Laboratory Parameters of Hemostasis, Adhesion Molecules, and Inflammation in Type 2 Diabetes Mellitus: Correlation with Glycemic Control


 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients Enrolled
2.2. Laboratory Determinations
2.3. Statistical Analysis
3. Results
3.1. Comparison between Patients with T2DM and Controls
3.2. Comparison between Patients with T2DM in Relation to the Degree of Glycemic Control
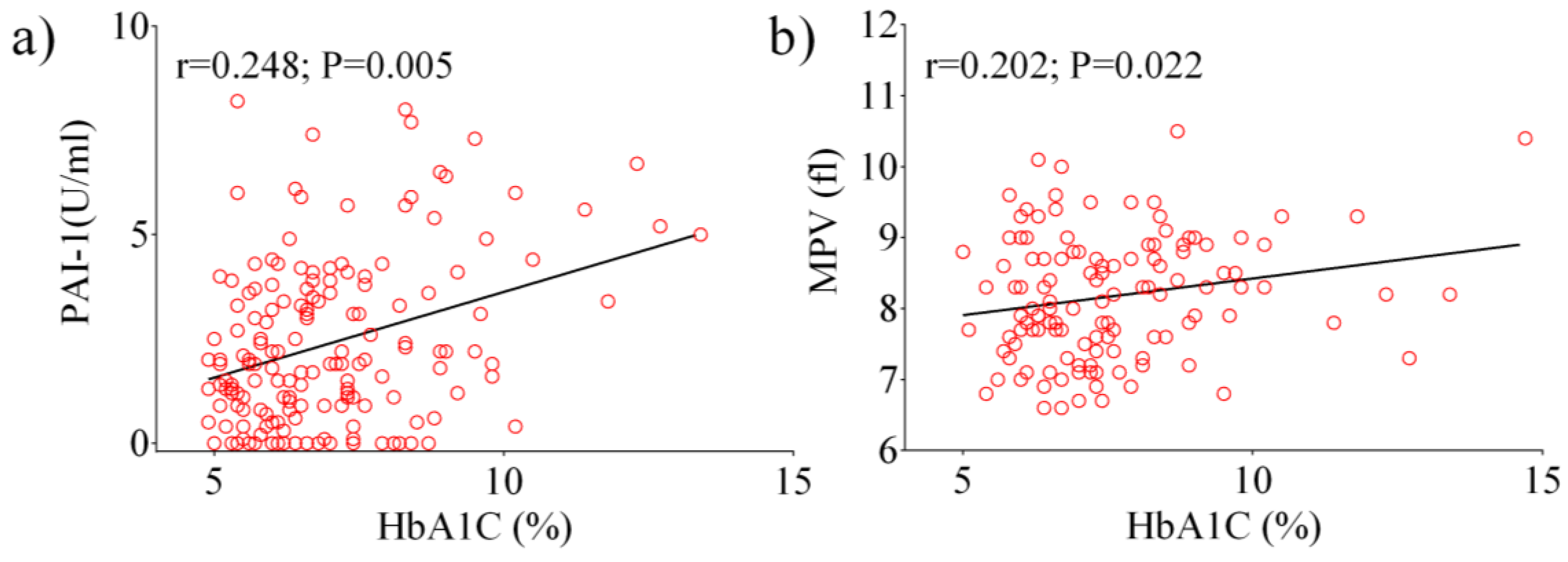
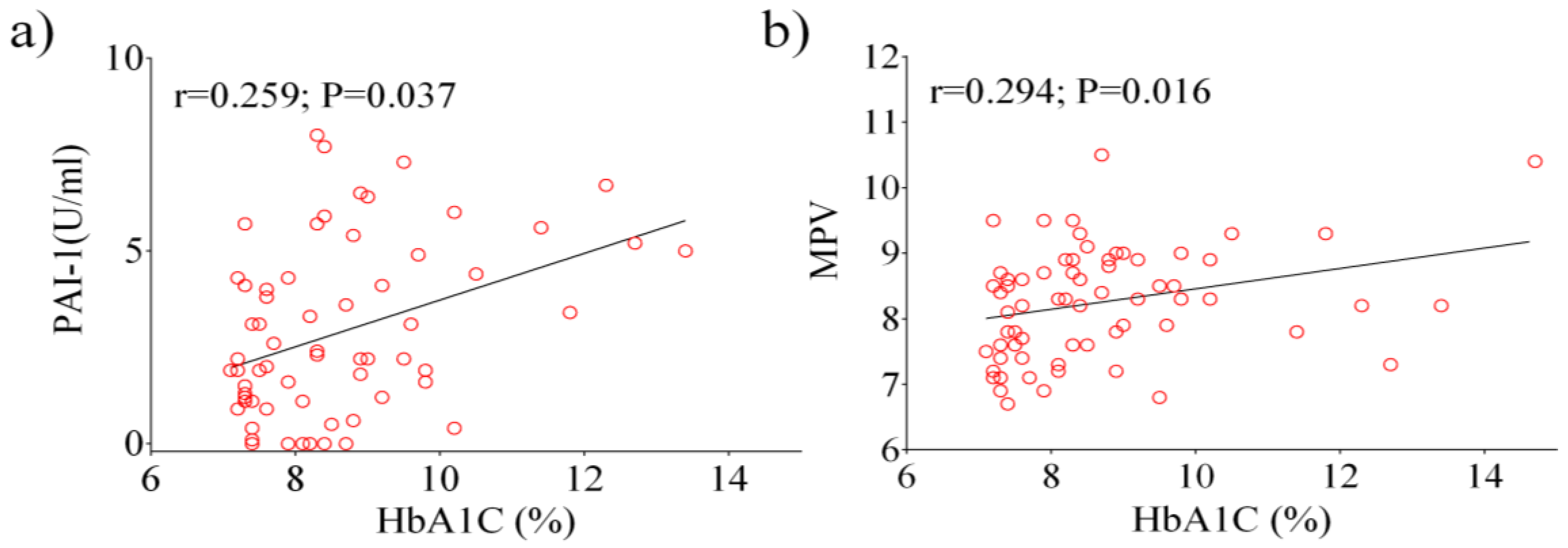
3.3. Correlation Analyses between Glycemic Control and other Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fox, C.S.; Coady, S.; Sorlie, P.D.; Levy, D.; Meigs, J.B.; D’Agostino, R.B., Sr.; Wilson, P.; Savage, P.J. Trends in cardiovascular complications of diabetes. JAMA 2004, 292, 2495–2499. [Google Scholar] [CrossRef] [PubMed]
- Carr, M.E. Diabetes mellitus: A hypercoagulable state. J. Diabetes Complicat. 2001, 15, 44–54. [Google Scholar] [CrossRef]
- Dunn, E.J.; Ariëns, R.A.; Grant, P.J. The influence of type 2 diabetes on fibrin structure and function. Diabetologia 2005, 48, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Paneni, F.; Costantino, S.; Cosentino, F. Insulin resistance, diabetes, and cardiovascular risk. Curr. Atheroscler. Rep. 2014, 16, 419. [Google Scholar] [CrossRef]
- Grant, P.J. Diabetes mellitus as a prothrombotic condition. J. Intern. Med. 2007, 262, 157–172. [Google Scholar] [CrossRef]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef]
- Rask-Madsen, C.; King, G.L. Mechanisms of disease: Endothelial dysfunction in insulin resistance and diabetes. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 46–56. [Google Scholar] [CrossRef]
- Jansson, PA. Endothelial dysfunction in insulin resistance and type 2 diabetes. J. Intern. Med. 2007, 262, 173–183. [Google Scholar] [CrossRef]
- Auwerx, J.; Bouillon, R.; Collen, D.; Geboers, J. Tissue-type plasminogen activator antigen and plasminogen activator inhibitor in diabetes mellitus. Arteriosclerosis 1988, 8, 68–72. [Google Scholar] [CrossRef]
- Simionescu, M. Implications of early structural-functional changes in the endothelium for vascular disease. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 266–274. [Google Scholar] [CrossRef]
- Vaughan, D.E. PAI-1 and atherothrombosis. J. Thromb. Haemost. 2005, 3, 1879–1883. [Google Scholar] [CrossRef]
