Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis

Abstract
1. Background
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
2.3. Data Analysis
3. Results
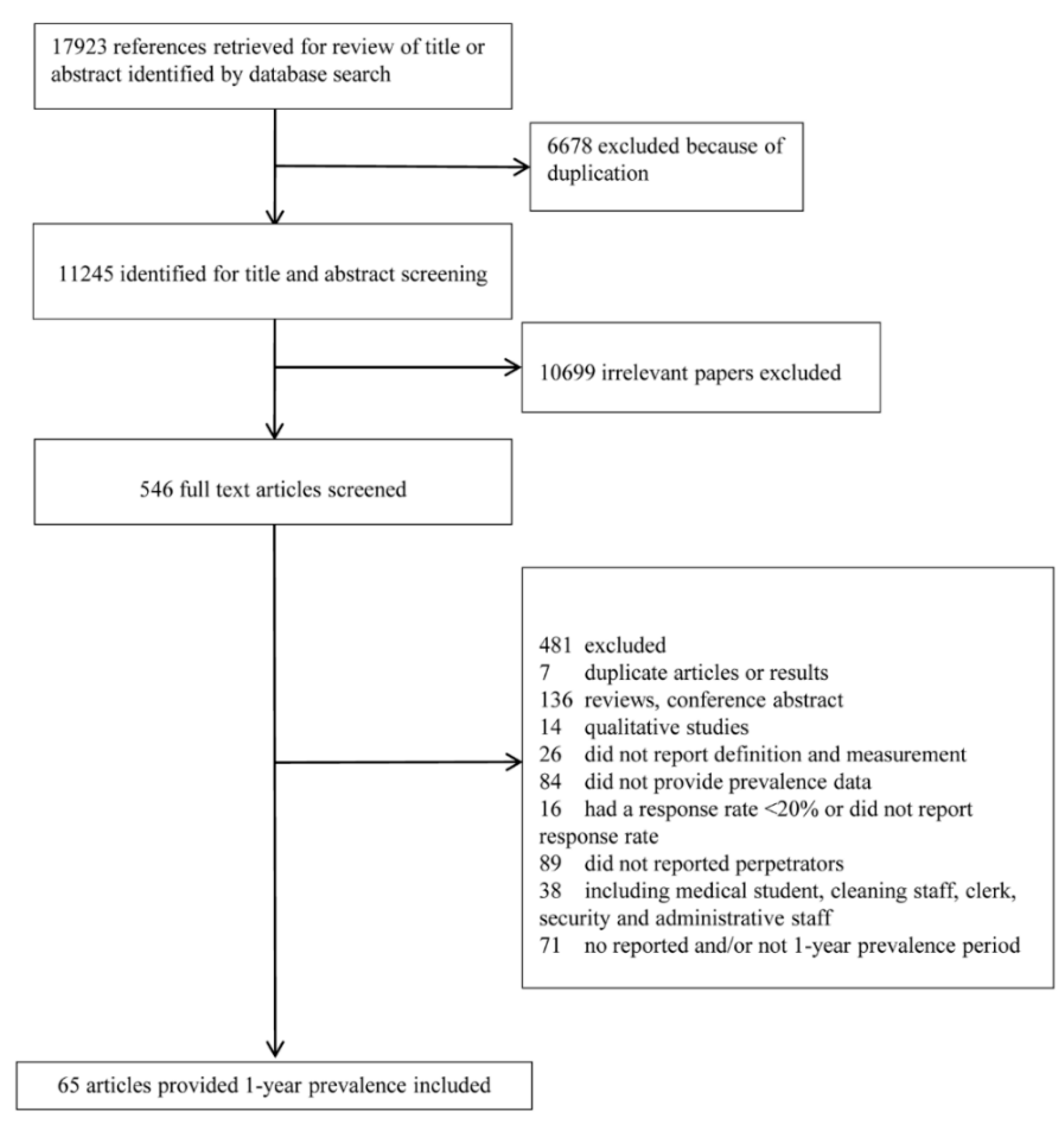
3.1. Study Selection
3.2. Study Characteristics
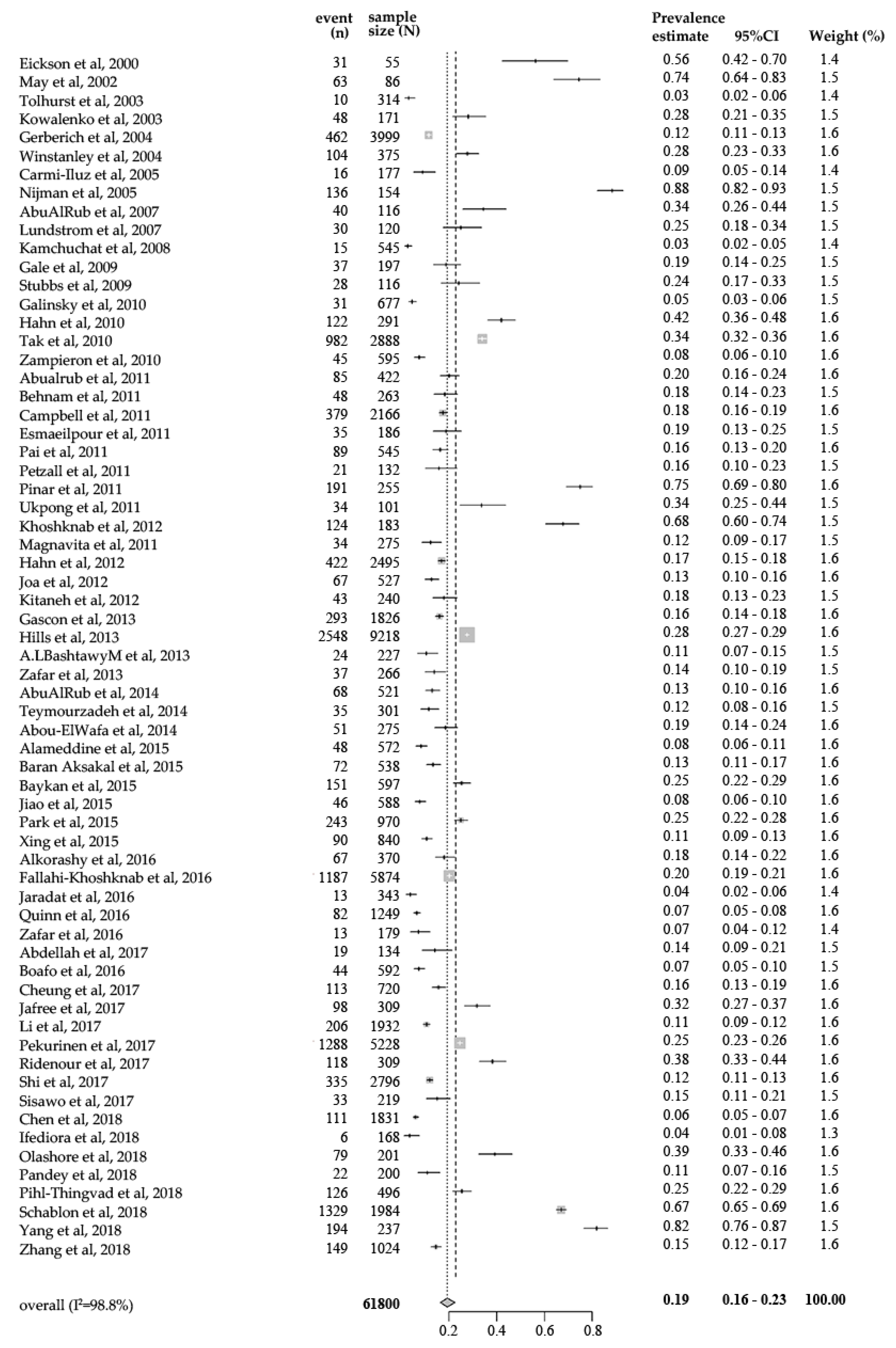
3.3. Pooled One-Year Prevalence of Workplace Physical Violence
3.4. Subgroup Analyses
3.5. Meta-Regression Analyses
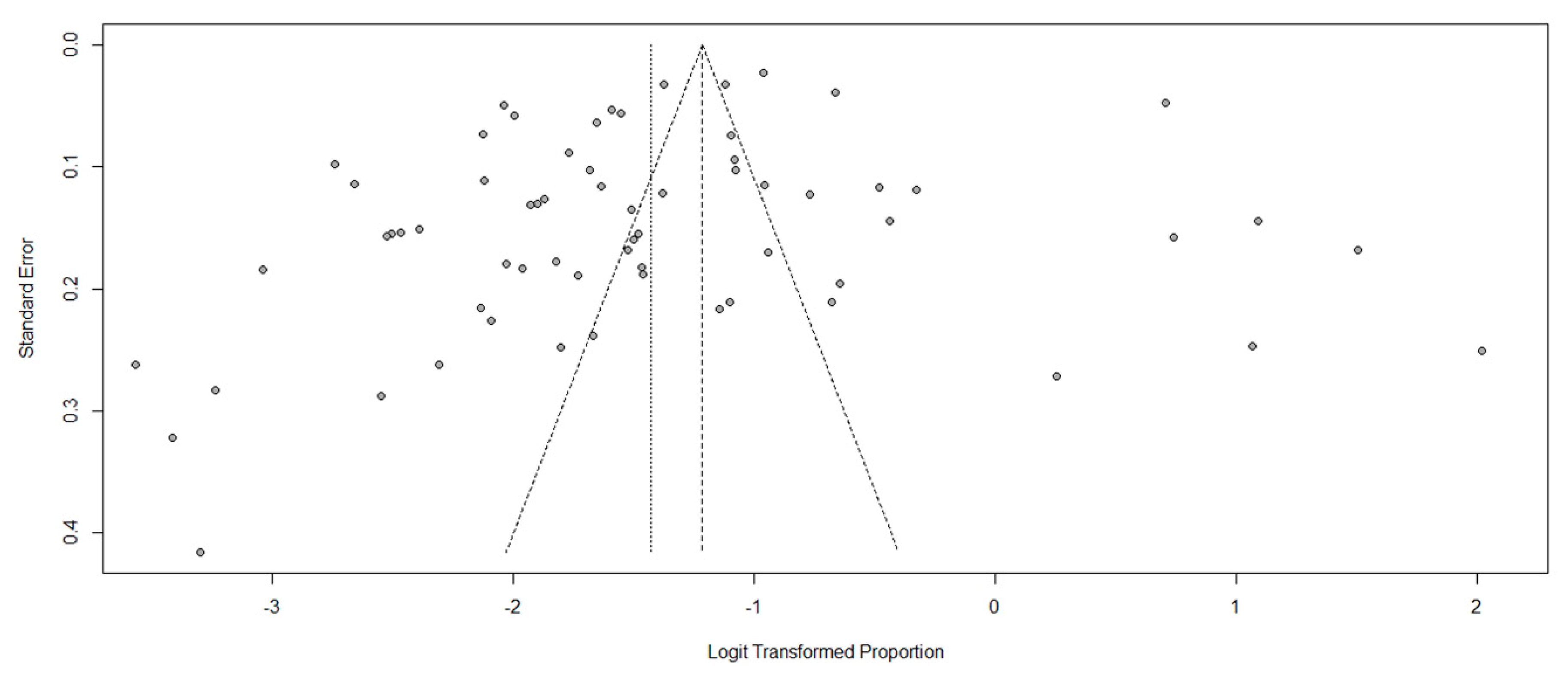
3.6. Sensitivity Analysis and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Phillips, J.P. Workplace Violence against Health Care Workers in the United States. N. Engl. J. Med. 2016, 374, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Piquero, N.L.; Piquero, A.R.; Craig, J.M.; Clipper, S.J. Assessing research on workplace violence, 2000–2012. Aggress. Violent Behav. 2013, 18, 383–394. [Google Scholar] [CrossRef]
- Harrell, E. Workplace Violence, 1993–2009. National Crime Victimization Survey and the Census of Fatal Occupational Injuries; Bureau of Justice Statistics: Washington, DC, USA, 2011.
- Wiskow, C. Guidelines on Workplace Violence in the Health Sector. Available online: https://www.who.int/violence_injury_prevention/violence/interpersonal/en/WV_ComparisonGuidelines.pdf (accessed on 21 March 2019).
