Abstract
Gallstone ileus is a rare but serious complication of gallstone disease, often requiring surgical intervention. While enterolithotomy remains the standard treatment, the role of additional biliary surgery, particularly subtotal cholecystectomy, remains controversial. This study examines the management of gallstone ileus in a rural setting, where limited surgical resources and access to specialized biliary interventions pose unique challenges. We present a case series of four patients diagnosed with gallstone ileus in a rural healthcare facility. All patients underwent initial enterolithotomy for bowel obstruction relief. Surgical outcomes, complications, and the necessity for a second intervention, including subtotal cholecystectomy, were evaluated. Ever patient had a successful recovery. Of the four cases, two patients underwent a subtotal cholecystectomy. No perioperative mortality was observed, but limited access to advanced imaging and specialized biliary surgery influenced clinical decision-making. The rural setting in which these series occurred comes with its unique challenges regarding resource management and technological demands.
1. Introduction
Gallstone ileus is a rare but serious complication of cholelithiasis that results from the passage of a large gallstone into the intestinal tract, typically via a cholecystoenteric fistula. This fistula forms due to chronic inflammation of the gallbladder, allowing a gallstone to enter and obstruct the small intestine, most often in the terminal ileum [1,2]. The condition accounts for 1–4% of all mechanical bowel obstructions, and it is more prevalent in elderly individuals, particularly those with a history of biliary disease [3]. Diagnosis can be challenging due to its nonspecific clinical presentation, including abdominal pain, nausea, vomiting, and signs of intestinal obstruction [4].
Gallstone ileus is of critical importance due to its high morbidity and mortality, particularly in the elderly population. The condition is frequently underdiagnosed because its symptoms can mimic other causes of bowel obstruction, leading to delays in treatment and poor outcomes [5,6]. Early diagnosis through imaging techniques such as abdominal CT scans, which may reveal Rigler’s triad (pneumobilia, intestinal obstruction, and an ectopic gallstone), is crucial for timely intervention [7]. Despite advancements in diagnostic tools, surgical treatment remains the primary method to relieve the obstruction and address the underlying cause [8].
Understanding gallstone ileus is vital for improving patient outcomes, particularly in settings where early diagnostic tools may not be readily available. While the condition is more common in elderly patients in developed urban settings with access to advanced diagnostic imaging, its impact in rural healthcare settings can be more pronounced due to diagnostic delays and limited access to surgical interventions [9]. Focusing on rural healthcare research is essential to optimize management protocols and enhance early recognition of gallstone ileus, thus reducing its associated complications [10]. We hereby present a case series, four patients from a rural jungle area in the Colombian Amazon.
2. Materials and Methods
A retrospective, monocentric case series was conducted, involving patients who presented with Gallstone ileus. Data from four patients were collected retrospectively between 2018 and 2024 from Hospital de María Inmaculada in Florencia, Caquetá, Colombia, where the surgeries were performed. Surgeons were General Surgeons with more than 20 years of experience and the setting was a university hospital. The following variables were evaluated during the study period: gender, age, preoperative vital signs, preoperative laboratory results, medical images, surgical procedures, antibiotic regimen, need for ICU care, length of hospital stay, complications, and mortality. Postoperative follow-ups were conducted when possible.
The surgical approach was tailored to each case based on intraoperative findings. Postoperative management included an antibiotic course, after which patients were discharged. Ethical approval was waived due to the retrospective nature of the study, which relied on clinical record data. This study falls under the category of “research with no risk” as outlined by Resolution 8430 of 1993 in Colombian legislation. According to Article 11 of this regulation, such research involves the retrospective review of clinical records without intervention or modification of the participants’ biological, physiological, psychological, or social variables and does not involve sensitive aspects of behavior. Informed consent was obtained from all the patients. To preserve confidentiality, medical records were accessed only by the treating surgeon at the institution, who exclusively extracted the data for the purposes of this study.
3. Results
A total of four patients are presented in this case series. All the patients were in their eighth decade of their life and 75% were female. Regarding symptoms, all patients presented vomit and abdominal pain, however only one presented signs of acute abdomen. Vital signs only reported one patient with tachycardia and two with high blood pressure. Preoperative hemogram reported leukocytosis and neutrophilia in every patient, a high level of creatinine of one patient, and high glycemic levels in one patient. CT scans reported gallstones inside the intestinal tract (Figure 1) and cholecystoduodenal fistula (Figure 2) as findings. Every patient had an enterotomy as a surgical procedure. However, two patients had also a subtotal cholecystectomy. Surgical procedures also evidenced the presence of gallstones which were documented via photographs and removed (Figure 3). Evaluating complications, one patient had a surgical site infection, while the other was diagnosed with healthcare-related pneumonia. The other two patients did not present any complications. The average hospital stay was 9.5 days. One patient required treatment in the ICU (Table 1).
