
COVID-19 Pandemic Increases the Impact of Low Back Pain: A Systematic Review and Metanalysis

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search
2.2. Inclusion Criteria
2.3. Data Collection, Analysis, and Outcomes
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
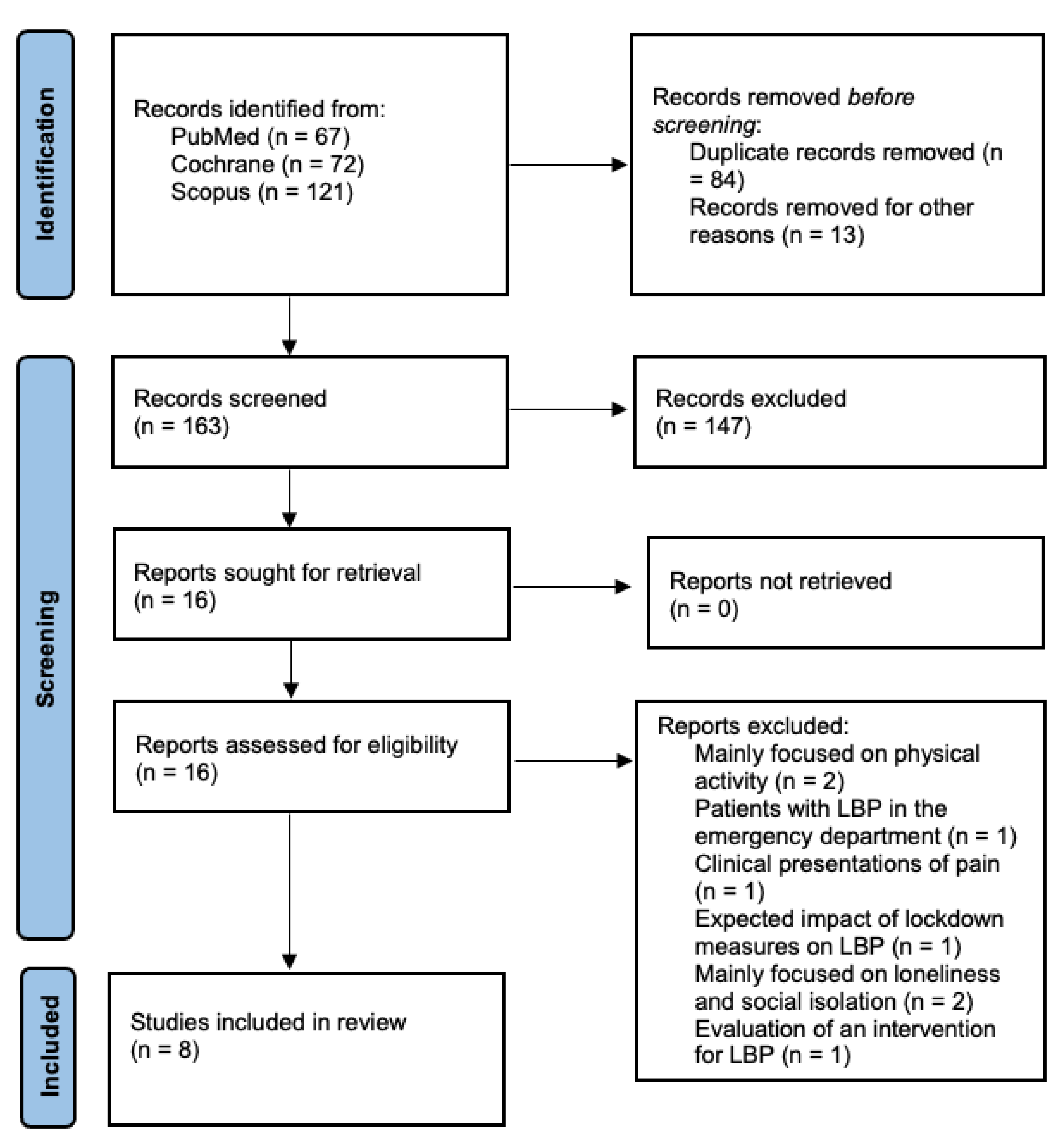
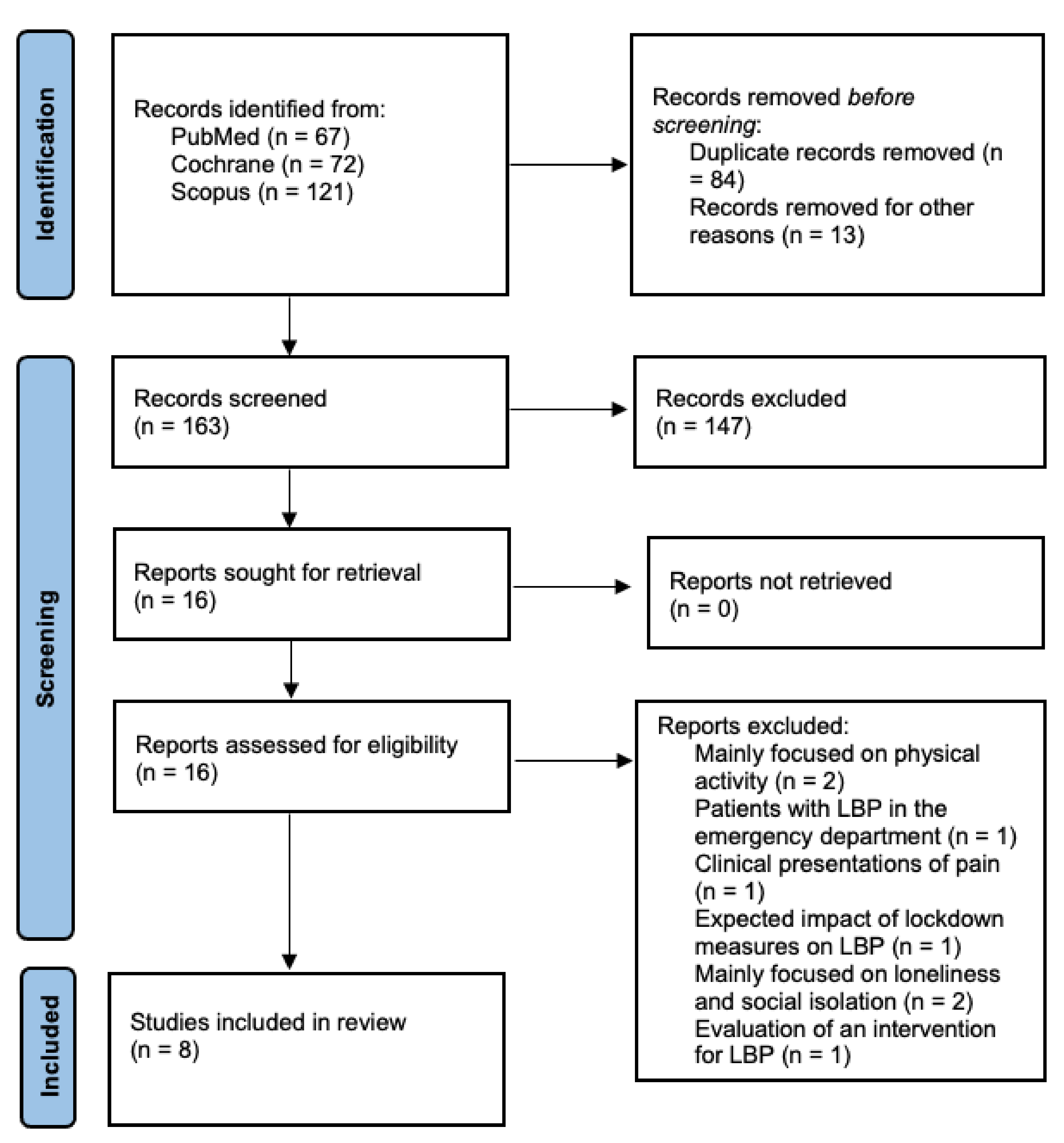
3.1. Literature Search
3.2. Demographic Data
3.3. Methodological Evaluation
3.4. Effect of Intervention
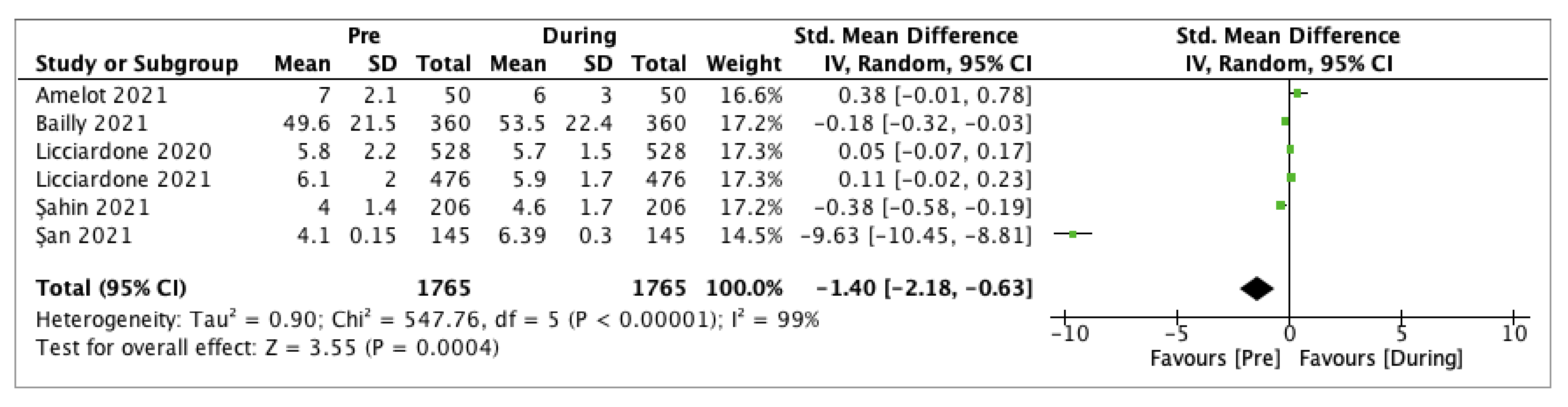
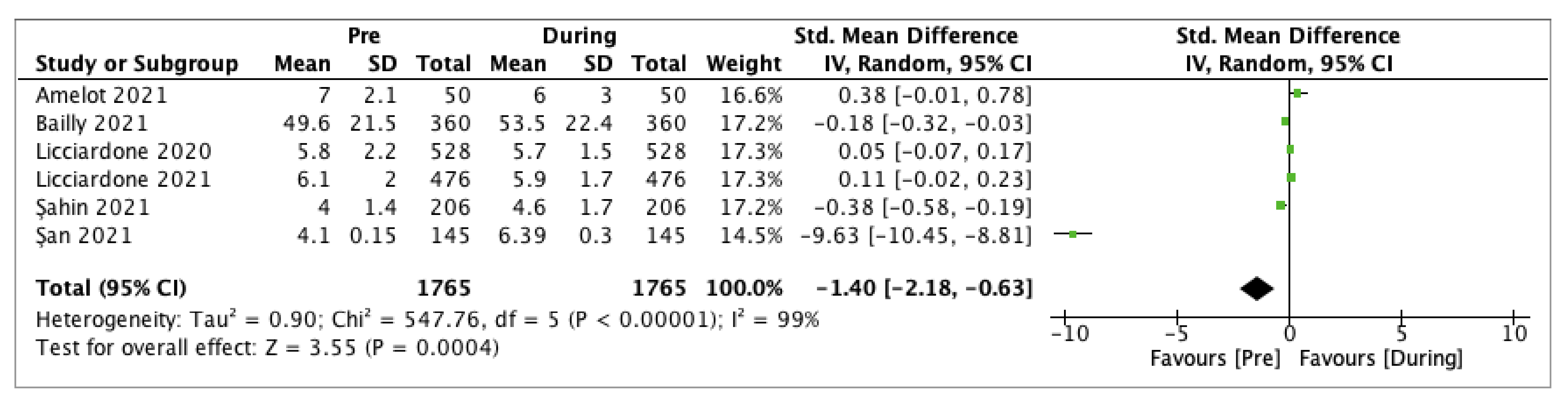
3.4.1. Low Back Pain Intensity
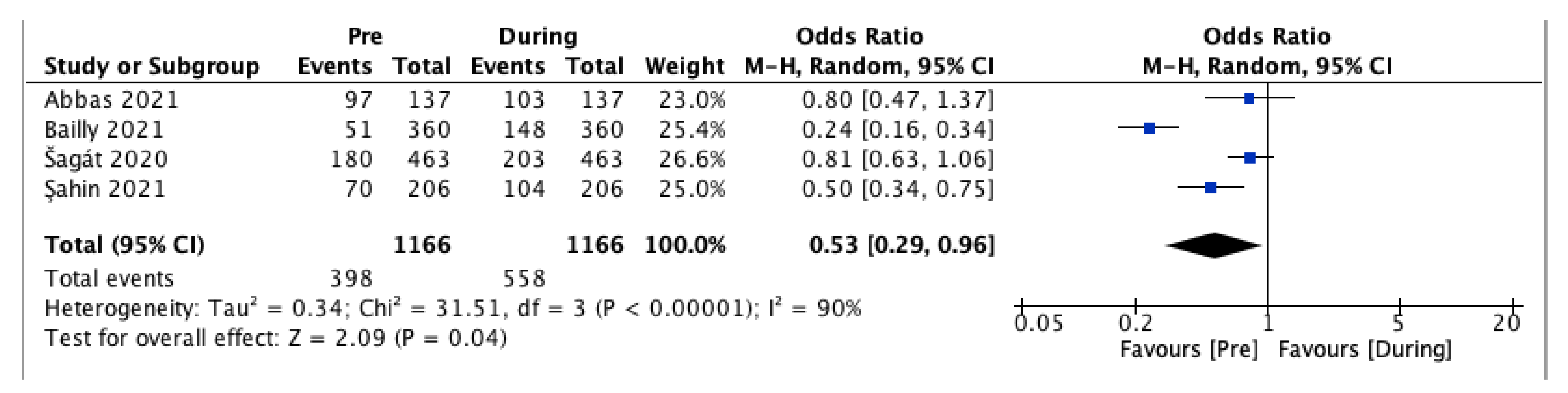
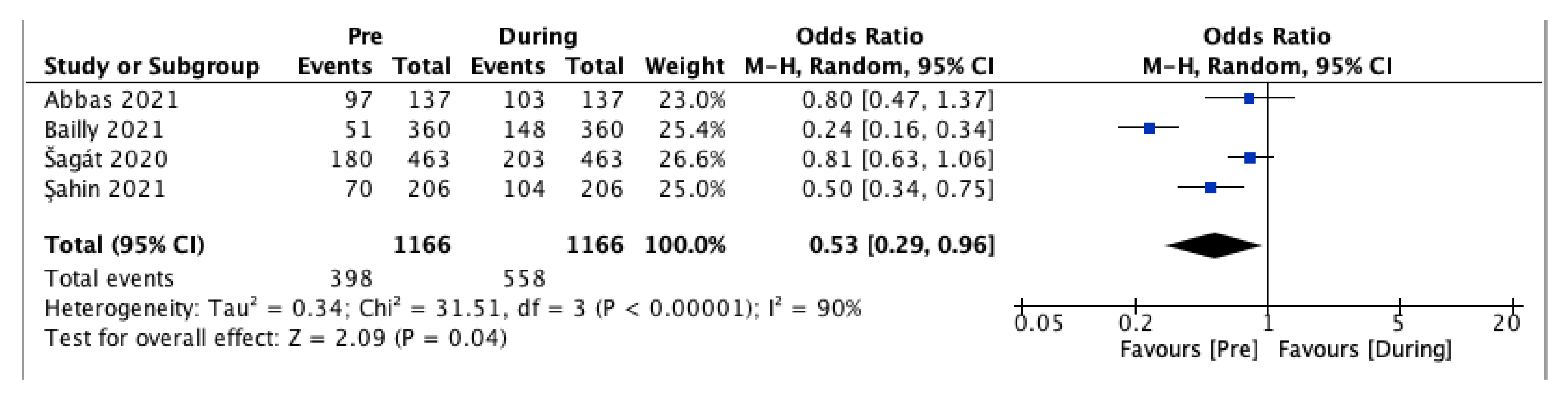
3.4.2. LBP Prevalence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; Chu, D.K.; Akl, E.A.; El-harakeh, A.; Bognanni, A.; et al. Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Roggio, F.; Trovato, B.; Ravalli, S.; Di Rosa, M.; Maugeri, G.; Bianco, A.; Palma, A.; Musumeci, G. One Year of COVID-19 Pandemic in Italy: Effect of Sedentary Behavior on Physical Activity Levels and Musculoskeletal Pain among University Students. Int. J. Environ. Res. Public Health 2021, 18, 8680. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Kan, M.-Y. The Varying Impacts of COVID-19 and Its Related Measures in the UK: A Year in Review. PLoS ONE 2021, 16, e0257286. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, G.; Thiede, B.; Hejazi, B.; Schlenczek, O.; Bodenschatz, E. An Upper Bound on One-to-One Exposure to Infectious Human Respiratory Particles. Proc. Natl. Acad. Sci. USA 2021, 118, e2110117118. [Google Scholar] [CrossRef] [PubMed]
- Rescott, M.L.; De Rosa, O.; Cellini, N.; Coppola, A.; Cerasuolo, M.; Malloggi, S.; Giganti, F.; Ficca, G. Changes in Dream Features across the First and Second Waves of the Covid-19 Pandemic. J. Sleep Res. 2021, 31, e13425. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Serrano-Ibáñez, E.R.; Esteve, R.; Ramírez-Maestre, C.; Ruiz-Párraga, G.T.; López-Martínez, A.E. Chronic Pain in the Time of COVID-19: Stress Aftermath and Central Sensitization. Br. J. Health Psychol. 2021, 26, 544–552. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of Physical Inactivity on Major Non-Communicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Stewart, S.A.; Bagg, M.K.; Stanojevic, S.; Yamato, T.P.; Saragiotto, B.T. Some Types of Exercise Are More Effective than Others in People with Chronic Low Back Pain: A Network Meta-Analysis. J. Physiother. 2021, 67, 252–262. [Google Scholar] [CrossRef]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Malmivaara, A.; van Tulder, M.W. Exercise Therapy for Chronic Low Back Pain. Cochrane Database Syst. Rev. 2021, 9, CD009790. [Google Scholar] [CrossRef]
- Russo, F.; Papalia, G.F.; Vadalà, G.; Fontana, L.; Iavicoli, S.; Papalia, R.; Denaro, V. The Effects of Workplace Interventions on Low Back Pain in Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12614. [Google Scholar] [CrossRef] [PubMed]
- Hendrick, P.; Milosavljevic, S.; Hale, L.; Hurley, D.A.; McDonough, S.; Ryan, B.; Baxter, G.D. The Relationship between Physical Activity and Low Back Pain Outcomes: A Systematic Review of Observational Studies. Eur. Spine J. 2011, 20, 464–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vadalà, G.; Russo, F.; De Salvatore, S.; Cortina, G.; Albo, E.; Papalia, R.; Denaro, V. Physical Activity for the Treatment of Chronic Low Back Pain in Elderly Patients: A Systematic Review. J. Clin. Med. 2020, 9, 1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of Low Back Pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G.; Bovo, C. Current Epidemiology of Low Back Pain. J. Hosp. Manag. Health Policy 2020, 4, 15. [Google Scholar] [CrossRef]
- Vadalà, G.; De Salvatore, S.; Ambrosio, L.; Russo, F.; Papalia, R.; Denaro, V. Robotic Spine Surgery and Augmented Reality Systems: A State of the Art. Neurospine 2020, 17, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What Low Back Pain Is and Why We Need to Pay Attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Russo, F.; Di Tecco, C.; Fontana, L.; Adamo, G.; Papale, A.; Denaro, V.; Iavicoli, S. Prevalence of Work Related Musculoskeletal Disorders in Italian Workers: Is There an Underestimation of the Related Occupational Risk Factors? BMC Musculoskelet. Disord. 2020, 21, 738. [Google Scholar] [CrossRef]