- Caroleo, M.; Carbone, E.A.; Greco, M.; Corigliano, D.M.; Arcidiacono, B.; Fazia, G.; Rania, M.; Aloi, M.; Gallelli, L.; Segura-Garcia, C.; et al. Brain-Behavior-Immune Interaction: Serum Cytokines and Growth Factors in Patients with Eating Disorders at Extremes of the Body Mass Index (BMI) Spectrum. Nutrients 2019, 11, 1995. [Google Scholar] [CrossRef] [PubMed]
- Dali-Youcef, N.; Mecili, M.; Ricci, R.; Andrés, E. Metabolic inflammation: Connecting obesity and insulin resistance. Ann. Med. 2013, 45, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, D. Type 2 diabetes as an inflammatory cardiovascular disorder. Curr. Mol. Med. 2005, 5, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Stolar, M. Glycemic control and complications in type 2 diabetes mellitus. Am. J. Med. 2010, 123, S3–S11. [Google Scholar] [CrossRef]
- American Diabetes Association. Glycemic targets: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42 (Suppl. 1), S61–S70. [Google Scholar] [CrossRef]
- Accattato, F.; Greco, M.; Pullano, S.A.; Caré, I.; Fiorillo, A.S.; Pujia, A.; Montalcini, T.; Foti, D.P.; Brunetti, A.; Gulletta, E. Effects of acute physical exercise on oxidative stress and inflammatory status in young, sedentary obese subjects. PLoS ONE 2017, 12, e0178900. [Google Scholar] [CrossRef]
- Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; Stampfer, M.; et al. Diabetes mellitus fasting blood glucose concentration and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar]
- Stern, M.P. Diabetes and cardiovascular disease: The “common soil” hypothesis. Diabetes 1995, 44, 369–374. [Google Scholar] [CrossRef]
- Brunetti, A.; Chiefari, E.; Foti, D. Recent advances in the molecular genetics of type 2 diabetes mellitus. World J. Diabetes 2014, 5, 128–140. [Google Scholar] [CrossRef]
- De Rosa, S.; Arcidiacono, B.; Chiefari, E.; Brunetti, A.; Indolfi, C.; Foti, D.P. Type 2 diabetes mellitus and cardiovascular disease: Genetic and epigenetic links. Front. Endocrinol (Lausanne) 2018, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; McGee, D.L. Diabetes and cardiovascular disease. The Framingham study. JAMA 1979, 241, 2035–2038. [Google Scholar] [CrossRef] [PubMed]
- Bansilal, S.; Farkouh, M.E.; Fuster, V. Role of insulin resistance and hyperglycemia in the development of atherosclerosis. Am. J. Cardiol. 2007, 99, 6B–14B. [Google Scholar] [CrossRef] [PubMed]
