–707. [Google Scholar] [CrossRef]
- Senkevich, T.G.; Yutin, N.; Wolf, Y.I.; Koonin, E.V.; Moss, B. Ancient Gene Capture and Recent Gene Loss Shape the Evolution of Orthopoxvirus-Host Interaction Genes. mBio 2021, 12, e0149521. [Google Scholar] [CrossRef]
- Davies, D.H.; Molina, D.M.; Wrammert, J.; Miller, J.; Hirst, S.; Mu, Y.; Pablo, J.; Unal, B.; Nakajima-Sasaki, R.; Liang, X.; et al. Proteome-Wide Analysis of the Serological Response to Vaccinia and Smallpox. Proteomics 2007, 7, 1678–1686. [Google Scholar] [CrossRef]
- Gilchuk, I.; Gilchuk, P.; Sapparapu, G.; Lampley, R.; Singh, V.; Kose, N.; Blum, D.L.; Hughes, L.J.; Satheshkumar, P.S.; Townsend, M.B.; et al. Cross-Neutralizing and Protective Human Antibody Specificities to Poxvirus Infections. Cell 2016, 167, 684–694.e9. [Google Scholar] [CrossRef]
- Mercer, J.; Snijder, B.; Sacher, R.; Burkard, C.; Bleck, C.K.E.; Stahlberg, H.; Pelkmans, L.; Helenius, A. RNAi Screening Reveals Proteasome- and Cullin3-Dependent Stages in Vaccinia Virus Infection. Cell Rep. 2012, 2, 1036–1047. [Google Scholar] [CrossRef]
- Uhlén, M.; Fagerberg, L.; Hallström, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, Å.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Proteomics. Tissue-Based Map of the Human Proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef]
- Bastian, F.B.; Roux, J.; Niknejad, A.; Comte, A.; Fonseca Costa, S.S.; de Farias, T.M.; Moretti, S.; Parmentier, G.; de Laval, V.R.; Rosikiewicz, M.; et al. The Bgee Suite: Integrated Curated Expression Atlas and Comparative Transcriptomics in Animals. Nucleic Acids Res. 2021, 49, D831–D847. [Google Scholar] [CrossRef] [PubMed]
- Pokorny, L.; Burden, J.J.; Albrecht, D.; Bamford, R.; Leigh, K.E.; Sridhar, P.; Knowles, T.J.; Modis, Y.; Mercer, J. The Vaccinia Virus Chondroitin Sulfate Binding Protein Drives Host Membrane Curvature to Facilitate Fusion. bioRxiv 2022, preprint. [Google Scholar] [CrossRef]
- Barron, M.; Rohde, R.E. Monkeypox: What We Do and Don’t Know about Recent Outbreaks [Internet]. 2022. Available online: https://asm.org/Articles/2022/May/Monkeypox-What-We-Do-and-Don-t-Know-About-Recent-O (accessed on 14 October 2022).
- McFadden, G. Poxvirus Tropism. Nat. Rev. Microbiol. 2005, 3, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of High-Consequence Pathogens and Pathology (DHCPP). How It Spreads [Internet]. 2022. Available online: https://www.cdc.gov/poxvirus/monkeypox/if-sick/transmission.html (accessed on 14 October 2022).
- Kozlov, M. Monkeypox Goes Global: Why Scientists Are on Alert. Nature 2022, 606, 15–16. [Google Scholar] [CrossRef]
- Peiro-Mestres, A.; Fuertes, I.; Camprubi-Ferrer, D.; Marcos, M.A.; Vilella, A.; Navarro, M.; Rodriguez-Elena, L.; Riera, J.; Catala, A.; Martinez, M.J.; et al. Frequent Detection of Monkeypox Virus DNA in Saliva, Semen, and Other Clinical Samples from 12 Patients, Barcelona, Spain, May to June 2022. Eur. Surveill. 2022, 27, 2200503. [Google Scholar] [CrossRef]
- World Health Organization. Monkeypox [Internet]. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 14 October 2022).
