Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study





Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Data Collection Instruments
2.3.1. Primary Outcome
2.3.2. Secondary Outcomes
2.4. Procedures
2.5. Statistical Analyses
3. Results
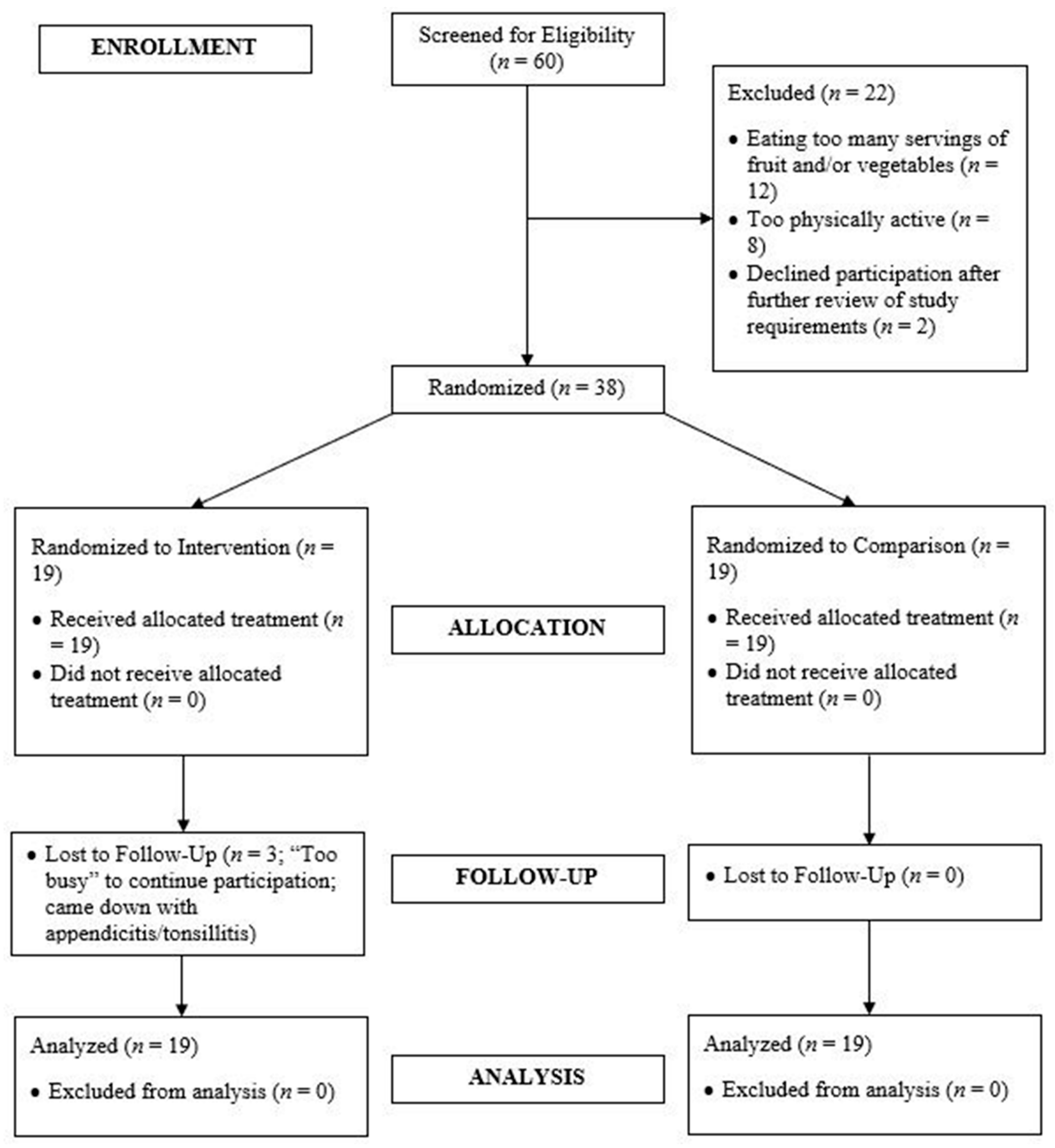
3.1. Participant Flow
3.2. Primary Outcome
Intervention Interest, Use/Acceptability, Adherence, and Retention
3.3. Secondary Outcomes
3.3.1. Physical Activity
3.3.2. Physiological Outcomes
3.3.3. Psychosocial Outcomes
3.3.4. Dietary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Deliens, T.; Deforche, B.; De Bourdeaudhuij, I.; Clarys, P. Determinants of physical activity and sedentary behaviour in university students: A qualitative study using focus group discussions. BMC Public Health 2015, 15. [Google Scholar] [CrossRef]
- Desai, M.; Miller, W.; Staples, B.; Bravender, T. Risk Factors Associated With Overweight and Obesity in College Students. J. Am. Coll. Health 2008, 57, 109–114. [Google Scholar] [PubMed]
- Peterson, N.; Sirard, J.; Kulbok, P.; DeBoer, M.; Erickson, J. Sedentary behavior and physical activity of young adult university students. Res. Nurs. Health 2018, 41, 30–38. [Google Scholar] [PubMed]
- Larson, N.; Neumark-Sztainer, D.; Story, M.; Burgess-Champoux, T. Whole-Grain Intake Correlates among Adolescents and Young Adults: Findings from Project EAT. J. Am. Diet. Assoc. 2010, 110, 230–237. [Google Scholar] [PubMed]