- Lanctot, N.; Guay, S. The aftermath of workplace violence among healthcare workers: A systematic literature review of the consequences. Aggress. Violent Behav. 2014, 19, 492–501. [Google Scholar] [CrossRef]
- Shi, L.; Wang, L.; Jia, X.; Li, Z.; Mu, H.; Liu, X.; Peng, B.; Li, A.; Fan, L. Prevalence and correlates of symptoms of post-traumatic stress disorder among Chinese healthcare workers exposed to physical violence: A cross-sectional study. BMJ Open 2017, 7, e016810. [Google Scholar] [CrossRef]
- Zafar, W.; Khan, U.R.; Siddiqui, S.A.; Jamali, S.; Razzak, J.A. Workplace Violence and Self-reported Psychological Health: Coping with Post-traumatic Stress, Mental Distress, and Burnout among Physicians Working in the Emergency Departments Compared to Other Specialties in Pakistan. J. Emerg. Med. 2016, 50, 167–177. [Google Scholar] [CrossRef]
- Alameddine, M.; Mourad, Y.; Dimassi, H. A National Study on Nurses’ Exposure to Occupational Violence in Lebanon: Prevalence, Consequences and Associated Factors. PLoS ONE 2015, 10, e0137105. [Google Scholar] [CrossRef]
- Jaradat, Y.; Nielsen, M.B.; Kristensen, P.; Nijem, K.; Bjertness, E.; Stigum, H.; Bast-Pettersen, R. Workplace aggression, psychological distress, and job satisfaction among Palestinian nurses: A cross-sectional study. Appl. Nurs. Res. ANR 2016, 32, 190–198. [Google Scholar] [CrossRef]
- McGovern, P.; Kochevar, L.; Lohman, W.; Zaidman, B.; Gerberich, S.G.; Nyman, J.; Findorff-Dennis, M. The cost of work-related physical assaults in Minnesota. Health Serv. Res. 2000, 35, 663. [Google Scholar]
- Sumner, S.A.; Mercy, J.A.; Dahlberg, L.L.; Hillis, S.D.; Klevens, J.; Houry, D. Violence in the United States: Status, Challenges, and Opportunities. JAMA 2015, 314, 478–488. [Google Scholar] [CrossRef]
- Schat, A.C.H.; Kelloway, E.K. Reducing the adverse consequences of workplace aggression and violence: The buffering effects of organizational support. J. Occup. Health Psychol. 2003, 8, 110–122. [Google Scholar] [CrossRef]
- Nowrouzi-Kia, B.; Isidro, R.; Chai, E.; Usuba, K.; Chen, A. Antecedent factors in different types of workplace violence against nurses: A systematic review. Aggress. Violent Behav. 2019, 44, 1–7. [Google Scholar] [CrossRef]
- Guay, S.; Goncalves, J.; Jarvis, J. Verbal violence in the workplace according to victims’ sex a systematic review of the literature. Aggress. Violent Behav. 2014, 19, 572–578. [Google Scholar] [CrossRef]
- Pihl-Thingvad, J.; Brandt, L.P.A.; Andersen, L.L. Consistent Use of Assistive Devices for Patient Transfer Is Associated with Less Patient-Initiated Violence: Cross-Sectional Study Among Health Care Workers at General Hospitals. Workplace Health Saf. 2018, 66, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Kamchuchat, C.; Chongsuvivatwong, V.; Oncheunjit, S.; Yip, T.W.; Sangthong, R. Workplace violence directed at nursing staff at a general hospital in Southern Thailand. J. Occup. Health 2008, 50, 201–207. [Google Scholar] [CrossRef]
- May, D.D.; Grubbs, L.M. The extent, nature, and precipitating factors of nurse assault among three groups of registered nurses in a regional medical center. J. Emerg. Nurs. JEN Off. Publ. Emerg. Dep. Nurses Assoc. 2002, 28, 11–17. [Google Scholar] [CrossRef]
- Nikathil, S.; Olaussen, A.; Gocentas, R.A.; Symons, E.; Mitra, B. Review article: Workplace violence in the emergency department: A systematic review and meta analysis. Emerg. Med. Australas. 2017, 29, 265–275. [Google Scholar] [CrossRef]
- Cornaggia, C.M.; Beghi, M.; Pavone, F.; Barale, F. Aggression in psychiatry wards: A systematic review. Psychiatry Res. 2011, 189, 10–20. [Google Scholar] [CrossRef]
- Taylor, J.L.; Rew, L. A systematic review of the literature: Workplace violence in the emergency department. J. Clin. Nurs. 2011, 20, 1072–1085. [Google Scholar] [CrossRef]
- Spector, P.E.; Zhou, Z.E.; Che, X.X. Nurse exposure to physical and nonphysical violence, bullying, and sexual harassment: A quantitative review. Int. J. Nurs. Stud. 2014, 51, 72–84. [Google Scholar] [CrossRef]
- Lu, L.; Dong, M.; Wang, S.B.; Zhang, L.; Ng, C.H.; Ungvari, G.S.; Li, J.; Xiang, Y.T. Prevalence of Workplace Violence Against Health-Care Professionals in China: A Comprehensive Meta-Analysis of Observational Surveys. Trauma Violence Abus. 2018. [Google Scholar] [CrossRef]
- Pompeii, L.; Dement, J.; Schoenfisch, A.; Lavery, A.; Souder, M.; Smith, C.; Lipscomb, H. Perpetrator, worker and workplace characteristics associated with patient and visitor perpetrated violence (Type II) on hospital workers: A review of the literature and existing occupational injury data. J. Saf. Res. 2013, 44, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Erickson, L.; Williams-Evans, S.A. Attitudes of emergency nurses regarding patient assaults. J. Emerg. Nurs. JEN Off. Publ. Emerg. Dep. Nurses Assoc. 2000, 26, 210–215. [Google Scholar] [CrossRef]
- Tolhurst, H.; Baker, L.; Murray, G.; Bell, P.; Sutton, A.; Dean, S. Rural general practitioner experience of work-related violence in Australia. Aust. J. Rural Health 2003, 11, 231–236. [Google Scholar] [PubMed]
- Kowalenko, T.; Walters, B.L.; Compton, S. Workplace violence: A survey of Michigan College of Emergency Physicians. Ann. Emerg. Med. 2003, 42, S6. [Google Scholar]
- Gerberich, S.G.; Church, T.R.; McGovern, P.M.; Hansen, H.E.; Nachreiner, N.M.; Geisser, M.S.; Ryan, A.D.; Mongin, S.J.; Watt, G.D. An epidemiological study of the magnitude and consequences of work related violence: The Minnesota Nurses’ Study. Occup. Environ. Med. 2004, 61, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Winstanley, S.; Whittington, R. Aggression towards health care staff in a UK general hospital: Variation among professions and departments. J. Clin. Nurs. 2004, 13, 3–10. [Google Scholar] [CrossRef]
- Carmi-Iluz, T.; Peleg, R.; Freud, T.; Shvartzman, P. Verbal and physical violence towards hospital- and community-based physicians in the Negev: An observational study. BMC Health Serv. Res. 2005, 5, 54. [Google Scholar] [CrossRef]