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Reddy, N.G. Monkeypox Infection: Relevance of Oral Health Screening. Oral Dis. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Català, A.; Clavo-Escribano, P.; Riera-Monroig, J.; Martín-Ezquerra, G.; Fernandez-Gonzalez, P.; Revelles-Peñas, L.; Simon-Gozalbo, A.; Rodríguez-Cuadrado, F.J.; Castells, V.G.; de la Torre Gomar, F.J.; et al. Monkeypox Outbreak in Spain: Clinical and Epidemiological Findings in a Prospective Cross-Sectional Study of 185 Cases. Br. J. Dermatol. 2022, 187, 765–772. [Google Scholar] [CrossRef]
- Weaver, J.R.; Isaacs, S.N. Monkeypox Virus and Insights into Its Immunomodulatory Proteins. Immunol. Rev. 2008, 225, 96–113. [Google Scholar] [CrossRef]
- Chittajallu, V.; Vozzo, C.; Friedman, K.; Glessing, B.; Nguyen, V. Odynophagia Secondary to Mpox-Associated Esophageal Ulceration. Am. J. Gastroenterol. 2022, 118, 774. [Google Scholar] [CrossRef] [PubMed]
- Lane, H.C.; Fauci, A.S. Monkeypox—Past as Prologue. N. Engl. J. Med. 2022, 387, 749–750. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Da Silva Fontoura, D.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical Features and Novel Presentations of Human Monkeypox in a Central London Centre during the 2022 Outbreak: Descriptive Case Series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of High-Consequence Pathogens and Pathology (DHCPP). Monkeypox [Internet]. 2022. Available online: https://www.cdc.gov/poxvirus/mpox/index.html (accessed on 14 October 2022).
- Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of High-Consequence Pathogens and Pathology (DHCPP). Clinical Recognition [Internet]. 2022. Available online: https://www.cdc.gov/poxvirus/mpox/clinicians/clinical-recognition.html (accessed on 14 October 2022).
- Eichner, M.; Dietz, K. Transmission Potential of Smallpox: Estimates Based on Detailed Data from an Outbreak. Am. J. Epidemiol. 2003, 158, 110–117. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Yorita, K.L.; Kuehnert, M.J.; Davidson, W.B.; Huhn, G.D.; Holman, R.C.; Damon, I.K. Clinical Manifestations of Human Monkeypox Influenced by Route of Infection. J. Infect. Dis. 2006, 194, 773–780. [Google Scholar] [CrossRef]
- Miura, F.; van Ewijk, C.E.; Backer, J.A.; Xiridou, M.; Franz, E.; de Coul, E.O.; Brandwagt, D.; van Cleef, B.; van Rijckevorsel, G.; Swaan, C.; et al. Estimated Incubation Period for Monkeypox Cases Confirmed in the Netherlands, May 2022. Eur. Surveill. 2022, 27, 2200448. [Google Scholar] [CrossRef]
- Karthikeyan Balasubramanian, S.; Vinayachandran, D. Letter to the Editor Oral Lesions in Monkeypox—A Definite Consideration! J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 595. [Google Scholar] [CrossRef] [PubMed]