- Racette, S.; Deusinger, S.; Strube, M.; Highstein, G.; Deusinger, R. Weight changes, exercise, and dietary patterns during freshman and sophmore years of college. J. Am. Coll. Health 2005, 53, 245–251. [Google Scholar] [PubMed]
- Giskes, K.; van Lenthe, F.; Avendano-Pabon, M.; Brug, J. A systematic review of environmental factors and obesogenic dietary intakes among adults: Are we getting closer to understanding obesogenic environments? Obes. Rev. 2011, 12, e95–e106. [Google Scholar] [PubMed]
- Malhotra, R.; Østbye, T.; Riley, C.; Finkelstein, E. Young adult weight trajectories through midlife by body mass category. Obesity 2013, 21, 1923–1934. [Google Scholar] [CrossRef]
- Cawley, J.; Meyerhoefer, C. The medical care costs of obesity: An instrumental variables approach. J. Health Econ. 2012, 31, 219–230. [Google Scholar] [CrossRef]
- Welch, V.; Petkovic, J.; Simeon, R.; Presseau, J.; Gagnon, D.; Hossain, A.; Pardo Pardo, J.; Pottie, K.; Rader, T.; Sokolovski, A.; et al. Interactive social media interventions for health behaviour change, health outcomes, and health equity in the adult population (protocol). Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Partridge, S.; Redfern, J. Obesity prevention in young people: The role of technology in primary care. J. Prim. Care Gen. Pract. 2018, 2. Available online: https://scientonline.org/open-access/obesity-prevention-in-young-people-the-role-of-technology-in-primary-care.pdf (accessed on 19 September 2019).