- Nijman, H.; Bowers, L.; Oud, N.; Jansen, G. Psychiatric nurses’ experiences with inpatient aggression. Aggress. Behav. 2005, 31, 217–227. [Google Scholar] [CrossRef]
- AbuAlRub, R.F.; Khalifa, M.F.; Habbib, M.B. Workplace violence among Iraqi hospital nurses. J. Nurs. Scholarsh. Off. Publ. Sigma Theta Tau Int. Honor Soc. Nurs. 2007, 39, 281–288. [Google Scholar] [CrossRef]
- Lundstrom, M.; Saveman, B.I.; Eisemann, M.; Astrom, S. Prevalence of violence and its relation to caregivers’ demographics and emotional reactions: An explorative study of caregivers working in group homes for persons with learning disabilities. Scand. J. Caring Sci. 2007, 21, 84–90. [Google Scholar] [CrossRef]
- Gale, C.; Arroll, B.; Coverdale, J. The 12-Month Prevalence of Patient-Initiated Aggression against Psychiatrists: A New Zealand National Survey. Int. J. Psychiatry Med. 2009, 39, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Dickens, G. Physical assault by patients against physiotherapists working in mental health settings. Physiotherapy 2009, 95, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Galinsky, T.; Feng, H.A.; Streit, J.; Brightwell, W.; Pierson, K.; Parsons, K.; Proctor, C. Risk Factors Associated with Patient Assaults of Home Healthcare Workers. Rehabil. Nurs. 2010, 35, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.; Müller, M.; Needham, I.; Dassen, T.; Kok, G.; Halfens, R.J.G. Factors associated with patient and visitor violence experienced by nurses in general hospitals in Switzerland: A cross-sectional survey. J. Clin. Nurs. 2010, 19, 3535–3546. [Google Scholar] [CrossRef] [PubMed]
- Tak, S.; Sweeney, M.H.; Alterman, T.; Baron, S.; Calvert, G.M. Workplace Assaults on Nursing Assistants in US Nursing Homes: A Multilevel Analysis. Am. J. Public Health 2010, 100, 1938–1945. [Google Scholar] [CrossRef]
- Zampieron, A.; Galeazzo, M.; Turra, S.; Buja, A. Perceived aggression towards nurses: Study in two Italian health institutions. J. Clin. Nurs. 2010, 19, 2329–2341. [Google Scholar] [CrossRef]
- Abualrub, R.F.; Al-Asmar, A.H. Physical violence in the workplace among Jordanian hospital nurses. J. Transcult. Nurs. Off. J. Transcult. Nurs. Soc. 2011, 22, 157–165. [Google Scholar] [CrossRef]
- Behnam, M.; Tillotson, R.D.; Davis, S.M.; Hobbs, G.R. Violence in the emergency department: A national survey of emergency medicine residents and attending physicians. J. Emerg. Med. 2011, 40, 565–579. [Google Scholar] [CrossRef]
- Campbell, J.C.; Messing, J.T.; Kub, J.; Agnew, J.; Fitzgerald, S.; Fowler, B.; Sheridan, D.; Lindauer, C.; Deaton, J.; Bolyard, R. Workplace violence: Prevalence and risk factors in the safe at work study. J. Occup. Environ. Med. 2011, 53, 82–89. [Google Scholar] [CrossRef]
- Esmaeilpour, M.; Salsali, M.; Ahmadi, F. Workplace violence against Iranian nurses working in emergency departments. Int. Nurs. Rev. 2011, 58, 130–137. [Google Scholar] [CrossRef]
- Pai, H.C.; Lee, S. Risk factors for workplace violence in clinical registered nurses in Taiwan. J. Clin. Nurs. 2011, 20, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Petzall, K.; Tallberg, J.; Lundin, T.; Suserud, B.O. Threats and violence in the Swedish pre-hospital emergency care. Int. Emerg. Nurs. 2011, 19, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Pinar, R.; Ucmak, F. Verbal and physical violence in emergency departments: A survey of nurses in Istanbul, Turkey. J. Clin. Nurs. 2011, 20, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Ukpong, D.I.; Owoeye, O.; Udofia, O.; Abasiubong, F.; Ukpong, S. Violence against mental health staff: A survey in a Nigerian psychiatric hospital. Psychiatrist 2011, 35, 46–49. [Google Scholar] [CrossRef]
- Khoshknab, M.F.; Tamizi, Z.; Ghazanfari, N.; Mehrabani, G. Prevalence of workplace violence in psychiatric wards, Tehran, Iran. Pak. J. Biol. Sci. PJBS 2012, 15, 680–684. [Google Scholar] [CrossRef]
- Magnavita, N.; Heponiemi, T. Workplace violence against nursing students and nurses: An Italian experience. J. Nurs. Scholarsh. Off. Publ. Sigma Theta Tau Int. Honor Soc. Nurs. 2011, 43, 203–210. [Google Scholar] [CrossRef]
- Hahn, S.; Hantikainen, V.; Needham, I.; Kok, G.; Dassen, T.; Halfens, R.J.G. Patient and visitor violence in the general hospital, occurrence, staff interventions and consequences: A cross-sectional survey. J. Adv. Nurs. 2012, 68, 2685–2699. [Google Scholar] [CrossRef]
- Joa, T.S.; Morken, T. Violence towards personnel in out-of-hours primary care: A cross-sectional study. Scand. J. Prim. Health Care 2012, 30, 55–60. [Google Scholar] [CrossRef]
- Kitaneh, M.; Hamdan, M. Workplace violence against physicians and nurses in Palestinian public hospitals: A cross-sectional study. BMC Health Serv. Res. 2012, 12, 469. [Google Scholar] [CrossRef]
- Gascon, S.; Leiter, M.P.; Andrés, E.; Santed, M.A.; Pereira, J.P.; Cunha, M.J.; Albesa, A.; Montero-Marín, J.; García-Campayo, J.; Martínez-Jarreta, B. The role of aggressions suffered by healthcare workers as predictors of burnout. J. Clin. Nurs. 2013, 22, 3120–3129. [Google Scholar] [CrossRef]
- Hills, D.J.; Joyce, C.M. Personal, professional, and work factors associated with Australian clinical medical practitioners’ experiences of workplace aggression. Ann. Occup. Hyg. 2013, 57, 898–912. [Google Scholar] [PubMed]
- Albashtawy, M. Workplace violence against nurses in emergency departments in Jordan. Int. Nurs. Rev. 2013, 60, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Zafar, W.; Siddiqui, E.; Ejaz, K.; Shehzad, M.U.; Khan, U.R.; Jamali, S.; Razzak, J.A. Health care personnel and workplace violence in the emergency departments of a volatile metropolis: Results from Karachi, Pakistan. J. Emerg. Med. 2013, 45, 761–772. [Google Scholar] [CrossRef] [PubMed]
- AbuAlRub, R.F.; Al Khawaldeh, A.T. Workplace physical violence among hospital nurses and physicians in underserved areas in Jordan. J. Clin. Nurs. 2014, 23, 1937–1947. [Google Scholar] [CrossRef] [PubMed]