- Sookaromdee, P.; Wiwanitkit, V. Letter to the Editor Mouth Sores and Monkeypox: A Consideration. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 593–594. [Google Scholar] [CrossRef] [PubMed]
- Marennikova, S.S.; Seluhina, E.M.; Mal’ceva, N.N.; Cimiskjan, K.L.; Macevic, G.R. Isolation and Properties of the Causal Agent of a New Variola-like Disease (Monkeypox) in Man. Bull. World Health Organ. 1972, 46, 599. [Google Scholar] [PubMed]
- Nörz, D.; Brehm, T.T.; Tang, H.T.; Grewe, I.; Hermanussen, L.; Matthews, H.; Pestel, J.; Degen, O.; Günther, T.; Grundhoff, A.; et al. Clinical Characteristics and Comparison of Longitudinal QPCR Results from Different Specimen Types in a Cohort of Ambulatory and Hospitalized Patients Infected with Monkeypox Virus. J. Clin. Virol. 2022, 155, 105254. [Google Scholar] [CrossRef] [PubMed]
- Huggett, J.F.; French, D.; O’Sullivan, D.M.; Moran-Gilad, J.; Zumla, A. Monkeypox: Another Test for PCR. Eur. Surveill. 2022, 27, 2200497. [Google Scholar] [CrossRef]
- Huo, S.; Chen, Y.; Lu, R.; Zhang, Z.; Zhang, G.; Zhao, L.; Deng, Y.; Wu, C.; Tan, W. Development of Two Multiplex Real-Time PCR Assays for Simultaneous Detection and Differentiation of Monkeypox Virus IIa, IIb, and I Clades and the B.1 Lineage. Biosaf. Health 2022, 4, 392–398. [Google Scholar] [CrossRef]
- Yefet, R.; Friedel, N.; Tamir, H.; Polonsky, K.; Mor, M.; Cherry-Mimran, L.; Taleb, E.; Hagin, D.; Sprecher, E.; Israely, T.; et al. Monkeypox Infection Elicits Strong Antibody and B Cell Response against A35R and H3L Antigens. iScience 2023, 26, 105957. [Google Scholar] [CrossRef]
- Nonaka, T.; Wong, D.T.W. Saliva Diagnostics: Salivaomics, Saliva Exosomics, and Saliva Liquid Biopsy. J. Am. Dent. Assoc. 2023, 154, 696–704. [Google Scholar] [CrossRef]
- Coppens, J.; Vanroye, F.; Brosius, I.; Liesenborghs, L.; van Henten, S.; Vanbaelen, T.; Bracke, S.; Berens-Riha, N.; De Baetselier, I.; Kenyon, C.; et al. Alternative Sampling Specimens for the Molecular Detection of Mpox (Formerly Monkeypox) Virus. J. Clin. Virol. 2023, 159, 105372. [Google Scholar] [CrossRef]
- Tan, D.H.S.; Jaeranny, S.; Li, M.; Sukhdeo, S.S.; Monge, J.C.; Callejas, M.F.; Hasso, M.; Fattouh, R.; Lalonde, S.D.; Lam, J.; et al. Atypical Clinical Presentation of Monkeypox Complicated by Myopericarditis. Open Forum Infect. Dis. 2022, 9, ofac394. [Google Scholar] [CrossRef]
- Rodrigues, R.P.C.B.; Aguiar, E.M.G.; Cardoso-Sousa, L.; Caixeta, D.C.; Guedes, C.C.F.V.; Siqueira, W.L.; Maia, Y.C.P.; Cardoso, S.V.; Sabino-Silva, R. Differential Molecular Signature of Human Saliva Using ATR-FTIR Spectroscopy for Chronic Kidney Disease Diagnosis. Braz. Dent. J. 2019, 30, 437–445. [Google Scholar] [CrossRef]
- Yang, X.; Tang, G.; Shi, L.; Xu, F. Transmission and Detection of Monkeypox Virus in Saliva: Implications for Dental Practice and Public Health. J. Dent. Sci. 2023, 18, 913–915. [Google Scholar] [CrossRef] [PubMed]
