The Effects of Diet and Dietary Interventions on the Quality of Life among Breast Cancer Survivors: A Cross-Sectional Analysis and a Systematic Review of Experimental Studies

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Cross-Sectional Study
2.1.1. Study Design
2.1.2. Dietary Assessment
2.1.3. Assessment of Quality of Life
2.1.4. Statistical Analysis
2.2. Systematic Review
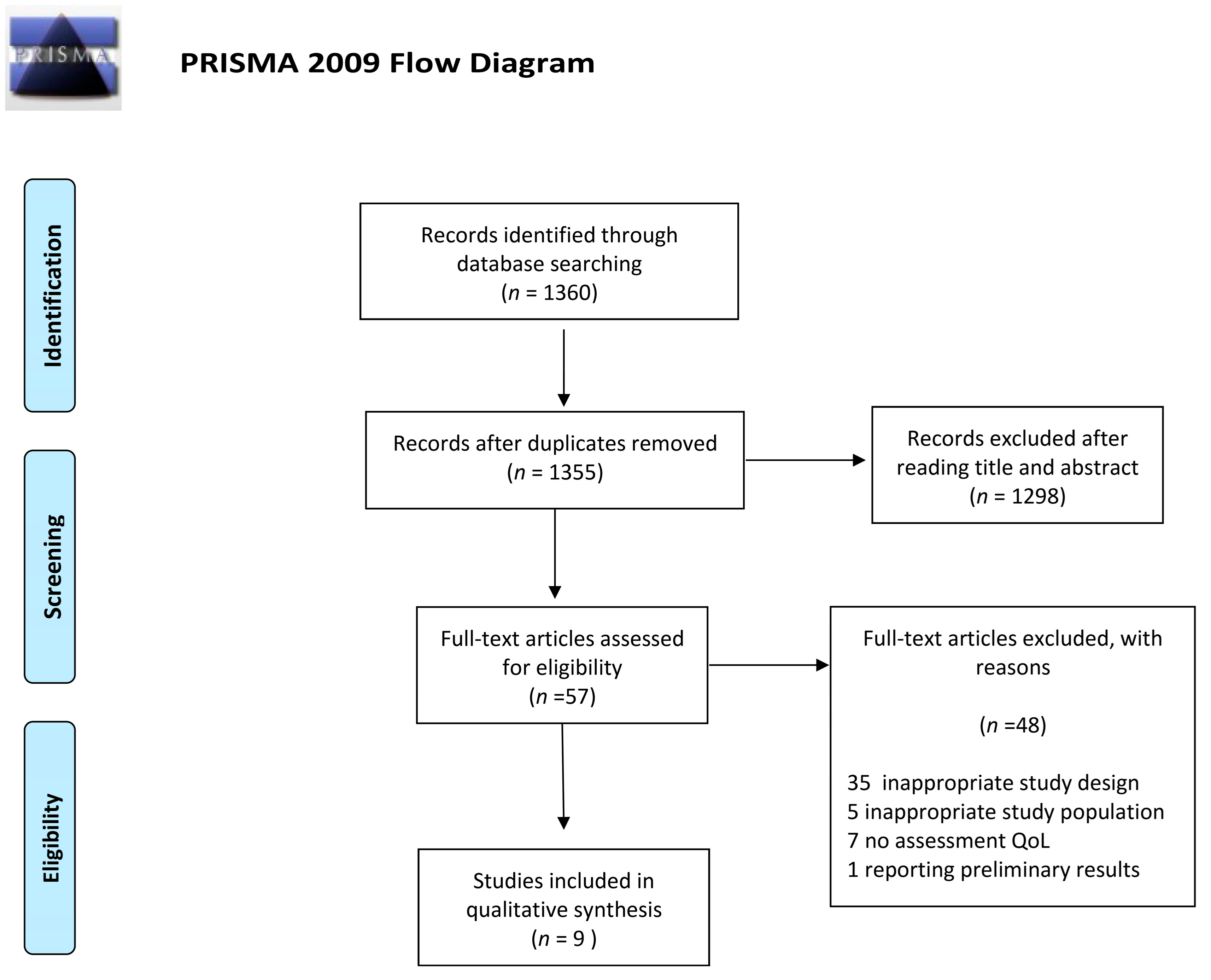
2.2.1. Literature Search and Study Selection
2.2.2. Data Extraction
2.2.3. Risk of bias assessment
3. Results
3.1. Cross-Sectional Study
3.1.1. Study Population and Quality of Life
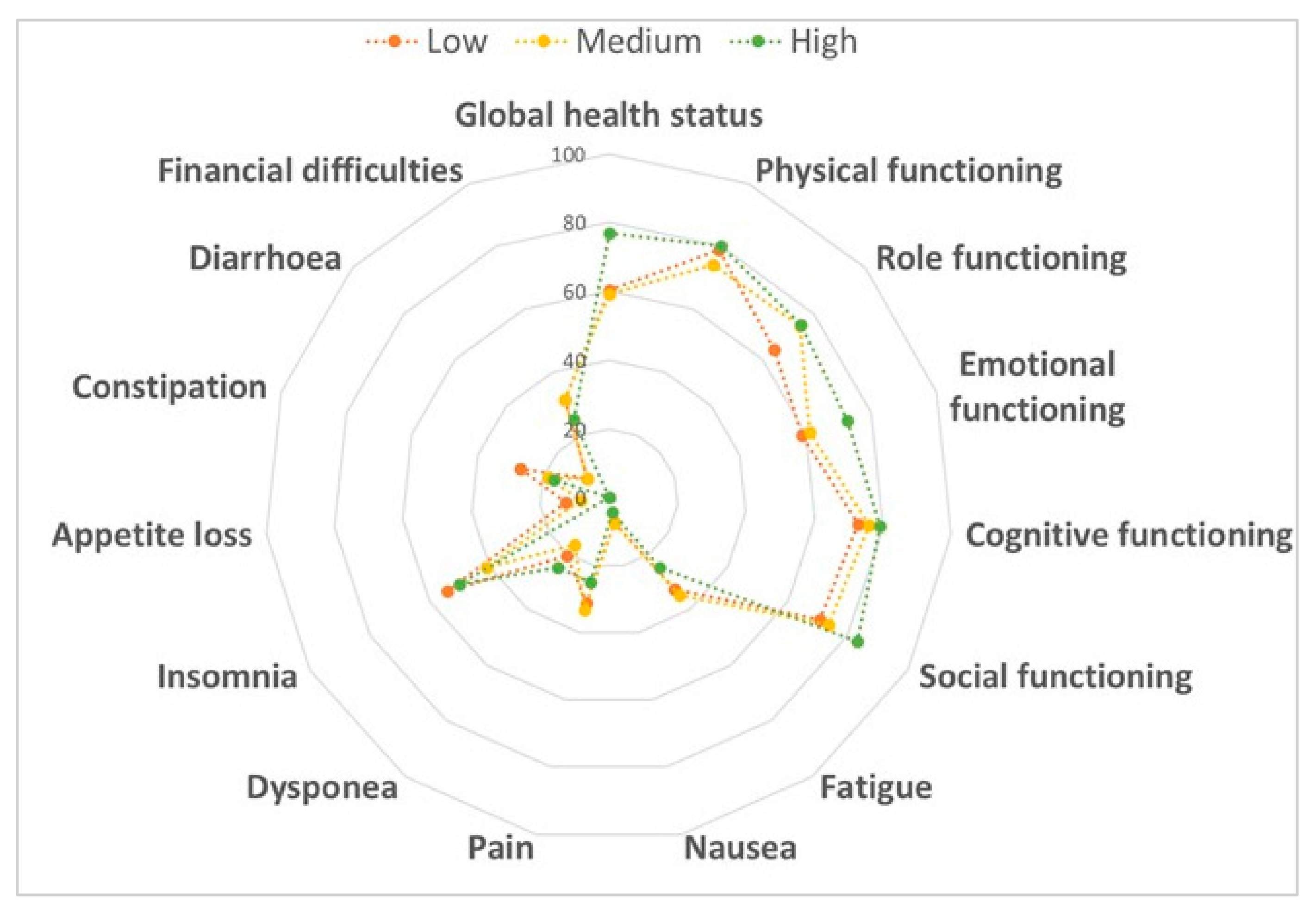
3.1.2. Mediterranean Diet and Quality of Life
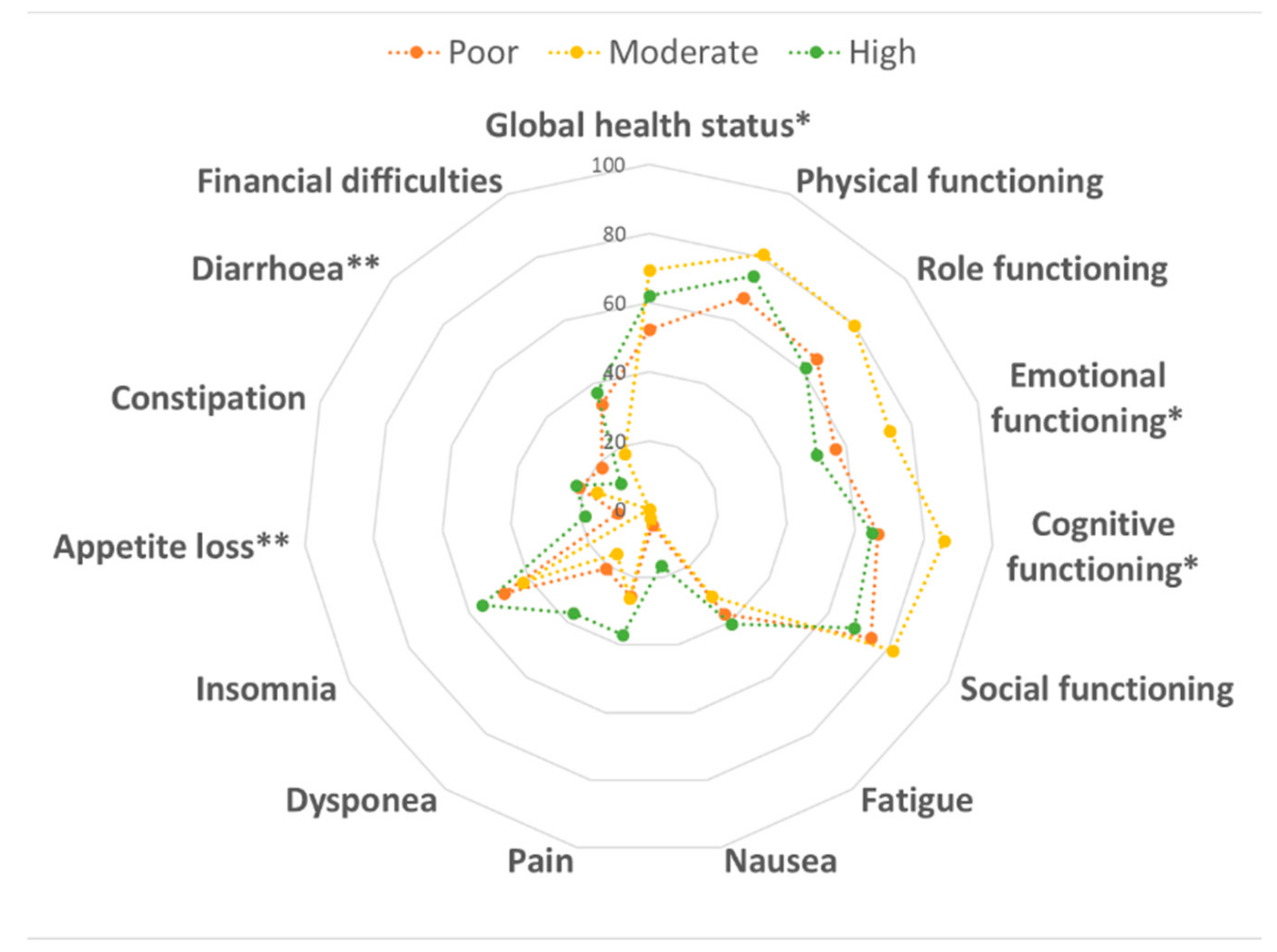
3.1.3. Physical Activity and Quality of Life
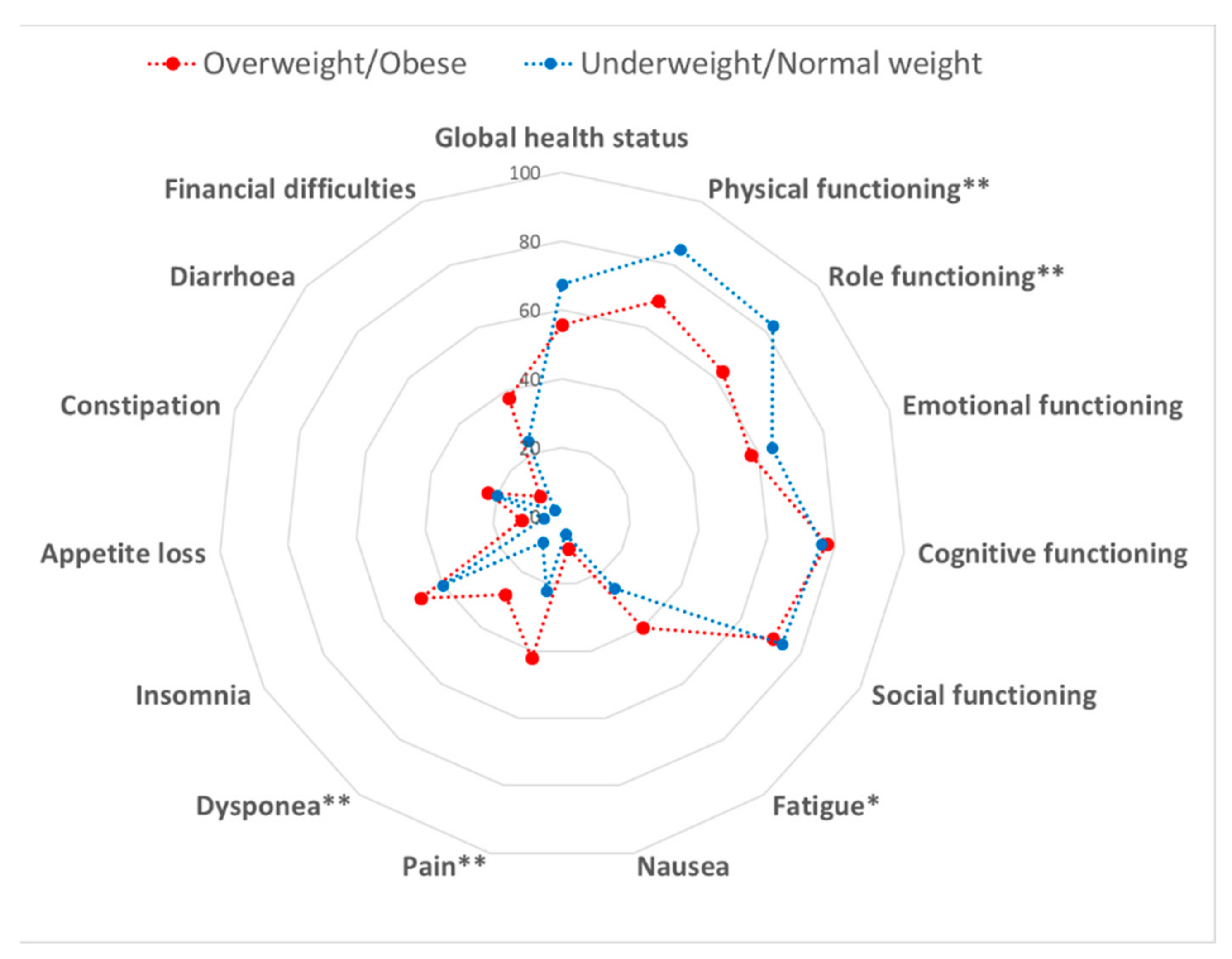
3.1.4. Weight Status and Quality of Life
3.2. Findings from the Systematic Review
3.3. Risk of Bias in Randomized Controlled Trials
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- WHO, World Health Organization. Available online: https://www.who.int/en/news-room/fact-sheets/detail/cancer (accessed on 2 January 2020).
- Sant, M.; Allemani, C.; Santaquilani, M.; Knijn, A.; Marchesi, F.; Capocaccia, R.; Group, E.W. EUROCARE-4. Survival of cancer patients diagnosed in 1995–1999. Results and commentary. Eur. J. Cancer 2009, 45, 931–991. [Google Scholar] [CrossRef] [PubMed]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J. Clin. Oncol. 2016, 34, 611–635. [Google Scholar] [CrossRef] [PubMed]
- Bines, J.; Gradishar, W.J. Primary care issues for the breast cancer survivor. Compr. Ther. 1997, 23, 605–611. [Google Scholar]