- Teymourzadeh, E.; Rashidian, A.; Arab, M.; Akbari-Sari, A.; Hakimzadeh, S.M. Nurses exposure to workplace violence in a large teaching hospital in Iran. Int. J. Health Policy Manag. 2014, 3, 301–305. [Google Scholar] [CrossRef]
- Abou-ElWafa, H.S.; El-Gilany, A.H.; Abd-El-Raouf, S.E.; Abd-Elmouty, S.M.; El-Sayed, R.E.S.H. Workplace Violence Against Emergency Versus Non-Emergency Nurses in Mansoura University Hospitals, Egypt. J. Interpers. Violence 2015, 30, 857–872. [Google Scholar] [CrossRef]
- Baran Aksakal, F.N.; Karaşahin, E.F.; Uğraş Dikmen, A.; Avci, E.; Özkan, S. Workplace physical violence, verbal violence, and mobbing experienced by nurses at a university hospital. Turk. J. Med Sci. 2015, 45, 1360–1368. [Google Scholar] [CrossRef]
- Baykan, Z.; Oktem, I.S.; Cetinkaya, F.; Nacar, M. Physician exposure to violence: A study performed in Turkey. Int. J. Occup. Saf. Ergon. 2015, 21, 291–297. [Google Scholar] [CrossRef]
- Jiao, M.; Ning, N.; Li, Y.; Gao, L.; Cui, Y.; Sun, H.; Kang, Z.; Liang, L.; Wu, Q.; Hao, Y. Workplace violence against nurses in Chinese hospitals: A cross-sectional survey. BMJ Open 2015, 5, e006719. [Google Scholar] [CrossRef]
- Park, M.; Cho, S.H.; Hong, H.J. Prevalence and Perpetrators of Workplace Violence by Nursing Unit and the Relationship Between Violence and the Perceived Work Environment. J. Nurs. Scholarsh. 2015, 47, 87–95. [Google Scholar] [CrossRef]
- Xing, K.; Jiao, M.; Ma, H.; Qiao, H.; Hao, Y.; Li, Y.; Gao, L.; Sun, H.; Kang, Z.; Liang, L.; et al. Physical Violence against General Practitioners and Nurses in Chinese Township Hospitals: A Cross-Sectional Survey. PLoS ONE 2015, 10, e0142954. [Google Scholar] [CrossRef] [PubMed]
- Alkorashy, H.A.E.; Al Moalad, F.B. Workplace violence against nursing staff in a Saudi university hospital. Int. Nurs. Rev. 2016, 63, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Fallahi-Khoshknab, M.; Oskouie, F.; Najafi, F.; Ghazanfari, N.; Tamizi, Z.; Afshani, S. Physical violence against health care workers: A nationwide study from Iran. Iran. J. Nurs. Midwifery Res. 2016, 21, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.M.; Markkanen, P.K.; Galligan, C.J.; Sama, S.R.; Kriebel, D.; Gore, R.J.; Brouillette, N.M.; Okyere, D.; Sun, C.; Punnett, L.; et al. Occupational health of home care aides: Results of the safe home care survey. Occup. Environ. Med. 2016, 73, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Abdellah, R.F.; Salama, K.M. Prevalence and risk factors of workplace violence against health care workers in emergency department in Ismailia, Egypt. Pan Afr. Med. J. 2017, 26, 21. [Google Scholar] [CrossRef] [PubMed]
- Boafo, I.M.; Hancock, P. Workplace Violence Against Nurses: A Cross-Sectional Descriptive Study of Ghanaian Nurses. Sage Open 2017, 7. [Google Scholar] [CrossRef]
- Cheung, T.; Lee, P.H.; Yip, P.S.F. Workplace Violence toward Physicians and Nurses: Prevalence and Correlates in Macau. Int. J. Environ. Res. Public Health 2017, 14, 879. [Google Scholar] [CrossRef]
- Jafree, S.R. Workplace violence against women nurses working in two public sector hospitals of Lahore, Pakistan. Nurs. Outlook 2017, 65, 420–427. [Google Scholar] [CrossRef]
- Li, Z.; Yan, C.M.; Shi, L.; Mu, H.T.; Li, X.; Li, A.Q.; Zhao, C.S.; Sun, T.; Gao, L.; Fan, L.H.; et al. Workplace violence against medical staff of Chinese children’s hospitals: A cross-sectional study. PLoS ONE 2017, 12, e0179373. [Google Scholar] [CrossRef]
- Pekurinen, V.; Willman, L.; Virtanen, M.; Kivimaki, M.; Vahtera, J.; Valimaki, M. Patient Aggression and the Wellbeing of Nurses: A Cross-Sectional Survey Study in Psychiatric and Non-Psychiatric Settings. Int. J. Environ. Res. Public Health 2017, 14, 1245. [Google Scholar] [CrossRef]
- Ridenour, M.L.; Hendricks, S.; Hartley, D.; Blando, J.D. Workplace Violence and Training Required by New Legislation Among NJ Nurses. J. Occup. Environ. Med. 2017, 59, e35–e40. [Google Scholar] [CrossRef] [PubMed]
- Sisawo, E.J.; Ouédraogo, S.Y.Y.A.; Huang, S.L. Workplace violence against nurses in the Gambia: Mixed methods design. BMC Health Serv. Res. 2017, 17, 311. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lv, M.; Wang, M.; Wang, X.; Liu, J.; Zheng, N.; Liu, C. Incidence and risk factors of workplace violence against nurses in a Chinese top-level teaching hospital: A cross-sectional study. Appl. Nurs. Res. ANR 2018, 40, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Ifediora, C.O. Evaluation of aggression in Australian after-hours doctor home-visit services. J. Eval. Clin. Pract. 2018, 24, 388–395. [Google Scholar] [CrossRef]
- Olashore, A.A.; Akanni, O.O.; Molebatsi, K.; Ogunjumo, J.A. Post-traumatic stress disorder among the staff of a mental health hospital: Prevalence and risk factors. S. Afr. J. Psychiatry 2018, 24. [Google Scholar] [CrossRef]
- Pandey, M.; Bhandari, T.R.; Dangal, G. Workplace Violence and its Associated Factors among Nurses. J. Nepal Health Res. Counc. 2018, 15, 235–241. [Google Scholar] [CrossRef]
- Schablon, A.; Wendeler, D.; Kozak, A.; Nienhaus, A.; Steinke, S. Prevalence and consequences of aggression and violence towards nursing and care staff in Germany—A survey. Int. J. Environ. Res. Public Health 2018, 15, 1274. [Google Scholar] [CrossRef]
- Yang, B.X.; Stone, T.E.; Petrini, M.A.; Morris, D.L. Incidence, Type, Related Factors, and Effect of Workplace Violence on Mental Health Nurses: A Cross-sectional Survey. Arch. Psychiatr. Nurs. 2018, 32, 31–38. [Google Scholar] [CrossRef]
- Zhang, S.E.; Liu, W.; Wang, J.; Shi, Y.; Xie, F.; Cang, S.; Sun, T.; Fan, L. Impact of workplace violence and compassionate behaviour in hospitals on stress, sleep quality and subjective health status among Chinese nurses: A cross-sectional survey. BMJ Open 2018, 8, e019373. [Google Scholar] [CrossRef]
- Hahn, S.; Zeller, A.; Needham, I.; Kok, G.; Dassen, T.; Halfens, R.J.G. Patient and visitor violence in general hospitals: A systematic review of the literature. Aggress. Violent Behav. 2008, 13, 431–441. [Google Scholar] [CrossRef]