- Clark, S.; Horton, R. Low Back Pain: A Major Global Challenge. Lancet 2018, 391, 2302. [Google Scholar] [CrossRef]
- Shiri, R.; Falah-Hassani, K.; Heliövaara, M.; Solovieva, S.; Amiri, S.; Lallukka, T.; Burdorf, A.; Husgafvel-Pursiainen, K.; Viikari-Juntura, E. Risk Factors for Low Back Pain: A Population-Based Longitudinal Study. Arthritis Care Res. 2019, 71, 290–299. [Google Scholar] [CrossRef] [Green Version]
- Cannata, F.; Vadalà, G.; Russo, F.; Papalia, R.; Napoli, N.; Pozzilli, P. Beneficial Effects of Physical Activity in Diabetic Patients. J. Funct. Morphol. Kinesiol. 2020, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Suka, M.; Yamauchi, T.; Yanagisawa, H. Changes in Health Status, Workload, and Lifestyle after Starting the COVID-19 Pandemic: A Web-Based Survey of Japanese Men and Women. Environ. Health Prev. Med. 2021, 26, 37. [Google Scholar] [CrossRef] [PubMed]
- Vyas, L.; Butakhieo, N. The Impact of Working from Home during COVID-19 on Work and Life Domains: An Exploratory Study on Hong Kong. Policy Des. Pract. 2020, 4, 59–76. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological Guidance for Systematic Reviews of Observational Epidemiological Studies Reporting Prevalence and Cumulative Incidence Data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Gałczyk, M.; Zalewska, A.; Białokoz-Kalinowska, I.; Sobolewski, M. Chronic Back Condition and the Level of Physical Activity as Well as Internet Addiction among Physiotherapy Students during the COVID-19 Pandemic in Poland. Int. J. Environ. Res. Public Health 2021, 18, 6718. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Traeger, A.C.; Machado, G.C.; Shaheed, C.A.; Jones, C.; Maher, C.G. Effect of COVID-19 on Management of Patients with Low Back Pain in the Emergency Department. Australas. Emerg. Care 2021, in press. [Google Scholar] [CrossRef]
- Murat, S.; Karatekin, B.D.; Icagasioglu, A.; Ulasoglu, C.; İçten, S.; Incealtin, O. Clinical Presentations of Pain in Patients with COVID-19 Infection. Ir. J. Med. Sci. 2021, 190, 913–917. [Google Scholar] [CrossRef]
