Abstract
The musculocutaneous nerve (MCN) is the terminal branch of the lateral cord of the brachial plexus, and emerges at the inferior border of pectoralis minor muscle. The nerve can interact with the median nerve (MN), adhering to the nerve and sharing fibers with it. During anatomical dissection of twelve cadavers, we have detected a rare variation of the anastomosis between MCN and MN. The knowledge of this anatomical variation could be of great relevance during surgical and clinical practices.
1. Introduction
The musculocutaneous nerve (MCN) and the median nerve (MN) derive from the brachial plexus, that is usually formed by the union of the ventral rami of the four lower cervical spinal nerves and the first thoracic spinal nerve (C5-T1) []. These nerves are two of the four terminal nerves of the brachial plexus; communications between MCN and the MN are often observed due to failed nerve fiber segregation during embryological development [].
In its most common anatomic form, the MCN arises from the lateral cord of the brachial plexus, pierces and innervates the coracobrachialis muscle (CBM), descending between the biceps brachii and the brachialis muscles. It then continues into the forearm as the lateral antebrachial cutaneous nerve []. The MCN runs laterally to the MN and innervates the anterior arm muscles and the skin covering the lateral surface of the forearm.
The lateral and medial roots of the MN originate from the lateral and medial cords of the brachial plexus, respectively. In the arm, the MN has no branches and is located medially to the coracobrachialis muscle, entering the forearm through the cubital fossa, passing posteriorly to the flexor retinaculum at the wrist, and through the carpal tunnel to reach the palmar aspect of the hand. The MN supplies most of the anterior forearm and thenar muscles, in addition its sensory fibers laterally innervating the palmar surface of the hand and the dorsal surface of digits I-III at the level of the distal phalanx [,]. In Figure 1, we have presented the classical localization of the above-mentioned nerves in the axillary region.
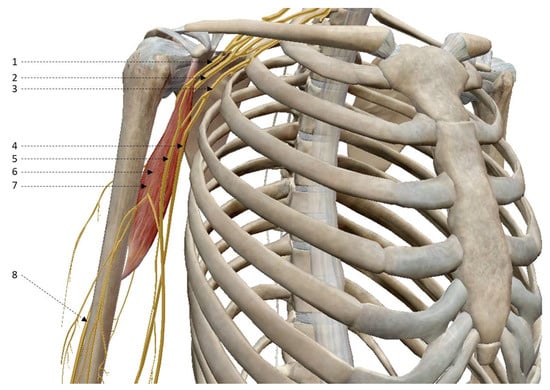
Figure 1.
Anatomical relationship between the musculocutaneous nerve and median nerve in the axillary region. Right upper limb, front vision. 1, lateral cord of brachial plexus; 2, posterior cord of brachial plexus; 3, medial cord of brachial plexus; 4, ulnar nerve; 5, median nerve; 6, coracobrachialis muscle; 7, musculocutaneous nerve; 8, radial nerve.
Anatomical variations of the communication between the MCN and the MN are relatively common as a consequence of different factors during embryological development. Anastomoses between the MNC and the MN have been described in literature []; in particular, the most commonly used classification proposed by Le Minor divides the existing topographic relations between the MCN and the MN into five categories []. Other classifications have been suggested by Guerri-Guttenberg and Inglotti [] and Venieratos and Anangnostopolou [].
During the 2018 summer school of anatomical dissection at the laboratory of the Medical University of Gdansk, we had the opportunity to dissect twelve cadavers. Here, we report a case of a rare anatomical variation of an anastomosis between the MCN and MN, which does not correspond to the standard classifications.
2. Materials and Methods
Dissections were performed on 12 adult donor corpses (eight males and four females) of Caucasian race. In particular, 12 bilateral upper limbs (24 limbs) were studied. Age of cadavers at time of death varied between 56–87 years (mean—79.56 years, median—78 years). Cadavers were dissected at the laboratory of the Department of Anatomy and Neurobiology, Medical University of Gdansk, Poland, during a summer school of anatomical dissection. Causes of death were unknown. All cadavers did not present lesions and had no history upper limb surgery. All human cadaveric tissues used in the study were derived from donors who gave their written consent, premortem, to the use of their body for educational and scientific purposes. Gratitude to the donor cadavers and their families is expressed within the Acknowledgments section, in accordance with the formula proposed recently by 20 editors-in-chief of 17 anatomical journals []. The Institutional Ethics Committee gave approval for conducting this study (Institutional Review Board number: Ordinance No. 26/2016 of the Rector of the Medical University of Gdańsk of 6 June 2016 on the implementation of the “Program of Conscious Donation of Corpses”).