- Hills, D.; Joyce, C. A review of research on the prevalence, antecedents, consequences and prevention of workplace aggression in clinical medical practice. Aggress. Violent Behav. 2013, 18, 554–569. [Google Scholar] [CrossRef]
- Wassell, J.T. Workplace violence intervention effectiveness: A systematic literature review. Saf. Sci. 2009, 47, 1049–1055. [Google Scholar] [CrossRef]
- Mata, D.A.; Ramos, M.A.; Bansal, N.; Khan, R.; Guille, C.; Di Angelantonio, E.; Sen, S. Prevalence of Depression and Depressive Symptoms Among Resident Physicians: A Systematic Review and Meta-analysis. JAMA 2015, 314, 2373–2383. [Google Scholar] [CrossRef] [PubMed]
- Yon, Y.; Mikton, C.R.; Gassoumis, Z.D.; Wilber, K.H. Elder abuse prevalence in community settings: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e147–e156. [Google Scholar] [CrossRef]
- Lepping, P.; Lanka, S.V.N.; Turner, J.; Stanaway, S.E.R.S.; Krishna, M. Percentage prevalence of patient and visitor violence against staff in high-risk UK medical wards. Clin. Med. 2013, 13, 543–546. [Google Scholar] [CrossRef] [PubMed]
- Shafran-Tikva, S.; Zelker, R.; Stern, Z.; Chinitz, D. Workplace violence in a tertiary care Israeli hospital—A systematic analysis of the types of violence, the perpetrators and hospital departments. Isr. J. Health Policy Res. 2017, 6, 43. [Google Scholar] [CrossRef]
- Guay, S.; Goncalves, J.; Jarvis, J. A systematic review of exposure to physical violence across occupational domains according to victims’ sex. Aggress. Violent Behav. 2015, 25, 133–141. [Google Scholar] [CrossRef]
- Farrell, G.A.; Shafiei, T.; Chan, S.P. Patient and visitor assault on nurses and midwives: An exploratory study of employer ‘protective’ factors. Int. J. Ment. Health Nurs. 2014, 23, 88–96. [Google Scholar] [CrossRef]
- Wang, N.; Wu, D.; Sun, C.; Li, L.; Zhou, X. Workplace Violence in County Hospitals in Eastern China: Risk Factors and Hospital Attitudes. J. Interpers. Violence 2018. [Google Scholar] [CrossRef]
- Hasan, M.I.; Hassan, M.Z.; Bulbul, M.M.I.; Joarder, T.; Chisti, M.J. Iceberg of workplace violence in health sector of Bangladesh. BMC Res. Notes 2018, 11, 702. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | WHO Region | Sample Size | Event | Income Classification | Professional Group | Setting | Region of Health Care Setting | Method of Data Collection | Response Rate | Sampling | Quality Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eickson et al., 2000 [24] | U.S. | Americas | 55 | 31 | High income | nurses | emergency department | urban | self-administered | 98.00% | convenience | 4 |
| May et al., 2002 [17] | U.S. | Americas | 86 | 64 | High income | nurses | general hospital | urban | self-administered | 68.80% | convenience | 3 |
| Tolhurst et al., 2003 [25] | Australia | Western Pacific | 314 | 10 | High income | physicians | primary care | rural | self-administered | 51.80% | purposive | 4 |
| Kowalenko et al., 2003 [26] | U.S. | Americas | 171 | 48 | High income | physicians | emergency department | mixed | self-administered | 68.40% | random | 4 |
| Gerberich et al., 2004 [27] | U.S. | Americas | 3999 | 462 | High income | nurses | Hospital/nursing home/other setting | mixed | self-administered | 78.00% | random | 6 |
| Winstanley et al., 2004 [28] | U.K. | European | 375 | 104 | High income | nurses/physicians | general hospital | mixed | self-administered | 33.00% | all | 6 |
| Carmi-Iluz et al., 2005 [29] | Israel | European | 177 | 16 | High income | physicians | hospital/community | mixed | self-administered | 88.50% | convenience | 4 |
| Nijman et al., 2005 [30] | U.K. | European | 154 | 136 | High income | nurses | psychiatric | urban | self-administered | 39.00% | all | 4 |
| AbuAlRub et al., 2007 [31] | Iraq | Eastern Mediterranean | 116 | 40 | Upper middle income | nurses | general hospital | urban | face-to-face interview | 100.00% | purposive | 5 |
| Lundstrom et al., 2007 [32] | Sweden | European | 120 | 30 | High income | nurses/assistant nurses/nurse’s aides | nursing home | urban | self-administered | 81.00% | / | 4 |
| Kamchuchat et al., 2008 [16] | Thailand | South-East Asia | 545 | 15 | Upper middle income | nurses | general hospital | / | self-administered | 91.70% | all | 7 |
| Gale et al., 2009 [33] | New Zealand | Western Pacific | 197 | 37 | High income | physicians | psychiatric | mixed | self-administered | 63.90% | all | 4 |
| Stubbs et al., 2009 [34] | U.K. | European | 116 | 28 | High income | physicians | psychiatric | mixed | self-administered | 65.00% | all | 4 |
| Galinsky et al., 2010 [35] | U.S. | Americas | 677 | 31 | High income | nurses/assistant nurses/nurse’s aides | home healthcare | urban | face-to-face interview | 64.00% | convenience | 4 |
| Hahn et al., 2010 [36] | Switzerland | European | 291 | 122 | High income | nurses | general hospital | / | self-administered | 71.00% | purposive | 4 |
| Tak et al., 2010 [37] | U.S. | Americas | 2888 | 982 | High income | assistant nurses | nursing home | / | telephone interview | 70.60% | random | 7 |
| Zampieron et al., 2010 [38] | Italy | European | 595 | 45 | High income | nurses | general hospital | urban | self-administered | 85.00% | convenience | 6 |
| Abualrub et al., 2011 [39] | Jordan | Eastern Mediterranean | 422 | 85 | Upper middle income | nurses | general hospital | / | self-administered | 84.40% | convenience | 5 |
| Behnam et al., 2011 [40] | U.S. | Americas | 263 | 48 | High income | physicians | emergency department | mixed | self-administered | 97.00% | random | 6 |
| Campbell et al., 2011 [41] | U.S. | Americas | 2166 | 379 | High income | nurses | hospital/elder care | urban | self-administered | 52.00% | all | 5 |
| Esmaeilpour et al., 2011 [42] | Iran | Eastern Mediterranean | 186 | 35 | Upper middle income | nurses | emergency department | urban | self-administered | 94.80% | / | 6 |
