Fever Time Series Analysis Using Slope Entropy. Application to Early Unobtrusive Differential Diagnosis



Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
- Fever of more than or equal to 7 days duration.
- Individuals with an intact tympanic membrane.
- Subjects aged between 18–65 years.
2.2. Slope Entropy
- Symbol 2, if .
- Symbol 1, if and .
- Symbol 0, if .
- Symbol −1, if and .
- Symbol −2, if .
| Algorithm 1 Computing SlopEn |
| SlopEn(, m, , ) |
| (Empty list of patterns found) |
| for |
| (Empty pattern) |
| for |
| if () (Add symbol 0) |
| if () (Add symbol 1) |
| if () (Add symbol 2) |
| if () (Add symbol −1) |
| if () (Add symbol −2) |
| unique (Compute relative frequency of each pattern, #=sizeof operator) |
| log |
2.3. Performance Assessment
3. Experiments And Results
3.1. Input Parameter Configuration
3.2. Classification Performance
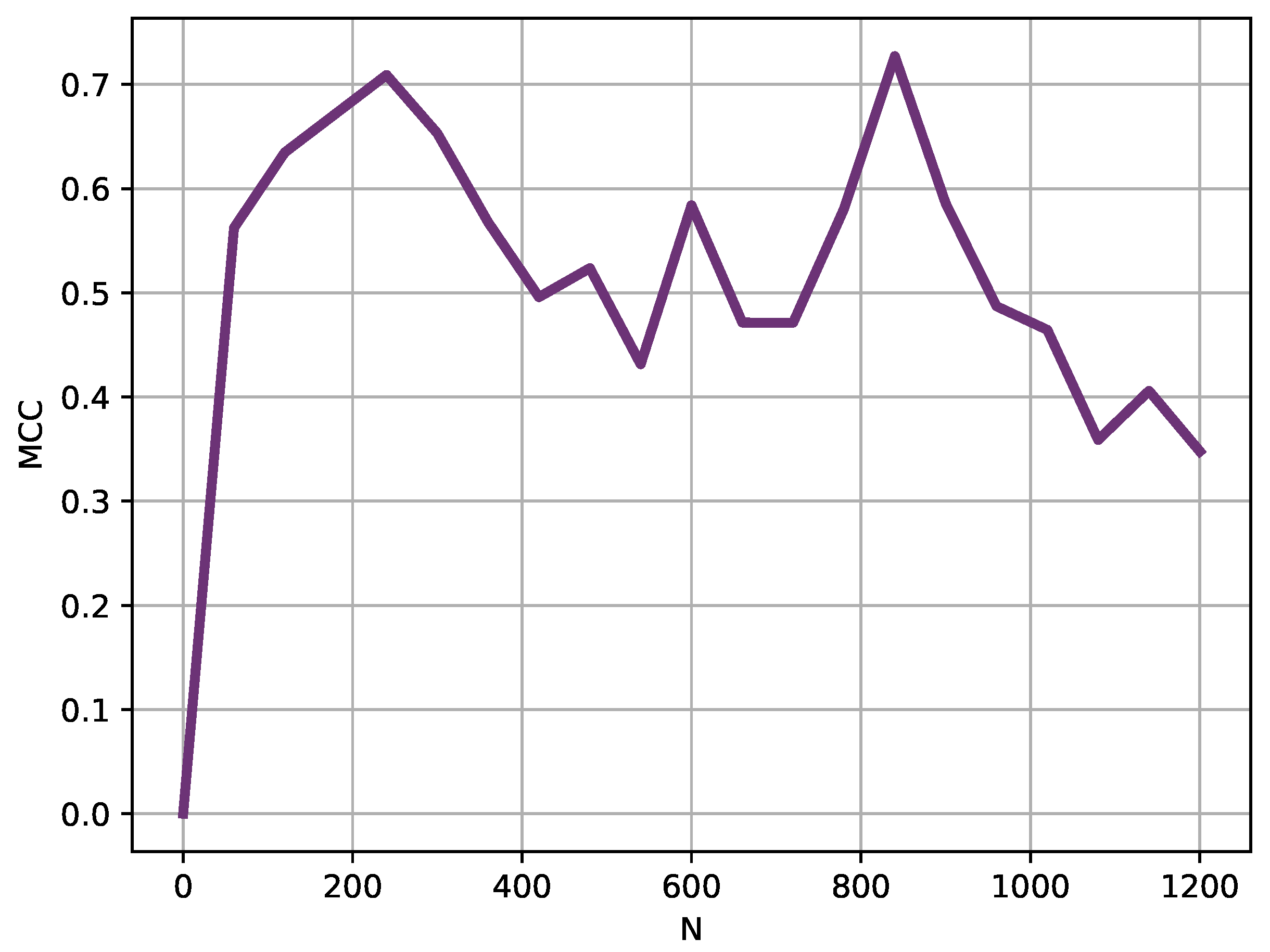
3.3. Window Analysis
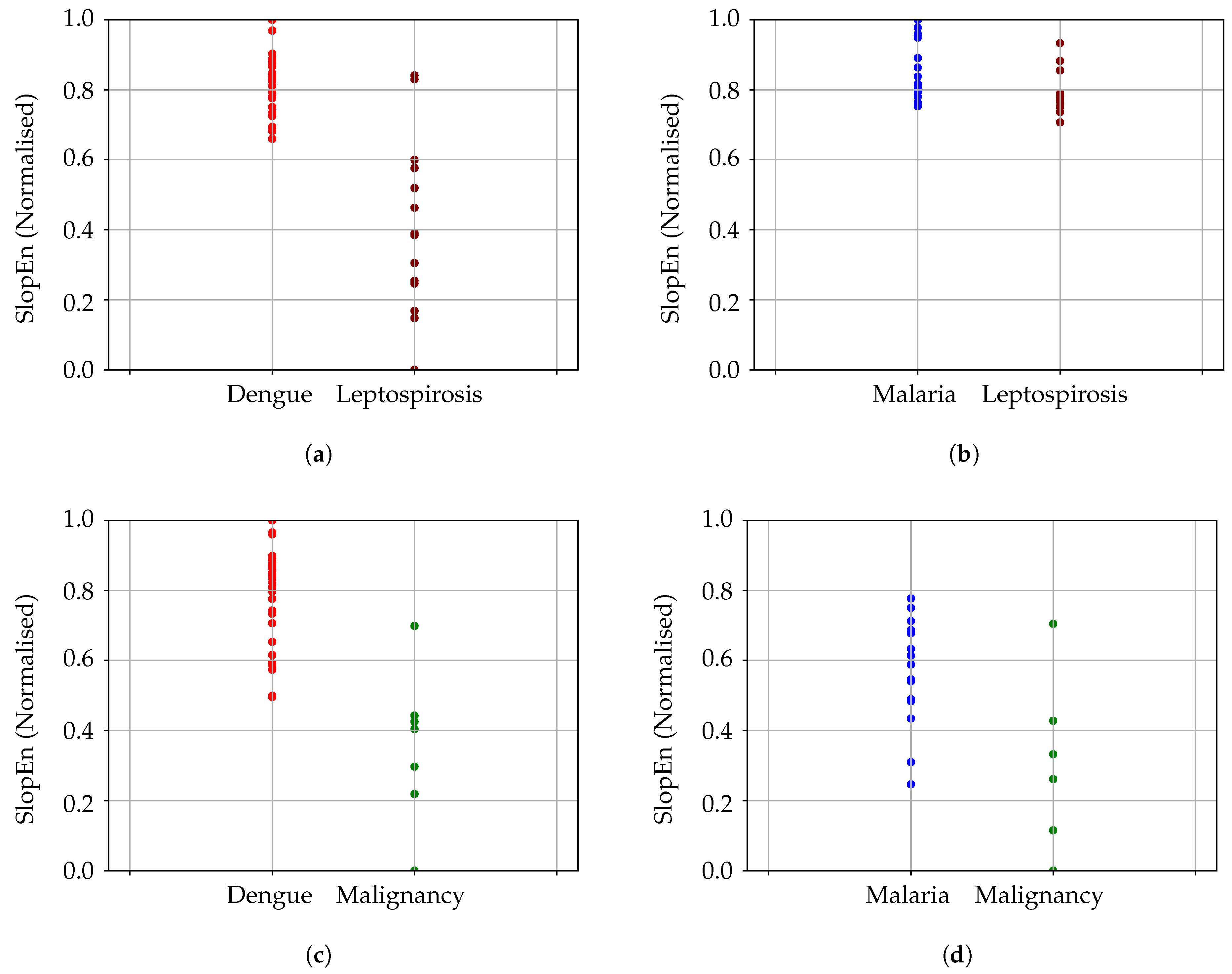
3.4. Generalization Analysis
3.5. Results Summary
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Varela-Entrecanales, M.; Cuesta-Frau, D.; Madrid, J.A.; Churruca, J.; Miró-Martínez, P.; Ruiz, R.; Martinez, C. Holter monitoring of central and peripheral temperature: Possible uses and feasibility study in outpatient settings. J. Clin. Monit. Comput. 2009, 23, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Frau, D.; Varela-Entrecanales, M.; Valor-Perez, R.; Vargas, B. Development of a Novel Scheme for Long-Term Body Temperature Monitoring: A Review of Benefits and Applications. J. Med. Syst. 2015, 39, 39. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jordán-Núnez, J.; Miró-Martínez, P.; Vargas, B.; Varela-Entrecanales, M.; Cuesta-Frau, D. Statistical models for fever forecasting based on advanced body temperature monitoring. J. Crit. Care 2017, 37, 136–140. [Google Scholar] [CrossRef]
- Papaioannou, V.E.; Chouvarda, I.G.; Maglaveras, N.K.; Baltopoulos, G.I.; Pneumatikos, I.A. Temperature multiscale entropy analysis: A promising marker for early prediction of mortality in septic patients. Physiol. Meas. 2013, 34, 1449. [Google Scholar] [CrossRef]
