Abstract
Previous research found an inverse U-shaped association between age and different measures of wisdom, with the apex in late midlife. What might explain the negative relation between age and wisdom during the later years of life? This research investigated the impact of subjective physical health and mastery, using data from the Successful AGing Evaluation (SAGE) study of 976 adults between the ages of 51 and 99 years (M = 77.23, SD = 12.18). Physical health tends to decline with advancing years and, therefore, might reduce older adults’ sense of mastery and control over their lives, which might adversely affect their wisdom. Results showed that age correlated negatively with subjective health, wisdom, and mastery. In multivariate regression and path analyses, the negative relations of age and ill health on wisdom became non-significant after mastery was entered into the model. If wisdom declines in old age due to ill health that results in a perceived loss of mastery, enabling older adults to maintain their sense of control might preserve wisdom.
1. Introduction
Does wisdom grow or decline with age? Sternberg [1] presented five generalized views regarding the relationship between age and wisdom. First, according to the received view, if wisdom comes with experience, the old adage “with age comes wisdom” should be true. Yet, life experience might not be enough for wisdom to emerge. Rather, learning from experience might be required for wisdom development [2]. Second, the fluid intelligence view posits that, similar to fluid intelligence, which is the “ability to think flexibly in novel ways” (p. 13) [1] and comprehend and effectively manipulate new information [3], wisdom increases until early adulthood as individuals gain experiences and learn to navigate the world but then levels off and starts to decline in middle age together with a decline in fluid intelligence. Third, based on the crystallized intelligence view, wisdom is closer to crystallized than fluid intelligence. Both crystallized intelligence and wisdom increase continuously up to old age, because individuals continue to learn about the crystallized stock of knowledge that a culture has accumulated and are able to utilize their acquired knowledge, experience, and skills effectively until the beginning of physical and cognitive decline for many people in their 80s [4]. Fourth, the fluid and crystallized intelligence view declares that wisdom development is a combination of fluid and crystallized intelligence and, therefore, increases until late middle age and then declines. Fifth, the declining wisdom view claims that wisdom declines with age, starting in early life. This view is based on Meacham’s [5] definition of wisdom as a balance between knowing and doubting. Young adults have wisdom, because their knowledge about the world is balanced by doubts (uncertainty) about the future. Yet, when they grow older, they either become successful, which might give them the illusion that they know more than they do, leading to self-centered certainty and over-confidence, or they encounter hardships and failures, which might make them doubt their abilities and life choices, resulting in a loss of meaning and confidence in the world. Both scenarios destroy the balance between knowing and doubting.
Given these different views, what is the empirical evidence about the relationship between age and wisdom? Unfortunately, no longitudinal data exists that could answer this question. Based on available cross-sectional data from Western parts of the world, the answer depends on the definition and operationalization of wisdom [6,7,8,9]. Wisdom, defined as self-transcendence and assessed by the Adult Self-Transcendence Inventory (ASTI), was unrelated to age in age-diverse samples ranging from 18 to 95 years [10,11]. The San Diego Wisdom Scale (SD-WISE), consisting of social advising, emotional regulation, pro-social behaviors, insight, tolerance, and decisiveness, correlated negatively with age in a sample of adults ranging from 25 to 104 years, with a mean age of 58 years [12]. By contrast, age correlated positively with the Jeste–Thomas Wisdom Index, which added spirituality to the SD-WISE, in a slightly younger sample of respondents that ranged in age from 20 to 82 years, with a mean age of 46 years [13]. None of these studies tested whether the association between age and wisdom was curvilinear. Wise reasoning was found to be positively correlated with age in samples of adults ranging from 25 to 93 years [14], unrelated to age when comparing performances of younger (age 20–40 years) and older (age 60–80 years) participants [15], and curvilinearly related to age, with both younger and older adults scoring on average higher than middle-aged adults on the Situated Wise Reasoning Scale (SWIS), the scale version of wise reasoning [16].
However, wisdom assessed by the Berlin Wisdom Paradigm (BWP) [17] as expert knowledge in life planning, life management, and life review showed an inverse U-shaped association with age, with a sharp increase during adolescence until early adulthood, then a slight increase followed by a slight decrease after midlife, and a more pronounced decline after age 70 [18,19,20]. A similar pattern was observed for the Self-Assessed Wisdom Scale (SAWS) [21,22], which measures wisdom as a combination of critical life experiences, reflectiveness/reminiscence, openness to experiences, emotional regulation, and humor [23], and also the Three-Dimensional Wisdom Scale (3D-WS) [24], which consists of an integration of the cognitive, reflective, and compassionate dimensions of wisdom [25,26,27]. Hence, these three wisdom measures followed the fluid and crystallized intelligence view of age and wisdom.
The cognitive dimension of the Three-Dimensional Wisdom Model (3D-WM) [24,28] represents the ability and willingness to perceive reality as it is and a desire to know the truth, which entail a deep understanding of the interpersonal and intrapersonal aspects of life, including the positive and negative aspects of human nature, the inherent limits of knowledge, and life’s unpredictability and uncertainties. To arrive at such a comprehensive understanding of life requires the reflective wisdom dimension, defined as the ability and willingness to perceive phenomena and events, including oneself, from multiple perspectives through perspective-taking and self-examination to overcome subjectivity and projections. The resulting self-awareness and self-insight about one’s own faults and weaknesses likely lead to a reduction in self-centeredness and greater tolerance and empathy toward others, culminating in sympathetic and compassionate love for all beings, which describes the compassionate dimension of wisdom. The definition and operationalization of the 3D-WM are summarized in Table 1.