- Stegenga, M.E.; van der Crabben, S.N.; Levi, M.; de Vos, A.F.; Tanck, M.W.; Sauerwein, H.P.; van der Poll, T. Hyperglycemia stimulates coagulation, whereas hyperinsulinemia impairs fibrinolysis in healthy humans. Diabetes 2006, 55, 1807–1812. [Google Scholar] [CrossRef]
- Pafili, K.; Penlioglou, T.; Mikhailidis, D.P.; Papanas, N. Mean platelet volume and coronary artery disease. Curr. Opin. Cardiol. 2019, 34, 390–398. [Google Scholar] [CrossRef]
- Azad, N.; Agrawal, L.; Emanuele, N.V.; Klein, R.; Bahn, G.D.; McCarren, M.; Reaven, P.; Hayward, R.; Duckworth, W.; VADT Study Group. Association of PAI-1 and fibrinogen with diabetic retinopathy in the Veterans Affairs Diabetes Trial (VADT). Diabetes Care 2014, 37, 501–506. [Google Scholar] [CrossRef]
- Nicholas, S.B.; Aguiniga, E.; Ren, Y.; Kim, J.; Wong, J.; Govindarajan, N.; Noda, N.; Wang, W.; Kawano, Y.; Collis, A.; et al. Plasminogen activator inhibitor-1 deficiency retards diabetic nephropathy. Kidney Int. 2005, 67, 1297–1307. [Google Scholar] [CrossRef]
- Alessi, M.C.; Juhan-Vague, I. Contribution of PAI-1 to cardiovascular pathology. Arch. Mal. Coeur Vaiss. 2004, 97, 673–678. [Google Scholar]
- Meigs, J.B.; Mittleman, M.A.; Nathan, D.M.; Tofler, G.H.; Singer, D.E.; Murphy-Sheehy, P.M.; Lipinska, I.; D’Agostino, R.B.; Wilson, P.W. Hyperinsulinemia. hyperglycemia. and impaired hemostasis: The Framingham Offspring Study. JAMA 2000, 283, 221–228. [Google Scholar] [CrossRef]
- Juhan-Vague, I.; Alessi, M.C.; Mavri, A.; Morange, P.E. Plasminogen activator inhibitor-1. inflammation. obesity. insulin resistance and vascular risk. J. Thromb. Haemost. 2003, 1, 1575–1579. [Google Scholar] [CrossRef]
- Wang, C.C.L.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes—Mechanisms, Management, and Clinical Considerations. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef] [PubMed]
- Lusis, A.J. Atherosclerosis. Nature 2000, 407, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Oishi, Y.; Wakatsuki, T.; Nishikado, A.; Oki, T.; Ito, S. Circulating adhesion molecules and severity of coronary atherosclerosis. Coron. Artery Dis. 2000, 11, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Wautier, J.L.; Wautier, M.P. Blood cells and vascular cell interactions in diabetes. Clin. Hemorheol. Microcirc. 2001, 25, 49–53. [Google Scholar] [PubMed]