- Cuesta-Frau, D.; Varela, M.; Miró-Martínez, P.; Galdós, P.; Abásolo, D.; Hornero, R.; Aboy, M. Predicting survival in critical patients by use of body temperature regularity measurement based on approximate entropy. Med. Biol. Eng. Comput. 2007, 45, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, V.; Chouvarda, I.; Maglaveras, N.; Pneumatikos, I. Temperature variability analysis using wavelets and multiscale entropy in patients with systemic inflammatory response syndrome, sepsis, and septic shock. Crit. Care (London, UK) 2012, 16, R51. [Google Scholar] [CrossRef] [PubMed]
- Culver, A.; Coiffard, B.; Antonini, F.; Duclos, G.; Hammad, E.; Vigne, C.; Mege, J.L.; Baumstarck, K.; Boucekine, M.; Zieleskiewicz, L.; et al. Circadian disruption of core body temperature in trauma patients: A single-center retrospective observational study. J. Intensive Care 2020, 8, 4. [Google Scholar] [CrossRef]
- Drewry, A.M.; Fuller, B.; Bailey, T.; Hotchkiss, R.S. Body temperature patterns as a predictor of hospital-acquired sepsis in afebrile adult intensive care unit patients: A case-control study. Crit. Care (London, UK) 2013, 17, R200. [Google Scholar] [CrossRef]
- Bandt, C.; Pompe, B. Permutation Entropy: A Natural Complexity Measure for Time Series. Phys. Rev. Lett. 2002, 88, 174102. [Google Scholar] [CrossRef]
- Pincus, S.; Gladstone, I.; Ehrenkranz, R. A regularity statistic for medical data analysis. J. Clin. Monit. Comput. 1991, 7, 335–345. [Google Scholar] [CrossRef]
- Cuesta-Frau, D.; Molina-Picó, A.; Vargas, B.; González, P. Permutation Entropy: Enhancing Discriminating Power by Using Relative Frequencies Vector of Ordinal Patterns Instead of Their Shannon Entropy. Entropy 2019, 21, 1013. [Google Scholar] [CrossRef]
- Jost, K.; Pramana, I.; Delgado-Eckert, E.; Kumar, N.; Datta, A.; Frey, U.; Schulzke, S. Dynamics and complexity of body temperature in preterm infants nursed in incubators. PLoS ONE 2017, 12, e0176670. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, N.; Peng, C.K.; Morin, R.; Goldberger, A.L.; Lipsitz, L.A. Age-related alterations in the fractal scaling of cardiac interbeat interval dynamics. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1996, 271, R1078–R1084. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S. Assessing serial irregularity and its implications for health. Ann. N. Y. Acad. Sci. 2001, 954, 245–267. [Google Scholar] [CrossRef] [PubMed]
- Vargas, B.; Cuesta-Frau, D.; Ruiz-Esteban, R.; Cirugeda, E.; Varela, M. What Can Biosignal Entropy Tell Us About Health and Disease? Applications in Some Clinical Fields. Nonlinear Dyn. Psychol. Life Sci. 2015, 19, 419–436. [Google Scholar]