- Brown, B.W.; Brauner, C.; Minnotte, M.C. Noncancer deaths in white adult cancer patients. J. Natl. Cancer Inst. 1993, 85, 979–987. [Google Scholar] [CrossRef]
- Talamini, R.; Franceschi, S.; Favero, A.; Negri, E.; Parazzini, F.; La Vecchia, C. Selected medical conditions and risk of breast cancer. Br. J. Cancer 1997, 75, 1699–1703. [Google Scholar] [CrossRef]
- Andersen, B.L. Biobehavioral outcomes following psychological interventions for cancer patients. J. Consult. Clin. Psychol. 2002, 70, 590–610. [Google Scholar] [CrossRef]
- Shephard, R.J. Exercise in the prevention and treatment of cancer. An update. Sports Med. 1993, 15, 258–280. [Google Scholar] [CrossRef]
- Ahn, S.H.; Park, B.W.; Noh, D.Y.; Nam, S.J.; Lee, E.S.; Lee, M.K.; Kim, S.H.; Lee, K.M.; Park, S.M.; Yun, Y.H. Health-related quality of life in disease-free survivors of breast cancer with the general population. Ann. Oncol. 2007, 18, 173–182. [Google Scholar] [CrossRef]
- Vallance, J.K.; Courneya, K.S.; Plotnikoff, R.C.; Yasui, Y.; Mackey, J.R. Randomized controlled trial of the effects of print materials and step pedometers on physical activity and quality of life in breast cancer survivors. J. Clin. Oncol. 2007, 25, 2352–2359. [Google Scholar] [CrossRef]
- Blanchard, C.M.; Courneya, K.S.; Stein, K.; SCS-II, A.C.S.s. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Kushi, L.H.; Doyle, C.; McCullough, M.; Rock, C.L.; Demark-Wahnefried, W.; Bandera, E.V.; Gapstur, S.; Patel, A.V.; Andrews, K.; Gansler, T.; et al. American Cancer Society Guidelines on nutrition and physical activity for cancer prevention: Reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J. Clin. 2012, 62, 30–67. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Rock, C.L. Nutrition-related issues for the breast cancer survivor. Semin. Oncol. 2003, 30, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.M.; Day, J.M.; Katz, M.L.; Herndon, J.E.; Bittoni, M.A.; Oliveri, J.M.; Donohue, K.; Paskett, E.D. Exercise and dietary change after diagnosis and cancer-related symptoms in long-term survivors of breast cancer: CALGB 79804. Psychooncology 2009, 18, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Shin, H.; Bae, E.; Lim, H. Aspects of Health-Related Factors and Nutritional Care Needs by Survival Stage among Female Cancer Patients in South Korea. PLoS ONE 2016, 11, e0163281. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.M.; Ashing, K.T.; Modeste, N.N.; Herring, R.P.; Sealy, D.A. Contextual factors influencing health-related quality of life in African American and Latina breast cancer survivors. J. Cancer Surviv. 2015, 9, 441–449. [Google Scholar] [CrossRef]
- Orchard, T.S.; Andridge, R.R.; Yee, L.D.; Lustberg, M.B. Diet. Quality, Inflammation, and Quality of Life in Breast Cancer Survivors: A Cross-Sectional Analysis of Pilot Study Data. J. Acad. Nutr. Diet. 2018, 118, 578–588.e571. [Google Scholar] [CrossRef]
- Tangney, C.C.; Young, J.A.; Murtaugh, M.A.; Cobleigh, M.A.; Oleske, D.M. Self-reported dietary habits, overall dietary quality and symptomatology of breast cancer survivors: A cross-sectional examination. Breast Cancer Res. Treat. 2002, 71, 113–123. [Google Scholar] [CrossRef]
- Wayne, S.J.; Baumgartner, K.; Baumgartner, R.N.; Bernstein, L.; Bowen, D.J.; Ballard-Barbash, R. Diet. quality is directly associated with quality of life in breast cancer survivors. Breast Cancer Res. Treat. 2006, 96, 227–232. [Google Scholar] [CrossRef]