- Galbusera, F.; Côtè, P.; Negrini, S. Expected Impact of Lockdown Measures Due to COVID-19 on Disabling Conditions: A Modelling Study of Chronic Low Back Pain. Eur. Spine J. 2021, 30, 2944–2954. [Google Scholar] [CrossRef]
- Yamada, K.; Wakaizumi, K.; Kubota, Y.; Murayama, H.; Tabuchi, T. Loneliness, Social Isolation, and Pain Following the COVID-19 Outbreak: Data from a Nationwide Internet Survey in Japan. Sci. Rep. 2021, 11, 18643. [Google Scholar] [CrossRef]
- Rassu, F.S.; McFadden, M.; Aaron, R.V.; Wegener, S.T.; Ephraim, P.L.; Lane, E.; Brennan, G.; Minick, K.I.; Fritz, J.M.; Skolasky, R.L. The Relationship Between Neighborhood Deprivation and Perceived Changes for Pain-Related Experiences Among US Patients with Chronic Low Back Pain During the COVID-19 Pandemic. Pain Med. 2021, 22, 2550–2565. [Google Scholar] [CrossRef] [PubMed]
- Licciardone, J.C.; Pandya, V. Feasibility Trial of an EHealth Intervention for Health-Related Quality of Life: Implications for Managing Patients with Chronic Pain During the COVID-19 Pandemic. Healthcare 2020, 8, 381. [Google Scholar] [CrossRef] [PubMed]
- Licciardone, J.C. Impact of COVID-19 on Utilization of Nonpharmacological and Pharmacological Treatments for Chronic Low Back Pain and Clinical Outcomes. J. Osteopath. Med. 2021, 121, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Bailly, F.; Genevay, S.; Foltz, V.; Bohm-Sigrand, A.; Zagala, A.; Nizard, J.; Petit, A. Effects of COVID-19 Lockdown on Low Back Pain Intensity in Chronic Low Back Pain Patients: Results of the Multicenter CONFI-LOMB Study. Eur. Spine J. 2021, 31, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Amelot, A.; Jacquot, A.; Terrier, L.-M.; Aggad, M.; Planty-Bonjour, A.; Fouquet, B.; Cook, A.-R.; Zemmoura, I.; Velut, S.; Destrieux, C.; et al. Chronic Low Back Pain during COVID-19 Lockdown: Is There a Paradox Effect? Eur. Spine J. 2021, 31, 167–175. [Google Scholar] [CrossRef] [PubMed]
- San, A.U.; Serdar, K.; Kutay, T. The Effect of Social Isolation During the COVID-19 Pandemic on Patients with Chronic Low Back Pain Who Underwent a Spine Intervention. Pain Physician 2021, 24, 319–325. [Google Scholar] [CrossRef]