- Beeson, A.; Styczynski, A.; Hutson, C.L.; Whitehill, F.; Angelo, K.M.; Minhaj, F.S.; Morgan, C.; Ciampaglio, K.; Reynolds, M.G.; McCollum, A.M.; et al. Mpox Respiratory Transmission: The State of the Evidence. Lancet Microbe 2023, 4, e277–e283. [Google Scholar] [CrossRef] [PubMed]
- Caixeta, D.C.; Lima, C.; Xu, Y.; Guevara-Vega, M.; Espindola, F.S.; Goodacre, R.; Zezell, D.M.; Sabino-Silva, R. Monitoring Glucose Levels in Urine Using FTIR Spectroscopy Combined with Univariate and Multivariate Statistical Methods. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2022, 290, 122259. [Google Scholar] [CrossRef]
- Pettke, A.; Filén, F.; Widgren, K.; Jacks, A.; Glans, H.; Andreasson, S.; Muradrasoli, S.; Helgesson, S.; Hauzenberger, E.; Karlberg, M.L.; et al. Ten-Week Follow-Up of Monkeypox Case-Patient, Sweden, 2022. Emerg. Infect. Dis. 2022, 28, 2074–2077. [Google Scholar] [CrossRef]
- Allan-Blitz, L.; Carragher, K.; Sukhija-Cohen, A.; Ritchie, P.; Scott, H.; Li, H.; Klausner, J.D. Laboratory Validation and Clinical Performance of a Saliva-based Test for Monkeypox Virus. J. Med. Virol. 2023, 95, e28191. [Google Scholar] [CrossRef]
- Hernaez, B.; Muñoz-Gómez, A.; Sanchiz, A.; Orviz, E.; Valls-Carbo, A.; Sagastagoitia, I.; Ayerdi, O.; Martín, R.; Puerta, T.; Vera, M.; et al. Monitoring Monkeypox Virus in Saliva and Air Samples in Spain: A Cross-Sectional Study. Lancet Microbe 2023, 4, e21–e28. [Google Scholar] [CrossRef] [PubMed]
- Ghate, S.D.; Suravajhala, P.; Patil, P.; Vangala, R.K.; Shetty, P.; Rao, R.S.P. Molecular Detection of Monkeypox and Related Viruses: Challenges and Opportunities. Virus Genes 2023, 1, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.; Smith, B.; David, W.T. Saliva Ontology: An Ontology-Based Framework for a Salivaomics Knowledge Base. BMC Bioinf. 2010, 11, 302. [Google Scholar] [CrossRef]
- Yan, W.; Apweiler, R.; Balgley, B.M.; Boontheung, P.; Bundy, J.L.; Cargile, B.J.; Cole, S.; Fang, X.; Gonzalez-Begne, M.; Griffin, T.J.; et al. Systematic Comparison of the Human Saliva and Plasma Proteomes. Proteom. Clin. Appl. 2009, 3, 116–134. [Google Scholar] [CrossRef]
- Dawes, C.; Wong, D.T.W. Role of Saliva and Salivary Diagnostics in the Advancement of Oral Health. J. Dent. Res. 2019, 98, 133–141. [Google Scholar] [CrossRef]
- Barzegar Behrooz, A.; Latifi-Navid, H.; da Silva Rosa, S.C.; Swiat, M.; Wiechec, E.; Vitorino, C.; Vitorino, R.; Jamalpoor, Z.; Ghavami, S. Integrating Multi-Omics Analysis for Enhanced Diagnosis and Treatment of Glioblastoma: A Comprehensive Data-Driven Approach. Cancers 2023, 15, 3158. [Google Scholar] [CrossRef] [PubMed]
- Lozano, C.; Grenga, L.; Gallais, F.; Miotello, G.; Bellanger, L.; Armengaud, J. Mass Spectrometry Detection of Monkeypox Virus: Comprehensive Coverage for Ranking the Most Responsive Peptide Markers. Proteomics 2023, 23, e2200253. [Google Scholar] [CrossRef]
