Abstract
The COVID-19 pandemic instigated a paradigm shift in healthcare delivery with a rapid adoption of technology-enabled models of care, particularly within the general practice primary care setting. The emergence of the Metaverse and its associated technology mediums, specifically extended reality (XR) technology, presents a promising opportunity for further industry transformation. Therefore, the objective of this study was to explore the current application and utilisation of XR technologies within the general practice primary care setting to establish a baseline for tracking its evolution and integration. A systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was conducted and registered with the international database of prospectively registered systematic reviews as PROSPERO-CRD42022339905. Eleven articles met the inclusion criteria and were quality appraised and included for review. All databases searched, inclusive of search terms, are supplied to enhance the transparency and reproducibility of the findings. All study interventions used virtual reality technology exclusively. The application of virtual reality within the primary care setting was grouped under three domains: (1) childhood vaccinations, (2) mental health, and (3) health promotion. There is immense potential for the future application of XR technologies within the general practice primary care setting. As technology evolves, healthcare practitioners, XR technology specialists, and researchers should collaborate to harness the full potential of implementing XR mediums.
1. Introduction
The COVID-19 pandemic has resulted in considerable disruption to the delivery of general practice primary healthcare services. Resources were diverted to address pandemic acuity, where pandemic policies significantly disrupted the delivery of healthcare services and necessitated the rapid adoption of technology-enabled service models of care [1,2]. Digital technologies, such as virtual telehealth care, were widely adopted and incentivised to facilitate remote patient and practitioner interactions, limiting person-to-person contact to reduce viral transmission [1,3,4]. After the pandemic, the ever-increasing prevalence of non-communicable chronic disease, multimorbidity, aging populations, and the threat of future pandemics continue to challenge already strained global health services necessitating the continued transformation of traditional patient care services [3,5]. The continued evolution and integration of digital technologies, including the adoption of metaverse-enabled immersive extended reality (XR) mediums, have the potential to play a primary role in this transformation, further augmenting consumer and primary care physician interactions [3,4].
1.1. Extended Reality (XR)
Extended reality (XR) is an umbrella term used to describe a spectrum or continuum of “virtuality” technology mediums that are designed to alter our real-world view, including augmented reality (AR), virtual reality (VR), and mixed reality (MR) [3,6]. At one end of the spectrum is AR, referring to technology that augments the real-world view by overlaying or superimposing virtual objects onto it. This is typically achieved by using hardware such as smart glasses or smartphone/tablet devices, allowing users to see the digital elements while permitting full visibility of the user’s real-world surroundings [3,7]. At the other end of the spectrum is VR, which significantly differs from AR and involves the use of head-mounted displays (HMDs) or headsets to block out the real world entirely. This allows users to be fully immersed in a computer-simulated three-dimensional (3D) environment, creating the physical and mental sensation of being in a virtual world [3,7]. In VR, users can interact with the virtual environment via the use of handheld controllers and receive direct sensory (images and sounds) feedback [8]. One fundamental aspect of VR is the concept of immersion [9]. Immersion refers to the extent to which users feel fully engaged and absorbed in a virtual environment, perceiving it as a substitute for their real-world surroundings. Currently, to achieve immersion, several different technological HMDs can be applied, ranging from simple devices (utilising mobile smartphones with compatible headsets) to more advanced systems, such as the HTC Vive and Oculus Rift (as displayed in Figure 1). Head-mounted displays are designed to substitute the user’s real visual senses, allowing them to perceive and interact with the virtual environment as if it were real. Mixed reality sits in the middle of the spectrum between AR and VR, further blending the real and virtual worlds within a single display [2,6]. In MR, the real and virtual worlds blend seamlessly, creating an environment where physical objects behave as if they were part of the virtual world [6]. This integration is generally achieved through the use of HMDs to create experiences for purposeful interactions [4].
Figure 1.
(A) Microsoft HoloLens 2. (B) Oculus Rift CV1. (C) HTC Vive. (D) Oculus Quest 2 [7].
1.2. The Metaverse
The metaverse is an evolving concept first described in the science fiction novel “Snow Crash” by Stephenson [10], who envisioned a virtual world that people could explore and interact with by use of digital avatars [11]. The metaverse essentially represents the extension of the virtuality continuum, representing the convergence of the real world into an immersive online and virtual interconnected environment that can be used for real-time interactions [12]. The metaverse at this time is further explained as an immersive internet computer simulation that can be accessed by using XR and other emerging accessory technologies [7,13]. The metaverse and its architecture are only limited by technological advancements, enabling the integration of artificial intelligence (AI), digital twin technology, telecommunications, the internet of medical things (IMOT), blockchain technology, wearables, and the integration of robotics [4]. The vision for the metaverse and its potential impact on healthcare as described by Musamih et al. [4] signifies an evolutionary shift wherein the physical world, involving healthcare personnel and patients, converges in a virtual realm known as the “metaverse”. Within this digital environment, real-world participants can engage with healthcare services and systems using digital avatars that mimic real-world point-of-care interactions [4].