Deep dissection of upper limbs was performed in formalin-fixed adult human cadavers. The upper limbs were removed from the body, the arm positioned in a supine position, the skin incised and every fat layer was carefully removed not to damage vessels and nerves. Subsequently, the brachial fascia was separated from the underlying muscles and intermuscular septa, and three muscles of the anterior arm compartment (coracobrachialis, brachialis and biceps brachii) were separated. Finally, the musculocutaneous nerve and median nerve were identified and separated.
The following 3D image (Figure 1) depicting the region of interest was created with the “Human Anatomy Atlas” virtual anatomy software, supplied by the laboratory of the Human Anatomy section of the University of Palermo.
The morphological analysis of the MCN and MN consisted of the assessment of: (a) relationship of the MCN and CBM (observation if the MCN goes through the CBM or not); (b) lateral root of the MN (measurement of length and width); (c) medial root of the MN (measurement of length and width); (d) MN on the arm (measurement of length until the cubital fossa and width); (e) MCN (measurement of length and width of an upper part—till CBM, and lower part—till the point where muscular branches to biceps brachii m. emerge from the MCN). The measurements, length and width, have been taken with line ruler and Digital Digimatic Vernier Caliper (Mitutoyo, Japan), respectively. All measurements were carried out by the same investigator. Each measurement was taken twice, and accurate to the 1 mm (length) and 0.1 mm (width). As the final result, the average of both measurements was taken.
3. Results
In 23 out of the 24 cases studied, the MCN and the MN showed a typical morphology as per the classical anatomical description. The results obtained for individual parameters in the studied cases are summarized in Table 1. A representative case of the anatomical relationship between the musculocutaneous nerve and median nerve is shown in Figure 2. In all cases observed, except case 4 bilaterally, the MCN pierces the coracobrachialis muscle (Table 1). In one of the studied cases (case 9, see Table 1), the right upper limb of a male donor, we observed an anastomosis between the MCN and the MN (Figure 3). The MCN, after piercing the coracobrachialis muscle, continued its course descending laterally between the brachialis muscle and the biceps brachii muscle, innervating all three of them. 19 cm from its origin, at the lateral cord of the brachial plexus and 10 cm above the cubital fossa, the MCN anastomosed with the MN (Figure 3, point 7). At the anastomotic site, the two nerves were attached to each other, side-to-side, for a span of 1.7 cm, and some fibers were shared between the MCN and the MN. The roots of the MN originated from the lateral and medial cords of the brachial plexus, joined in a single trunk in the axilla and extended along the forearm. On the arm, just 10 cm above the cubital fossa, 15 cm from the union of the medial and lateral root of the MN, the anastomosis between the MN and the MCN was observed (Figure 3, point 7). This anastomosis between the MCN and the MN represents a new anatomical subvariant, since it does not fall neither within the classical Le Minor [], nor within the Venieratos and Anangnostopolou [] classifications. No vascular variations were observed in this case. Dissection using the same methods was also performed on the left upper limb of the same donor to study if the variation was present also in the other arm. Upon dissection of the left upper limb (axilla, arm, forearm), no anatomical variants were observed.

Table 1.
Measurements of the observed structures.
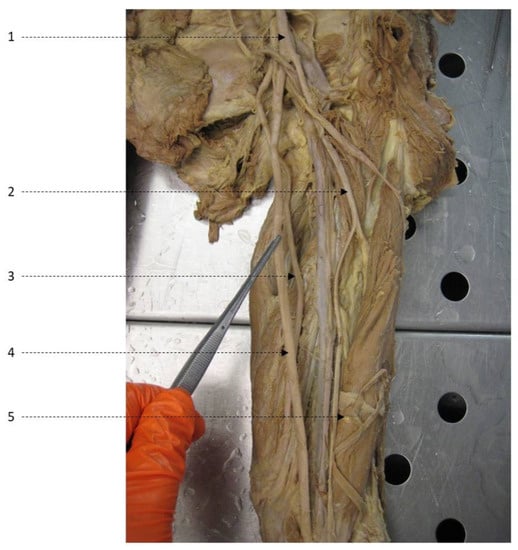
Figure 2.
