The Obemat2.0 Study: A Clinical Trial of a Motivational Intervention for Childhood Obesity Treatment

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
2. Study Hypothesis
2.2. Objectives
2.2.1. Primary Objective
2.2.2. Specific Objectives
- Reducing BMI z score,
- improving metabolic control (insulin resistance and lipids profile),
- improving body composition (fat mass and lean mass z scores),
- increasing physical activity,
- acquiring a healthy eating pattern,
- reducing psychosocial problems,
- increasing the adherence to the obesity treatment program in children with obesity between 8 and 13 years old.
- To assess the precision of body composition techniques (air-displacement plethysmography, dual X-ray absorptiometry, and biological impedance) to detect changes in body composition over time in children with obesity and to validate its use against the four component model
- To assess vascular function, by measuring the intima media thickness and estimating blood vessels properties (distension and rigidity), in relation to the obesity degree and metabolic profile
- To assess the respiratory function, and the association between the obesity degree and the degree of bronchial obstruction.
3. Materials and Methods
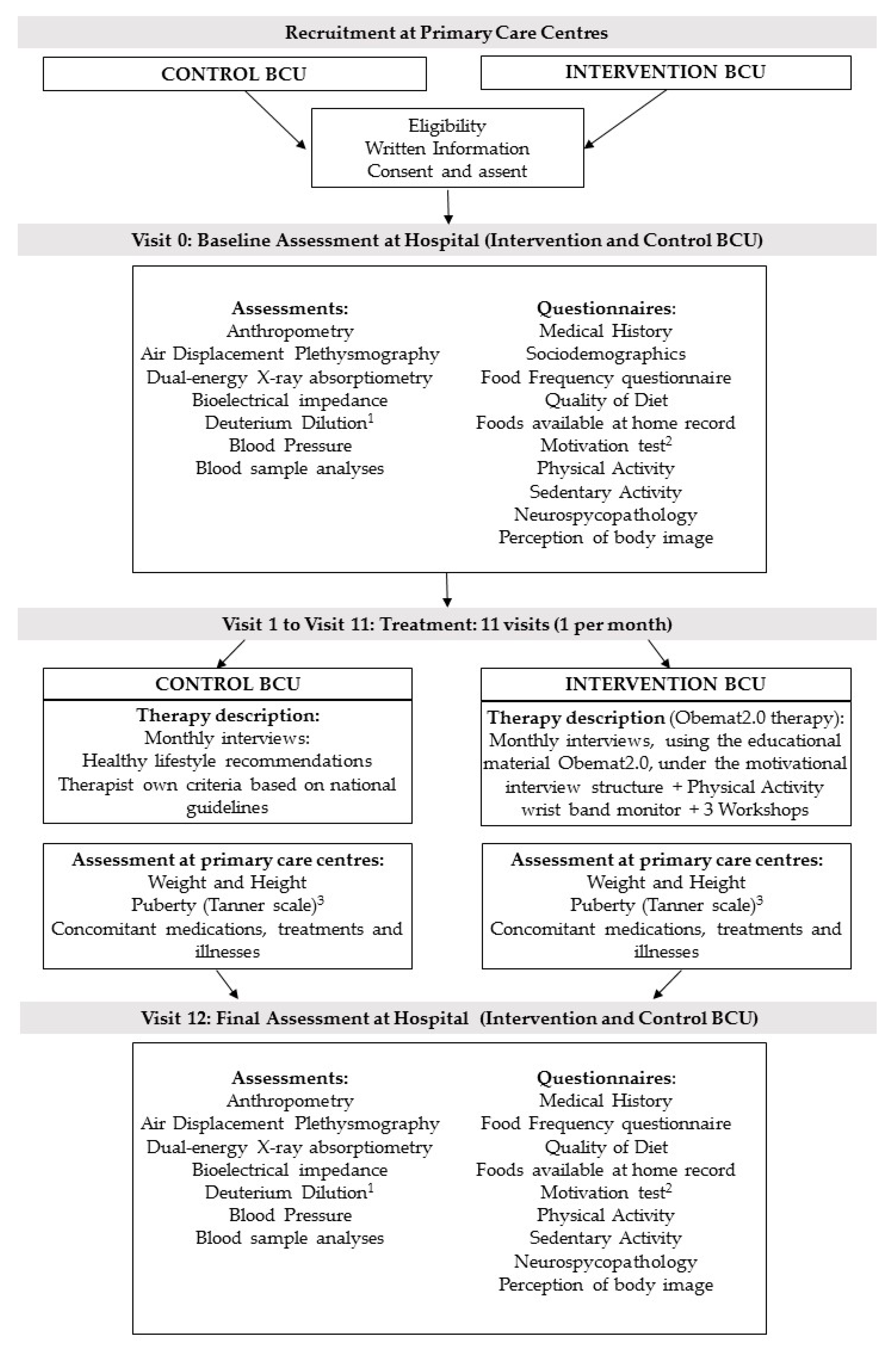
3.1. Study Design and Study Setting
3.2. Context and Time Frame of the Study
3.3. Sample Size
4. Recruitment and Allocation
4.1. Randomization of Therapists
4.2. Training of Therapists
5. Participants
6. Recruitment and Follow-Up of Participants
7. Protocol Variation
8. Description of the Interventions
8.1. Usual Care (Control Group)
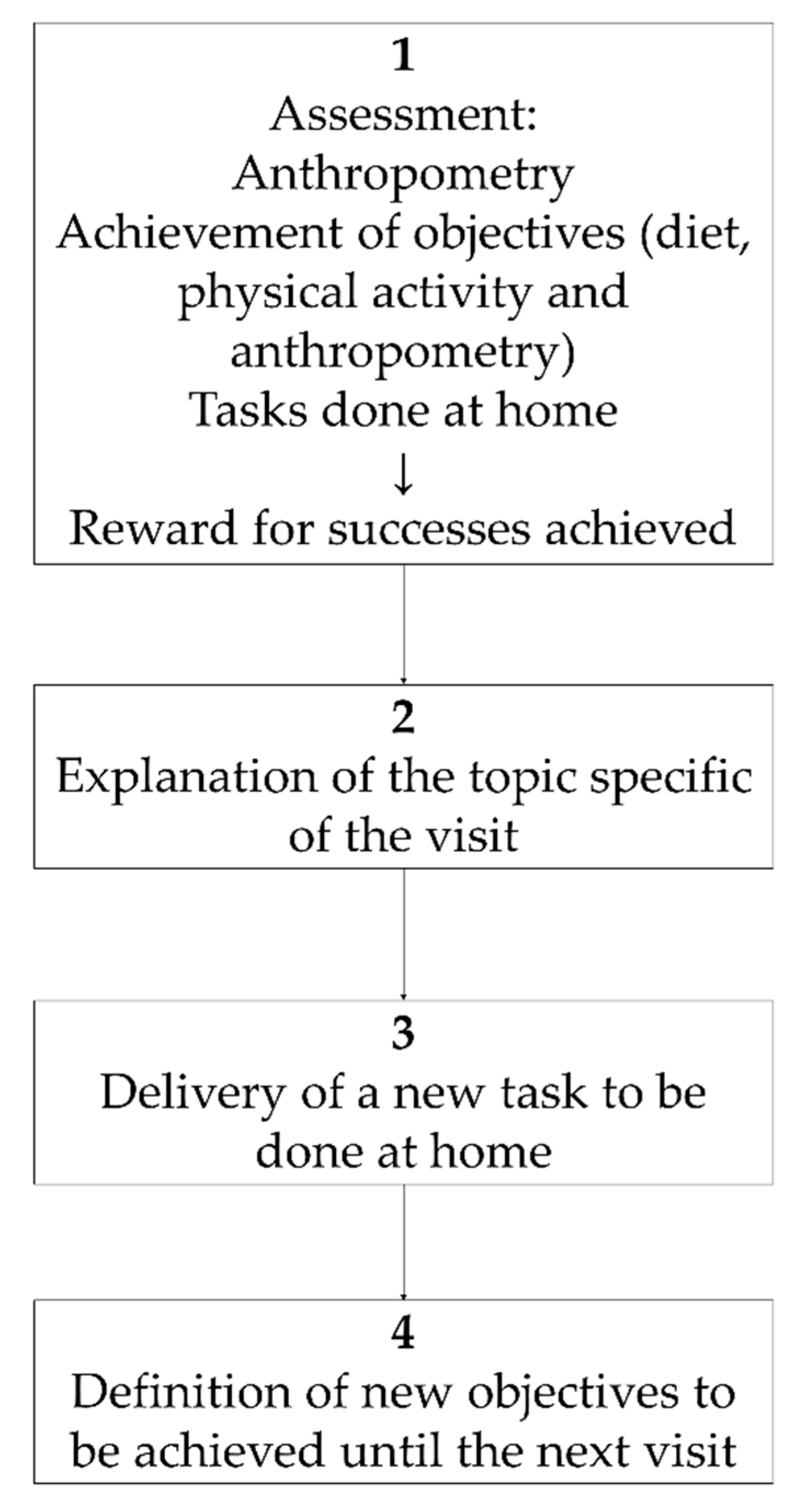
8.2. Obemat2.0 Intervention
9. Outcome Measures
9.1. Primary Outcome
9.2. Secondary Outcomes
10. Outcomes and Variables
10.1. Anthropometry
10.2. Body Composition
10.3. Vascular Function