- Henriksen, A.; Mikalsen, M.; Woldaregay, A.; Muzny, M.; Hartvigsen, G.; Sanders, J.; Wark, P.; Winfree, K.; Fallahzadeh, R.; Fernández, C.; et al. Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer Wrist-Worn Wearables. J. Med. Internet Res. 2018, 20, e110. [Google Scholar] [CrossRef]
- Muller, A.; Maher, C.; Vandelanotte, C.; Hingle, M.; Middelweerd, A.; Lopez, M.L.; Desmet, A.; Short, C.E.; Bardus, M.; Hand, R.; et al. Physical Activity, Sedentary Behavior, and Diet-Related eHealth and mHealth Research: Bibliometric Analysis. J. Med. Internet Res. 2018, 20, e122. [Google Scholar] [CrossRef] [PubMed]
- Schembre, S.; Liao, Y.; Robertson, M.; Dunton, G.F.; Kerr, J.; E Haffey, M.; Burnett, T.; Basen-Engquist, K.; Turner-McGrievy, B.; Gomez, I.N.; et al. Just-in-Time Feedback in Diet and Physical Activity Interventions: Systematic Review and Practical Design Framework. J. Med. Internet Res. 2018, 20, e106. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Gao, Z. Health Wearable Devices and Physical Activity Promotion. In Technology in Physical Activity and Health Promotion; Gao, Z., Ed.; Routledge Publishers: London, UK, 2017; pp. 148–164. [Google Scholar]
- Kim, Y.; Lumpkin, A.; Lochbaum, M.; Stegemeier, S.; Kitten, K. Promoting physical activity using wearable activity tracker in college students: A cluster randomized trial. J. Sport Sci. 2018, 36, 1889–1896. [Google Scholar] [CrossRef] [PubMed]
- Melton, B.; Buman, M.; Vogel, R.; Harris, B.; Bigham, L. Wearable devices to improve physical activity and sleep: A randomized controlled trial of college-aged African American women. J. Black Stud. 2016, 47, 610–625. [Google Scholar]
- Thorndike, A.; Mills, S.; Sonnenberg, L.; Palakshappa, D.; Gao, T.; Pau, C.T.; Regan, S. Activity Monitor Intervention to Promote Physical Activity of Physicians-In-Training: Randomized Controlled Trial. PLoS ONE 2014, 9, e100251. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cadmus-Bertram, L.; Natarajan, L.; White, M.M.; Madanat, H.; Nichols, J.F.; Ayala, G.X.; Pierce, J.P. Wearable sensor/device (fitbit one) and SMS text-messaging prompts to increase physical activity in overweight and obese adults: A randomized controlled trial. Telemed. E-Health 2015, 21, 782–792. [Google Scholar] [CrossRef]
- Thompson, W.; Kuhle, C.; Koepp, G.; McCrady-Spitzer, S.; Levine, J. “Go4Life” exercise counseling, accelerometer feedback, and activity levels in older people. Arch. Gerontol. Geriatr. 2014, 58, 314–319. [Google Scholar] [CrossRef]
- Cadmus-Bertram, L.; Marcus, B.; Patterson, R.; Parker, B.; Morey, B. Randomized Trial of a Fitbit-Based Physical Activity Intervention for Women. Am. J. Prev. Med. 2015, 49, 414–418. [Google Scholar] [CrossRef]
- Elliot, C.; Hamlin, M. Combined diet and physical activity is better than diet or physical activity alone at improving health outcomes for patients in New Zealand’s primary care intervention. BMC Public Health 2018, 18, 230. [Google Scholar] [CrossRef]
- Pew Research Center. Social Media Fact Sheet. 2017. Available online: http://www.pewinternet.org/fact-sheet/social-media/ (accessed on 19 December 2018).
- Cavallo, D.; Tate, D.; Ries, A.; Brown, J.; DeVellis, R.; Ammerman, A. A social-media based physical activity intervention: A randomized controlled trial. Am. J. Prev. Med. 2012, 43, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Bunn, J.; Navalta, J.; Fountaine, C.; Reece, J. Current State of Commercial Wearable Technology in Physical Activity Monitoring 2015–2017. Int. J. Exerc. Sci. 2018, 11, 503–515. [Google Scholar] [PubMed]
- National Wellness Institute. The Six Dimensions of Wellness. 2018. Available online: http://www.nationalwellness.org/?page=Six_Dimensions (accessed on 31 March 2018).