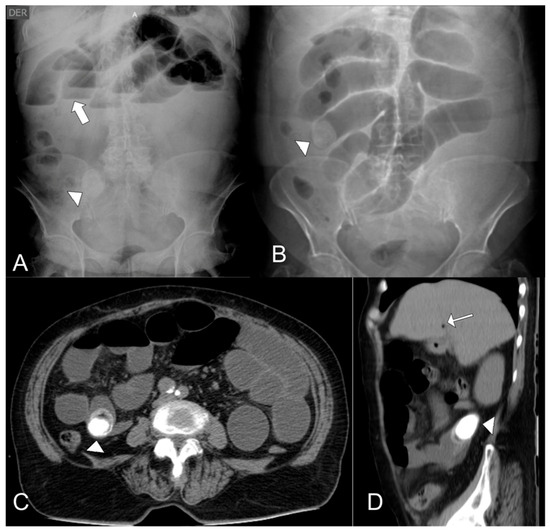
Figure 1.
(A) Plain abdominal X-ray showing a radiopaque object in the right flank (arrowhead), consistent with a gallstone, along with stepladder-pattern air-fluid levels (thick arrow). (B). Scout view from an abdominal computed tomography (CT) scan demonstrating a gallstone in the right flank (arrowhead) and dilated small bowel loops. (C). Axial contrast-enhanced abdominal CT scan revealing a thick-walled gallbladder containing a large calculus, along with pneumobilia and passage of oral contrast into the gallbladder. (D). Coronal contrast-enhanced abdominal CT scan showing a gallstone at the jejunal level (arrowhead) with a second, smaller adjacent gallstone, as well as pneumobilia (arrow).
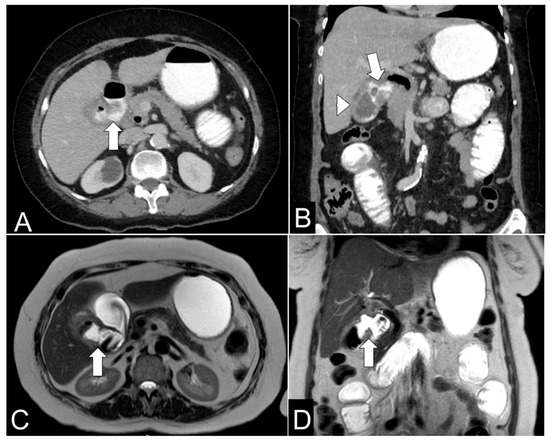
Figure 2.
(A) Axial contrast-enhanced abdominal CT scan showing a cholecystoduodenal fistula (arrow) with pneumobilia and passage of oral contrast into the gallbladder. (B) Coronal contrast-enhanced abdominal CT scan demonstrating a cholecystoduodenal fistula (arrow) with oral contrast passage into the gallbladder and cholelithiasis (arrowhead). (C) Axial T2-weighted MR cholangiography showing a cholecystoduodenal fistula (arrow) with pneumobilia. (D) Coronal T2-weighted MR cholangiography depicting a cholecystoduodenal fistula (arrow) with pneumobilia and cholelithiasis.
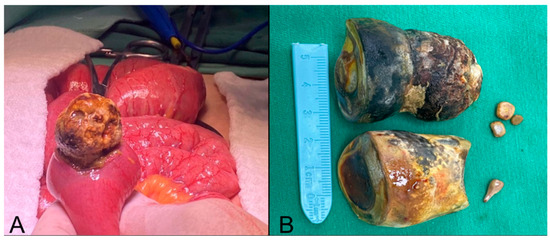
Figure 3.
(A) Enterotomy with calculus extraction. (B) Extracted calculi from the jejunum and gallbladder, along with smaller associated calculi.

Table 1.
Characterization of the variables involving the four patients including demographic, comorbidities, initial vital signs, initial lab reports, image and surgical findings, complications, and length of stay.
4. Discussion
In Colombia, traditional meals regularly follow a dietary structure known as “sopa y seco,” consisting of two components: a soup dish followed by a solid main dish (“seco”). The soup typically includes potatoes and/or rice, combined with vegetables and a protein source. The “seco” commonly contains rice, yuca (cassava), potato, and plantain, accompanied by some protein and/or vegetables. This meal structure results in a high overall carbohydrate load, which may contribute to poor glycemic control and a higher prevalence of obesity diabetes in these patients.