- Cuesta-Frau, D.; Miró-Martínez, P.; Oltra-Crespo, S.; Molina-Picó, A.; Dakappa, P.H.; Mahabala, C.; Vargas, B.; González, P. Classification of fever patterns using a single extracted entropy feature: A feasibility study based on Sample Entropy. Math. Biosci. Eng. 2020, 17, 235. [Google Scholar] [CrossRef]
- Dakappa, P.H.; Rao, S.B.; Bhat, G.K.; Mahabala, C. Unique temperature patterns in 24-h continuous tympanic temperature in tuberculosis. Trop. Dr. 2019, 49, 75–79. [Google Scholar] [CrossRef]
- Dakappa, P.H.; Prasad, K.; Rao, S.B.; Bolumbu, G.; Bhat, G.K.; Mahabala, C. A Predictive Model to Classify Undifferentiated Fever Cases Based on Twenty-Four-Hour Continuous Tympanic Temperature Recording. J. Healthc. Eng. 2017, 2017, 5707162. [Google Scholar] [CrossRef] [PubMed]
- Dakappa, P.H.; Prasad, K.; Rao, S.B.; Bolumbu, G.; Bhat, G.K.; Mahabala, C. Classification of Infectious and Noninfectious Diseases Using Artificial Neural Networks from 24-h Continuous Tympanic Temperature Data of Patients with Undifferentiated Fever. Crit. Rev. Biomed. Eng. 2018, 46, 173–183. [Google Scholar] [CrossRef]
- Ogoina, D. Fever, fever patterns and diseases called ‘fever’—A review. J. Infect. Public Health 2011, 4, 108–124. [Google Scholar] [CrossRef]
- Cuesta-Frau, D. Slope Entropy: A New Time Series Complexity Estimator Based on Both Symbolic Patterns and Amplitude Information. Entropy 2019, 21, 1167. [Google Scholar] [CrossRef]
- Shannon, C.E.; Weaver, W. The Mathematical Theory of Communication; The University of Illinois Press: Urbana, IL, USA, 1949. [Google Scholar]
- Abásolo, D.; Hornero, R.; Espino, P.; Álvarez, D.; Poza, J. Entropy analysis of the EEG background activity in Alzheimer’s disease patients. Physiol. Meas. 2006, 27, 241. [Google Scholar] [CrossRef]
- Sokunbi, M.O. Sample entropy reveals high discriminative power between young and elderly adults in short fMRI data sets. Front. Neuroinform. 2014, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Peng, C.; Ye, D. A study of sleep staging based on a sample entropy analysis of electroencephalogram. Bio-Med. Mater. Eng. 2015, 26, S1149–S1156. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Frau, D.; Novák, D.; Burda, V.; Molina-Picó, A.; Vargas, B.; Mraz, M.; Kavalkova, P.; Benes, M.; Haluzik, M. Characterization of Artifact Influence on the Classification of Glucose Time Series Using Sample Entropy Statistics. Entropy 2018, 20, 871. [Google Scholar] [CrossRef]