Building towards the vision of the metaverse, the therapeutic application of XR technology within medicine is increasing. A systematic review by Tang et al. (2021) [14] identified several applications of XR technology within the specialties of surgery (50 studies), urology (18 studies), neurology (13 studies), and medical education (66 studies for medical doctors and 56 studies for medical students). A narrative review by López-Ojeda and Hurley [15] further identified emerging applications of XR technologies within cardiology, dentistry, oncology, pain medicine, immunology, anaesthetics, dermatology, emergency medicine, family and internal medicine, obstetrics and gynaecology, ophthalmology, pathology, paediatrics, preventative medicine, and radiology. While XR has found its place in areas such as surgery and medical education, its therapeutic applications within the general practice primary care setting is an area for future development. General practitioners working in primary care settings are often the first point of contact for individuals seeking medical assistance, with the quality of care provided at this juncture significantly influencing health-seeking behaviours [16]. Given the reductions in face-to-face care due to the COVID-19 pandemic, understanding how XR technologies can be harnessed to improve diagnostics, treatment, and patient engagement within the primary care setting is pivotal to the continued provision of evidenced-based compassionate care [16]. Therefore, the aim of this systematic review was to investigate the utilisation and application of XR technologies within the general practice primary care setting to establish a baseline with which to track its evolution and application into the future. In the subsequent sections, we present our systematic approach towards identifying articles for inclusion and quality appraisal, culminating in a narrative synthesis of findings that contributes new insights to the evidence base.
2. Materials and Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [17]. An a priori review protocol and eligibility criterion were registered with the National Institute for Health prospective register for systematic reviews PROSPERO (CRD42022339905).
2.1. Data Sources and Searches
The literature search terms and broad search of 10 databases was undertaken in June 2022 with the assistance of a research librarian (L.R.) using the following search terms and Boolean operators: primary health* OR primary care OR primary health care OR primary medical care OR general practi* OR GP OR family physician* OR family practice OR family medicine OR family care OR family health OR family doctor OR medical specialist OR specialist physician OR office visit* OR ambulatory care OR primary medical care OR medical clinic* OR medical office OR community care OR community medicine OR community health OR community mental health OR homecare OR home based OR home health OR home visit* Or preventative care OR preventative service* OR preventative program* OR preventative health OR health promotion OR ongoing care OR standard care AND virtual reality OR mixed reality OR augmented reality OR extended reality OT head mounted display* OR virtual environment OR immersive technolog* OR immersive system*. The databases searched included Medline, PsycInfo, Emcare, ProQuest—Computer Science Database, Computers and Applied Sciences—EBSCOhost, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus, IEEE Xplore, Web of Science, and the Cochrane Library. An additional hand search of results from Google Scholar and one institutional library search engine (Primo) was conducted. All searches were limited to the English language and limited to studies published within the last ten years as per Supplementary File S1.
2.2. Eligibility Criterion
Studies were eligible for inclusion if they met the following criterion: (1) full-text articles reporting on randomised controlled trials, observational studies (cohort studies, case—control studies, cross-sectional studies), non-randomised pre/post-test studies, pilot feasibility studies or study protocols, and (2) the study evaluated the use of immersive extended reality technology within the general practice primary care service setting.
2.3. Study Selection
All records retrieved from the primary search strategy were downloaded into Endnote (v20) reference management software for the removal of duplicates and screening. The first round of screening (title and abstract) was conducted independently (blinded) by reviewers (S.F. and D.J.). Records not meeting the eligibility criterion were coded and screened out in hierarchical order as follows: (i) not an eligible study design (NS), (ii) not an eligible population (NP), (iii) not an eligible intervention (NI), and (iv) not an outcome of interest (NO). To ensure consistency of the coding scheme and screening process, the first 50 citations were used to pilot the screening criteria with consensus achieved between the two reviewers. Following the first round of screening, the reviewers then came together to compare Endnote libraries. Any discrepancies with the coding criteria were discussed between the reviewers until a consensus was achieved (arbitration by a third reviewer was not required). All records marked for retrieval during the first round of screening were then retrieved in full text and subjected to a critical review and second round of screening, following the coding criteria outlined above.
2.4. Quality Appraisal
Articles identified for inclusion were independently assessed for quality by two reviewers (D.J. and P.I.) using the Meta-tool for Quality Appraisal of Public Health Evidence (MetaQAT) [18]. The MetaQAT tool was chosen for its ability to appraise specific and generic (heterogenous) studies with high levels of rigor against four main criteria, including (1) relevance to the topic or research question; (2) reliability, assessing the level of transparency and quality of reporting; (3) validity, assessing the risk of bias; and (4) applicability, assessing the application of study findings for public health practice [18]. Written justification for answers (yes, no, unclear, and not applicable) to each criterion was required [18]. No articles in this review were excluded based on quality appraisal.
2.5. Data Extraction
Data extracted from each study included study characteristics (title, author/s, year, and country of publication), study design, methodology (participants, randomisation, blinding, instruments, tools), intervention (type and use of XR technology), and outcomes (analysis, study endpoints, results of adverse events, follow-up). Data extraction was conducted independently by reviewers (P.L., P.M., R.G., D.E., R.R.) and checked by the lead reviewer (D.J.).