- Kohl, H., III; Murray, T. Program and policy evaluation for physical activity and public health. In Foundations of Physical Activity and Public Health; Kohl, H., III, Murray, T., Eds.; Human Kinetics: Champaign, IL, USA, 2012; pp. 241–256. [Google Scholar]
- Matthews, C.; Hagströmer, M.; Pober, D.; Bowles, H. Best practices for using physical activity monitors in population-based research. Med. Sci. Sports Exerc. 2012, 44 (Suppl. S1), S68–S76. [Google Scholar] [PubMed]
- Brug, J.; Oenema, A.; Ferreira, I. Theory, evidence, and intervention mapping to improve behavior, nutrition, and physical activity interventions. Int. J. Behav. Nutr. Phys. 2005, 2, 2. [Google Scholar]
- Patten, M. The role of theory in research. In Understanding Research Methods: An overview of the Essentials, 9th ed.; Patten, M., Ed.; Pyrczak Publishing: Glendale, CA, USA, 2014; pp. 27–29. [Google Scholar]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [PubMed]
- Sriramatr, S.; Silalertdetkul, S.; Wachirathanin, P. Social cognitive theory associated with physical activity in undergraduate students: A cross-sectional study. Pac. Rim Int. J. Nurs. Res. 2016, 20, 95–105. [Google Scholar]
- Mirzaei-Alavijeh, M.; Soroush, A.; Nasirzadeh, M.; Hatamzadeh, N.; Zinat-Motlagh, F.; Jalilian, F.; Mohammadi, M.; Mahboubi, M. Socio-Cognitive Determinants of Regular Physical Activity among College Students. World Fam. Med. 2018, 16, 158–162. [Google Scholar]
- Marr, J.; Wilcox, S. Self-efficacy and Social Support Mediate the Relationship Between Internal Health Locus of Control and Health Behaviors in College Students. Am. J. Health Educ. 2015, 46, 122–131. [Google Scholar]
- Farmanbar, R.; Niknami, S.; Lubans, D.; Hidarnia, A. Predicting exercise behaviour in Iranian college students: Utility of an integrated model of health behaviour based on the transtheoretical model and self-determination theory. Health Educ. J. 2013, 72, 56–69. [Google Scholar]
- Phillips, L.; Chamberland, P.-E.; Hekler, E.; Abrams, J.; Eisenberg, M. Intrinsic rewards predict exercise via behavioral intentions for initiators but via habit strength for maintainers. Sport Exerc. Perform. 2016, 5, 352–364. [Google Scholar] [CrossRef]
- National Center of Complementary and Integrative Health. Pilot Studies: Common Uses and Misuses. 2017. Available online: https://nccih.nih.gov/grants/whatnccihfunds/pilot_studies (accessed on 16 June 2019).
- Leon, A.; Davis, L.; Kraemer, H. The role and interpretation of pilot studies in clinical research. J. Psychiatr. Res. 2011, 45, 626–629. [Google Scholar] [PubMed]
- Schulz, K.; Altman, D.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; Department of Health and Human Services: Washington, DC, USA, 2018.
- U.S. Department of Agriculture. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. 2015. Available online: http://health.gov/dietaryguidelines/2015-scientific-report/pdfs/scientific-report-of-the-2015-dietary-guidelines-advisory-committee.pdf (accessed on 8 April 2018).
- Thompson, F.; Subar, A.; Smith, A.; Midthune, D.; Radimer, K.L.; Kahle, L.L.; Kipnis, V. Fruit and vegetable assessment: Performance of 2 new short instruments and a food frequency questionnaire. J. Am. Diet. Assoc. 2002, 102, 1764–1772. [Google Scholar] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. 2018. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 20 April 2018).