| Pai et al., 2011 [43] | China Taiwan | Western Pacific | 545 | 89 | High income | nurses | health care setting | mixed | self-administered | 77.90% | random | 5 |
| Petzall et al., 2011 [44] | Switzerland | European | 132 | 21 | High income | ambulance personnel | ambulance stations | mixed | self-administered | 79.00% | convenience | 8 |
| Pinar et al., 2011 [45] | Turkey | European | 255 | 191 | Upper middle income | nurses | emergency department | urban | self-administered | 96.22% | all | 4 |
| Ukpong et al., 2011 [46] | Nigeria | African | 101 | 34 | Lower middle income | nurses/physicians | psychiatric | urban | self-administered | 84.20% | / | 5 |
| Khoshknab et al., 2012 [47] | Iran | Eastern Mediterranean | 183 | 124 | Upper middle income | nurses | psychiatric | urban | self-administered | 91.50% | random | 4 |
| Magnavita et al., 2011 [48] | Italy | European | 275 | 34 | High income | nurses | general hospital | / | self-administered | 94.20% | / | 6 |
| Hahn et al., 2012 [49] | Switzerland | European | 2495 | 422 | High income | health care professionals | general hospital | / | self-administered | 51.50% | all | 4 |
| Joa et al., 2012 [50] | Norway | European | 527 | 67 | High income | health care professionals | primary care | mixed | telephone interview | 75.00% | all | 6 |
| Kitaneh et al., 2012 [51] | Palestine | Eastern Mediterranean | 240 | 43 | Lower middle income | nurses/physicians | general hospital | / | self-administered | 88.70% | random | 6 |
| Gascon et al., 2013 [52] | Spain | European | 1826 | 293 | High income | health care professionals | hospital/primary care center | mixed | self-administered | 76.00% | random | 6 |
| Hills et al., 2013 [53] | Australia | Western Pacific | 9218 | 2548 | High income | physicians | health care setting | mixed | self-administered | 60.90% | all | 7 |
| A.LBashtawyM et al., 2013 [54] | Jordan | Eastern Mediterranean | 227 | 24 | Lower middle income | nurses | emergency department | / | self-administered | 72.50% | convenience | 6 |
| Zafar et al., 2013 [55] | Pakistan | Eastern Mediterranean | 266 | 37 | Lower middle income | nurses/physicians | emergency department | urban | self-administered | 86.00% | all | 4 |
| AbuAlRub et al., 2014 [56] | Jordan | Eastern Mediterranean | 521 | 68 | Lower middle income | nurses/physicians | general hospital | / | self-administered | 75.00% | all | 6 |
| Teymourzadeh et al., 2014 [57] | Iran | Eastern Mediterranean | 301 | 35 | Upper middle income | nurses | general hospital | urban | self-administered | 73.00% | all | 8 |
| Abou-ElWafa et al., 2014 [58] | Egypt | Eastern Mediterranean | 275 | 51 | Lower middle income | nurses | Emergency department/internal medicine | urban | self-administered | 96.15% | all | 8 |
| Alameddine et al., 2015 [8] | Lebanon | Eastern Mediterranean | 572 | 48 | Upper middle income | nurses | health care setting | / | self-administered | 64.80% | random | 6 |
| Baran Aksakal et al., 2015 [59] | Turkey | European | 538 | 72 | Upper middle income | nurses | general hospital | / | face-to-face interview | 82.76% | all | 6 |
| Baykan et al., 2015 [60] | Turkey | European | 597 | 151 | Upper middle income | physicians | health care workplace | / | self-administered | 75.90% | all | 8 |
| Jiao et al., 2015 [61] | China | Western Pacific | 588 | 46 | Upper middle income | nurses | general hospital | urban | self-administered | 84.00% | random | 7 |
| Park et al., 2015 [62] | Korea | Western Pacific | 970 | 243 | High income | nurses | general hospital | urban | self-administered | 95.20% | convenience | 8 |
| Xing et al., 2015 [63] | China | Western Pacific | 840 | 90 | Upper middle income | nurses/physicians | primary care | rural | self-administered | 84.80% | purposive | 5 |
| Alkorashy et al., 2016 [64] | Saudi Arabia | Eastern Mediterranean | 370 | 67 | High income | nurses | general hospital | urban | self-administered | 80.80% | convenience | 6 |
| Fallahi-Khoshknab et al., 2016 [65] | Iran | Eastern Mediterranean | 5874 | 1187 | Upper middle income | health care professionals | general hospital | / | self-administered | 90.36% | random | 5 |
| Jaradat et al., 2016 [9] | Palestine | Eastern Mediterranean | 343 | 13 | Lower middle income | nurses | hospitals/primary care | / | self-administered | 92.20% | / | 8 |
| Quinn et al., 2016 [66] | U.S. | Americas | 1249 | 82 | High income | home care aides | home healthcare | / | self-administered | 44.20% | / | 6 |
| Zafar et al., 2016 [7] | Pakistan | Eastern Mediterranean | 179 | 13 | Lower middle income | physicians | general hospital | urban | self-administered | 92.20% | all | 4 |
| Abdellah et al., 2017 [67] | Egypt | Eastern Mediterranean | 134 | 19 | Lower middle income | Health care professionals | emergency department | urban | self-administered | 94.40% | / | 7 |
| Boafo et al., 2016 [68] | Ghana | African | 592 | 44 | Lower middle income | nurses | general hospital | / | self-administered | 57.98% | random | 4 |
| Cheung et al., 2017 [69] | China | Western Pacific | 720 | 113 | Upper middle income | nurses/physicians | general hospital | urban | self-administered | 80.00% | convenience | 7 |
| Jafree et al., 2017 [70] | Pakistan | Eastern Mediterranean | 309 | 98 | Lower middle income | nurses | general hospital | urban | self-administered | 34.80% | random | 6 |
| Li et al., 2017 [71] | China | Western Pacific | 1932 | 206 | Upper middle income | nurses/physicians | pediatric hospital | urban | self-administered | 86.80% | random | 7 |
| Pekurinen et al., 2017 [72] | Finland | European | 5228 | 1288 | High income | nurses | general hospital | / | self-administered | 70.00% | all | 7 |
| Ridenour et al., 2017 [73] | U.S. | Americas | 309 | 118 | High income | nurses | general hospital | / | self-administered | 22.50% | random | 7 |
| Shi et al., 2017 [6] | China | Western Pacific | 2796 | 335 | Upper middle income | health care professionals | general hospital | / | self-administered | 64.25% | convenience | 6 |