- Mohammadi, S.; Sulaiman, S.; Koon, P.B.; Amani, R.; Hosseini, S.M. Impact of healthy eating practices and physical activity on quality of life among breast cancer survivors. Asian Pac. J. Cancer Prev. 2013, 14, 481–487. [Google Scholar] [CrossRef]
- Kim, N.H.; Song, S.; Jung, S.Y.; Lee, E.; Kim, Z.; Moon, H.G.; Noh, D.Y.; Lee, J.E. Dietary pattern and health-related quality of life among breast cancer survivors. BMC Womens Health 2018, 18, 65. [Google Scholar] [CrossRef] [PubMed]
- Lawler, S.; Maher, G.; Brennan, M.; Goode, A.; Reeves, M.M.; Eakin, E. Get Healthy after Breast Cancer—Examining the feasibility, acceptability and outcomes of referring breast cancer survivors to a general population telephone-delivered program targeting physical activity, healthy diet and weight loss. Support. Care Cancer 2017, 25, 1953–1962. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Hwang, E.; Moon, H.G.; Noh, D.Y.; Lee, J.E. Adherence to Guidelines for Cancer Survivors and Health-Related Quality of Life among Korean Breast Cancer Survivors. Nutrients 2015, 7, 10307–10319. [Google Scholar] [CrossRef] [PubMed]
- Boehmer, U.; Ozonoff, A.; Potter, J. Sexual Minority Women’s Health Behaviors and Outcomes After Breast Cancer. LGBT Health 2015, 2, 221–227. [Google Scholar] [CrossRef]
- Mosher, C.E.; Sloane, R.; Morey, M.C.; Snyder, D.C.; Cohen, H.J.; Miller, P.E.; Demark-Wahnefried, W. Associations between lifestyle factors and quality of life among older long-term breast, prostate, and colorectal cancer survivors. Cancer 2009, 115, 4001–4009. [Google Scholar] [CrossRef]