- Boughorbel, S.; Jarray, F.; El-Anbari, M. Optimal classifier for imbalanced data using Matthews Correlation Coefficient metric. PLoS ONE 2017, 12, e0177678. [Google Scholar] [CrossRef]
- Guilford, J.P. Psychometric Methods, 2nd ed.; McGraw-Hill: New York, NY, USA, 1954. [Google Scholar]
- Chicco, D.; Jurman, G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genom. 2020, 21, 6. [Google Scholar] [CrossRef]
- Song, B.; Zhang, G.; Zhu, W.; Liang, Z. ROC operating point selection for classification of imbalanced data with application to computer-aided polyp detection in CT colonography. Int. J. Comput. Assist. Radiol. Surg. 2013, 9, 79–89. [Google Scholar] [CrossRef]
- Wong, T.T. Performance evaluation of classification algorithms by k-fold and leave-one-out cross validation. Pattern Recognit. 2015, 48, 2839–2846. [Google Scholar] [CrossRef]
- Weiss, G. Mining with rarity: A unifying framework. SIGKDD Explor. 2004, 6, 7–19. [Google Scholar] [CrossRef]
- Kasem, A.; Ghaibeh, A.; Moriguchi, H. Empirical Study of Sampling Methods for Classification in Imbalanced Clinical Datasets. In International Conference on Computational Intelligence in Information Systems; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Romanovsky, A.; Simons, C.; Kulchitsky, V. “Biphasic” fevers often consist of more than two phases. Am. J. Physiol. 1998, 275, R323–R331. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Frau, D.; Pérez-Cortes, J.C.; García, G.A. Clustering of electrocardiograph signals in computer-aided Holter analysis. Comput. Methods Programs Biomed. 2003, 72 3, 179–196. [Google Scholar] [CrossRef]
- Cuesta-Frau, D.; Murillo-Escobar, J.P.; Orrego, D.A.; Delgado-Trejos, E. Embedded Dimension and Time Series Length. Practical Influence on Permutation Entropy and Its Applications. Entropy 2019, 21, 385. [Google Scholar] [CrossRef]
- Alcaraz, R.; Abásolo, D.; Hornero, R.; Rieta, J. Study of Sample Entropy ideal computational parameters in the estimation of atrial fibrillation organization from the ECG. In Proceedings of the 2010 Computing in Cardiology, Belfast, UK, 26–29 September 2010; pp. 1027–1030. [Google Scholar]
- Aboy, M.; Cuesta–Frau, D.; Austin, D.; Micó–Tormos, P. Characterization of Sample Entropy in the Context of Biomedical Signal Analysis. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 5942–5945. [Google Scholar]