Surgical management of biliary ileus involves three main strategies: (1) enterolithotomy alone; (2) enterolithotomy, cholecystectomy, and fistula closure in a single surgical procedure; and (3) initial enterolithotomy followed by delayed biliary surgery, typically 4 to 24 weeks later. The combination of enterolithotomy, cholecystectomy, and fistula closure in the same procedure is reserved for selected patients with acute or gangrenous cholecystitis or residual gallstones but is associated with higher morbidity and mortality rates [11,12]. On the other hand, initial enterolithotomy followed by elective surgery for the gallbladder and fistula poses a lower risk of complications [13]. While some fistulas may close spontaneously and the recurrence rate of gallstone ileus is less than 5% with enterolithotomy alone [1], up to 56% of patients may develop long-term biliary complications [8]. Therefore, it is recommended to leave the gallbladder and fistula untreated in elderly or frail patients with significant comorbidities [13]. Rather than a demonstration of procedural novelty, this case series highlights the complexity of surgical decision-making in gallstone ileus within settings with limited resources. In such environments, surgical strategies are based not only on disease severity but also on patient frailty, delayed diagnosis, and restricted access to advanced imaging and subspecialized hepatobiliary surgery. These constraints require pragmatic adaptations of standard approaches while prioritizing patient safety.
If only enterolithotomy is performed, follow-up should include assessment of biliary symptoms and imaging or endoscopy to detect residual gallstones or persistent fistulas. In cases of symptoms or evidence of stones or fistulas, surgery is recommended to perform cholecystectomy, fistula closure, and, if necessary, bile duct exploration [7]. A study from the Nationwide Inpatient Sample (2004–2009) involving 3268 cases found that 62% of patients were treated with enterolithotomy alone, while fistula closure occurred in 19% of cases but was associated with higher mortality (OR 2.86, CI 1.16–7.07) [6]. This study supports the existing literature, recommending enterolithotomy as the procedure of choice, reserving additional interventions for selected cases. Gallstone ileus is a rare but serious complication of gallstone disease. The need for a second surgical intervention, particularly a subtotal cholecystectomy, is exceedingly uncommon in the management of gallstone ileus [14] In most cases, once the obstruction is relieved, patients do not require further biliary surgery, as spontaneous closure of the biliary-enteric fistula often occurs [7]. Subtotal cholecystectomy is typically performed in cases where severe inflammation, fibrosis, or extensive adhesions make a total cholecystectomy high-risk, a scenario more commonly seen in complicated cholecystitis rather than gallstone ileus. In the rare instances where a second surgery becomes necessary, it is usually due to recurrent gallstone-related complications such as persistent cholecystobiliary fistulas, residual gallstones, or ongoing biliary symptoms that compromise the patient’s long-term health [15]. However, given that gallstone ileus predominantly affects elderly patients with significant comorbidities, the risks of a second surgical intervention must be carefully weighed against the benefits. This further contributes to the rarity of a delayed subtotal cholecystectomy in the overall treatment strategy for gallstone ileus, making it an exceptional rather than a routine occurrence in clinical practice.
In this scenario, subtotal cholecystectomy was selected instead of total cholecystectomy (Figure 4) because of severe local inflammation, dense adhesions, and distorted biliary anatomy, which substantially increases the risk of bile duct injury. In these kinds of patients, achieving a total cholecystectomy would have required advanced hepatobiliary exposure and surgical resources not available in the rural setting. Subtotal cholecystectomy therefore served as a damage control strategy, allowing for the definitive management of persistent biliary pathology while minimizing surgical risk [16]. Current clinical guidelines, including the Tokyo Guidelines 2018 (TG18), recommend definitive biliary surgery in carefully selected patients with adequate physiological reserve and institutional support [17]. However, these recommendations assume the availability of advanced imaging, specialized hepatobiliary expertise, and broad postoperative care. In contrast, the approach described in this series reflects a context adaptation of principles based on the guidelines, prioritizing technical safety and feasibility in a rural hospital environment [18].