3. Results
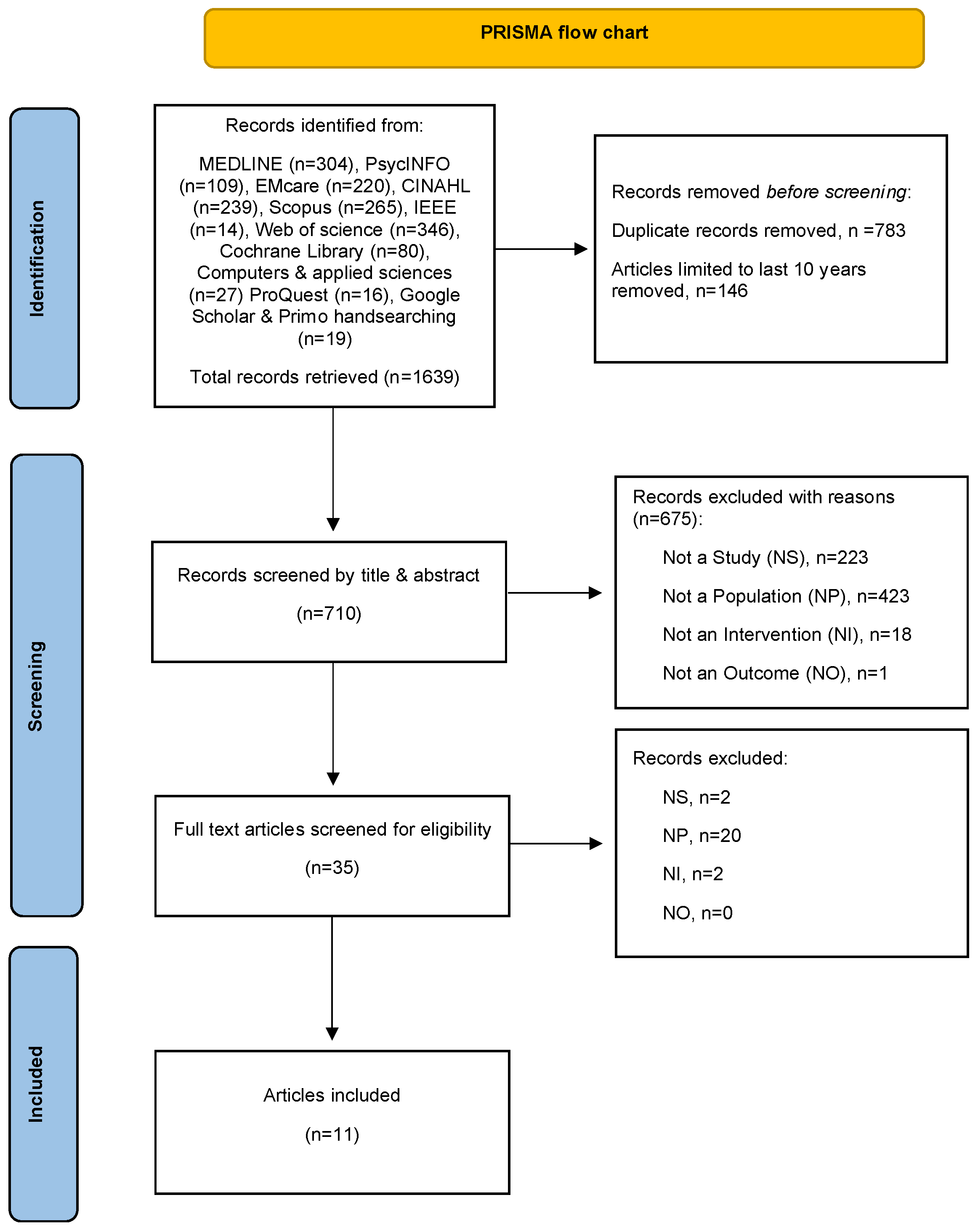
As per the flowchart illustrated in Figure 2, the comprehensive search strategy identified 1639 records. After duplicates were removed and date limitations were applied, 710 records were subject to the first round of screening (by title and abstract). Following the second round of screening, 11 articles (7 study papers and 4 study protocols) met the review criteria and were subject to quality appraisal. As anticipated in the review protocol, the heterogeneity of included articles, intervention types, and outcome measures precluded any pooling of results for meta-analysis, with the results presented as a narrative synthesis instead.
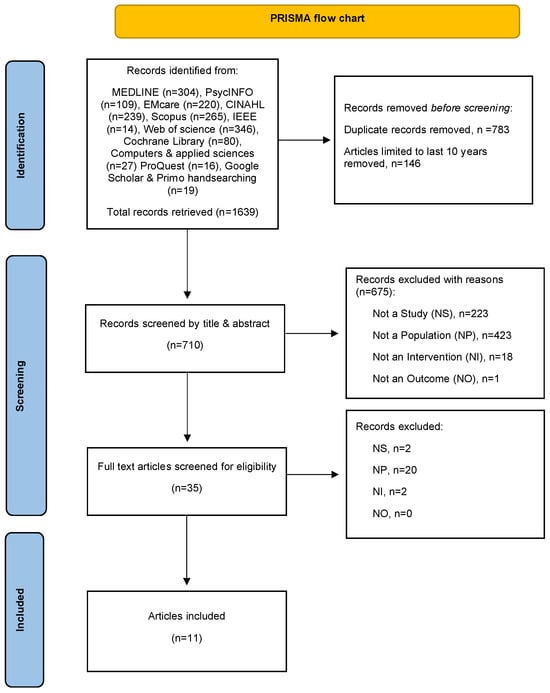
Figure 2.
PRISMA flow chart [19].
3.1. Study Characteristics
A summary of all included articles is presented in Table 1. Article publication dates ranged between 2018 and 2022, with studies conducted in Singapore [20,21,22,23], Spain [24,25], Brazil [26], Sweden [27], the United States of America [28], Australia [29], and Saudi Arabia [30]. Of the included articles, nine interventions were identified, with all interventions designed for and deployed using virtual reality technology.

Table 1.
Study characteristics.