- Abbas, J.; Hamoud, K.; Jubran, R.; Daher, A. Has the COVID-19 Outbreak Altered the Prevalence of Low Back Pain among Physiotherapy Students? J. Am. Coll. Health 2021, 1–6. [Google Scholar] [CrossRef]
- Šagát, P.; Bartík, P.; González, P.P.; Tohănean, D.I.; Knjaz, D. Impact of COVID-19Quarantine on Low Back Pain Intensity, Prevalence, and Associated Risk Factors among Adult Citizens Residing in Riyadh (Saudi Arabia): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7302. [Google Scholar] [CrossRef]
- Şahin, T.; Ayyildiz, A.; Gencer-Atalay, K.; Akgün, C.; Özdemir, H.M.; Kuran, B. Pain Symptoms in COVID-19. Am. J. Phys. Med. Rehabil. 2021, 100, 307–312. [Google Scholar] [CrossRef]
- Licciardone, J.C. Demographic Characteristics Associated With Utilization of Noninvasive Treatments for Chronic Low Back Pain and Related Clinical Outcomes During the COVID-19 Pandemic in the United States. J. Am. Board Fam. Med. 2021, 34, S77–S84. [Google Scholar] [CrossRef]
- Ge, H.; Wang, X.; Yuan, X.; Xiao, G.; Wang, C.; Deng, T.; Yuan, Q.; Xiao, X. The Epidemiology and Clinical Information about COVID-19. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1011–1019. [Google Scholar] [CrossRef]
- Tang, D.; Comish, P.; Kang, R. The Hallmarks of COVID-19 Disease. PLoS Pathog. 2020, 16, e1008536. [Google Scholar] [CrossRef] [PubMed]
- Ambrosio, L.; Vadalà, G.; Russo, F.; Papalia, R.; Denaro, V. The Role of the Orthopaedic Surgeon in the COVID-19 Era: Cautions and Perspectives. J. Exp. Orthop. 2020, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Huang, W.Y.; Sheridan, S.; Sit, C.H.-P.; Chen, X.-K.; Wong, S.H.-S. COVID-19 Pandemic Brings a Sedentary Lifestyle in Young Adults: A Cross-Sectional and Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 6035. [Google Scholar] [CrossRef] [PubMed]
- Hermassi, S.; Hayes, L.D.; Salman, A.; Sanal-Hayes, N.E.M.; Abassi, E.; Al-Kuwari, L.; Aldous, N.; Musa, N.; Alyafei, A.; Bouhafs, E.G.; et al. Physical Activity, Sedentary Behavior, and Satisfaction With Life of University Students in Qatar: Changes During Confinement Due to the COVID-19 Pandemic. Front. Psychol. 2021, 12, 704562. [Google Scholar] [CrossRef]