Table 1.
Definition and operationalization of the Three-Dimensional Wisdom Model (3D-WM).
A large internet study revealed that the decline with age tended to be steepest for the cognitive dimension of wisdom, following more the fluid intelligence view [26]. After an initial increase until midlife, the reflective wisdom dimension was relatively stable and even showed a slight increase after the age of 71. By contrast, the compassionate wisdom dimension followed a U-shaped pattern with the nadir at midlife. It appears that the cognitive aspects of wisdom are most affected by age-related decline, whereas other wisdom components might grow with age. Yet, if an integration of cognitive, reflective, and compassionate qualities is considered necessary for wisdom [28], the general trend between age and wisdom is negative for the second half of life.
The purpose of the present study was to explore what might explain this negative association between age and three-dimensional wisdom in later life. One reason for the inverse relation between older age and wisdom might be a decline in physical health. Although wisdom is positively related to health [30], because wise people tend to live healthy lives and avoid unhealthy behaviors [31], health still declines with advancing age, even among wise older adults, due to deteriorating biological processes [32,33]. A short-term longitudinal study indicated that the association between subjective physical health and wisdom was reciprocal. After controlling for baseline scores, wisdom was positively related to health 10 months later, but health was also positively related to wisdom 10 months later [34]. This suggests that ill health might negatively affect wisdom.
A decline in physical health might reduce older adults’ sense of mastery and control over their lives [35,36,37]. Ill health and feelings of diminished control, in turn, might prompt older adults to focus on themselves first rather than on others or the larger world by trying to improve their health and regain control. Therefore, ill health might diminish older adults’ wisdom through a loss of mastery and control that reduces their desire to comprehend the deeper truth about life (cognitive wisdom dimension), look at things from different perspectives (reflective wisdom dimension), and care about others (compassionate wisdom dimension). Specifically, the following hypotheses were tested:
Hypothesis 1:
Age is negatively correlated with physical health, mastery, and three-dimensional wisdom among older adults.
Hypothesis 2:
Ill health is negatively correlated with mastery and three-dimensional wisdom.
As mastery and wisdom tend to be significantly correlated [12,38,39], the question arises whether wisdom predicts mastery or mastery predicts wisdom. Among relatively healthy older adults, wisdom predicted mastery about 10 months later after controlling for baseline scores, but not vice versa [34]. Generally, wise people know how to cope with the vicissitudes of life because they have a deep understanding of life and are able to perceive phenomena and events from different perspectives, which gives them a sense of mastery over their fate [35,40,41,42], even though they are aware that they cannot control everything [9]. However, if older adults’ feeling of being in control is threatened by ill health, their diminished sense of mastery might negatively affect their wisdom rather than diminished wisdom reducing their sense of mastery.
Hypothesis 3:
Mastery accounts for the negative relations of age and ill health on wisdom.
Hypothesis 4:
Wisdom does not account for the negative relations of age and ill health on mastery.
Although the focus of this study was not to explain the negative association between age and mastery, Hypothesis 4 was included to determine the empirical order of the variable relations. In the final step, a path model was created to analyze whether and how the association between age and wisdom was mediated by ill health and mastery.
2. Methods
2.1. Procedure
The research is based on secondary data analysis of the Successful AGing Evaluation (SAGE) study, which received ethics approval from the University of California, San Diego, Human Research Protections Program [43,44]. Around 2012, SAGE employed a structured multicohort design to randomly select 1300 community residents of San Diego County, California, aged 50–100 years. SAGE is particularly suited to examine the association between age and wisdom in later life due to its over-sampling of older adults in their 80s and 90s. Non-English speakers, adults who needed daily skilled nursing care, and those with a self-reported diagnosis of dementia or terminal illness were excluded. Selected individuals completed an initial 25-min telephone interview to determine their eligibility and willingness to participate. Those who provided informed consent for study participation received a mail-in survey questionnaire, which took about 90 min to complete. As compensation, respondents were paid $10 for the phone interview and $20 for completing and returning the questionnaire. Of the selected 1300 adults, 1006 returned the questionnaire, which represents a 77% response rate. Compared to these 1006 study participants, the 294 adults who did not send back the questionnaire were on average two years younger and less likely to be white (72.8% versus 81.0%).
2.2. Sample
The data for the present study included 976 respondents between the ages of 51 and 99 years (M = 77 years, SD = 12.2, median age = 81 years) with valid values on all study variables. The age range spans three birth cohorts, with 32.8% of the respondents belonging to the Greatest Generation (born 1901–1927), 43.6% to the Silent Generation (born 1928–1945), and 23.6% to the Baby Boom Generation (born 1946–1964) [45]. Among the participants, 48.9% were women, 51.4% were married or lived in a marriage-like relationship, 31.7% were widowed, 13.2% were divorced or separated, and 3.7% were never married/other. Regarding race and ethnicity, 81.0% were White, 11.2% were Hispanic, 5.3% were Asian, 1.2% were African American, and 1.2% were of another race/ethnicity. With regard to education, 18.0% had not attended college, 37.6% had vocational training, attended some college, or had an associate degree, 24.9% had an undergraduate degree or professional degree, and 19.5% had a Master’s or Doctoral degree.