In terms of the study design, most articles described or conducted randomised controlled trials (RCTs) to test the feasibility and effectiveness of interventions, with or without qualitative participant data collection. The number of participants in these studies ranged between 12 and 116, with the age of participants ranging between 4 years old and 74 years old [20,22,23,25,27,28,30]. All seven study papers were deemed to be transparent and rigorous when assessed using the MetaQAT quality appraisal tool. The four protocol papers [21,24,26,29] received a not applicable rating for the applicability to public health criteria due to an absence of outcome data, as per Supplementary File S2. All interventions were grouped according to their healthcare application and synthesised under three overarching domains as follows.
3.2. IVR for Childhood Vaccinations
Two study papers [20,30] and two protocol papers [24,29] applied VR technology to reduce pain and/or fear associated with childhood vaccinations. Althumairi et al. [30] described the implementation of a 2 min, 3D-animated story experience (using Future Sight HMD by Melko Inc™) amongst children (n = 104) aged between 4 and 6 years. In this study, the VR story experience was simultaneously projected to a practice nurse, ensuring synchronisation of the VR experience with the vaccination procedure [30]. Using a non-randomised trial design, lower mean pain scores (as measured using the Wong-Baker face pain rating scale) and lower mean fear scores (measured using the children’s fear scale) were observed for those that received the VR intervention compared to those who did not [30].
The second study by Change et al. [20] conducted a proof-of-concept feasibility and single-centre RCT to test the analgesic effect of their VR intervention. Children in this study (n = 30 aged between 4 and 10 years) were exposed to a 2 min, purpose-built cartoon animation called the Soothing Immunisation Leveraging on Virtual Reality Experience (SILVER). In this study, both the parents and nursing staff anxiety scores were also measured prior to the vaccination procedure [20]. Based on an intention to treat (ITT) analysis, no differences in the children’s pain scores (as measured using the revised FACES pain scale) were observed between the intervention and control groups. Statistically significant lower fear scores (as measured using the children’s fear scale) were observed for those in the intervention group. Parental anxiety scores were also observed to be significantly lower for those who had children allocated to the intervention group [20].
The study protocol by Ellerton et al. [29] proposed the testing of The Virtual Reality for IMMunisation (VRIMM) experience using an RCT study design to evaluate its effectiveness as a diversional tactic for children receiving their 4-year-old vaccinations. The VR experience was described as a brief (1 min) interactive marine adventure beginning with a relaxation sequence and progressing to underwater scenes that included gaze-based tracking of virtual fish [29]. Vaccination administration occurred after 30 s from the commencement of the experience, with the revised FACES pain scale used as the primary outcome measure. Lastly, the protocol by Harrera et al. [29] also proposed the conduct of an RCT to evaluate the use of VR experience as an analgesic for childhood vaccinations for children aged 3–6 years. A purpose-built VR experience described as “Leia’s World” (VR Pharma Immersive Technologies SL) was deployed using Pico G2 VR goggles, with the efficacy measured using the FACES pain scale and children’s fear scale [29].
3.3. IVR for Mental Health Therapy or Assessment
Three papers reported on the design and testing of the Cognitive Assessment by Virtual Reality (CAVIRE) intervention [21,22,23]. Co-developed by a multidisciplinary team, the CAVIRE program (using the HTC VIVE Pro HMD with Leap Motion controller) assesses six cognitive domains, including (1) perceptual motor function, (2) executive function, (3) complex attention, (4) social cognition, (5) learning memory and (6) language.
Wong et al. [23] evaluated the feasibility of the CAIVRE system by comparing VR completion times with a traditional (written) assessment (Montreal Cognitive Assessment) amongst a cohort of cognitively healthy adults of various ages. Using a non-experimental design, the results indicate that the completion times for the CAVIRE system were significantly shorter than those from completing traditional paper-based assessments across all age groups [23]. Age-related differences in completion times were reported, whereby younger adults completed the assessments quicker than those in older age groups [23]. High levels of acceptability for the CAIVRE system were observed amongst participants, with 92% indicating that they found the CAVIRE system easy to use and 90% indicating that they would be willing to use the system again [23].
Tan et al. [22] further reported pilot study outcomes again using the CAIVRE system amongst healthy adults of various ages. Findings included within this article observed that younger aged adults achieved statistically significantly higher cognitive assessment scores compared with the older participants across all six cognitive domains.
Navarro-Haro et al. [25] and Polomo et al. [26] both proposed the use of VR for the delivery of mindfulness-based therapies. Navarro-Haro et al. [25] conducted a pilot RCT to test a purpose-built VR mindfulness-based skills training intervention (VR-DBT®) that was designed to reduce the symptoms of generalised anxiety disorder in people prone to attention deficits. Participants were randomly assigned to receive either a mindfulness-based intervention in a group setting without VR or a mindfulness-based group intervention and VR [25]. During the VR sessions, participants were seated and fitted with the Oculus Rift DK2 HMD with head tracking. The VR-DBT® experience was described as a “Mindful River World”, whereby participants floated slowly down a virtual river with trees, boulders, and mountains whilst listening to mindfulness skills via audio [25]. Using a pre- and post-design, both groups evidenced lower anxiety scores; however, those receiving mindfulness + VR were observed to be more adherent to their treatment when compared with those engaged in traditional mindfulness group-based therapy without VR.
Polomo et al. [26] presented a study protocol proposing the conduct of an RCT to test the feasibility and preliminary efficacy of a VR mindfulness training experience for people with multimorbidity. The VR experience adapted from an 8-week mindfulness-based health promotion program by Jon Kabat-Zinn was suggested to be developed. The VR experience will involve participants being immersed in a meditation room with an avatar of a mindfulness instructor where users can visualise themselves as an avatar within the experience [26]. In this VR experience, the instructor avatar conducts the formal practice of mindfulness using imaginative scenarios. Approximately ten different imaginative scenarios are to be created. Outcome measures for evaluation include a mindfulness scale (MAAS), quality of life (SF-36), Self-Compassion Scale (SCS), depression and anxiety scale (HADS), Viability of Technology Scale (VTS), and a sociodemographic questionnaire [26].