- Shin, W.K.; Song, S.; Jung, S.Y.; Lee, E.; Kim, Z.; Moon, H.G.; Noh, D.Y.; Lee, J.E. The association between physical activity and health-related quality of life among breast cancer survivors. Health Qual. Life Outcomes 2017, 15, 132. [Google Scholar] [CrossRef]
- Gong, X.H.; Wang, J.W.; Li, J.; Chen, X.F.; Sun, L.; Yuan, Z.P.; Yu, J.M. Physical exercise, vegetable and fruit intake and health-related quality of life in Chinese breast cancer survivors: A cross-sectional study. Qual. Life Res. 2017, 26, 1541–1550. [Google Scholar] [CrossRef]
- Leensen, M.C.J.; Groeneveld, I.F.; Heide, I.V.; Rejda, T.; van Veldhoven, P.L.J.; Berkel, S.V.; Snoek, A.; Harten, W.V.; Frings-Dresen, M.H.W.; de Boer, A.G.E.M. Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: A prospective study in the Netherlands. BMJ. Open 2017, 7, e014746. [Google Scholar] [CrossRef]
- Bellizzi, K.M.; Rowland, J.H.; Jeffery, D.D.; McNeel, T. Health behaviors of cancer survivors: Examining opportunities for cancer control intervention. J. Clin. Oncol. 2005, 23, 8884–8893. [Google Scholar] [CrossRef]
- Coups, E.J.; Ostroff, J.S. A population-based estimate of the prevalence of behavioral risk factors among adult cancer survivors and noncancer controls. Prev. Med. 2005, 40, 702–711. [Google Scholar] [CrossRef]
- Eakin, E.G.; Youlden, D.R.; Baade, P.D.; Lawler, S.P.; Reeves, M.M.; Heyworth, J.S.; Fritschi, L. Health behaviors of cancer survivors: Data from an Australian population-based survey. Cancer Causes Control 2007, 18, 881–894. [Google Scholar] [CrossRef] [PubMed]
- Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452.