2.3. Measures
Wisdom was measured by the cognitive, reflective, and compassionate dimensions of the Three-Dimensional Wisdom Scale (3D-WS) [24]. The cognitive wisdom dimension consisted of the average of 14 items (Cronbach’s α = 0.81) that assess knowledge of the positive and negative aspects of human nature and the ambiguity and uncertainty in life (e.g., People are either good or bad—reversed), the willingness to understand phenomena thoroughly (e.g., Ignorance is bliss—reversed), and the ability to make important decisions despite life’s unpredictability and uncertainties (I am hesitant about making important decisions after thinking about them—reversed). The reflective wisdom dimension was the average of 12 items (Cronbach’s α = 0.76) that measure the willingness to look at phenomena and events from different perspectives (e.g., I always try to look at all sides of a problem) and the absence of bitterness, subjectivity, and projections (e.g., When I look back on what has happened to me, I can’t help feeling resentful—reversed). The compassionate wisdom dimension was the average of 13 items (Cronbach’s α = 0.71) that gauge the presence of positive, caring, and nurturing emotions and behavior (e.g., Sometimes I feel a real compassion for everyone) and the absence of indifferent or negative emotions and behavior toward others (e.g., It’s not really my problem if others are in trouble and need help—reversed). All items were assessed on 5-point scales (1 = strongly disagree or not true of myself and 5 = strongly agree or definitely true of myself) and scored in the direction of greater wisdom. The average of the three dimensions (rather than the 39 items) was computed to measure three-dimensional wisdom (Cronbach’s α = 0.68; α = 0.86 for the 39 items). Three-dimensional wisdom in this sample ranged from 2.18 to 5. It should be noted that 12 participants did not provide an answer to the items of the cognitive wisdom dimension. Hence, for these 12 participants, wisdom consisted of the average of the reflective and compassionate wisdom dimensions.
Age was assessed in years.
Subjective ill health was the average of five items from the general health subscale of the SF-36 [46], assessed on 5-point scales and scored in the direction of ill health (Cronbach’s α = 0.75). One item inquired about respondents’ general health (1 = excellent and 5 = poor), whereas the remaining items asked how true or false (1 = definitely true and 5 = definitely false) four health-related statements were (e.g., I am as healthy as anybody I know; My health is excellent). Ill health ranged from 1 to 5.
Mastery was assessed by Pearlin and Schooler’s [47] 7-item Mastery Scale, which is the most commonly used scale to measure mastery. After all 4-point scale items (1 = strongly disagree and 4 = strongly agree) were scored in the direction of greater mastery (e.g., I can do just about anything I really set my mind to; I have little control over the things that happen to me—reversed), the mean of the items was computed, ranging from 1.57 to 4. Cronbach’s α was 0.78.
Control variables were highest educational level (2 = grade school (1–4 years of schooling) and 12 = doctoral degree), gender (0 = male and 1 = female), and race (0 = non-white and 1 = white).
3. Results
3.1. Bivariate Analyses
Table 2 shows the bivariate correlations between all study variables. As predicted by Hypothesis 1, age was negatively correlated with subjective health, mastery, and wisdom. Yet among the three wisdom dimensions, only the cognitive wisdom dimension was significantly negatively correlated with age. Ill health, by contrast, was negatively correlated with mastery, wisdom, and all three wisdom dimensions, corroborating Hypothesis 2. As expected, mastery was positively correlated with wisdom and its three dimensions.
Table 2.
Bivariate correlations; Pearson’s r.
Among the control variables, age was negatively correlated with education, and education was positively correlated with health, mastery, and wisdom, but not with the compassionate wisdom dimension. On average, older men had a higher education than older women. Compared to older men, older women tended to score lower on mastery but higher on wisdom and the compassionate wisdom dimension. White older adults were slightly older, on average, than non-White older adults and also tended to score higher on wisdom than non-Whites, but not on mastery and the compassionate wisdom dimension.
Because the sample comprised three birth cohorts, One-way Analyses of Variance (ANOVA) were conducted to analyze differences in ill health, mastery, wisdom, and education by birth cohort. As shown in Table 3, compared to younger cohorts, older cohorts had higher average scores on ill health but lower average scores on mastery, wisdom, and education. The differences in mean scores were statistically significant between the Baby Boom Generation and the Greatest Generation for all four variables, and the differences between the Baby Boom Generation and the Silent Generation were statistically significant for three of the variables, except for ill health. Yet, the average scores for the Silent Generation and the Greatest Generation only differed statistically for mastery. Hence, the Silent Generation and Greatest Generation appear to be more similar than the Baby Boom Generation.
Table 3.
One-way ANOVA of ill health, mastery, wisdom, and education by birth cohorts.
3.2. Multivariate Regression Analysis
Multivariate regression analysis was conducted in SPSS Version 30.0 (IBM Corp., Armonk, NY, USA) to test Hypotheses 3 and 4. As shown in Model 1 in Table 4 for wisdom as the dependent variable, the negative association between age and wisdom remained statistically significant after controlling for ill health, education, gender, and race. However, after adding mastery in Model 2, the negative associations of age and ill health on wisdom became non-significant.