- Ayabe, M.; Junichiro, A.; Kumahara, H.; Tanaka, H. Assessment of minute-by-minute stepping rate of physical activity under free-living conditions in female adults. Gait Posture 2011, 34, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Camhi, S.; Leonardi, C.; Johnson, W.D.; Katzmarzyk, P.T.; Earnest, C.P.; Church, T.S. Patterns of adult stepping cadence in the 2005–2006 NHANES. Prev. Med. 2011, 53, 178–181. [Google Scholar] [PubMed]
- Herrmann, S.; Barreira, T.; Kang, M.; Ainsworth, B. How many hours are enough? Accelerometer wear time may provide bias in daily activity estimates. J. Phys. Act. Health 2013, 10, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.; McIver, K.; Pate, R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sport Exerc. 2005, 37 (Suppl. S11), S531–S543. [Google Scholar]
- Golding, L.; Meyers, C.; Sinning, W. Y’s Way to Physical Fitness: The Complete Guide to Fitness Testing and Instruction, 4th ed.; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Aandstad, A.; Holtberget, K.; Hageberg, R.; Holme, I.; Anderssen, S. Validity and Reliability of Bioelectrical Impedance Analysis and Skinfold Thickness in Predicting Body Fat in Military Personnel. Mil. Med. 2014, 179, 208–217. [Google Scholar] [PubMed]
- Carlson, J.; Sallis, J.; Wagner, N.; Calfas, K.J.; Patrick, K.; Groesz, L.M.; Norman, G.J. Brief physical activity-related psychosocial measures: Reliability and construct validity. J. Phys. Act. Health 2012, 9, 1178–1186. [Google Scholar] [CrossRef]
- Ommundsen, Y.; Page, A.; Po-Wen, K.; Cooper, A. Cross-cultural, age and gender validation of a computerised questionnaire measuring personal, social and environmental associations with children’s physical activity: The European Youth Heart Study. Int. J. Behav. Nutr. Phys. 2008, 5, 29. [Google Scholar] [CrossRef]
- Trost, S.; Pate, R.; Saunders, R.; Ward, D.; Dowda, M.; Felton, G. A Prospective Study of the Determinants of Physical Activity in Rural Fifth-Grade Children. Prev. Med. 1997, 26, 257–263. [Google Scholar] [PubMed]
- Sechrist, K.; Walker, S.; Pender, N. Development and psychometric evaluation of the exercise benefits/barriers scale. Res. Nurs. Health 1987, 10, 357–365. [Google Scholar]
- Gesell, S.; Reynolds, E.; Ip, E.; Fenlason, L.C.; Pont, S.J.; Poe, E.K.; Barkin, S.L. Social influences of self-reported physical activity in Latino children. Clin. Pediatr. 2008, 47, 797–802. [Google Scholar]
- Saunders, R.; Pate, R.; Felton, G.; Dowda, M.; Weinrich, M.C.; Ward, D.S.; Parsons, M.A.; Baranowski, T. Development of Questionnaires to Measure Psychosocial Influences on Children’s Physical Activity. Prev. Med. 1997, 26, 241–247. [Google Scholar] [PubMed]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Duncan, T.; Tammen, V. Psychometric properties of the intrinsic motivation inventory in a competitive sport setting: A confirmatory factor analysis. Res. Q. Exerc. Sport 1987, 60, 48–58. [Google Scholar]
- Kipnis, V.; Subar, A.; Midthune, D.; Freedman, L.S.; Ballard-Barbash, R.; Troiano, R.P.; Bingham, S.; Schoeller, D.A.; Schatzkin, A.; Carroll, R.J. Structure of dietary measurement error: Results of the OPEN biomarker study. Am. J. Epidemiol. 2003, 158, 14–21. [Google Scholar]
- Moshfegh, A.; Rhodes, D.; Baer, D.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; A Ingwersen, L.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar]