- Wang, Z.; Tober-Lau, P.; Farztdinov, V.; Lemke, O.; Schwecke, T.; Steinbrecher, S.; Muenzner, J.; Kriedemann, H.; Sander, L.E.; Hartl, J.; et al. The Human Host Response to Monkeypox Infection: A Proteomic Case Series Study. EMBO Mol. Med. 2022, 14, e16643. [Google Scholar] [CrossRef] [PubMed]
- Pay, J.B.; Shaw, A.M. Towards Salivary C-Reactive Protein as a Viable Biomarker of Systemic Inflammation. Clin. Biochem. 2019, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guedes, S.F.F.; Neves, B.G.; Bezerra, D.S.; Souza, G.H.M.F.; Lima-Neto, A.B.M.; Guedes, M.I.F.; Duarte, S.; Rodrigues, L.K.A. Saliva Proteomics from Children with Caries at Different Severity Stages. Oral Dis. 2020, 26, 1219–1229. [Google Scholar] [CrossRef]
- Choi, S.; Baik, J.E.; Jeon, J.H.; Cho, K.; Seo, D.G.; Kum, K.Y.; Yun, C.H.; Han, S.H. Identification of Porphyromonas Gingivalis Lipopolysaccharide-Binding Proteins in Human Saliva. Mol. Immunol. 2011, 48, 2207–2213. [Google Scholar] [CrossRef]
- Tintor, G.; Jukić, M.; Šupe-Domić, D.; Jerončić, A.; Pogorelić, Z. Diagnostic Accuracy of Leucine-Rich α-2-Glycoprotein 1 as a Non-Invasive Salivary Biomarker in Pediatric Appendicitis. Int. J. Mol. Sci. 2023, 24, 6043. [Google Scholar] [CrossRef] [PubMed]
- Canakis, A.; Kim, R.E.; Sinha, P.; Raufman, J.P. Addressing the Risk of Monkeypox Exposure during Gastrointestinal Endoscopy. Ann. Gastroenterol. 2023, 36, 1–5. [Google Scholar] [CrossRef]
- Yinka-Ogunleye, A.; Aruna, O.; Dalhat, M.; Ogoina, D.; McCollum, A.; Disu, Y.; Mamadu, I.; Akinpelu, A.; Ahmad, A.; Burga, J.; et al. Outbreak of Human Monkeypox in Nigeria in 2017-18: A Clinical and Epidemiological Report. Lancet Infect. Dis. 2019, 19, 872–879. [Google Scholar] [CrossRef]
- Caixeta, D.C.; Paranhos, L.R.; Blumenberg, C.; Garcia-Júnior, M.A.; Guevara-Vega, M.; Taveira, E.B.; Nunes, M.A.C.; Cunha, T.M.; Jardim, A.C.G.; Flores-Mir, C.; et al. Salivary SARS-CoV-2 RNA for Diagnosis of COVID-19 Patients: A Systematic Revisew and Meta-Analysis of Diagnostic Accuracy. Jpn. Dent. Sci. Rev. 2023, 59, 219–238. [Google Scholar] [CrossRef]
- Ogoina, D.; Iroezindu, M.; James, H.I.; Oladokun, R.; Yinka-Ogunleye, A.; Wakama, P.; Otike-Odibi, B.; Usman, L.M.; Obazee, E.; Aruna, O.; et al. Clinical Course and Outcome of Human Monkeypox in Nigeria. Clin. Infect. Dis. 2020, 71, E210–E214. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of High-Consequence Pathogens and Pathology (DHCPP). Infection Control [Internet]. 2022. Available online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/infection-control-healthcare.html (accessed on 14 October 2022).
- The National Health Service (NHS). Monkeypox [Internet]. 2022. Available online: https://www.england.nhs.uk/publication/monkeypox/ (accessed on 14 October 2022).