Table 4.
Predictors of wisdom and mastery; multivariate regression analyses.
By contrast, after including ill health and the control variables for mastery as the dependent variable in Model 1 in Table 4, adding wisdom in Model 2 only reduced the negative relations of age and ill health on mastery, but they remained statistically significant. Hence, Hypothesis 3, that mastery accounts for the negative associations of age and ill health on wisdom, and Hypothesis 4, that wisdom does not account for the negative relations of age and ill health on mastery, were supported.
Among the control variables in Model 2, education was positively related to wisdom (but not mastery), women tended to score higher on wisdom and lower on mastery than men, and White older adults scored on average slightly higher on wisdom than non-White older adults (but not on mastery).
3.3. Path Analysis
In the final step, a path analysis in LISREL 9.30 (Scientific Software International, Inc., Skokie, IL, United States) was conducted based on the results of the multivariate regression analyses in Table 4. Because PRELIS 9.30 (Scientific Software International, Inc. (Skokie, IL, USA) indicated that the variables did not follow a multivariate normal distribution, covariance and asymptotic covariance matrices were computed and analyzed with a weighted least squares (WLS) estimation procedure in LISREL 9.30 to obtain corrected chi-square statistics and corrected standard errors and t-values of the direct, indirect, and total effects [48]. The WLS estimator is asymptotically sufficient even under the condition of nonnormality [49].
Figure 1 shows how ill health and mastery mediated the negative association between age and wisdom. Age was positively related to ill health, both age and ill health were negatively related to mastery, and mastery was positively associated with wisdom. Hence, older age was significantly indirectly negatively related to wisdom mediated by a lower sense of mastery and poorer physical health, which was also negatively related to mastery. Ill health, in turn, was significantly indirectly negatively associated with wisdom through a lower sense of mastery.
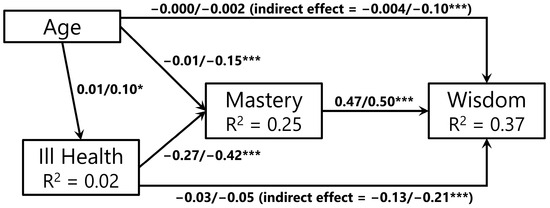
Figure 1.
Mediated path model. Note: n = 976; *** t-value > 3.90 (p < 0.0001), * t-value > 2.58 (p < 0.01). WLS estimation using LISREL 9.30; weighted least squares χ2 = 1.88 (df = 3, p = 0.60); RFI = 0.98, GFI = 1.00, IFI = 1.00, RMSEA = 0.00; unstandardized/standardized coefficient estimates controlling for significant effects of education, gender, and race; standard errors, t-values, and χ2 statistics corrected for non-normality. RFI = relative fit index, GFI = goodness of fit index, IFI = incremental fit index, RMSEA= root mean square error of approximation.
Among the control variables, education was negatively related to ill health (unstandardized/standardized effect = −0.03/−0.10, p < 0.01) and positively to mastery (unstandardized/standardized effect = 0.02/0.10, p < 0.001) and wisdom (unstandardized/standardized effect = 0.04/0.21, p < 0.0001). Older women tended to score lower on mastery (unstandardized/standardized effect = −0.06/−0.07, p < 0.05) and higher on wisdom (unstandardized/standardized effect = 0.17/0.19, p < 0.0001) than older men, and White older adults tended to score higher on wisdom than non-White older adults (unstandardized/standardized effect = 0.11/0.10, p < 0.001).
The variables in the path model accounted for 2% of the variation in ill health, 25% of the variation in mastery, and 37% of the variation in wisdom. The model fit the data well with a non-significant weighted least squares chi-square value of 1.88 (3 df, p = 0.60), a relative fit index (RFI) of 0.98 that was close to 1, a goodness of fit index (GFI) of 1, an incremental fit index (IFI) of 1, and a root mean square error of approximation (RMSEA) of 0, indicating close approximate fit [49,50,51].
4. Discussion
The purpose of this study was to investigate what might explain the negative association between age and wisdom after age 50. As in research that utilized the BWP [18,20] and the SAWS [23] to assess wisdom and previous research with the 3D-WS [25,26,27,35], the current study confirmed that age was negatively correlated with wisdom during the later years of life, which was primarily due to the cognitive wisdom dimension. With advanced age, the desire to think in depth about things appears to decrease [52] together with a decline in fluid intelligence [4] and in openness to experiences [23,53], whereas rigidity or dogmatism seems to increase [5,54]. Age was also negatively correlated with physical health and mastery, and ill health, in turn, was negatively associated with mastery and wisdom, supporting Hypotheses 1 and 2 and prior research [35,36,37,55,56].