- Baranowski, T. 24-hour recall and diet record methods. In Nutritional Epidemiology, 3rd ed.; Willett, W., Ed.; Oxford University Press: New York, NY, USA, 2013; pp. 49–69. [Google Scholar]
- Willett, W. Nature of variation in diet. In Nutritional Epidemiology, 3rd ed.; Willet, W., Ed.; Oxford University Press: New York, NY, USA, 2013; pp. 34–48. [Google Scholar]
- Wang, Y.; Bleich, S.; Gortmaker, S. Increasing Caloric Contribution From Sugar-Sweetened Beverages and 100% Fruit Juices Among US Children and Adolescents, 1988–2004. Pediatrics 2008, 121, e1604–e1614. [Google Scholar] [CrossRef]
- Popkin, B.; E Armstrong, L.; Bray, G.; Caballero, B.; Frei, B.; Willett, W. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 29–42. [Google Scholar]
- Arem, H.; Moore, S.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [PubMed]
- Smetaniuk, T.; Johnson, D.; Creurer, J.; Block, K.; Schlegel, M.; Butcher, S.; Oosman, S.N. Physial activity and sedentary behaviour of master of physical therapy students: An exploratory study of facilitators and barriers. Physiother. Can. 2017, 69, 260–270. [Google Scholar]
- Bopp, M.; Bopp, C.; Schuchert, M. Active transportation to and on campus is associated with objectively measured fitness outcomes among college students. J. Phys. Act. Health 2013, 12, 418–423. [Google Scholar]
- Sisson, S.; Tudor-Locke, C. Comparison of cyclists’ and motorists’ utilitarian physical activity at an urban university. Prev. Med. 2008, 46, 77–79. [Google Scholar] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M.; Lancet Physical Activity Series 2 Executive Committee; Lancet Sedentary Behaviour Working Group. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar]
- De Vos, P.; Hanck, C.; Neisingh, M.; Prak, D.; Groen, H.; Faas, M. Weight gain in freshman college students and perceived health. Prev. Med. Rep. 2015, 2, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-C.; Li, C.-I.; Lin, W.-Y.; Liu, C.-S.; Hsu, H.-S.; Lee, C.-C.; Chen, F.-N.; Li, T.-C.; Lin, C.-C. Percentage of Body Fat Assessment Using Bioelectrical Impedance Analysis and Dual-Energy X-ray Absorptiometry in a Weight Loss Program for Obese or Overweight Chinese Adults. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- Kenney, W.; Wilmore, J.; Costill, D. Body composition and nutrition for sport. In Physiology of Sport and Exercise, 6th ed.; Kenney, W., Wilmore, J., Costill, D., Eds.; Human Kinetics: Champaign, IL, USA, 2015; pp. 371–405. [Google Scholar]
- Kenney, W.; Wilmore, J.; Costill, D. Adaptations to aerobic and anaerobic training. In Physiology of Sport and Exercise, 6th ed.; Kenney, W., Wilmore, J., Costill, D., Eds.; Human Kinetics: Champaign, IL, USA, 2015; pp. 261–291. [Google Scholar]
- Von, A.D.; Ebert, S.; Ngamvitroj, A.; Park, N.; Kang, D.-H. Predictors of health behaviors in college students. J. Adv. Nurs. 2004, 48, 463–474. [Google Scholar]
- Voorhees, C. Personal, social, and physical environmental correlates of physical activity levels in urban Latinas. Am. J. Prev. Med. 2003, 25, 61–68. [Google Scholar]
- Farren, G.; Zhang, T.; Martin, S.; Thomas, K. Factors related to metting physical activity guidelines in active college students: A social cognitive perspective. J. Am. Coll. Health 2017, 65, 10–21. [Google Scholar]