- Alcaraz, R.; Abásolo, D.; Hornero, R.; Rieta, J.J. Optimal parameters study for Sample Entropy-based atrial fibrillation organization analysis. Comput. Methods Programs Biomed. 2010, 99, 124–132. [Google Scholar] [CrossRef]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The Appropriate Use of Approximate Entropy and Sample Entropy with Short Data Sets. Ann. Biomed. Eng. 2013, 41, 349–365. [Google Scholar] [CrossRef]
- Cuesta-Frau, D.; Miró-Martínez, P.; Oltra-Crespo, S.; Jordán-Núñez, J.; Vargas, B.; González, P.; Varela-Entrecanales, M. Model Selection for Body Temperature Signal Classification Using Both Amplitude and Ordinality-Based Entropy Measures. Entropy 2018, 20, 853. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diseases | Method | Sensitivity | Specificity | MCC |
|---|---|---|---|---|
| (DE, MA) | SlopEn | 1 | 0.93 | 0.9066 |
| SampEn | 0.81 | 0.87 | 0.6347 | |
| (DE, LE) | SlopEn | 1 | 0.87 | 0.8500 |
| SampEn | 0.90 | 0.86 | 0.7163 | |
| (MA, LE) | SlopEn | 0.85 | 0.73 | 0.6310 |
| SampEn | 0.80 | 0.56 | 0.3133 | |
| (DE, ML) | SlopEn | 1 | 0.85 | 0.82 |
| SampEn | 0.83 | 0.85 | 0.5534 | |
| (MA, ML) | SlopEn | 0.81 | 0.85 | 0.5635 |
| SampEn | 0.75 | 0.85 | 0.4377 | |
| (NT, TU) | SlopEn | 0.68 | 0.67 | 0.6849 |
| SampEn | 0.61 | 0.68 | – | |
| (NI, TU) | SlopEn | 0.61 | 0.71 | 0.6607 |
| SampEn | 0.78 | 0.75 | – | |
| (NI, NT) | SlopEn | 0.55 | 0.54 | 0.05 |
| SampEn | 0.64 | 0.75 | – |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuesta-Frau, D.; Dakappa, P.H.; Mahabala, C.; Gupta, A.R. Fever Time Series Analysis Using Slope Entropy. Application to Early Unobtrusive Differential Diagnosis. Entropy 2020, 22, 1034. https://doi.org/10.3390/e22091034
Cuesta-Frau D, Dakappa PH, Mahabala C, Gupta AR. Fever Time Series Analysis Using Slope Entropy. Application to Early Unobtrusive Differential Diagnosis. Entropy. 2020; 22(9):1034. https://doi.org/10.3390/e22091034
Chicago/Turabian StyleCuesta-Frau, David, Pradeepa H. Dakappa, Chakrapani Mahabala, and Arjun R. Gupta. 2020. "Fever Time Series Analysis Using Slope Entropy. Application to Early Unobtrusive Differential Diagnosis" Entropy 22, no. 9: 1034. https://doi.org/10.3390/e22091034
APA StyleCuesta-Frau, D., Dakappa, P. H., Mahabala, C., & Gupta, A. R. (2020). Fever Time Series Analysis Using Slope Entropy. Application to Early Unobtrusive Differential Diagnosis. Entropy, 22(9), 1034. https://doi.org/10.3390/e22091034