When physical health starts to decline with advanced age, it is perhaps not surprising that older adults’ sense of mastery also tends to decrease. Unless someone dies before physical deterioration takes place, the longer people live, the higher the likelihood that they will be affected by age-related diseases and disabilities. Most older adults probably realize that they have only limited control over the biological processes that accompany aging [32,33] and that health-related behavior, medical interventions, and medications might give them extra years of life, but will not reverse the aging process. A diminished sense of control due to physical decline might then spill over into other areas of life. If older adults start to believe that they have little control over their lives, they might not be interested in pursuing a deeper kind of knowledge (cognitive wisdom dimension) but just allow things to happen without thinking too deeply about it. Rather than looking at phenomena from different perspectives to understand and improve their situation (reflective wisdom dimension), they might blame other people or external circumstances for their lack of control. And instead of caring for the well-being of others (compassionate wisdom dimension), they might feel that they need to take care of their own well-being first. Indeed, mastery fully mediated the negative relations of age and ill health on wisdom as predicted by Hypothesis 3. By contrast, the negative relations of age and ill health on mastery remained statistically significant after wisdom was added to the model. This confirmed the possible empirical order of the variable relations in the path model and corroborated Hypothesis 4. The findings suggest that enabling older adults to maintain their sense of control might offset a decline in wisdom in the later years of life due to ill health that might result in a perceived loss of mastery.
The major limitation of the study is the cross-sectional nature of the data. Cross-sectional studies cannot ascertain changes with advancing age, only differences between individuals of different ages. The negative relations of age on wisdom, mastery, and health might not be due to biological aging but to cohort effects [6,8,26,57]. The oldest respondents belonged to the Greatest Generation, who not only experienced the Great Depression [58] but also World War II (WWII), with many of the men serving in the war [59]. The subsequent Silent Generation was alive during WW II but too young to serve in the war. The Baby Boom Generation was born after WWII and grew up during a period of relative stability and economic growth [60]. Hence, compared to the Baby Boom Generation, the older generations might have felt a lower sense of mastery over their lives and less interest in the attainment of wisdom due to the earlier experienced economic and political upheaval that prioritized survival rather than self-development [61]. By contrast, the higher educated Baby Boom Generation might have been more motivated to develop wisdom, feel in control of their lives, and take care of their health than the older cohorts because of societal changes after WWII that emphasized self-improvement [62].
Furthermore, the associations between ill health, mastery, and wisdom are probably reciprocal. Wise older people and those who feel a sense of mastery over the circumstances in their life are likely to engage in health-promoting behavior, such as exercising, eating well, and avoiding alcohol, drug, and tobacco use [31,63,64], which might delay but not eliminate the onset of age-related physical decline that leads to a reduced sense of mastery. Moreover, wise older adults know how to deal with the vicissitudes of life by understanding life and its unpredictability thoroughly, perceiving phenomena from multiple perspectives, and engaging in problem-focused active coping, which likely gives them a sense of control over their lives [35,40,41]. They also might select alternative means or goals to compensate for age-related losses and achieve the desired outcome [65], for example, by replacing jogging with walking, or utilize secondary (subjective) control strategies to adjust mentally to physical restrictions [66,67], for example, by gratefully accepting and enjoying the help and companionship of others rather than feeling resentful about their loss of independence [9]. These strategies likely preserve some sense of mastery. Yet, longitudinal studies are required to analyze how wisdom, mastery, and health change during the second half of life and how these variables are related to each other as people grow older.
As in all survey research, it is also possible that the true cause of the negative association between age and wisdom in the later years of life is an omitted variable that is significantly related to both age and wisdom. Yet, possible confounders that tend to be associated with wisdom, such as resilience, optimism, subjective well-being, and perceived stress [40,68], were unrelated to age in the present study.
Another limitation is the generalizability of the findings. Although the structured multicohort design was chosen to obtain a representative random sample of older community residents of San Diego County in California with an oversample of residents above the age of 80 years, San Diego County is not representative of the United States and other parts of the world. Hence, future research will need to test how generalizable the findings are across the globe.
Finally, it is possible that wise behavior might increase with age, even if scores on wisdom measures decline due to a decrease in socially desirable responding [18]. Qualitative research is necessary to compare how older adults who were identified by wisdom measures as relatively wise and not-so-wise behave in everyday life and how they cope with stressful situations.
5. Conclusions
It appears that the negative association between age and wisdom during the later years of life might be due to a loss of perceived control over one’s life, particularly after health deteriorates. If this is the case, restoring a sense of mastery in older adults who suffer from ill health might preclude the loss of wisdom. Self-driving cars and artificially intelligent devices might give older adults the freedom and support to remain in control of their lives by providing mobility [69] and assisting with activities of daily living [70]. Yet, wise aging might also necessitate a shift from self-centered goals to self-transcendent goals that do not require optimal physical health to pursue these goals [9], such as volunteering for a good cause, which likely bolsters feelings of mastery [71]. A sustained sense of mastery, in turn, might preserve the cognitive, reflective, and compassionate qualities of wisdom and contribute to aging well [34,35,38,40].
Funding
No funding was provided for the analysis of the data and writing of the article.
Institutional Review Board Statement
The Successful AGing Evaluation (SAGE) study was conducted in accordance with the Declaration of Helsinki and approved by the University of California, San Diego, Human Research Protections Program. This secondary analysis of the de-identified data did not include any identifiable private information.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the author on request.