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Houston Miller, N.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [PubMed]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schröder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: The PREDIMED study. J. Am. Diet. Assoc. 2008, 108, 1134–1144; discussion 1145. [Google Scholar] [CrossRef]
- Martínez-González, M.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fiol, M.; Wärnberg, J.; Arós, F.; Ruíz-Gutiérrez, V.; Lamuela-Raventós, R.M.; et al. Cohort profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Bulló, M.; Garcia-Aloy, M.; Martínez-González, M.A.; Corella, D.; Fernández-Ballart, J.D.; Fiol, M.; Gómez-Gracia, E.; Estruch, R.; Ortega-Calvo, M.; Francisco, S.; et al. Association between a healthy lifestyle and general obesity and abdominal obesity in an elderly population at high cardiovascular risk. Prev. Med. 2011, 53, 155–161. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Fernández-Jarne, E.; Serrano-Martínez, M.; Marti, A.; Martinez, J.A.; Martín-Moreno, J.M. Mediterranean diet and reduction in the risk of a first acute myocardial infarction: An operational healthy dietary score. Eur. J. Nutr. 2002, 41, 153–160. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Yun, Y.H.; Bae, S.H.; Kang, I.O.; Shin, K.H.; Lee, R.; Kwon, S.I.; Park, Y.S.; Lee, E.S. Cross-cultural application of the Korean version of the European Organization for Research and Treatment of Cancer (EORTC) Breast-Cancer-Specific Quality of Life Questionnaire (EORTC QLQ-BR23). Support. Care Cancer 2004, 12, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.H.; Park, Y.S.; Lee, E.S.; Bang, S.M.; Heo, D.S.; Park, S.Y.; You, C.H.; West, K. Validation of the Korean version of the EORTC QLQ-C30. Qual. Life Res. 2004, 13, 863–868. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; Collaboration, T.C., Ed.; Cochrane Library: London, UK, 2008. [Google Scholar]
- Scott, N.W.; Fayers, P.M.; Bottomley, A.; Aaronson, N.K.; de Graeff, A.; Groenvold, M.; Koller, M.; Petersen, M.A.; Sprangers, M.A.; EORTC and the Quality of Life Cross-Cultural Meta-Analysis Group. Comparing translations of the EORTC QLQ-C30 using differential item functioning analyses. Qual. Life Res. 2006, 15, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Bauersfeld, S.P.; Kessler, C.S.; Wischnewsky, M.; Jaensch, A.; Steckhan, N.; Stange, R.; Kunz, B.; Brückner, B.; Sehouli, J.; Michalsen, A. The effects of short-term fasting on quality of life and tolerance to chemotherapy in patients with breast and ovarian cancer: A randomized cross-over pilot study. BMC Cancer 2018, 18, 476. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Shin, M.S.; Lee, H.S.; Lee, E.S.; Ro, J.S.; Kang, H.S.; Kim, S.W.; Lee, W.H.; Kim, H.S.; Kim, C.J.; et al. Randomized pilot test of a simultaneous stage-matched exercise and diet intervention for breast cancer survivors. Oncol. Nurs Forum 2011, 38, E97–E106. [Google Scholar] [CrossRef]
- Morey, M.C.; Snyder, D.C.; Sloane, R.; Cohen, H.J.; Peterson, B.; Hartman, T.J.; Miller, P.; Mitchell, D.C.; Demark-Wahnefried, W. Effects of home-based diet and exercise on functional outcomes among older, overweight long-term cancer survivors: RENEW: A randomized controlled trial. JAMA 2009, 301, 1883–1891. [Google Scholar] [CrossRef]
- Kwiatkowski, F.; Mouret-Reynier, M.A.; Duclos, M.; Bridon, F.; Hanh, T.; Van Praagh-Doreau, I.; Travade, A.; Vasson, M.P.; Jouvency, S.; Roques, C.; et al. Long-term improvement of breast cancer survivors’ quality of life by a 2-week group physical and educational intervention: 5-year update of the ‘PACThe’ trial. Br J. Cancer 2017, 116, 1389–1393. [Google Scholar] [CrossRef]
- Travier, N.; Fonseca-Nunes, A.; Javierre, C.; Guillamo, E.; Arribas, L.; Peiró, I.; Buckland, G.; Moreno, F.; Urruticoechea, A.; Oviedo, G.R.; et al. Effect of a diet and physical activity intervention on body weight and nutritional patterns in overweight and obese breast cancer survivors. Med. Oncol. 2014, 31, 783. [Google Scholar] [CrossRef]
- Travier, N.; Guillamo, E.; Oviedo, G.R.; Valls, J.; Buckland, G.; Fonseca-Nunes, A.; Alamo, J.M.; Arribas, L.; Moreno, F.; Sanz, T.E.; et al. Is Quality of Life Related to Cardiorespiratory Fitness in Overweight and Obese Breast Cancer Survivors? Women Health 2015, 55, 505–524. [Google Scholar] [CrossRef]