10.4. Respiratory Function
10.5. Adherence to the Intervention
11. Conditions for Discontinuation of Participation in this Study and Follow-Up Actions
12. Follow-Up of Adverse Events
13. Statistical Analysis Plan
14. Ethics
15. Study Status
16. Discussion
17. Limitations and Strengths
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- O’Connor, E.A.; Evans, C.V.; Burda, B.U.; Walsh, E.S.; Eder, M.; Lozano, P. Screening for Obesity and Intervention for Weight Management in Children and Adolescents. JAMA 2017, 317, 2427. [Google Scholar] [CrossRef] [PubMed]
- Mead, E.; Brown, T.; Rees, K.; Azevedo, L.B.; Whittaker, V.; Jones, D.; Olajide, J.; Mainardi, G.M.; Corpeleijn, E.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 2017, 6, CD012651. [Google Scholar] [CrossRef] [PubMed]
- Rajjo, T.; Mohammed, K.; Alsawas, M.; Ahmed, A.T.; Farah, W.; Asi, N.; Almasri, J.; Prokop, L.J.; Murad, M.H. Treatment of Pediatric Obesity: An Umbrella Systematic Review. J. Clin. Endocrinol. Metab. 2017, 102, 763–775. [Google Scholar] [PubMed]
- Elvsaas, I.K.Ø.; Giske, L.; Fure, B.; Juvet, L.K. Multicomponent Lifestyle Interventions for Treating Overweight and Obesity in Children and Adolescents: A Systematic Review and Meta-Analyses. J. Obes 2017, 2017, 5021902. [Google Scholar] [CrossRef] [PubMed]
- Story, M.T.; Neumark-Stzainer, D.R.; Sherwood, N.E.; Holt, K.; Sofka, D.; Trowbridge, F.L.; Barlow, S.E. Management of child and adolescent obesity: Attitudes, barriers, skills, and training needs among health care professionals. Pediatrics 2002, 110, 210–214. [Google Scholar]
- Poobalan, A.S.; Aucott, L.S.; Precious, E.; Crombie, I.K.; Smith, W.C. Weight loss interventions in young people (18 to 25 year olds): A systematic review. Obes. Rev. 2010, 11, 580–592. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.D.; Cushing, C.C.; Aylward, B.S.; Craig, J.T.; Sorell, D.M.; Steele, R.G. Effectiveness of motivational interviewing interventions for adolescent substance use behavior change: A meta-analytic review. J. Consult. Clin. Psychol. 2011, 79, 433–440. [Google Scholar] [CrossRef]