- Blüher, M.; Unger, R.; Rassoul, F.; Richter, V.; Paschke, R. Relation between glycaemic control, hyperinsulinaemia and plasma concentrations of soluble adhesion molecules in patients with impaired glucose tolerance or Type II diabetes. Diabetologia 2002, 45, 210–216. [Google Scholar] [CrossRef]
- Ruszkowska-Ciastek, B.; Sokup, A.; Wernik, T.; Ruprecht, Z.; Góralczyk, B.; Góralczyk, K.; Gadomska, D.; Rość, D. Effect of uncontrolled hyperglycemia on levels of adhesion molecules in patients with diabetes mellitus type 2. J. Zhejiang Univ. Sci. B 2015, 16, 355–361. [Google Scholar] [CrossRef]
- Ridker, P.M.; Buring, J.E.; Rifai, N. Soluble P-selectin and the risk of future cardiovascular events. Circulation 2001, 103, 491–495. [Google Scholar] [CrossRef]
- Zalewski, G.; Ciccarone, E.; Di Castelnuovo, A.; Zito, F.; Capani, F.; de Gaetano, G.; Donati, M.B.; Iacoviello, L.; GENDIABE, investigators. P–selectin gene genotypes or haplotypes and cardiovascular complications in type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 418–425. [Google Scholar] [CrossRef]
- Bielinski, S.J.; Berardi, C.; Decker, P.A.; Kirsch, P.S.; Larson, N.B.; Pankow, J.S.; Sale, M.; de Andrade, M.; Sicotte, H.; Tang, W.; et al. P-selectin and subclinical and clinical atherosclerosis: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2015, 240, 3–9. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Nawaz, S.S.; Youssef, A.M.; Al Ghonaim, S.K.; Siddiqui, K. IL-18, VCAM-1 and P-selectin as early biomarkers in mormoalbuminuric Type 2 diabetes patients. Biomark. Med. 2019, 13, 467–478. [Google Scholar] [CrossRef]
- Twig, G.; Afek, A.; Shamiss, A.; Derazne, E.; Tzur, D.; Gordon, B.; Tirosh, A. White blood cells count and incidence of type 2 diabetes in young men. Diabetes Care 2013, 36, 276–282. [Google Scholar] [CrossRef]
- Vozarova, B.; Weyer, C.; Lindsay, R.S.; Pratley, R.E.; Bogardus, C.; Tataranni, P.A. High white blood cell count is associated with a worsening of insulin sensitivity and predicts the development of type 2 diabetes. Diabetes 2002, 51, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Lou, M.; Luo, P.; Tang, R.; Peng, Y.; Yu, S.; Huang, W.; He, L. Relationship between neutrophil-lymphocyte ratio and insulin resistance in newly diagnosed type 2 diabetes mellitus patients. BMC Endocr. Disord. 2015, 15, 9. [Google Scholar] [CrossRef] [PubMed]