- Russo, F.; De Salvatore, S.; Ambrosio, L.; Vadalà, G.; Fontana, L.; Papalia, R.; Rantanen, J.; Iavicoli, S.; Denaro, V. Does Workers’ Compensation Status Affect Outcomes after Lumbar Spine Surgery? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6165. [Google Scholar] [CrossRef]
- Russo, F.; Ambrosio, L.; Ngo, K.; Vadalà, G.; Denaro, V.; Fan, Y.; Sowa, G.; Kang, J.D.; Vo, N. The Role of Type I Diabetes in Intervertebral Disc Degeneration. Spine 2019, 44, 1177–1185. [Google Scholar] [CrossRef]
- Petrucci, G.; Papalia, G.F.; Russo, F.; Vadalà, G.; Piredda, M.; De Marinis, M.G.; Papalia, R.; Denaro, V. Psychological Approaches for the Integrative Care of Chronic Low Back Pain: A Systematic Review and Metanalysis. Int. J. Environ. Res. Public Health 2021, 19, 60. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Maher, C.G.; Wiech, K.; Van Zundert, J.; Meloto, C.B.; Diatchenko, L.; Battié, M.C.; Goossens, M.; Koes, B.; Linton, S.J. Low Back Pain. Nat. Rev. Dis. Primer 2018, 4, 52. [Google Scholar] [CrossRef]
- Marshall, P.W.M.; Schabrun, S.; Knox, M.F. Physical Activity and the Mediating Effect of Fear, Depression, Anxiety, and Catastrophizing on Pain Related Disability in People with Chronic Low Back Pain. PLoS ONE 2017, 12, e0180788. [Google Scholar] [CrossRef]
- Wang, Y.; Kala, M.P.; Jafar, T.H. Factors Associated with Psychological Distress during the Coronavirus Disease 2019 (COVID-19) Pandemic on the Predominantly General Population: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0244630. [Google Scholar] [CrossRef] [PubMed]
- Linton, S.J. A Review of Psychological Risk Factors in Back and Neck Pain. Spine 2000, 25, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Rainville, J.; Sobel, J.B.; Hartigan, C.; Wright, A. The Effect of Compensation Involvement on the Reporting of Pain and Disability by Patients Referred for Rehabilitation of Chronic Low Back Pain. Spine 1997, 22, 2016–2024. [Google Scholar] [CrossRef]