Lundin et al. [27] described the testing of a novel VR–cognitive behavioural therapy (VR-CBT) intervention designed for the treatment of people with panic disorders and agoraphobia (PDA). Developed in collaboration with psychologists, clinical researchers, human–computer interaction researchers, and filmmakers, a 360-degree video was used to create virtual environments (VEs) (Lundin et al. 2022). The virtual environments used for the VR-CBT were situations feared and avoided by individuals with PDA, including being in a subway carriage, in a walking tunnel, in a busy train station, in an elevator, in an auditorium, and on a tall bridge [26]. Environments were selected in collaboration with the patient and were typically those that simulated or resembled situations that the patient found anxiety-provoking in real life. Pre- and post-test measures used for evaluation suggest (n = 12 participants) that VR-CBT demonstrated a significant reduction in agoraphobic avoidance and panic disorder scores from baseline to post-treatment [27].
3.4. IVR for Health Promotion/Disease Prevention
Under the framework of a pilot RCT, Gibson et al. [28] aimed to determine whether presenting brief motivational videos in VR vs. mobile 360° video had differential effects on risk perceptions and enrolment in a diabetes prevention program. Participants (n = 116) in this study were randomised to one of two study groups, namely, mobile 360° video and mobile VR, and completed pre- and post-evaluation measures. The videos developed demonstrate the possible negative future complications of diabetes [28]. Those assigned to the mobile 360° video group watched the videos on their smartphone (the viewer moved their phone to “look around” the world of the movie), while those assigned to mobile VR watched the videos using their smartphone inside a cardboard VR headset with headphones. The results suggest no significant differences in the risk perception scores in those who used VR compared with using a mobile device [28].
4. Discussion
This systematic review provides a baseline for the use of extended reality (XR) technology implemented within the general practice primary care setting. Although there is a long way to go before the level of technology integration is seamless at the point of care service level or can be provided within the metaverse as envisaged by Musamih et al. [4], this review has determined both practical and novel therapeutic applications of VR technology mediums in this context.
Many of the studies included in this review examined the use of VR as a distraction technique for children receiving immunisations in the primary care setting [20,24,29,30]. Observed reductions in children’s fear scores suggest potential improvements in the patient’s experience of this procedure. For most children, medical procedures often provoke fear and anxiety. Not only can these procedures hamper recovery and lead to post-traumatic stress symptoms but they may also become the catalyst for the avoidance of health care later in life [31]. The use of VR in this context shows promise and may go some way to reducing fear associated with childhood vaccinations, which improves the overall patient experience and reduces distress in children. Chang et al. [20] revealed a unique finding whereby the use of VR for childhood immunisations also reduced the anxiety levels of the child’s parents. That is, just by witnessing less procedure-induced fear from their children, the parents’ stress levels were decreased [20]. Therefore, VR as an intervention to reduce stress levels may have a meaningful impact on improving the overall wellness of patients and their families, potentially enhancing adherence to child immunisation schedules.
While the use of VR as a method to alleviate pain associated with childhood vaccinations has yielded mixed results [20,24,29,30], indicating the need for further research investigation, a recent systematic review and meta-analysis by Huang et al. [32] suggests that VR holds promise as a potential analgesic. The review aimed to assess the effectiveness of VR exposure for pain management in terms of pain intensity and types (acute and chronic) amongst adult (>18 yrs) and juvenile (<18 yrs) age groups. A meta-analysis of 26 pooled studies that evaluated pain intensity as the primary outcome (using the visual analogue scale) observed lower pain scores for those in the intervention groups compared with those receiving usual care (WMD −1.62; 95% CI −1.86, −1.38; p < 0.001). A subgroup analysis of both juvenile and adult participants also observed reductions in pain intensity for those exposed to VR [32]. An analysis of types of pain additionally observed that those in the VR group evidenced lower pain scores in response to an acute pain stimulus, with no difference in pain scores evidenced for those with chronic pain [32].
The application of VR as an emerging technology in the field of mental health shows the potential to enrich the delivery of traditional assessments and therapies [33,34]. Mental health disorders, such as anxiety, depression, and post-traumatic stress, continue to afflict a significant proportion of global populations, with the availability of qualified mental health professionals suggested to be unable to meet demand, particularly for people residing outside of urban areas [34,35]. Within this context, the feasibility of remotely delivering mental health therapies under the stewardship of a qualified medical practitioner holds promise for overcoming workforce and geographic barriers. In response to these challenges, VR interventions emerge as potential adjuncts to traditional therapies adaptable to various self-guided treatment programs. For example, VR can safely expose patients to anxiety-inducing stimuli, such as crowded spaces or heights, in a safe and controlled manner [27,36,37]. Additionally, mindfulness-based interventions have gained popularity in mental health treatment, with the use of VR offering a unique platform for which to provide tailored practices that facilitate relaxation, stress reduction, and emotional regulation [25,34].