- Shiny, A.; Bibin, Y.S.; Shanthirani, C.S.; Regin, B.S.; Anjana, R.M.; Balasubramanyam, M.; Jebarani, S.; Mohan, V. Association of neutrophil-lymphocyte ratio with glucose intolerance: An indicator of systemic inflammation in patients with type 2 diabetes. Diabetes Technol. Ther. 2014, 16, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Sen, N.; Afsar, B.; Ozcan, F.; Buyukkaya, E.; Isleyen, A.; Akcay, A.B.; Yuzgecer, H.; Kurt, M.; Karakas, M.F.; Basar, N.; et al. The neutrophil to lymphocyte ratio was associated with impaired myocardial perfusion and long term adverse outcome in patients with ST-elevated myocardial infarction undergoing primary coronary intervention. Atherosclerosis 2013, 228, 203–210. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control | T2DM | p | |
|---|---|---|---|
| N | 41 (13♀–28♂) | 41 (22♀–19♂) | |
| Age (yrs) | 51 ± 7.55 | 54 ± 5.10 | 0.95 |
| Fasting glucose (mg/dL) | 89 ± 4.86 | 161 ± 47.01 | <0.0001 |
| HbA1c (%) | 5.4 ± 0.2 | 7.3 ± 1.5 | <0.0001 |
| Hemostasis and platelet parameters | |||
| PT (%) | 98.22 ± 8.54 | 105.49 ± 8.35 | <0.0001 |
| aPTT (s) | 27.02 ± 2.56 | 26.76 ± 7.28 | 0.824 |
| Fibrinogen (mg/dL) | 297.51 ± 65.04 | 312.79 ± 74.62 | 0.345 |
| PAI-1 (IU/mL) | 2.02 ± 2.20 | 3 ± 1.7 | 0.040 |
| PLT (10^3 /μL) | 238.37 ± 67.18 | 247.49 ± 65.56 | 0.536 |
| MPV (fl) | 7.88 ± 0.69 | 8.12 ± 0.83 | 0.232 |
| Adhesion molecules | |||
| VCAM–1 (ng/mL) | 290 ± 193.93 | 384 ± 191.36 | 0.040 |
| ICAM–1 (ng/mL) | 245 ± 116.69 | 282 ± 142.31 | 0.232 |
| E-selectin (ng/mL) | 13 ± 11.62 | 15 ± 8.45 | 0.381 |
| P-selectin(ng/mL) | 65 ± 45.49 | 65 ± 33.21 | 0.960 |
| L-selectin (ng/mL) | 839 ± 340.13 | 963 ± 415.97 | 0.206 |
| WBC and differential count | |||
| WBC (10^3/μL) | 6.4 ± 1.4 | 7.6 ± 2.4 | 0.009 |
| Neutrophils (10^3/μL) | 3.6 ± 0.9 | 4.4 ± 1.7 | 0.008 |
| Lymphocytes (10^3/μL)) | 2.1 ± 0.4 | 2.4 ± 0.9 | 0.082 |
| NLR | 1.7 ± 0.4 | 2.0 ± 0.8 | 0.067 |
| HbA1c < 7% | HbA1c ≥ 7% | p | |
|---|---|---|---|
| N | 58 (30♀–28♂) | 75 (41♀–34♂) | |
| Age (yrs) | 64.63 ± 10.9 | 66.43 ± 10.4 | 0.340 |
| Fasting glucose (mg/dL) | 126.89 ± 20.9 | 181.04 ± 66.4 | <0.0001 |
| HbA1c (%) | 6.2 ± 0.4 | 8.5 ± 1.6 | <0.0001 |
| Hemostasis and platelet parameters | |||
| PT (%) | 99.37 ± 13.5 | 104.10 ± 8.2 | 0.015 |
| aPTT (s) | 26.51 ± 3.2 | 25.89 ± 5.8 | 0.474 |