- Befort, C.A.; Klemp, J.R.; Austin, H.L.; Perri, M.G.; Schmitz, K.H.; Sullivan, D.K.; Fabian, C.J. Outcomes of a weight loss intervention among rural breast cancer survivors. Breast Cancer Res. Treat. 2012, 132, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Colditz, G.A.; Rock, C.L.; Sedjo, R.L.; Liu, J.; Wolin, K.Y.; Krontiras, H.; Byers, T.; Pakiz, B.; Parker, B.A.; et al. Quality of life outcomes from the Exercise and Nutrition Enhance Recovery and Good Health for You (ENERGY)-randomized weight loss trial among breast cancer survivors. Breast Cancer Res. Treat. 2015, 154, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Swisher, A.K.; Abraham, J.; Bonner, D.; Gilleland, D.; Hobbs, G.; Kurian, S.; Yanosik, M.A.; Vona-Davis, L. Exercise and dietary advice intervention for survivors of triple-negative breast cancer: Effects on body fat, physical function, quality of life, and adipokine profile. Support. Care Cancer 2015, 23, 2995–3003. [Google Scholar] [CrossRef] [PubMed]
- Haleh, G.; Neriman, A. Effects of a Lifestyle Interventions Program on Quality of Life in Breast Cancer Survivors. Int. J. Hematol. Oncol. 2017. [Google Scholar] [CrossRef]
- Lua, P.L.; Salihah, N.Z.; Mazlan, N. Nutritional status and health-related quality of life of breast cancer patients on chemotherapy. Malays. J. Nutr. 2012, 18, 173–184. [Google Scholar]
- Zhu, G.; Zhang, X.; Wang, Y.; Xiong, H.; Zhao, Y.; Sun, F. Effects of exercise intervention in breast cancer survivors: A meta-analysis of 33 randomized controlled trails. OncoTargets Ther. 2016, 9, 2153–2168. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Study Design | Population Characteristics | Intervention | QoL Assessment | Main Findings |
|---|---|---|---|---|---|---|
| Bauersfeld, 2018 [47] | Germany | Randomized cross-over pilot study | 30 breast cancer patients with scheduled chemotherapy | Short-term fasting followed by normo-caloric diet or vice versa in the first half of chemotherapy | FACT-G and FACT-F | The reduction in QoL after chemotherapy was less than the minimally important difference with short-term fasting but greater than the minimally important difference for non-fasted periods (p < 0.05). There were no serious adverse effects of intervention |
| Befort, 2011 [53] | USA | Single-arm trial | 34 obese stage I–III breast cancer survivors | Participants were instructed to follow a diet with ≥5 fruit and vegetable servings per day, prepackaged frozen entrees, and shakes. They were also instructed to gradually increase their physical activity to 225 minutes per week of moderate intensity activity | Breast Cancer Prevention Trial Symptom Checklist, PHQ-9, and the 32-item Body Image and Relationships scale | Significant improvements were evident for several QoL domains, including joint pain (p < 0.001), depression (p = 0.001), depression (p = 0.001), strength and health (p < 0.001), social barriers (p = 0.02) and sexuality (p < 0.001). The intervention also significantly reduced weight, waist circumference, daily energy intake and increased fruit and vegetables consumption and physical activity level |
| Demark-Wahnefried, 2015 [54] | USA | Randomized controlled trial | 692 obese or overweight women with a history of stage I–III breast cancer diagnosis who completed treatment | Intensive program consisting of six months of group sessions, personalized guidance via telephone and/or email to reduce weight and adhere to dietary and physical activity guidelines of the American Cancer Society. Controls received two contacts, one at baseline and another at six months | SF-36 | From baseline to 6 months, significant decreases in physical function (p = 0.01) and increases in symptoms (p = 0.002) were observed among controls, but not in the intervention arm. Improvements in vitality were evident in both arms, with greater improvement in the intervention arm (p = 0.05). By contrast, depressive symptoms increased in the intervention arm and became significant after 24 months (p = 0.031) |