Acknowledgments
I am grateful to Dilip V. Jeste for giving me access to the data. A previous version of the paper (with Dilip V. Jeste) was presented at the Gerontological Society of America Annual Meetings in Tampa, FL, in November 2023.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Sternberg, R.J. Older but not wiser? The relationship between age and wisdom. Ageing Int. 2005, 30, 5–26. [Google Scholar] [CrossRef]
- Staudinger, U.M.; Glück, J. Psychological wisdom research: Commonalities and differences in a growing field. Annu. Rev. Psychol. 2011, 62, 215–241. [Google Scholar] [CrossRef]
- Li, S.-C.; Lindenberger, U.; Hommel, B.; Aschersleben, G.; Prinz, W.; Baltes, P.B. Transformations in the couplings among intellectual abilities and constituent cognitive processes across the life span. Psychol. Sci. 2004, 15, 155–163. [Google Scholar] [CrossRef]
- Kaufman, A.S. WAIS-III IQs, Horn’s theory, and generational changes from young adulthood to old age. Intelligence 2001, 29, 131–167. [Google Scholar] [CrossRef]
- Meacham, J.A. The loss of wisdom. In Wisdom: Its Nature, Origins, and Development; Sternberg, R.J., Ed.; Cambridge University Press: New York, NY, USA, 1990; pp. 181–211. [Google Scholar]
- Glück, J. The development of wisdom during adulthood. In The Cambridge Handbook of Wisdom; Glück, J., Sternberg, R.J., Eds.; Cambridge University Press: Cambridge, UK, 2019; pp. 323–346. [Google Scholar]
- Grossmann, I.; Weststrate, N.M.; Ardelt, M.; Brienza, J.P.; Dong, M.; Ferrari, M.; Fournier, M.A.; Hu, C.S.; Nusbaum, H.C.; Vervaeke, J. The science of wisdom in a polarized world: Knowns and unknowns. Psychol. Inq. 2020, 31, 103–133. [Google Scholar] [CrossRef]
- Glück, J. Wisdom and aging. Curr. Opin. Psychol. 2024, 55, 101742. [Google Scholar] [CrossRef]
- Glück, J.; Jäger, L.; Auer-Spath, I.; Harbig, I.A. Finding the balance to quiet the striving: The difference between successful aging and wise aging. Gerontologist 2025, 65, gnae126. [Google Scholar] [CrossRef] [PubMed]
- Levenson, M.R.; Jennings, P.A.; Aldwin, C.M.; Shiraishi, R.W. Self-transcendence: Conceptualization and measurement. Int. J. Aging Hum. Dev. 2005, 60, 127–143. [Google Scholar] [CrossRef]
- Glück, J.; König, S.; Naschenweng, K.; Redzanowski, U.; Dorner-Hörig, L.; Strasser, I.; Wiedermann, W. How to measure wisdom: Content, reliability, and validity of five measures. Front. Psychol. 2013, 4, 1–13. [Google Scholar] [CrossRef]
- Thomas, M.L.; Bangen, K.J.; Palmer, B.W.; Sirkin, A.v.; Avanzino, J.A.; Depp, C.A.; Glorioso, D.; Daly, R.E.; Jeste, D.V. A new scale for assessing wisdom based on common domains and a neurobiological model: The San Diego Wisdom Scale (SD-WISE). J. Psychiatr. Res. 2019, 108, 40–47. [Google Scholar] [CrossRef]
- Jeste, D.V.; Thomas, M.L.; Liu, J.; Daly, R.E.; Tu, X.M.; Treichler, E.B.H.; Palmer, B.W.; Lee, E.E. Is spirituality a component of wisdom? Study of 1786 adults using expanded San Diego Wisdom Scale (Jeste-Thomas Wisdom Index). J. Psychiatr. Res. 2021, 132, 174–181. [Google Scholar] [CrossRef]
- Grossmann, I.; Na, J.; Varnuma, M.E.W.; Park, D.C.; Kitayama, S.; Nisbett, R.E. Reasoning about social conflicts improves into old age. Proc. Natl. Acad. Sci. USA 2010, 107, 7246–7250. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, I.; Kross, E. Exploring Solomon’s paradox: Self-distancing eliminates the self-other asymmetry in wise reasoning about close relationships in younger and older adults. Psychol. Sci. 2014, 25, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Brienza, J.P.; Kung, F.Y.H.; Santos, H.C.; Bobocel, D.R.; Grossmann, I. Wisdom, bias, and balance: Toward a process-sensitive measurement of wisdom-related cognition. J. Personal. Soc. Psychol. 2018, 115, 1093–1126. [Google Scholar] [CrossRef] [PubMed]
- Baltes, P.B.; Staudinger, U.M. Wisdom: A metaheuristic (pragmatic) to orchestrate mind and virtue toward excellence. Am. Psychol. 2000, 55, 122–136. [Google Scholar] [CrossRef]
- Glück, J. The development of wisdom. In The Psychology of Wisdom: An Introduction; Sternberg, R.J., Glück, J., Eds.; Cambridge University Press: Cambridge, UK, 2022; pp. 175–192. [Google Scholar]
- Pasupathi, M.; Staudinger, U.M.; Baltes, P.B. Seeds of wisdom: Adolescents’ knowledge and judgment about difficult life problems. Dev. Psychol. 2001, 37, 351–361. [Google Scholar] [CrossRef]
- Staudinger, U.M. Older and wiser? Integrating results on the relationship between age and wisdom-related performance. Int. J. Behav. Dev. 1999, 23, 641–664. [Google Scholar] [CrossRef]