Typical anatomical relationship between the musculocutaneous nerve and median nerve. Left upper limb, anterior view. 1, lateral cord; 2, musculocutaneous nerve, 3, ulnar nerve; 4, median nerve; 5, biceps brachii muscle.
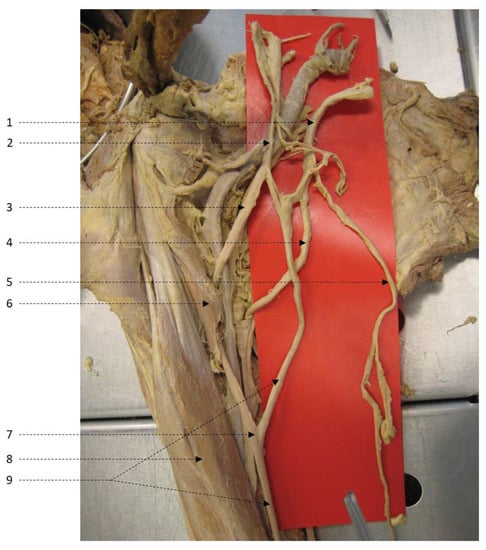
Figure 3.
Anatomical variation of musculocutaneous nerve and median nerve communication. Right upper limb, anterior view. 1, medial cord; 2, lateral cord; 3, musculocutaneous nerve; 4, ulnar nerve; 5, medial antebrachial cutaneous nerve; 6, coracobrachialis muscle; 7, communicating branch (MCN-MN anastomosis); 8, biceps brachii muscle; 9, median nerve.
4. Discussion
Over the years, many efforts have been made to increase the knowledge on anatomical variants, since their importance is recognized in both clinical and surgical fields []. Among the elements of the peripheral nervous system, the brachial plexus seem to be the most variable one []; anatomical variations of the MCN, including its total absence, being among the most significant and present in 10 to 54% of the population according to past studies [,,]. Anatomical studies of embryos suggesting that the MCN is derived from the MN may provide some explanation [,] for this high recurrence. The MCN and the lateral root of MN represent two terminal nerves of the lateral cord of the brachial plexus []. In literature, many papers have described variants in the communication between the MCN and the MN, that are actually the most frequent anatomical variations in the infraclavicular region of the brachial plexus [,]. The first description of communicating branch between the MCN and the MN was reported by Gegenbaur et al. [], and after this study many other classifications based on such anatomical variations have been drafted. The most specific and most commonly used classifications today are those proposed by Le Minor [] and Venieratos and Anangnostopolou [].
According to the Le Minor classification, the large number of variations of the musculocutaneous nerve are classified into five different types in relation to the course of the nerve:
- (i)
- type I: classic description without anastomoses between the MCN and the MN, with the former passing through the coracobrachialis muscle;
- (ii)
- type II: fibers link both nerves in the distal section of the arm;
- (iii)
- type III: lateral root of the MN is merged with the MCN;
- (iv)
- type IV: all fibers of the MCN are merged with the lateral root of the MN, they follow the MN for some distance and then separate from it as a lateral branch;
- (v)
- type V: the MCN is absent and branches are located in the upper arm [].
According to the Venieratos and Anangnostopolou classification, variations are classified into three different types in relation to the sites of communication:
- (i)
- type I: communications are proximal to the entry point of the MCN into the coracobrachialis muscle;
- (ii)
- type II: communications are distal to the muscle;
- (iii)
- type III: the MCN doesn’t pierce the coracobrachialis muscle [].
In the presented study, anatomical dissections were conducted on more than twenty upper limbs, and in 95% of them, type I of MCN-MN variation according to the Le Minor classification was observed. The previously undescribed anatomical variant of MCN-MN anastomosis was found exclusively in one of the studied cadavers, unilaterally. This anatomical variant identified by us does not directly fit within the above-reported classifications. The only variation that shows some similarities is type II of MCN-MN communication according to the Le Minor classification. However, in our case there was no separate branch connecting the MCN and the MN, and the anastomosis was located not at the distal portion, but at the midpoint of the arm. The anastomosis found was in the form of a side-to-side adjacent 1.7 cm section between the two nerves (with visible sharing of fibers between them). In accordance with our findings, Nascimento et al. also reported an anatomical anastomosis between the MCN and the MN localized in a comparable position []. In our case, it should also be noted that the anatomical variant was present only on one arm of the donor. This seems to be quite common: Venieratos and Anangnostopolou [] reported bilateral presence of variations only in 37.5% of cases with detected MCN-MN communication variants. However, further studies and dissections are needed to verify the recurrence of this rare anastomosis between the MCN and the MN.