One distinct application of VR identified in this review is the application of VR for health promotion. The role of VR in confirming and enhancing behavioural strategies, self-motivation, goal setting, problem-solving, and self-reinforcement is emerging [38]. Leveraging this capacity, VR has the potential to augment health promotion efforts in various conditions, including obesity, testicular disorder awareness, smoking cessation, and type 2 diabetes [28,38,39,40]. However, the application of VR for health promotion in the primary care setting remains in its infancy, with the work by Gibson et al. [28] offering the only perspectives in this context. Gibson’s study employed VR as a motivational tool to potentially prevent type 2 diabetes, and although measures of engagement or behaviour change were not conducted, this work demonstrates additional applications of this technology [28]. Further investigation is warranted to explore the efficacy and feasibility of VR interventions within primary care, which can contribute to advancing health literacy.
As evidenced in this review, the application of VR in the general practice primary care setting encompasses a range of hardware and software. Diverse VR hardware ranging from the most basic cardboard VR that uses one’s own smartphone [28] to more sophisticated systems, such as the Oculus Quest, were used [20]. Achieving standardisation in VR hardware is an ongoing process, evolving alongside technological advancements. A lack of standardisation can lead to variations in the perceived quality of VR experiences, which influences the overall satisfaction with VR interventions and requires consideration in future research studies. In terms of software, a crucial consideration is the collaborative design or co-design of VR applications in the healthcare context [41,42,43]. While the principles of collaborative design are acknowledged in VR research, its widespread implementation remains limited. Among the studies included in this review, only four detailed the involvement of patients, clinicians, and developers in the design process [20,21,27,28]. While VR holds promise in enhancing patient experiences, treatment outcomes, and engagement in primary care interventions, the incorporation of collaborative design principles could further amplify their impact.
Limitations
To our knowledge, this was the first systematic review to evaluate the application of XR technologies within the general practice primary medical care setting. Although a rigorous methodology was followed, the inherent value of conducting a meta-analysis within the context of systematic reviews is undeniable [44,45]. Given that the application of XR technologies is in its infancy and very much an emerging field of investigation, a meta-analysis was not feasible and this is a primary limitation of this review.
5. Conclusions
This methodically rigorous systematic review and narrative synthesis laid out the foundations for tracking the evolution and application of XR technologies within the general practice primary care setting. Although an emerging field within this context, our analysis revealed that XR mediums, specifically VR, show potential for reducing the fear associated with childhood immunisations, enabling the delivery of personalised mental health assessments and therapies, and acting as a potential medium for the delivery of health-promoting content. There is immense potential for the future application of XR technologies within the general practice primary care setting to augment current practice, improve adherence to treatment plans, and enhance the overall patient care experience. As technology evolves, healthcare practitioners, XR technology specialists, and researchers should collaborate to harness the full potential of implementing XR mediums within this context to support the delivery of innovative, quality and compassionate medical care.
Supplementary Materials
The following supporting information can be downloaded from https://www.mdpi.com/article/10.3390/virtualworlds2040021/s1: Supplementary File S1. Systematic review search results June 2022; Supplementary File S2. MetaQAT quality appraisal.
Author Contributions
Conceptualisation—D.J., S.F. and P.I. contributed to the conception and methodological design of the study. Methodology—L.R. was responsible for the search strategy development and primary electronic database search; D.J. and S.F. were responsible for the article screening; D.J. and P.I. were responsible for the quality appraisal; and R.G., D.E., P.S.M., P.I., P.L. and R.R. were responsible for the data extraction. All authors contributed to the writing and reviewing of the manuscript and the preparation and review of tables. M.H. undertook critical review of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Matenge, S.; Sturgiss, E.; Desborough, J.; Dykgraaf, S.H.; Dut, G.; Kidd, M. Ensuring the continuation of routine primary care during the COVID-19 pandemic: A review of the international literature. Fam. Pract. 2021, 39, 747–761. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S. Use of Extended Reality in Medicine During the COVID-19 Pandemic. In Extended Reality Usage During COVID 19 Pandemic; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1–14. [Google Scholar]