- Miller, N.H. Motivational interviewing as a prelude to coaching in healthcare settings. J. Cardiovasc. 2010, 25, 247–251. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Mook, D. Motivation: The Organization of Action; W.W. Norton & Company: New York, NY, USA; London, UK, 1995. [Google Scholar]
- Feliu Rovira, A.; París Miró, N.; Zaragoza-Jordana, M.; Ferré Pallás, N.; Chiné Segura, M.; Sabench Pereferrer, F.; Subias, J.E. Eficacia clínica y metabólica de una nueva terapia motivacional (OBEMAT) para el tratamiento de la obesidad en la adolescencia. An. Pediatria 2013, 78, 157–166. [Google Scholar] [CrossRef]
- Martin, L.J.; Burke, S.M.; Shapiro, S.; Carron, A.V.; Irwin, J.D.; Petrella, R.; Prapavessis, H.; Shoemaker, K. The use of group dynamics strategies to enhance cohesion in a lifestyle intervention program for obese children. BMC Public Health 2009, 9, 277. [Google Scholar] [CrossRef] [PubMed]
- Tripicchio, G.L.; Ammerman, A.S.; Neshteruk, C.; Faith, M.S.; Dean, K.; Befort, C.; Ward, D.S.; Truesdale, K.P.; Burger, K.S.; Davis, A. Technology Components as Adjuncts to Family-Based Pediatric Obesity Treatment in Low-Income Minority Youth. Child. Obes. 2017, 13, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; McNarry, M.A.; Mackintosh, K.A. Feasibility and Effectiveness of Using Wearable Activity Trackers in Youth: A Systematic Review. JMIR mHealth uHealth 2016, 4, e129. [Google Scholar] [CrossRef] [PubMed]
- Darling, K.E.; Sato, A.F. Systematic Review and Meta-Analysis Examining the Effectiveness of Mobile Health Technologies in Using Self-Monitoring for Pediatric Weight Management. Child. Obes. 2017, 13, 347–355. [Google Scholar] [CrossRef]