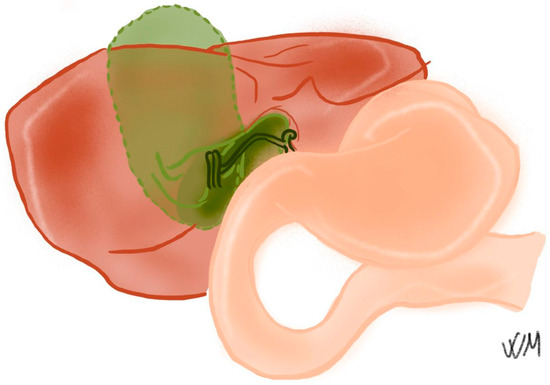
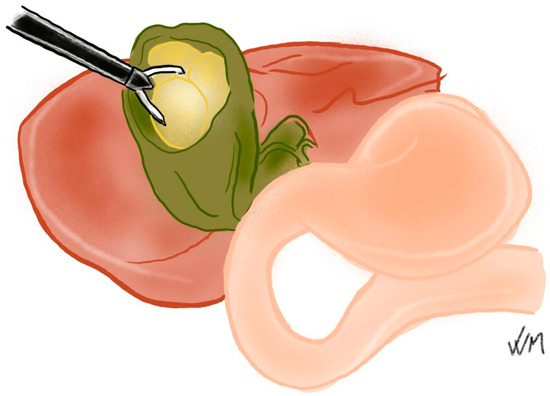
Figure 4.
Diagram depicting the difference between a total cholecystectomy and subtotal techniques. While the gallbladder is completely extracted on the total cholecystectomy, on difficult cases its recommended to partially open the gallbladder, extracting the stones and suturing it afterwards. Source: Self-elaborated by Valentina Velasco Muñoz.
This study has various important limitations. The retrospective design and small sample size introduce intrinsic selection bias, limiting the generalizability of the findings of these patients. Additionally, long-term follow-up was incomplete due to the rural setting and difficulties in infrastructure, preventing vigorous assessment of late biliary complications, fistula persistence, or recurrence. Finally, as a study conducted in only one institution in a rural setting, the results may not reflect outcomes achievable in urban institutions with high resources. Future research should focus on prospective, multicenter studies comparing enterolithotomy alone with staged or combined biliary approaches across rural and urban settings. Such studies would help clarify the long-term outcomes, likelihood, cost-effectiveness, and the role of subtotal cholecystectomy in hospitals without specialized hepatobiliary services [19,20,21].
5. Conclusions
Different complications arising from cholelithiasis must be considered when treating these kinds of patients. The predominant approach remains enterolithotomy alone, given its lower morbidity and mortality rates, with additional biliary surgery reserved for highly selected cases. While subtotal cholecystectomy as a second surgical intervention for gallstone ileus is exceedingly rare, its necessity arises in select cases where persistent biliary complications, such as residual gallstones, cholecystobiliary fistulas, or recurrent symptoms, compromise long-term patient outcomes. However, in rural settings where limited resources and access to specialized surgical expertise may influence decision-making, understanding the role of subtotal cholecystectomy in gallstone ileus remains a relevant area of study. The small sample size of this case series underscores the need for further research to evaluate the safety, feasibility, and long-term benefits of this approach, particularly in settings with restricted access to advanced biliary interventions. These findings have practical clinical implications, particularly in settings with limited resources, where early recognition and application of this approach may help improve patient outcomes and guide decision-making in the absence of advanced infrastructure and resources. Future investigations should focus on longitudinal patient outcomes, alternative surgical strategies, and cost-effectiveness analyses, aiming to refine management protocols and optimize treatment for gallstone ileus in both high-resource and underserved healthcare environments.
Author Contributions
Conceptualization, O.G. and F.E.C.; methodology, S.A.S.-G.; validation, O.G.; investigation, S.A.S.-G., V.V.-M., N.E., F.E.C. and O.G.; writing—original draft preparation, S.A.S.-G., V.V.-M., N.E., F.E.C. and O.G.; writing—review and editing, S.A.S.-G., V.V.-M., N.E., F.E.C. and O.G.; visualization, S.A.S.-G. and V.V.-M.; supervision, F.E.C. and O.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval was waived due to the retrospective nature of the study, which relied on clinical record data. This study falls under the category of “research with no risk” as outlined by Resolution 8430 of 1993 in Colombian legislation. According to Article 11 of this regulation, such research involves the retrospective review of clinical records without intervention or modification of the participants’ biological, physiological, psychological, or social variables and does not involve sensitive aspects of behavior.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CT | Computer Tomography |
| ICU | Intensive Care Unit |
| OR | Odds Ratio |
References
- Reisner, R.M.; Cohen, J.R. Gallstone ileus: A review of 1001 reported cases. Am. Surg. 1994, 60, 441–446. [Google Scholar] [PubMed]