| Kim, 2011 [48] | Korea | Randomized controlled trial | 45 women with breast cancer who completed treatment | Telephone counseling with a personal prescription for regular exercise and balanced diet programs based on the guidelines for cancer survivors | QLQ-C30 | Compared with controls, the intervention group reported greater improvement in emotional functioning (p = 0.004), fatigue (p = 0.001) and depression (p = 0.035), and also in motivational readiness for exercise (p = 0.006) and diet (p < 0.001) |
| Kwiatkowski, 2017 [50] | France | Randomized controlled trial | 251 breast cancer patients post chemotherapy | Two-week intervention in hydrothermal center, consisting of daily group supervised physical training, dietary education, physiotherapy and psychological support | SF-36 | The intervention improved QoL at 6 and 12 months (p < 0.001; p = 0.032), with greater improvements in mental and physical sub-scores (p-values < 0.001) |
| Morey, 2009 [49] | USA | Randomized controlled trial | 143 breast cancer patients | 12-month diet and exercise intervention delivered via telephone counseling and tailored mailed materials versus a delayed-intervention control arm | SF-36 | The intervention significantly improved physical activity, dietary behaviors, and overall QoL (p-values < 0.05). At 12 months, the mean function scores declined less rapidly in the intervention group compared with the control group (p = 0.03). |
| Travier, 2015 [52] | Spain | Phase II single-arm trial | 37 breast cancer survivors who had completed chemotherapy and/or radiotherapy | 12-week intervention including dietary and physical activity recommendations, with the aim of promoting weight loss | QLQ-C30 and SF-36 | Participants who completed the intervention reported significant improvements in QoL (p < 0.001) and its sub-scores (p-values < 0.05), and also in weight, BMI and cardiorespiratory fitness |
| Ghavami, 2017 [56] | Turkey | Randomized controlled trial | 40 breast cancer survivors with stage I–III breast cancer and 40 control | Practice supervised aerobic exercises with dietary energy restriction training for 24 weeks | QLQ-C30 | Compared with controls, the intervention significantly improved symptom relief (p < 0.001), functional (p < 0.001) and global health status (p < 0.001) |
| Swisher, 2015 [55] | USA | Randomized controlled trial | Survivors of triple-negative breast cancer:13 intervention, 10 control | Supervised, moderate-intensity aerobic exercise (150 min per week, for 12 weeks) and diet counseling (two individual sections with a dietitian) | FACT-B | Compared with control, the intervention significantly improved overall physical wellbeing (p < 0.05), and breast-cancer specific subscales (p < 0.01) and total score (p < 0.05). The intervention also reduced body fat and sedentary time |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Quattrocchi, A.; Degrassi, F.; Catalano, F.; Basile, G.; Agodi, A. The Effects of Diet and Dietary Interventions on the Quality of Life among Breast Cancer Survivors: A Cross-Sectional Analysis and a Systematic Review of Experimental Studies. Cancers 2020, 12, 322. https://doi.org/10.3390/cancers12020322
Barchitta M, Maugeri A, Magnano San Lio R, Quattrocchi A, Degrassi F, Catalano F, Basile G, Agodi A. The Effects of Diet and Dietary Interventions on the Quality of Life among Breast Cancer Survivors: A Cross-Sectional Analysis and a Systematic Review of Experimental Studies. Cancers. 2020; 12(2):322. https://doi.org/10.3390/cancers12020322
Chicago/Turabian StyleBarchitta, Martina, Andrea Maugeri, Roberta Magnano San Lio, Annalisa Quattrocchi, Flori Degrassi, Francesca Catalano, Guido Basile, and Antonella Agodi. 2020. "The Effects of Diet and Dietary Interventions on the Quality of Life among Breast Cancer Survivors: A Cross-Sectional Analysis and a Systematic Review of Experimental Studies" Cancers 12, no. 2: 322. https://doi.org/10.3390/cancers12020322
APA StyleBarchitta, M., Maugeri, A., Magnano San Lio, R., Quattrocchi, A., Degrassi, F., Catalano, F., Basile, G., & Agodi, A. (2020). The Effects of Diet and Dietary Interventions on the Quality of Life among Breast Cancer Survivors: A Cross-Sectional Analysis and a Systematic Review of Experimental Studies. Cancers, 12(2), 322. https://doi.org/10.3390/cancers12020322