- Kothandan, S.K. School based interventions versus family based interventions in the treatment of childhood obesity—A systematic review. Arch. Public Health 2014, 72, 3. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.L.; Perrin, E.M. Obesity Prevention and Treatment in Primary Care. Acad. Pediatr. 2018, 18, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Kleber, M.; Lass, N.; Toschke, A.M. Body mass index patterns over 5 y in obese children motivated to participate in a 1-y lifestyle intervention: Age as a predictor of long-term success. Am. J. Clin. Nutr. 2010, 91, 1165–1171. [Google Scholar] [CrossRef]
- IMIM Institut Hospital del Mar d’Investigacions Mèdiques; GRANMO: Barcelona, Spain, 2012.
- Gao, F.; Earnest, A.; Matchar, D.B.; Campbell, M.J.; Machin, D. Sample size calculations for the design of cluster randomized trials: A summary of methodology. Contempor. Clin. Trials 2015, 42, 41–50. [Google Scholar] [CrossRef]
- Dirección Xeral de Saúde Pública (Xunta de Galicia). Epidat Software 4.2; Dirección Xeral de Saúde Pública: Santiago de Compostela, Spain, 2004. [Google Scholar]
- Hernández, M.; Castellet, J.; Narvaíza, J.L.; Rincón, J.M.; Ruiz, I.; Sánchez, E.; Sobradillo, B.; Zurimendi, A. Curvas y Tablas de Crecimiento [Growth Charts and Tables]; Growth and Development Research Institute, Orbegozo Foundation: Madrid, Spain, 1988. [Google Scholar]
- Grupo de trabajo de la Guía de Práctica Clínica sobre la Prevención y el Tratamiento de la Obesidad Infantojuvenil, Ministerio de Ciencia e Innovación [Spanish Ministry of Sciencee and Innovation]. Guía de Práctica Clínica sobre la Prevención y el Tratamiento de la Obesidad Infantojuvenil. Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad y Política Social; The Cochrane Collaboration: London, UK, 2009.