- Chengoden, R.; Victor, N.; Huynh-The, T.; Yenduri, G.; Jhaveri, R.H.; Alazab, M.; Bhattacharya, S.; Hegde, P.; Maddikunta, P.K.R.; Gadekallu, T.R. Metaverse for Healthcare: A Survey on Potential Applications, Challenges and Future Directions. arXiv 2022, arXiv:2209.04160. [Google Scholar] [CrossRef]
- Musamih, A.; Yaqoob, I.; Salah, K.; Jayaraman, R.; Al-Hammadi, Y.; Omar, M.; Ellahham, S. Metaverse in Healthcare Applications Challenges and Future Directions. IEEE Consum. Electron. Mag. 2022, 12, 33–46. [Google Scholar] [CrossRef]
- Sun, M.; Xie, L.; Liu, Y.; Li, K.; Jiang, B.; Lu, Y.; Yang, Y.; Yu, H.; Song, Y.; Bai, C.; et al. The Metaverse in Current Digital Medicine. Clin. eHealth 2022, 5, 52–57. [Google Scholar] [CrossRef]
- Milgram, P.; Kishino, F. A taxonomy of mixed reality visual displays. IEICE Trans. Inf. Syst. 1994, 77, 1321–1329. [Google Scholar]
- Bansal, G.; Rajgopal, K.; Chamola, V.; Xiong, Z.; Niyato, D. Healthcare in Metaverse: A Survey on Current Metaverse Applications in Healthcare. IEEE Access 2022, 10, 119914–119946. [Google Scholar] [CrossRef]
- Fealy, S.; Jones, D.; Hutton, A.; Graham, K.; McNeill, L.; Sweet, L.; Hazelton, M. The integration of immersive virtual reality in tertiary nursing and midwifery education: A scoping review. Nurse Educ. Today 2019, 79, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Verma, J.K.; Paul, S. Augmented Reality and Virtual Reality Creating Ripple in Medical and Pharmaceutical World; Springer Singapore Pte. Limited: Singapore, 2022; Volume 998. [Google Scholar]
- Stephenson, N. Snow Crash; Bantum Books: New York, NY, USA, 1992. [Google Scholar]
- Tacgin, Z.; Hagin, A. Enhanced Learning Environments Technology and Innovation, 1st ed.; Zeynep Tacgin, A.H., Ed.; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2022. [Google Scholar]
- Skalidis, I.; Fournier, S.; Skalidis, E.; Maurizi, N. Virtual hospitals and digital doctors: How far are we from the CardioVerse? Eur. Heart J. 2022, 44, 7–9. [Google Scholar] [CrossRef]
- Yang, D.; Zhou, J.; Chen, R.; Song, Y.; Song, Z.; Zhang, X.; Wang, Q.; Wang, K.; Zhou, C.; Sun, J.; et al. Expert consensus on the metaverse in medicine. Clin. eHealth 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Tang, Y.M.; Chau, K.Y.; Kwok, A.P.K.; Zhu, T.; Ma, X. A systematic review of immersive technology applications for medical practice and education—Trends, application areas, recipients, teaching contents, evaluation methods, and performance. Educ. Res. Rev. 2021, 35, 100429. [Google Scholar] [CrossRef]
- López-Ojeda, W.; Hurley, R.A. Extended-reality technologies: An overview of emerging applications in medical education and clinical care. J. Neuropsychiatry Clin. Neurosci. 2021, 33, A4-177. [Google Scholar] [CrossRef] [PubMed]
- Shea, S.; Lionis, C. Compassionate Care within the Primary Health Care Setting: Before and During a Public Health Crisis. In The Art and Science of Compassionate Care: A Practical Guide; Springer: Berlin/Heidelberg, Germany, 2023; pp. 43–59. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Rosella, L.; Bowman, C.; Pach, B.; Morgan, S.; Fitzpatrick, T.; Goel, V. The development and validation of a meta-tool for quality appraisal of public health evidence: Meta Quality Appraisal Tool (MetaQAT). Public Health 2016, 136, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Chang, Z.Y.; Kang, G.C.-Y.; Koh, E.Y.L.; Fong, R.J.K.; Tang, J.; Goh, C.K.; Tan, N.C. Immersive Virtual Reality in Alleviating Pain and Anxiety in Children During Immunization in Primary Care: A Pilot Randomized Controlled Trial. Front. Pediatr. 2022, 10, 847257. [Google Scholar] [CrossRef]
- Lim, J.E.; Wong, W.T.; Teh, T.A.; Lim, S.H.; Allen, J.C.; Quah, J.H.M.; Malhotra, R.; Tan, N.C. A Fully-Immersive and Automated Virtual Reality System to Assess the Six Domains of Cognition: Protocol for a Feasibility Study. Front. Aging Neurosci. 2021, 12, 604670. [Google Scholar] [CrossRef]
- Tan, N.C.; Lim, J.E.; Allen, J.C.; Wong, W.T.; Quah, J.H.M.; Muthulakshmi, P.; Teh, T.A.; Lim, S.H.; Malhotra, R. Age-Related Performance in Using a Fully Immersive and Automated Virtual Reality System to Assess Cognitive Function. Front. Psychol. 2022, 13, 847590. [Google Scholar] [CrossRef]
- Wong, W.T.; Tan, N.C.; Lim, J.E.; Allen, J.C.; Lee, W.S.; Quah, J.H.M.; Paulpandi, M.; Teh, T.A.; Lim, S.H.; Malhotra, R. Comparison of Time Taken to Assess Cognitive Function Using a Fully Immersive and Automated Virtual Reality System vs. the Montreal Cognitive Assessment. Front. Aging Neurosci. 2021, 13, 756891. [Google Scholar] [CrossRef]
- Herrera, M.d.l.C.; Fuster-Casanovas, A.; Catalina, Q.M.; Mensa, M.C.; Pinillos, P.A.; Guitart, I.V.; Carrión, S.G.; Vidal-Alaball, J. Use of Virtual Reality in the Reduction of Pain After the Administration of Vaccines Among Children in Primary Care Centers: Protocol for a Randomized Clinical Trial. JMIR Res. Protoc. 2022, 11, e35910. [Google Scholar] [CrossRef]
- Navarro-Haro, M.V.; Modrego-Alarcón, M.; Hoffman, H.G.; López-Montoyo, A.; Navarro-Gil, M.; Montero-Marin, J.; García-Palacios, A.; Borao, L.; García-Campayo, J. Evaluation of a Mindfulness-Based Intervention With and Without Virtual Reality Dialectical Behavior Therapy® Mindfulness Skills Training for the Treatment of Generalized Anxiety Disorder in Primary Care: A Pilot Study. Front. Psychol. 2019, 10, 55. [Google Scholar] [CrossRef]