| Fibrinogen (mg/dL) | 333.19 ± 97.2 | 338.75 ± 86.7 | 0.739 |
| PAI–1 (IU/mL) | 2.23 ± 1.8 | 2.79 ± 2.1 | 0.125 |
| PLT (10^3/μL) | 232.43 ± 70.6 | 235.76 ± 56.6 | 0.764 |
| MPV (fl) | 8.12 ± 0.9 | 8.17 ± 0.9 | 0.750 |
| Adhesion molecules | |||
| VCAM-1 (ng/mL) | 458.07 ± 371.0 | 451.99 ± 236.4 | 0.909 |
| ICAM-1 (ng/mL) | 277.9 ± 140.9 | 274.11 ± 133.6 | 0.877 |
| E–selectin (ng/mL) | 12.42 ± 8.4 | 18.36 ± 15.2 | 0.009 |
| P–selectin (ng/mL) | 52.64 ± 34.1 | 70.08 ± 42.4 | 0.012 |
| L–selectin (ng/mL) | 921.54 ± 361.9 | 1008.97 ± 463.80 | 0.282 |
| WBC and differential count | |||
| WBC (10^3/μL) | 7.48 ± 2.1 | 7.61 ± 2.2 | 0.746 |
| Neutrophils (10^3/μL) | 4.20 ± 1.5 | 4.60 ± 1.8 | 0.173 |
| Lymphocytes (10^3/μL) | 2.45 ± 1.1 | 2.17 ± 0.7 | 0.082 |
| NLR | 1.90 ± 0.8 | 2.28 ± 0.97 | 0.019 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palella, E.; Cimino, R.; Pullano, S.A.; Fiorillo, A.S.; Gulletta, E.; Brunetti, A.; Foti, D.P.; Greco, M. Laboratory Parameters of Hemostasis, Adhesion Molecules, and Inflammation in Type 2 Diabetes Mellitus: Correlation with Glycemic Control. Int. J. Environ. Res. Public Health 2020, 17, 300. https://doi.org/10.3390/ijerph17010300
Palella E, Cimino R, Pullano SA, Fiorillo AS, Gulletta E, Brunetti A, Foti DP, Greco M. Laboratory Parameters of Hemostasis, Adhesion Molecules, and Inflammation in Type 2 Diabetes Mellitus: Correlation with Glycemic Control. International Journal of Environmental Research and Public Health. 2020; 17(1):300. https://doi.org/10.3390/ijerph17010300
Chicago/Turabian StylePalella, Eleonora, Rossella Cimino, Salvatore A. Pullano, Antonino S. Fiorillo, Elio Gulletta, Antonio Brunetti, Daniela P. Foti, and Marta Greco. 2020. "Laboratory Parameters of Hemostasis, Adhesion Molecules, and Inflammation in Type 2 Diabetes Mellitus: Correlation with Glycemic Control" International Journal of Environmental Research and Public Health 17, no. 1: 300. https://doi.org/10.3390/ijerph17010300
APA StylePalella, E., Cimino, R., Pullano, S. A., Fiorillo, A. S., Gulletta, E., Brunetti, A., Foti, D. P., & Greco, M. (2020). Laboratory Parameters of Hemostasis, Adhesion Molecules, and Inflammation in Type 2 Diabetes Mellitus: Correlation with Glycemic Control. International Journal of Environmental Research and Public Health, 17(1), 300. https://doi.org/10.3390/ijerph17010300