- Volinn, E.; Van Koevering, D.; Loeser, J.D. Back Sprain in Industry: The Role of Socioeconomic Factors in Chronicity. Spine 1991, 16, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Fallon, N.; Brown, C.; Twiddy, H.; Brian, E.; Frank, B.; Nurmikko, T.; Stancak, A. Adverse Effects of COVID-19-Related Lockdown on Pain, Physical Activity and Psychological Well-Being in People with Chronic Pain. Br. J. Pain 2021, 15, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Asmundson, G.J.G.; Taylor, S. How Health Anxiety Influences Responses to Viral Outbreaks like COVID-19: What All Decision-Makers, Health Authorities, and Health Care Professionals Need to Know. J. Anxiety Disord. 2020, 71, 102211. [Google Scholar] [CrossRef] [PubMed]
- Bontrup, C.; Taylor, W.R.; Fliesser, M.; Visscher, R.; Green, T.; Wippert, P.-M.; Zemp, R. Low Back Pain and Its Relationship with Sitting Behaviour among Sedentary Office Workers. Appl. Ergon. 2019, 81, 102894. [Google Scholar] [CrossRef]
- Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. [Google Scholar] [CrossRef]
- Alzahrani, H.; Mackey, M.; Stamatakis, E.; Zadro, J.R.; Shirley, D. The Association between Physical Activity and Low Back Pain: A Systematic Review and Meta-Analysis of Observational Studies. Sci. Rep. 2019, 9, 8244. [Google Scholar] [CrossRef]
- European Agency for Safety and Health at Work; IKEI; Panteia. Work-Related Musculoskeletal Disorders: Prevalence, Costs and Demographics in the EU; Publications Office: Luxembourg, 2019. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Type of Study | Study Group | Population | ||
|---|---|---|---|---|---|---|---|
| N. | Age | Sex | |||||
| Licciardone et al. [33] | 2021 | USA | PP | 476 | 54 ± 13.2 | 26.7% M 73.3% F | Patients suffering from chronic LBP |
| Bailly et al. [34] | 2021 | France | CS | 360 | 52.1 ± 13.4 | 41.4% M 58.6% F | Patients suffering from chronic LBP |
| Amelot et al. [35] | 2021 | France | PS | 50 | 52.6 | 48% M 52% F | Patients suffering from chronic LBP |
| Şan et al. [36] | 2021 | Turkey | PS | 145 | 54.78 ± 1.08 | N.R. | Patients who underwent spine surgery within the past year for chronic LBP |
| Abbas et al. [37] | 2021 | Israel | CS | 137 | 27 ± 3 | 42% M 58% F | Physiotherapy students |