| Sisawo et al., 2017 [74] | Gambia | African | 219 | 33 | low income | nurses | general hospital | mixed | face-to-face interview | 98.20% | purposive | 5 |
| Chen et al., 2018 [75] | China | Western Pacific | 1831 | 111 | Upper middle income | nurses | general hospital | urban | self-administered | 92.30% | all | 5 |
| Ifediora et al., 2018 [76] | Australia | Western Pacific | 168 | 6 | High income | physicians | primary care | / | self-administered | 56.00% | / | 7 |
| Olashore et al., 2018 [77] | Botswana | African | 201 | 79 | Upper middle income | health care professionals | psychiatric | urban | self-administered | 95.70% | all | 3 |
| Pandey et al., 2018 [78] | Nepal | South-East Asia | 200 | 22 | low income | nurses | general hospital | / | self-administered | 100.00% | random | 5 |
| Pihl-Thingvad et al., 2018 [15] | Denmark | European | 496 | 126 | High income | health care professionals | general hospital | urban | self-administered | 28.00% | all | 7 |
| Schablon et al., 2018 [79] | Germany | European | 1984 | 1329 | High income | nurses | hospital/elder care/residential facility | / | self-administered | 40.90% | random | 6 |
| Yang et al., 2018 [80] | China | Western Pacific | 237 | 194 | Upper middle income | nurses | psychiatric | urban | self-administered | 84.50% | / | 5 |
| Zhang et al., 2018 [81] | China | Western Pacific | 1024 | 149 | Upper middle income | nurses | general hospital | / | self-administered | 75.18% | snowball | 4 |
| Subgroup | Studies | Pooled Prevalence % (95% CI) | I2 | Test of Difference within Each Subgroup | |
|---|---|---|---|---|---|
| Q | p | ||||
| WHO Region | 10.60 | 0.0599 | |||
| European | 18 | 26.38 (18.42–36.25) | 99.2% | ||
| Americas | 10 | 23.61 (15.25–34.67) | 99.0% | ||
| African | 4 | 20.71 (8.59–42.07) | 97.3% | ||
| Eastern Mediterranean | 17 | 17.07 (13.15–21.86) | 95.7% | ||
| Western Pacific | 14 | 14.53 (10.05–20.54) | 98.9% | ||
| South-East Asia | 2 | 5.62 (1.38–20.14) | 94.5% | ||
| Income classification | 9.84 | 0.0020 | |||
| High-income | 32 | 21.66 (17.49–26.51) | 99.0% | ||
| Upper-middle-income | 20 | 19.98 (14.61–26.69) | 98.7% | ||
| Lower-middle-income | 11 | 13.75 (9.49–19.50) | 93.6% | ||
| Low-income | 2 | 13.14 (9.62–17.70) | 33.6% | ||
| Year of publication | 1.06 | 0.3036 | |||
| 2000–2010 | 17 | 22.83 (15.31–32.61) | 98.6% | ||
| 2011–2018 | 48 | 18.22 (15.17–21.73) | 98.8% | ||
| Sample size | 9.91 | 0.0016 | |||
| ≤500 | 37 | 24.48 (18.84–31.16) | 97.2% | ||
| >500 | 28 | 13.96 (10.99–17·57) | 99.3% | ||
| Response rate | 4.31 | 0.0379 | |||
| ≤50% | 7 | 38.53 (18.75–63.00) | 99.4% | ||
| >50% | 58 | 17.65 (15.33–20.23) | 98.1% | ||
| Professional group | 4.38 | 0.0364 | |||
| nurses | 34 | 22.99 (17.11–30.16) | 99.1% | ||
| physicians | 10 | 14.66 (10.67–19.81) | 94.4% | ||
| Method of collection | 0.88 | 0.6441 | |||
| Self-administered | 59 | 19.66 (16.60–23.14) | 98·8% | ||
| face-to-face interview | 4 | 13.93 (6.39–27.76) | 96.3% | ||
| Telephone interview | 2 | 21.61 (7.40–48.73) | 98.8% | ||
| Gender | 0.04 | 0.8392 | |||
| Male | 3 | 7.37 (2.00–23.69) | 89.5% | ||
| Female | 3 | 8.40 (6.72–10.46) | 37.9% | ||
| Sampling | 0.84 | 0.6572 | |||
| all | 21 | 20.82 (16.89–25.38) | 98.2% | ||
| Random | 17 | 20.86 (14.19–29.59) | 99.4% | ||
| convenience | 17 | 17.64 (12.82–23.79) | 97.1% | ||
| Region of health care setting | 7.93 | 0.0190 | |||
| Urban | 27 | 26.16 (19.11–34.69) | 98.5% | ||
| Rural/township | 2 | 6.11 (1.80–18.76) | 93.1% | ||
| Mixed | 13 | 17.85 (13.68–22.97) | 97.7% | ||
| Type of health care setting | 39.52 | <0.0001 | |||
| Tertiary hospital | 18 | 22.48 (15.35–31.69) | 98.4% | ||
| Secondary hospital | 3 | 18·83 (9.94–32.77) | 91.3% | ||
| Primary care facilities | 6 | 6.51 (4.36–9.64) | 90.2% | ||
| nursing home | 2 | 30.33 (22.32–39.75) | 75.7% | ||
| Quality score | 3.92 | 0.0476 | |||
| ≤5 | 31 | 24.00 (16.41–33.69) | 99.0% | ||
| >5 | 34 | 15.86 (13.53–18.51) | 98.3% | ||
| Univariate Analysis | β | 95% CI | R2 | p Value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Publish year (continuous variable) | −0.0483 | −0.1076 | 0.0109 | 2.29% | 0.1100 |
| Sample size (n < 500 vs. n ≥ 500) | −0.6983 | −1.2281 | −0.1685 | 8.72% | 0.0098 |
| Response rate (continuous variable) | −0.7139 | −2.1540 | 0.7262 | 0.00% | 0.3313 |
| Income Classification (high income vs. other) | 0.2798 | −0.2698 | 0.8294 | 0.00% | 0.3183 |
| Professional (nurses vs. other) | −0.6344 | −1.5518 | 0.2831 | 1.66% | 0.1753 |
| Region of health care setting (urban vs. rural) | 0.6527 | −0.0754 | 1.3808 | 4.78% | 0.0789 |
| Type of health care setting (tertiary hospital vs. primary care facilities) | 1.4696 | 0.5297 | 2.4095 | 14.20% | 0.0022 |
| Method of data collection (Self-administered vs. others) | 0.4451 | −0.1229 | 1.0130 | 2.22% | 0.1245 |
| Quality score (continuous variable) | −0.2125 | −0.4117 | −0.0134 | 5.41% | 0.0364 |
| Multivariate Analysis | |||||
| Sample size (n < 500 vs. n ≥ 500) | −0.1671 | −0.7712 | 0.4369 | / | 0.5876 |
| Type of health care setting (tertiary hospital vs. primary care facilities) | 1.8345 | 0.8373 | 2.8316 | / | 0.0003 |
| Quality score (continuous variable) | −0.3008 | −0.5314 | −0.0703 | / | 0.0105 |
| Overall | 24.87% | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.-L.; Li, R.-Q.; Qiu, D.; Xiao, S.-Y. Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 299. https://doi.org/10.3390/ijerph17010299
Li Y-L, Li R-Q, Qiu D, Xiao S-Y. Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(1):299. https://doi.org/10.3390/ijerph17010299
Chicago/Turabian StyleLi, Yi-Lu, Rui-Qi Li, Dan Qiu, and Shui-Yuan Xiao. 2020. "Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 1: 299. https://doi.org/10.3390/ijerph17010299
APA StyleLi, Y.-L., Li, R.-Q., Qiu, D., & Xiao, S.-Y. (2020). Prevalence of Workplace Physical Violence against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(1), 299. https://doi.org/10.3390/ijerph17010299