- Webster, J.D. An exploratory analysis of a self-assessed wisdom scale. J. Adult Dev. 2003, 10, 13–22. [Google Scholar] [CrossRef]
- Webster, J.D. Measuring the character strength of wisdom. Int. J. Aging Hum. Dev. 2007, 65, 163–183. [Google Scholar] [CrossRef]
- Webster, J.D.; Westerhof, G.J.; Bohlmeijer, E.T. Wisdom and mental health across the lifespan. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 209–218. [Google Scholar] [CrossRef]
- Ardelt, M. Empirical assessment of a three-dimensional wisdom scale. Res. Aging 2003, 25, 275–324. [Google Scholar] [CrossRef]
- Thomas, M.L.; Bangen, K.J.; Ardelt, M.; Jeste, D.V. Development of a 12-item abbreviated Three-Dimensional Wisdom Scale (3D-WS-12): Item selection and psychometric properties. Assessment 2017, 24, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Ardelt, M.; Pridgen, S.; Nutter-Pridgen, K.L. The relation between age and three-dimensional wisdom: Variations by wisdom dimensions and education. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2018, 73, 1339–1349. [Google Scholar] [CrossRef] [PubMed]
- Bergsma, A.; Ardelt, M. Self-reported wisdom and happiness: An empirical investigation. J. Happiness Stud. 2012, 13, 481–499. [Google Scholar] [CrossRef]
- Ardelt, M. Wisdom as expert knowledge system: A critical review of a contemporary operationalization of an ancient concept. Hum. Dev. 2004, 47, 257–285. [Google Scholar] [CrossRef]
- Clayton, V.P.; Birren, J.E. The development of wisdom across the life-span: A reexamination of an ancient topic. In Life-Span Development and Behavior; Baltes, P.B., Brim, O.G., Jr., Eds.; Academic Press: New York, NY, USA, 1980; Volume 3, pp. 103–135. [Google Scholar]
- Zadworna, M. Effects of wisdom on mental health in old age: Exploring the pathways through developmental tasks attainment and self-rated health. Psychol. Res. Behav. Manag. 2023, 16, 4541–4554. [Google Scholar] [CrossRef]
- Zadworna, M.; Stetkiewicz-Lewandowicz, A. The relationships between wisdom, positive orientation and health-related behavior in older adults. Sci. Rep. 2023, 13, 16724. [Google Scholar] [CrossRef]
- Khan, S.S.; Singer, B.D.; Vaughan, D.E. Molecular and physiological manifestations and measurement of aging in humans. Aging Cell 2017, 16, 624–633. [Google Scholar] [CrossRef]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. Hallmarks of aging: An expanding universe. Cell 2023, 186, 243–278. [Google Scholar] [CrossRef]
- Ardelt, M. Disentangling the relations between wisdom and different types of well-being in old age: Findings from a short-term longitudinal study. J. Happiness Stud. 2016, 17, 1963–1984. [Google Scholar] [CrossRef]
- Ardelt, M.; Edwards, C.A. Wisdom at the end of life: An analysis of mediating and moderating relations between wisdom and subjective well-being. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 502–513. [Google Scholar] [CrossRef]
- Gadalla, T.M. Sense of mastery, social support, and health in elderly Canadians. J. Aging Health 2009, 21, 581–595. [Google Scholar] [CrossRef]
- Pearlin, L.I.; Nguyen, K.B.; Schieman, S.; Milkie, M.A. The life-course origins of mastery among older people. J. Health Soc. Behav. 2007, 48, 164–179. [Google Scholar] [CrossRef]
- Ardelt, M. Wisdom and well-being. In The Cambridge Handbook of Wisdom; Sternberg, R.J., Glück, J., Eds.; Cambridge University Press: Cambridge, UK, 2019; pp. 602–625. [Google Scholar]
- Puchalska-Wasyl, M.M. Do wisdom and well-being always go hand in hand? The role of dialogues with oneself. J. Happiness Stud. 2023, 24, 1059–1074. [Google Scholar] [CrossRef]
- Ardelt, M.; Jeste, D.V. Wisdom as a resiliency factor for subjective well-being in later life. Psychosoz. Und Med. Rehabil. Pract. Clin. Behav. Med. Rehabil. 2022, 118, 13–28. [Google Scholar]
- Etezadi, S.; Pushkar, D. Why are wise people happier? An explanatory model of wisdom and emotional well-being in older adults. J. Happiness Stud. 2013, 14, 929–950. [Google Scholar] [CrossRef]
- Weststrate, N.M.; Glück, J. Hard-earned wisdom: Exploratory processing of difficult life experience is positively associated with wisdom. Dev. Psychol. 2017, 53, 800–814. [Google Scholar] [CrossRef] [PubMed]
- Jeste, D.V.; Savla, G.N.; Thompson, W.K.; Vahia, I.V.; Glorioso, D.K.; Martin, A.v.S.; Palmer, B.W.; Rock, D.; Golshan, S.; Kraemer, H.C.; et al. Association between older age and more successful aging: Critical role of resilience and depression. Am. J. Psychiatry 2013, 170, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.L.; Kaufmann, C.N.; Palmer, B.W.; Depp, C.A.; Martin, A.S.; Glorioso, D.K.; Thompson, W.K.; Jeste, D.V. Paradoxical trend for improvement in mental health with aging: A community-based study of 1,546 adults aged 21–100 years. J. Clin. Psychiatry 2016, 77, e1019–e1025. [Google Scholar] [CrossRef]