- Blake, H.; Stanulewicz, N.; McGill, F. Predictors of physical activity and barriers to exercise in nursing and medical students. J. Adv. Nurs. 2017, 73, 917–929. [Google Scholar] [PubMed]
- Grubbs, L.; Carter, J. The Relationship of Perceived Benefits and Barriers to Reported Exercise Behaviors in College Undergraduates. Fam. Community Health 2002, 25, 76–84. [Google Scholar] [PubMed]
- Kohl, H., III; Murray, T. Overweight and obesity. In Foundations of Physical Activity and Public Health; Kohl, H., III, Murray, T., Eds.; Human Kinetics: Champaign, IL, USA, 2012; pp. 95–117. [Google Scholar]
- Poddar, K.; Hosig, K.; Anderson, E.; Nickols-Richardson, S.; Duncan, S. Web-Based Nutrition Education Intervention Improves Self-Efficacy and Self-Regulation Related to Increased Dairy Intake in College Students. J. Am. Acad. Nutr. Diet. 2010, 110, 1723–1727. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Comments | |
|---|---|
| Positive Features |
|
| Negative Features |
|
| Experimental (n = 19) | Comparison (n = 19) | p-Value | |
|---|---|---|---|
| Demographic and Anthropometric Variables | |||
| Sex | |||
| Female | 15 | 13 | 0.71 |
| Male | 4 | 6 | |
| Race/Ethnicity | |||
| Non-Hispanic White | 16 | 11 | 0.20 |
| Asian | 3 | 8 | |
| Age [years] | 21.2 (4.0) | 21.8 (2.8) | 0.58 |
| Height [cm] | 171.5 (3.9) | 170.0 (8.2) | 0.48 |
| Weight [kg] | 73.4 (11.3) | 69.0 (15.8) | 0.33 |
| Body Mass Index | 24.9 (3.3) | 23.8 (4.6) | 0.39 |
| Physiological Variables | |||
| Body Fat Percentage | 27.7 (8.0) | 26.4 (7.0) | 0.61 |
| Cardiorespiratory Fitness [BPM] | 104.2 (19.1) | 112.5 (22.7) | 0.23 |
| Physical Activity Variables | |||
| MVPA/Day [min] | 6.1 (7.0) | 5.8 (5.9) | 0.90 |
| LPA/Day [min] | 180.7 (30.7) | 161.6 (50.8) | 0.17 |
| SB/Day [min] | 534.7 (30.3) | 553.6 (50.3) | 0.18 |
| Psychosocial Variables | |||
| Self-Efficacy | 2.3 (0.4) | 2.2 (0.8) | 0.78 |
| Social Support | 2.1 (0.5) | 2.2 (0.9) | 0.69 |
| Enjoyment | 2.4 (0.4) | 2.3 (0.5) | 0.57 |
| Barriers | 27.2 (5.0) | 30.0 (5.7) | 0.11 |
| Outcome Expectancy | 9.9 (1.8) | 9.5 (2.3) | 0.53 |
| Intrinsic Motivation | 4.5 (1.0) | 4.5 (1.3) | 0.89 |
| Dietary Variables | |||
| Daily Caloric Consumption [cals] | 1986 (461.9) | 1953 (526.5) | 0.84 |
| Daily Fruit Intake [cups] | 0.8 (0.5) | 0.8 (0.7) | 0.73 |
| Daily Vegetable Intake [cups] | 1.5 (0.7) | 1.3 (0.7) | 0.48 |
| Daily Whole Grain Intake [oz. equivalents] | 1.2 (0.9) | 0.6 (0.7) | 0.03 |
| Daily Sugar-Sweetened Beverage Kcalories | 110.1 (32.5) | 128.0 (42.9) | 0.48 |
| Group | Baseline | 6 Weeks | % Change at 6 Weeks | 12 Weeks | % Change at 12 Weeks | |
|---|---|---|---|---|---|---|
| Physical Activity Outcomes | ||||||
| MVPA/Day [min] | Experimental | 6.1 (7.0) | 10.3 (6.5) | 173.1 (225.2) | 8.1 (5.6) | 110.7 (194.8) |
| Comparison | 5.8 (5.9) | 7.4 (5.3) | 134.4 (212.2) | 6.7 (6.1) | 44.6 (124.5) | |
| LPA/Day [min] | Experimental | 180.7 (30.7) | 162.4 (30.3) | −8.1 (21.0) | 164.2 (43.1) | −6.9 (25.4) |
| Comparison | 161.6 (50.8) | 166.1 (63.7) | 6.1 (32.8) | 175.5 (51.2) | 16.3 (42.8) | |
| SB/Day [min] | Experimental | 534.7 (30.3) | 549.0 (29.2) | 2.9 (7.4) | 548.7 (44.6) | 2.9 (10.0) |
| Comparison | 553.6 (50.3) | 559.9 (52.4) | 1.5 (9.5) | 538.9 (50.3) | −2.1 (10.6) | |
| Dietary Outcomes | ||||||
| Daily Kcaloric Consumption [cals] | Experimental | 1986.1 (461.9) | 1971.7 (553.4) | −0.1 (21.4) | 1945.1 (569.6) | −0.9 (23.7) |