{kind=link}
{kind=link}
{kind=link}
| Receptor | Gene Name | Uberon | Anatomical Entity | Expression Score |
|---|---|---|---|---|
| Laminin (Laminin subunit alpha 1) | LAMA1 | UBERON:0001830 | Minor salivary gland | 68.59 |
| Laminin (Laminin subunit gamma 2) | LAMC2 | UBERON:0001830 | Minor salivary gland | 79.86 |
| UBERON:0007371 | Superior surface of tongue | 59.56 | ||
| Chondroitin Sulfate (Chondroitin sulfate proteoglycan 4) | CSPG4 | UBERON:0001830 | Minor salivary gland | 70.60 |
| UBERON:0007371 | Superior surface of tongue | 70.23 | ||
| Heparan sulfate (Sulfatase 1) | SULF1 | UBERON:0001830 | Minor salivary gland | 77.09 |
| UBERON:0007371 | Superior surface of tongue | 67.66 | ||
| UBERON:0011876 | Body of tongue | 66.51 | ||
| Heparan sulfate (Sulfatase 2) | SULF2 | UBERON:0001830 | Minor salivary gland | 93.40 |
| UBERON:0001723 | Tongue | 88.59 | ||
| UBERON:0011876 | Body of tongue | 88.55 | ||
| UBERON:0007371 | Superior surface of tongue | 87.51 |
| Receptor | Gene Name | Anatomical Entity | RNA Expression | Protein | |||
|---|---|---|---|---|---|---|---|
| Consensus nTPM | HPA pTPM | GTEx pTPM | FANTOM5 Scaled Tags Per Million | ||||
| Laminin (Laminin subunit alpha 1) | LAMA1 | Oral mucosa | No data | No data | No data | No data | Not detected |
| Salivary gland | 1.3 | 1.3 | 1.0 | 4.1 | Low | ||
| Tongue | 0.0 | 0.0 | No data | 0.6 | No data | ||
| Laminin (Laminin subunit gamma 2) | LAMC2 | Oral mucosa | No data | No data | No data | No data | Not detected |
| Salivary gland | 12.9 | 3.5 | 12.9 | 1.3 | Low | ||
| Tongue | 2.3 | 2.3 | No data | 6.3 | No data | ||
| Chondroitin Sulfate (Chondroitin sulfate proteoglycan 4) | CSPG4 | Oral mucosa | No data | No data | No data | No data | Low |
| Salivary gland | 4.7 | 1.9 | 4.7 | 13.0 | Medium | ||
| Tongue | 10.0 | 10.0 | No data | 34.8 | No data | ||
| Heparan sulfate (Sulfatase 1) | SULF1 | Oral mucosa | No data | No data | No data | No data | Not detected |
| Salivary gland | 4.3 | 2.4 | 4.3 | 8.8 | Not detected | ||
| Tongue | 11.2 | 11.2 | No data | 34.1 | No data | ||
| Heparan sulfate (Sulfatase 2) | SULF2 | Oral mucosa | No data | No data | No data | No data | Not detected |
| Salivary gland | 34.0 | 9.9 | 34.0 | 18.3 | High | ||
| Tongue | 22.5 | 22.5 | No data | 22.4 | No detected | ||
| Brand Assay | Molecular Target | Processing Workload Capacity | Turnaround Strategy | Features/Analytical Performance |
|---|---|---|---|---|
| John Hopkins assay | MPXV (E9L), OPXV (B6R) | High-throughput | Variable by cycle threshold | LOD (95%) 100 copies/mL, analytical sensitivity, specificity is adequate and high reproducibility, tested in skin lesion swabs |
| US CDC assay | OPXV (E9L-NVAR), MPXV (B6R) (Multiplexed) | High-throughput | Variable by cycle threshold | LOD 16 copies/mL, assessed in Routine liquid transport media evaluated for Quantstudio 6 |
| Novaplex MPX assay | MPXV | High-throughput | Variable by cycle threshold | 100% sensitivity, evaluated for BioRad CFX 96 |
| Bio-Speedy assay | MPXV (F3L) | High-throughput | Variable by cycle threshold | 94% sensitivity, evaluated for BioRad CFX 96 |
| ACON Biotech assay | MPXV (F3L) | High-throughput | Variable by cycle threshold | LOD 250 copies/mL, includes internal control, evaluated for BioRad CFX 96 |
| Altona Diagnostics assay | OPXV | High-throughput | Variable by cycle threshold | Includes internal control, evaluated for BioRad CFX 96 |