- Palomo, P.; Rodrigues de Oliveira, D. Study Protocol for a randomized controlled trial of mindfulness training with immersive technology (virtual reality) to improve the quality of life of patients with multimorbidity in Primary Care- the Mindful-VR study. Annu. Rev. Cyber Ther. Telemed. 2018, 16, 140–147. [Google Scholar]
- Lundin, J.; Lundström, A.; Gulliksen, J.; Blendulf, J.; Ejeby, K.; Nyman, H.; Björkander, D.; Hedman-Lagerlöf, E. Using 360-degree videos for virtual reality exposure in CBT for panic disorder with agoraphobia: A feasibility study. Behav. Cogn. Psychother. 2022, 50, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Gibson, B.; Simonsen, S.; Jensen, J.D.; Yingling, L.; Schaefer, J.; Sundaresh, V.; Zhang, Y.; Altizer, R. Mobile Virtual Reality Versus Mobile 360° Video to Promote Enrollment in the Diabetes Prevention Program Among Hispanic Adults: Pilot Study. JMIR Diabetes 2022, 7, e26013. [Google Scholar] [CrossRef] [PubMed]
- Ellerton, K.; Tharmarajah, H.; Medres, R.; Brown, L.; Ringelblum, D.; Vogel, K.; Dolphin, A.; McKellar, S.; Bridson, F.; John-White, M.; et al. The VRIMM study: Virtual Reality for IMMunisation pain in young children—Protocol for a randomised controlled trial. BMJ Open 2020, 10, e038354. [Google Scholar] [CrossRef]
- Althumairi, A.; Sahwan, M.; Alsaleh, S.; Alabduljobar, Z.; Aljabri, D. Virtual Reality: Is It Helping Children Cope with Fear and Pain During Vaccination? J. Multidiscip. Healthc. 2021, 14, 2625–2632. [Google Scholar] [CrossRef]
- Eijlers, R.; Utens, E.M.W.J.; Staals, L.M.; Nijs, P.F.A.d.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Systematic Review and Meta-analysis of Virtual Reality in Pediatrics: Effects on Pain and Anxiety. Anesth. Analg. 2019, 129, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Lin, J.; Han, R.; Peng, C.; Huang, A. Using Virtual Reality Exposure Therapy in Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Value Health 2022, 25, 288–301. [Google Scholar] [CrossRef]
- Riva, G.; Serino, S. Virtual Reality in the Assessment, Understanding and Treatment of Mental Health Disorders. J. Clin. Med. 2020, 9, 3434. [Google Scholar] [CrossRef]
- Thunström, A.O.; Sarajlic Vukovic, I.; Ali, L.; Larson, T.; Steingrimsson, S. Prevalence of virtual reality (VR) games found through mental health categories on STEAM: A first look at VR on commercial platforms as tools for therapy. Nord. J. Psychiatry 2022, 76, 474–485. [Google Scholar] [CrossRef]
- Asiain, J.; Braun, M.; Roussos, A.J. Virtual reality as a psychotherapeutic tool: Current uses and limitations. Br. J. Guid. Couns. 2022, 50, 1–28. [Google Scholar] [CrossRef]
- Baghaei, N.; Chitale, V.; Hlasnik, A.; Stemmet, L.; Liang, H.-N.; Porter, R. Virtual Reality for Supporting the Treatment of Depression and Anxiety: Scoping Review. JMIR Ment. Health 2021, 8, e29681. [Google Scholar] [CrossRef] [PubMed]
- Best, P.; Meireles, M.; Schroeder, F.; Montgomery, L.; Maddock, A.; Davidson, G.; Galway, K.; Trainor, D.; Campbell, A.; Van Daele, T. Freely Available Virtual Reality Experiences as Tools to Support Mental Health Therapy: A Systematic Scoping Review and Consensus Based Interdisciplinary Analysis. J. Technol. Behav. Sci. 2022, 7, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Al-Rasheed, A.; Alabdulkreem, E.; Alduailij, M.; Alduailij, M.; Alhalabi, W.; Alharbi, S.; Lytras, M.D. Virtual Reality in the Treatment of Patients with Overweight and Obesity: A Systematic Review. Sustainability 2022, 14, 3324. [Google Scholar] [CrossRef]
- Keijsers, M.; Vega-Corredor, M.C.; Hoermann, S.; Tomintz, M. Virtual Reality Technology Use in Cigarette Craving and Smoking Interventions (I “Virtually” Quit): Systematic Review. J. Med. Internet Res. 2021, 23, e24307. [Google Scholar] [CrossRef] [PubMed]
- Saab, M.M.; Landers, M.; Cooke, E.; Murphy, D.; Hegarty, J. Feasibility and usability of a virtual reality intervention to enhance men’s awareness of testicular disorders (E-MAT). Virtual Real. J. Virtual Real. Soc. 2019, 23, 169–178. [Google Scholar] [CrossRef]
- Bryant, L.; Sedlarevic, N.; Stubbs, P.; Bailey, B.; Nguyen, V.; Bluff, A.; Barnett, D.; Estela, M.; Hayes, C.; Jacobs, C.; et al. Collaborative co-design and evaluation of an immersive virtual reality application prototype for communication rehabilitation (DISCOVR prototype). Disabil. Rehabil. Assist. Technol. 2022. ahead of print. [Google Scholar] [CrossRef]
- Desselle, M.R.; Holland, L.R.; McKittrick, A.; Kennedy, G.; Yates, P.; Brown, J. “A Wanderer’s Tale”: The development of a virtual reality application for pain and quality of life in Australian burns and oncology patients. Palliat. Support. Care 2023, 21, 454–460. [Google Scholar] [CrossRef]
- Liddicoat, S. Mental health facility codesign: A new research method for integrating the service user voice in design processes using virtual reality. Gen. Psychiatry 2019, 32, e100061. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Pati, D.; Lorusso, L.N. How to Write a Systematic Review of the Literature. HERD Health Environ. Res. Des. J. 2018, 11, 15–30. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).