| Comparison | 1953.4 (526.5) | 1935.3 (478.0) | −0.9 (23.6) | 1810.1 (512.6) | −4.6 (22.2) | |
| Daily Fruit Intake [cups] | Experimental | 0.8 (0.5) | 0.8 (0.5) | 31.6 (130.6) | 1.0 (0.9) | 36.7 (157.5) |
| Comparison | 0.8 (0.7) | 0.6 (1.6) | −7.3 (99.6) | 0.6 (0.7) | −7.0 (97.0) | |
| Daily Vegetable Intake | Experimental | 1.5 (0.7) | 1.3 (0.7) | 20.1 (118.9) | 1.3 (0.5) | 14.5 (22.0) |
| Comparison | 1.3 (0.7) | 1.7 (1.0) | 64.0 (104.7) | 1.0 (0.6) | −0.7 (85.9) | |
| Daily Whole Grain Intake [oz. equivalents] | Experimental | 1.2 (0.9) | 1.1 (0.8) | 29.4 (132.6) | 1.1 (0.9) | 9.8 (89.6) |
| Comparison | 0.6 (0.7) | 1.0 (0.9) | 110.0 (189.0) | 0.8 (1.0) | 93.0 (188.0) | |
| Daily SSB Consumption Calories | Experimental | 110.1 (32.5) | 279.6 (137.7) | 179.9 (166.2) | 147.8 (99.3) | 47.1 (109.0) |
| Comparison | 128.0 (42.9) | 136.8 (115.3) | 1.7 (60.2) | 110.8 (47.8) | −7.5 (49.1) | |
| Group | Baseline | 12 Weeks | % Change at 12 Weeks | |
|---|---|---|---|---|
| Physiological Outcomes | ||||
| Weight [kg] | Experimental | 73.4 (11.3) | 72.9 (9.0) | −0.2 (5.7) |
| Comparison | 69.0 (15.8) | 68.5 (14.7) | −0.5 (2.5) | |
| Body Fat Percentage | Experimental | 27.7 (8.0) | 29.8 (6.4) | 11.1 (17.5) |
| Comparison | 26.4 (7.0) | 26.7 (7.2) | 1.7 (8.0) | |
| Cardiorespiratory Fitness [BPM] | Experimental | 104.2 (19.1) | 106.0 (16.9) | 2.6 (9.2) |
| Comparison | 112.5 (22.7) | 109.2 (20.6) | −2.0 (12.1) | |
| Psychosocial Outcomes | ||||
| Self-Efficacy | Experimental | 2.3 (0.4) | 3.0 (0.5) | 33.7 (29.3) |
| Comparison | 2.2 (0.8) | 2.7 (0.9) | 28.7 (63.6) | |
| Social Support | Experimental | 2.1 (0.5) | 2.8 (0.7) | 36.5 (47.3) |
| Comparison | 2.2 (0.9) | 2.5 (1.1) | 19.0 (54.6) | |
| Enjoyment | Experimental | 2.4 (0.4) | 2.5 (0.3) | 9.3 (24.0) |
| Comparison | 2.3 (0.6) | 2.4 (0.5) | 5.7 (16.3) | |
| Barriers | Experimental | 27.2 (5.0) | 26.1 (4.0) | −1.7 (22.1) |
| Comparison | 30.0 (5.7) | 28.0 (5.0) | −4.5 (21.0) | |
| Outcome Expectancy | Experimental | 9.9 (1.8) | 10.5 (1.3) | 8.3 (16.0) |
| Comparison | 9.5 (2.3) | 9.8 (2.1) | 7.7 (29.5) | |
| Intrinsic Motivation | Experimental | 4.5 (1.0) | 5.0 (1.1) | 13.7 (16.7) |
| Comparison | 4.5 (1.3) | 5.0 (1.4) | 12.3 (24.6) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pope, Z.C.; Barr-Anderson, D.J.; Lewis, B.A.; Pereira, M.A.; Gao, Z. Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 3579. https://doi.org/10.3390/ijerph16193579
Pope ZC, Barr-Anderson DJ, Lewis BA, Pereira MA, Gao Z. Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study. International Journal of Environmental Research and Public Health. 2019; 16(19):3579. https://doi.org/10.3390/ijerph16193579
Chicago/Turabian StylePope, Zachary C., Daheia J. Barr-Anderson, Beth A. Lewis, Mark A. Pereira, and Zan Gao. 2019. "Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study" International Journal of Environmental Research and Public Health 16, no. 19: 3579. https://doi.org/10.3390/ijerph16193579
APA StylePope, Z. C., Barr-Anderson, D. J., Lewis, B. A., Pereira, M. A., & Gao, Z. (2019). Use of Wearable Technology and Social Media to Improve Physical Activity and Dietary Behaviors among College Students: A 12-Week Randomized Pilot Study. International Journal of Environmental Research and Public Health, 16(19), 3579. https://doi.org/10.3390/ijerph16193579