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Trinidad Rodríguez, I.; Fernández Ballart, J.; Cucó Pastor, G.; Biarnés Jordà, E.; Arija Val, V. Validación de un cuestionario de frecuencia de consumo alimentario corto: Reproducibilidad y validez. Nutr. Hosp. 2008, 23, 242–252. [Google Scholar]
- Janz, K.; Lutuchy, E.; Wenthe, P.; Levy, S. Measuring activity in children and adolescents using self-report: PAQ-C and PAQ-A. Med. Sci. Sports Exerc. 2008, 40, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Booth, M.L.; Okely, A.D. The reliability of the Adolescent Sedentary Activity Questionnaire (ASAQ). Prev Med. 2007, 45, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Marshall, W.A.; Tanner, J.M. Variations in pattern of pubertal changes in girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Marshall, W.A.; Tanner, J.M. Variations in the pattern of pubertal changes in boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Anthro Software for PC; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Wells, J.C.; Fuller, N.J.; Dewit, O.; Fewtrell, M.S.; Elia, M.; Cole, T.J. Four-component model of body composition in children: Density and hydration of fat-free mass and comparison with simpler models. Am. J. Clin. Nutr. 1999, 69, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Goran, M.I.; McCrory, M.A. Body-composition assessment via air-displacement plethysmography in adults and children: A review. Am. J. Clin. Nutr. 2002, 75, 453–467. [Google Scholar] [CrossRef]
- Lohman, T.G. Assessment of Body Composition in Children. Pediatr. Exerc. Sci. 1989, 1, 19–30. [Google Scholar] [CrossRef]
- International Atomic Energy Agency. Assessment of Body Composition and Total Energy Expenditure in Humans Using Stable Isotope Techniques; IAEA: Viena, Austria, 2009. [Google Scholar]
- Wells, J.C.K.; Williams, J.E.; Chomtho, S.; Darch, T.; Grijalva-Eternod, C.; Kennedy, K.; Haroun, D.; Wilson, C.; Cole, T.J.; Fewtrell, M.S. Pediatric reference data for lean tissue properties: Density and hydration from age 5 to 20 y. Am. J. Clin. Nutr. 2010, 91, 610–618. [Google Scholar] [CrossRef]
- Wells, J.; Williams, J.; Chomtho, S.; Darch, T.; Grijalva-Eternod, C.; Kennedy, K.; Haroun, D.; Wilson, C.; Cole, T.J.; Fewtrell, M.S. Body-composition reference data for simple and reference techniques and a 4-component model: A new UK reference child. Am. J. Clin. Nutr. 2012, 96, 1316–1326. [Google Scholar] [CrossRef]
- Gioia, G.A.; Isquith, P.Q.; Guy, S.C.; Kenworthy, L. BRIEF—Evaluación Conductual de la Función Ejecutiva; TEA Ediciones: Madrid, Spain, 2016. [Google Scholar]
- Goodman, A.; Goodman, R. Strengths and difficulties questionnaire as a dimensional measure of child mental health. J. Am. Acad. Child. Adolesc. Psychiatry 2009, 48, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Sørensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the study of obesity and thinness. Res. Publ Assoc. Res. Nerv. Ment. Dis. 1983, 60, 115–120. [Google Scholar] [PubMed]
- Eckstein, K.C.; Mikhail, L.M.; Ariza, A.J.; Thomson, J.S.; Millard, S.C.; Binns, H.J.; Pediatric Practice Research Group. Parents’ Perceptions of Their Child’s Weight and Health. Pediatrics 2006, 117, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.B.; Wakefield, D.; Rowe, T.M.; Carlisle, P.S.; Cloutier, M.M. Diagnosing pediatric asthma: Validating the Easy Breathing Survey. J. Pediatr. 2001, 139, 267–272. [Google Scholar] [CrossRef]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Available online: www.ginasthma.org (accessed on 20 February 2017).