5. Conclusions
In conclusion, we consider the variation we found as rare, since it is not directly included in any classifications present in literature. In our opinion, this anatomical variation of the anastomosis between the median and the musculocutaneous nerve might assume significant relevance during surgical and clinical practices. A very unusual morphology—a communicating segment between the nerves—may suggest that the structures can be separated during surgery, which could be potentially detrimental to the patient. We hope that our case report will increase the awareness of clinicians and contribute to the improvement of patient safety.
Author Contributions
Dissections—writing—original draft preparation, R.B., A.G.D., N.D.L., G.L.D.G., E.M., G.S., L.L.B., A.M.G., W.P., F.R., E.S. and J.H.S.; supervision, S.W., F.B. and F.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the Medical University of Gdańsk (Ordinance No. 26/2016 of 6 June 2016).
Informed Consent Statement
Premortem informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bergman, R.A.; Tubbs, R.S.; Shoja, M.M.; Loukas, M. Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; pp. 1069–1089. [Google Scholar]
- Standring, S. Pectoral girdle, shoulder region and axilla. In Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 39th ed.; Elsevier Churchill Livingstone: London, UK, 2005; pp. 817–849. [Google Scholar]
- Le Minor, J.M. A rare variant of the median and musculocutaneous nerves in man. Arch. Anat. Histol. Embryol. 1990, 73, 33–42. [Google Scholar] [PubMed]
- Guerri-Guttenberg, R.A.; Ingolotti, M. Classifying musculocutaneous nerve variations. Clin. Anat. 2009, 22, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Venieratos, D.; Anagnostopoulou, S. Classification of communications between the musculocutaneous and median nerves. Clin. Anat. 1998, 11, 327–331. [Google Scholar] [CrossRef]
- Iwanaga, J.; Singh, V.; Ohtsuka, A.; Hwang, Y.; Kim, H.J.; Moryś, J.; Ravi, K.S.; Ribatti, D.; Trainor, P.A.; Sañudo, J.R.; et al. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin. Anat. 2021, 34, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Haviarova, Z.; El Falougy, H.; Killingerova, A.; Matejcik, V. Variation of the median nerve course and its clinical importance. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2009, 153, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Pedrini, F.A.; Mariani, G.A.; Orsini, E.; Quaranta, M.; Ratti, S.; Cocco, L.; Manzoli, L.; Billi, A.M. Unilateral absence of Casserio’s nerve and a communicating branch to the median nerve. An additional variant of brachial flexors motor innervation. Ital. J. Anat. Embryol. 2016, 124, 16–25. [Google Scholar]
- Chitra, R. Various types of intercommunications between musculocutaneous and median nerves: An analytical study. Ann. Indian Acad. Neurolog. 2007, 10, 100–104. [Google Scholar] [CrossRef]
- Radunovic, M.; Vukasanovic-Bozaric, A.; Radojevic, N.; Vukadinovic, T. A new anatomical variation of the musculocutaneous and the median nerve anastomosis. Folia Morphol. 2013, 72, 176–179. [Google Scholar] [CrossRef] [PubMed][Green Version]
- El Falougy, H.; Selmeciova, P.; Kubikova, E.; Stenova, J.; Haviarova, Z. The variable communicating branches between musculocutaneous and median nerves: A morphological study with clinical implications. Bratisl Lek List. 2013, 114, 290–294. [Google Scholar] [CrossRef]
- Gegenbaur, C. Uber das Verhaltniss des N. musculocutaneous zum N. medianus. Jena. Zeitschr F Med. U Nat. 1867, 3, 258–263. [Google Scholar]
- Nascimento, S.R.; Ruiz, C.R.; Pereira, E.; Andrades, L.; de Souza, C.C. Rare anatomical variation of the musculocutaneous nerve-case report. Rev. Bras. Ortop. 2016, 51, 366–369. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).