| Bioperfectus Technologies | MPXV (F3L) | High-throughput | Variable by cycle threshold | LOD 5 copies/reaction, includes internal control, evaluated for BioRad CFX 96 |
| DaAn Gene | MPXV (F3L) | High-throughput | Variable by cycle threshold | LOD 200 copies/mL, includes internal control, evaluated for BioRad CFX 96 |
| Shanghai ZJ Bio-Tech Co assay | MPXV (F3L) | High-throughput | Variable by cycle threshold | LOD 5000 copies/mL, includes internal control, evaluated for BioRad CFX 96 |
| Perkin Elmer Pkamp Monkeypox Virus RT-PCR RUO kit | MPXV (F3L) | High-throughput | Variable by cycle threshold | LOD 20 copies/reaction, includes internal control, evaluated for BioRad CFX 96 |
| Sansure Biotech Monkeypox Virus Nucleic Acid Diagnostic Kit | MPXV (F3L) | High-throughput | Variable by cycle threshold | LOD 200 copies/mL, includes internal control, evaluated for BioRad CFX 96 |
| Thermo-Fischer Taqman Monkeypox Virus Microbe Detection | MPXV (J1L) | High-throughput | Variable by cycle threshold | LOD < 10 copies/reaction, evaluated for BioRad CFX 96 |
| TIB Mobiol LightMix Modular Orthopox Virus/Monkeypox Virus | OPXV (14kDa), MPXV (J2L/J2R) | High-throughput | Variable by cycle threshold | LOD < 10 copies/reaction, evaluated for BioRad CFX 96 |
| FilmArray Sentinel Panel & FilmArray BioThreat Panel (BioFire) | OPXV | Low-throughput. | 60 min | No reagent preparation. One test each per assay. |
| BD Max | LDT | Low-throughput | 180 min | Automated extraction/amplification. Permits to run 24 samples in 3 h. |
| Roche Omni Cobas 6800/8800 (Roche) | LDT, Cobas MPXV (Multiplexed) | Intermediate-throughput | 210 min | Automated extraction/amplification. Permits to run 800 tests in 8 h |
| Alinity (Abbott Molecular) | LDT, Alinity m MPXV (Multiplexed) | Intermediate-throughput | <60 min | Automated extraction/amplification. Permits A random access, up to 300 tests in 8 h |
| Panther Fusion Open Access (Hologic) | LDT, can multiplex up to 5 targets | Intermediate-throughput | <140 min | Automated extraction/amplification. Permits random access, up to 800 tests in 8 h. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Junior, M.A.; Andrade, B.S.; Guevara-Vega, M.; de Melo, I.S.; Cunha, T.M.; Jardim, A.C.G.; Sabino-Silva, R. Oral Infection, Oral Pathology and Salivary Diagnostics of Mpox Disease: Relevance in Dentistry and OMICs Perspectives. Int. J. Mol. Sci. 2023, 24, 14362. https://doi.org/10.3390/ijms241814362
Garcia-Junior MA, Andrade BS, Guevara-Vega M, de Melo IS, Cunha TM, Jardim ACG, Sabino-Silva R. Oral Infection, Oral Pathology and Salivary Diagnostics of Mpox Disease: Relevance in Dentistry and OMICs Perspectives. International Journal of Molecular Sciences. 2023; 24(18):14362. https://doi.org/10.3390/ijms241814362
Chicago/Turabian StyleGarcia-Junior, Marcelo Augusto, Bruno Silva Andrade, Marco Guevara-Vega, Igor Santana de Melo, Thúlio M. Cunha, Ana Carolina Gomes Jardim, and Robinson Sabino-Silva. 2023. "Oral Infection, Oral Pathology and Salivary Diagnostics of Mpox Disease: Relevance in Dentistry and OMICs Perspectives" International Journal of Molecular Sciences 24, no. 18: 14362. https://doi.org/10.3390/ijms241814362
APA StyleGarcia-Junior, M. A., Andrade, B. S., Guevara-Vega, M., de Melo, I. S., Cunha, T. M., Jardim, A. C. G., & Sabino-Silva, R. (2023). Oral Infection, Oral Pathology and Salivary Diagnostics of Mpox Disease: Relevance in Dentistry and OMICs Perspectives. International Journal of Molecular Sciences, 24(18), 14362. https://doi.org/10.3390/ijms241814362