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.; Stocks, J. GLI-2012 Desktop Software for Individual Calculations, Version 3.3.1 build 5.
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, 834–840. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 284, 3043–3045.
- Committee on Hospital Care. American Academy of Pediatrics. Family-centered care and the pediatrician’s role. Pediatrics 2003, 112, 691–697. [Google Scholar] [CrossRef]
- Britt, E.; Hudson, S.M.; Blampied, N.M. Motivational interviewing in health settings: A review. Patient Educ. Couns. 2004, 53, 147–155. [Google Scholar] [CrossRef]
- Lundahl, B.; Moleni, T.; Burke, B.L.; Butters, R.; Tollefson, D.; Butler, C.; Rollnick, S. Motivational interviewing in medical care settings: A systematic review and meta-analysis of randomized controlled trials. Patient Educ. Couns. 2013, 93, 157–168. [Google Scholar] [CrossRef]
- Borrello, M.; Pietrabissa, G.; Ceccarini, M.; Manzoni, G.M.; Castelnuovo, G. Motivational Interviewing in Childhood Obesity Treatment. Front. Psychol. 2015, 6, 1732. [Google Scholar] [CrossRef] [PubMed]
- Resnicow, K.; McMaster, F.; Bocian, A.; Harris, D.; Zhou, Y.; Snetselaar, L.; Schwartz, R.; Myers, E.; Gotlieb, J.; Foster, J.; et al. Motivational interviewing and dietary counseling for obesity in primary care: An RCT. Pediatrics 2015, 135, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Perrin, E.M.; Flower, K.B.; Garrett, J.; Ammerman, A.S. Preventing and treating obesity: pediatricians’ self-efficacy, barriers, resources, and advocacy. Ambul. Pediatr. 2005, 5, 150–156. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Visit | Topic to Be Discussed | Task Proposed to Be Done |
|---|---|---|
| V1 | General concept of obesity. Acknowledgement of the problem and self-willingness to change | The patient should complete a list with the pros and cons of following the treatment against obesity |
| V2 | Recommendations for food shopping. | Parents should sign a compromise to follow the food shopping list recommendations |
| Workshop 1: Strategies to increase physical activity by using an eHealth monitor | ||
| V3 | Dietetic balance Healthy Menu | To design a menu for the whole week which follows the healthy balance and is adapted to the family preferences |
| Workshop 2: Food products labeling and recommended food portions | ||
| V4 | To explore daily physical activities that could be increased (such us walking to school, taking care of chores such as walking the dog) | To make a list of activities that the child could do to reduce sedentary behavior |
| Workshop 3: Cooking methods. Workshop at the kitchen. | ||
| V5 | What can I do if I have “anxiety”? What to do, what kind of healthy snacks could I have? | To make a list of lifestyle behaviors the patient realize is doing properly and those that should be improved to treat his/her obesity |
| V6 | Habits around the table: family meals at regular times without TV nor screens, avoiding conflicts about food during mealtime, table without any food not assigned to any member of the family (i.e., full piece of bread in the middle of the table, excess of cooked food available) | To set the rules and record the order and schedules of the family around meals |
| V7 | Breakfast and mid-afternoon snacks | To keep a 7 day record of all breakfasts and mid-afternoon snacks eaten (the week prior to the next visit) |
| V8 | Recommended portion sizes Preparing foods to avoid leftovers | To record during the next month how many days there is an excess of prepared food |
| V9 | Different types of physical activity: sport, daily activities, daily displacements, family outdoors activities | To plan family physical activities such as biking, hiking, promenades, etc. |