- Pew Research Center. The Whys and Hows of Generations Research; Pew Research Center: Washington, DC, USA, 2015; pp. 1–16. [Google Scholar]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Pearlin, L.I.; Schooler, C. The structure of coping. J. Health Soc. Behav. 1978, 19, 2–21. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D.; du Toit, S.; du Toit, M. LISREL 8: New Statistical Features; Scientific Software International: Chicago, IL, USA, 1999. [Google Scholar]
- Bollen, K.A. Structural Equations with Latent Variables; Wiley: New York, NY, USA, 1989. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Bruinsma, J.; Crutzen, R. A longitudinal study on the stability of the need for cognition. Personal. Individ. Differ. 2018, 127, 151–161. [Google Scholar] [CrossRef]
- Costa, P.T., Jr.; McCrae, R.R.; Löckenhoff, C.E. Personality across the life span. Annu. Rev. Psychol. 2019, 70, 423–448. [Google Scholar] [CrossRef]
- Schultz, P.W.; Searleman, A. Rigidity of thought and behavior: 100 years of research. Genet. Soc. Gen. Psychol. Monogr. 2002, 128, 165–207. [Google Scholar]
- Nicolaisen, M.; Moum, T.; Thorsen, K. Mastery and depressive symptoms: How does mastery influence the impact of stressors from midlife to old age? J. Aging Health 2018, 30, 1084–1107. [Google Scholar] [CrossRef]
- Pudrovska, T.; Schieman, S.; Pearlin, L.I.; Nguyen, K. The sense of mastery as a mediator and moderator in the association between economic hardship and health in late life. J. Aging Health 2005, 17, 634–660. [Google Scholar] [CrossRef]
- Alwin, D.F.; McCammon, R.J. Generations, cohorts, and social change. In Handbook of the Life Course; Mortimer, J.T., Shanahan, M.J., Eds.; Springer: New York, NY, USA, 2003; pp. 23–49. [Google Scholar]
- Amadeo, K. Great Depression Timeline: 1929–1941; The Balance: New York, NY, USA, 2019. [Google Scholar]
- Brokaw, T. The Greatest Generation, Random House trade pbk. ed.; Random House: New York, NY, USA, 2005; p. 38. 412p. [Google Scholar]
- Collins, R.M. More: The Politics of Economic Growth in Postwar America; Oxford University Press: Oxford, UK; New York, NY, USA, 2000; p. 11. 299p. [Google Scholar]
- Koltko-Rivera, M.E. Rediscovering the later version of Maslow’s hierarchy of needs: Self-transcendence and opportunities for theory, research, and unification. Rev. Gen. Psychol. 2006, 10, 302–317. [Google Scholar] [CrossRef]
- Seligman, M.E.P. What You Can Change and What You Can’t: The Complete Guide to Successful Self-Improvement, 1st ed.; Knopf: New York, NY, USA, 1994; p. 10. 317p. [Google Scholar]
- Seeman, M.; Seeman, T.E. Health behavior and personal autonomy: A longitudinal study of the sense of control in illness. J. Health Soc. Behav. 1983, 24, 144–160. [Google Scholar] [CrossRef]
- Assari, S.; Najand, B.; Donovan, A. Sense of mastery explains social patterning of health. Healthcare 2025, 13, 1511. [Google Scholar] [CrossRef] [PubMed]
- Baltes, P.B.; Freund, A.M. The intermarriage of wisdom and selective optimization with compensation: Two meta-heuristics guiding the conduct of life. In Flourishing: Positive Psychology and the Life Well-Lived; Keyes, C.L.M., Haidt, J., Eds.; American Psychological Association: Washington, DC, USA, 2003; pp. 249–273. [Google Scholar]
- Heckhausen, J. Developmental regulation across adulthood: Primary and secondary control of age-related challenges. Dev. Psychol. 1997, 33, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Heckhausen, J.; Wrosch, C.; Schulz, R. Agency and motivation in adulthood and old age. Annu. Rev. Psychol. 2019, 70, 191–217. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.D.; Weststrate, N.M.; Ferrari, M.; Munroe, M.; Pierce, T.W. Wisdom and meaning in emerging adulthood. Emerg. Adulthood 2018, 6, 118–136. [Google Scholar] [CrossRef]
- Shu, S.; Woo, B.K.P. Applications of self-driving vehicles in an aging population. JMIR Form. Res. 2025, 9, e66180. [Google Scholar] [CrossRef]
- Gabriella, C.; Riccardo De, B.; Francesca, F.; Andrea, O.; Alessandro, U.; Amedeo, C. AI and robotics to help older adults: Revisiting projects in search of lessons learned. Paladyn J. Behav. Robot. 2021, 12, 356–378. [Google Scholar] [CrossRef]
- Ang, S.; Malhotra, R. How helping you helps me: A longitudinal analysis of volunteering and pathways to quality of life among older adults in Singapore. J. Gerontol. Ser. B 2024, 79, gbae013. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.