| Šagát et al. [38] | 2020 | Saudi Arabia | CS | 463 | 18–34 (n = 252) 35–49 (n = 166) 50–64 (n = 45) | N.R. | Non-specific adult population |
| Şahin et al. [39] | 2021 | Turkey | RS | 206 | 56.24 ± 16.99 | 49% M 51% F | Patients affected by COVID-19 |
| Licciardone et al. [40] | 2020 | USA | PP | 528 | 53.9 ± 13.0 | 25.9% M 74.9% F | Patients suffering from chronic LBP |
| Licciardone (2021) | Bailly | Amelot | Şan | Abbas | Šagát | Şahin | Licciardone (2020) | |
|---|---|---|---|---|---|---|---|---|
| Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | Yes | Unclear | Yes | Yes | Unclear | Yes |
| No | No | No | No | No | No | No | No |
| Yes | Unclear | Yes | Yes | Unclear | Yes | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Low | Moderate | Moderate | Moderate | Moderate | Moderate | Moderate | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papalia, G.F.; Petrucci, G.; Russo, F.; Ambrosio, L.; Vadalà, G.; Iavicoli, S.; Papalia, R.; Denaro, V. COVID-19 Pandemic Increases the Impact of Low Back Pain: A Systematic Review and Metanalysis. Int. J. Environ. Res. Public Health 2022, 19, 4599. https://doi.org/10.3390/ijerph19084599
Papalia GF, Petrucci G, Russo F, Ambrosio L, Vadalà G, Iavicoli S, Papalia R, Denaro V. COVID-19 Pandemic Increases the Impact of Low Back Pain: A Systematic Review and Metanalysis. International Journal of Environmental Research and Public Health. 2022; 19(8):4599. https://doi.org/10.3390/ijerph19084599
Chicago/Turabian StylePapalia, Giuseppe Francesco, Giorgia Petrucci, Fabrizio Russo, Luca Ambrosio, Gianluca Vadalà, Sergio Iavicoli, Rocco Papalia, and Vincenzo Denaro. 2022. "COVID-19 Pandemic Increases the Impact of Low Back Pain: A Systematic Review and Metanalysis" International Journal of Environmental Research and Public Health 19, no. 8: 4599. https://doi.org/10.3390/ijerph19084599
APA StylePapalia, G. F., Petrucci, G., Russo, F., Ambrosio, L., Vadalà, G., Iavicoli, S., Papalia, R., & Denaro, V. (2022). COVID-19 Pandemic Increases the Impact of Low Back Pain: A Systematic Review and Metanalysis. International Journal of Environmental Research and Public Health, 19(8), 4599. https://doi.org/10.3390/ijerph19084599