| V10 | To revise the recommended daily or weekly portions of the different food groups (fruits and vegetables 4–5 per day, pulses 2–3 per week, etc.). Distribution and balance in lunch and dinner within the same day | To do a 7 day food diary during the week prior to the next visit |
| V11 | Food shopping: coming back to “avoiding the negative stimulus” and planning the shopping list Strategies to avoid the access to energy dense foods | Plan the family menu for the next week and plan the shopping list avoiding unnecessary energy dense foods |
| Parameter/Test | V0 | V1 | V2 | V3 | V4 | V5 | V6 | V7 | V8 | V9 | V10 | V11 | V12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical history: Birth characteristics, feeding in early life | ∗ | ||||||||||||
| Sociodemographic questionnaire | ∗ | ||||||||||||
| Medical examination: Tanner maturation stage, Acantosis Nigricans, systolic and diastolic Blood Pressure z score | ∗ | ∗ | ∗ | ∗ | |||||||||
| Anthropometry: weight, height, body mass index z score | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ |
| Anthropometry: waist circumference | ∗ | ∗ | |||||||||||
| Body composition: Bone mineral content and density, Fat Mass, Fat Free Mass, Total Body Water (all standardized as z scores for age and gender) | ∗ | ∗ | |||||||||||
| Blood sampling: HOMA-IR, Lipid metabolism, Liver enzymes and Thyroid Hormones | ∗ | ∗ | |||||||||||
| Neuropsychology, behaviour, and self-perception: BRIEF score, SDQ score, perception of body figure | ∗ | ∗ | |||||||||||
| Diet: Food Frequency Questionnaire, Quality of Mediterranean Diet in children (Kidmed) and pantry | ∗ | ∗ | |||||||||||
| Physical and Sedentary Activity questionnaires, daily steps 1 | ∗ | ∗ | |||||||||||
| Motivational interview 1 | ∗ | ∗ | |||||||||||
| Adherence to treatment: attendance to visits, attendance to workshops 1, use of the eHealth monitor 1 | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | ∗ | |
| Vascular function: Intima media thickness and vessels properties (ultrasound scan) | ∗ | ||||||||||||
| Respiratory Function (Easy Breathing Survey, forced spirometry and bronchodilator test) | ∗ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luque, V.; Feliu, A.; Escribano, J.; Ferré, N.; Flores, G.; Monné, R.; Gutiérrez-Marín, D.; Guillen, N.; Muñoz-Hernando, J.; Zaragoza-Jordana, M.; et al. The Obemat2.0 Study: A Clinical Trial of a Motivational Intervention for Childhood Obesity Treatment. Nutrients 2019, 11, 419. https://doi.org/10.3390/nu11020419
Luque V, Feliu A, Escribano J, Ferré N, Flores G, Monné R, Gutiérrez-Marín D, Guillen N, Muñoz-Hernando J, Zaragoza-Jordana M, et al. The Obemat2.0 Study: A Clinical Trial of a Motivational Intervention for Childhood Obesity Treatment. Nutrients. 2019; 11(2):419. https://doi.org/10.3390/nu11020419
Chicago/Turabian StyleLuque, Veronica, Albert Feliu, Joaquín Escribano, Natalia Ferré, Gemma Flores, Raquel Monné, Desirée Gutiérrez-Marín, Núria Guillen, Judit Muñoz-Hernando, Marta Zaragoza-Jordana, and et al. 2019. "The Obemat2.0 Study: A Clinical Trial of a Motivational Intervention for Childhood Obesity Treatment" Nutrients 11, no. 2: 419. https://doi.org/10.3390/nu11020419
APA StyleLuque, V., Feliu, A., Escribano, J., Ferré, N., Flores, G., Monné, R., Gutiérrez-Marín, D., Guillen, N., Muñoz-Hernando, J., Zaragoza-Jordana, M., Gispert-Llauradó, M., Rubio-Torrents, C., Núñez-Roig, M., Alcázar, M., Ferré, R., Basora, J. M., Hsu, P., Alegret-Basora, C., Arasa, F., ... Closa-Monasterolo, R. (2019). The Obemat2.0 Study: A Clinical Trial of a Motivational Intervention for Childhood Obesity Treatment. Nutrients, 11(2), 419. https://doi.org/10.3390/nu11020419