- Lassandro, F.; Romano, S.; Ragozzino, A.; Rossi, G.; Valente, T.; Ferrara, I.; Romano, L.; Grassi, R. Role of helical CT in diagnosis of gallstone ileus and related conditions. Am. J. Roentgenol. 2005, 185, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Masannat, Y.; Masannat, Y.; Shatnawei, A. Gallstone ileus: A review. Mt. Sinai J. Med. 2006, 73, 1132–1134. [Google Scholar] [PubMed]
- Ayantunde, A.A.; Agrawal, A. Gallstone ileus: Diagnosis and management. World J. Surg. 2007, 31, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Muthukumarasamy, G.; Venkata, S.P.; Shaikh, I.A.; Somani, B.K.; Ravindran, R. Gallstone ileus: Surgical strategies and clinical outcome. J. Dig. Dis. 2008, 9, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Halabi, W.J.; Kang, C.Y.; Ketana, N.; Lafaro, K.J.; Nguyen, V.Q.; Stamos, M.J.; Imagawa, D.K.; Demirjian, A.N. Surgery for gallstone ileus: A nationwide comparison of trends and outcomes. Ann. Surg. 2014, 259, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Nuño-Guzmán, C.M.; Marín-Contreras, M.E.; Figueroa-Sánchez, M.; Corona, J.L. Gallstone ileus, clinical presentation, diagnostic and treatment approach. World J. Gastrointest. Surg. 2016, 8, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Richon, J.; Burgan, S.; Rohner, A. Gallstone ileus. Br. J. Surg. 1990, 77, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Sanjuán, J.C.; Casado, F.; Fernández, M.J.; Morales, D.J.; Naranjo, A. Cholecystectomy and fistula closure versus enterolithotomy alone in gallstone ileus. Br. J. Surg. 1997, 84, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Jakubauskas, M.; Luksaite, R.; Sileikis, A.; Strupas, K.; Poskus, T. Gallstone Ileus: Management and Clinical Outcomes. Medicina 2019, 55, 598. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Louis, M.; Gibson, B.; Jones, L.; Singh, H. Mechanical Small Bowel Obstruction Due to Gallstone Ileus: Diagnostic Challenges and Surgical Management. Cureus 2023, 15, e44153. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Neary, P.M.; Dowdall, J.F. Evolution of entero-biliary fistula following gallstone ileus management. BMJ Case Rep. 2012, 2012, bcr2012006929. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tsang, C.F. A rare case of gallstone ileus-the unanswered question. J. Surg. Case Rep. 2021, 2021, rjab164, Erratum in: J. Surg. Case Rep. 2021, 2021, rjab250. https://doi.org/10.1093/jscr/rjab250. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Helmy, N.A.; Ryska, O. Gallstone Ileus Post-cholecystectomy: A Case Review. Cureus 2023, 15, e33345. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, D.; Wang, Z.; Duan, Z.J.; Jin, S. Laparoscopic treatment of an upper gastrointestinal obstruction due to Bouveret’s syndrome. World J. Gastroenterol. 2013, 19, 6943–6946. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Elshaer, M.; Gravante, G.; Thomas, K.; Sorge, R.; Al-Hamali, S.; Ebdewi, H. Subtotal cholecystectomy for difficult gallbladders: Systematic review and meta-analysis. JAMA Surg. 2015, 150, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Suzuki, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Endo, I.; Iwashita, Y.; Hibi, T.; Pitt, H.A.; Umezawa, A.; et al. Tokyo Guidelines 2018: Flowchart for the management of acute cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.W.; Lin, Y.; Ntakiyiruta, G.; Mutabazi, Z.A.; Davis, W.A.; Morris, M.A.; Smink, D.S.; Riviello, R.; Yule, S. Contextual Challenges to Safe Surgery in a Resource-limited Setting: A Multicenter, Multiprofessional Qualitative Study. Ann. Surg. 2018, 267, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Platt, R.; Davis, R.; Finkelstein, J.; Go, A.S.; Gurwitz, J.H.; Roblin, D.; Soumerai, S.; Ross-Degnan, D.; Andrade, S.; Goodman, M.J.; et al. Multicenter epidemiologic and health services research on therapeutics in the HMO Research Network Center for Education and Research on Therapeutics. Pharmacoepidemiol. Drug Saf. 2001, 10, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.; MacDougall, D. Rural Health Care Planning Initiatives and Frameworks: Technology Review [Internet]; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK602612/ (accessed on 11 December 2025).
- Wang, Y.; Hu, X.J.; Wang, H.H.X.; Duan, H.Y.; Chen, Y.; Li, Y.T.; Luo, Z.L.; Li, X.; Wang, J.J.; Mercer, S.W. Follow-up care delivery in community-based hypertension and type 2 diabetes management: A multi-centre, survey study among rural primary care physicians in China. BMC Fam. Pract. 2021, 22, 224. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.