Abstract
Microplastics and nanoplastics (MNPs) are pervasive contaminants infiltrating water, food, and human tissues. The sharp rise in plastic production—with over half manufactured between 2003 and 2022—has heightened concerns about their health impacts. Methods included: (1) a literature review of clinical studies on MNPs focusing on human health and (2) analysis of Standardized Mortality Rates (SMRs) for 44 groups of diseases in Italy (2003–2022, Italian National Institute of Statistics, ISTAT data). The outcomes suggest that MNPs have been connected to pathological alterations in a number of organ systems, such as the gastrointestinal tract (intestine, liver, and pancreas), breathing system, eyes, brain, and vascular structures. SMRs increased significantly in only eight of the 46 illness categories examined between 2003 and 2022. The analysis of clinical and epidemiological data allows us to identify a possible clinical assessment consisting of a 30-variable diagnostic questionnaire (Chicago Cluster Evaluation System, CCES), encompassing laboratory markers, clinical signs, and ultrasound findings. A binomial distribution model suggests that more than 8 positive responses may indicate a presumptive diagnosis of Microplastic Syndrome (MP-Sy). This framework reflects observed clinical/epidemiological patterns and provides a foundation for hypothesis-driven research. Prospective longitudinal studies are warranted to validate the proposed definition and its diagnostic utility. The aim of the present study is to propose a preliminary clinical framework for a potential MP-Sy integrating toxicological evidence with epidemiological data, define diagnostic criteria and assess their consistency with observed disease trends.
1. Introduction
Since the 1950s, billions of tonnes of plastics have accumulated globally, contaminating landfills and ecosystems and affecting both humans and wildlife [1]. Originating mainly from fossil fuels such as coal, oil, and gas, plastics have profoundly shaped industrial and technological progress. However, inadequate waste management and the expanding plastics industry have driven pollution to critical levels, with plastic waste projected to exceed 40 million Mt annually by 2030 [2]. Global production has risen exponentially—from under 2 million tonnes in 1950 to about 800 million today—creating widespread contamination by microplastics (MPs, 1 µm–5 mm) and nanoplastics (NPs, 1 nm–<1 µm), collectively referred to as micro- and nanoplastics (MNPs) [3].
The human body is exposed to these newly created contaminants through the skin, ingestion, and inhalation [4,5]. They have been identified in many human tissues, where they can cause lesions and dysfunctions that can have a substantial clinical impact [6,7]. Despite advances in the toxicodynamics of MNPs, the pathophysiology is still mostly unknown. Several studies published in the literature, suggests that MNPs cause cytokine release, oxidative stress, inflammatory cascades, and overall cytotoxicity [8,9,10].
The main pathways via which MNPs enter the human body are the gastrointestinal, respiratory, and cutaneous. Exposure to the environment differs by location and by indoor and outdoor environments; larger concentrations are usually found outside [11]. Conventional monitoring of air quality focuses on PM2.5 to PM10, yet many MNPs are larger than 10 µm and go unnoticed. Larger particles may stick to the upper respiratory tract or be passed to the throat and consumed, but they hardly ever make it to the alveoli [12].
MNPs have been found in meats, fish, vegetables, cereals, fruits, honey, salts, dairy products, and drinking water. The gastrointestinal route has been the most thoroughly studied [13,14,15,16]. Daily consumption ranges from nanograms to milligrams [17], and interplay with mucus, microbiota, dysbiosis [18], biofilm formation [19], and gut–brain axis regulation [20,21] is facilitated by digestion fragmentation. Comparatively less is known about dermal exposure through packaging and cosmetics [22,23]. To comprehend systemic impacts, MNP absorption, distribution, metabolism, and excretion (ADME) must be clarified (Figure 1).
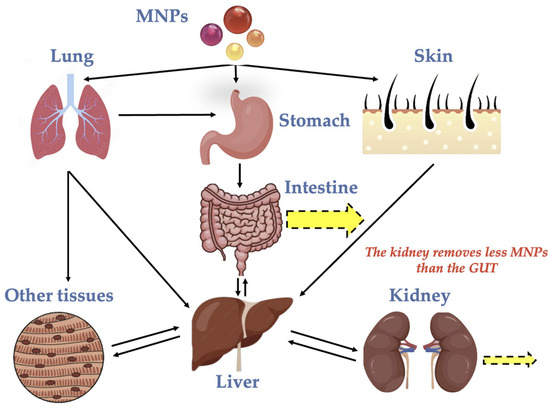
Figure 1.
The development of MNPs in the human body (ADME).
The gastrointestinal, respiratory, and cutaneous systems are the primary entry points for MNPs into the body. There are regional and indoor/outdoor variations in atmospheric pollution, with indoor levels being higher [20]. Although PM2.5–PM10 are currently measured by air monitoring, many MNPs are larger than 10 µm and are hence undetectable. Even though they are not absorbed by the alveoli, larger airborne particles have the ability to stick to the upper airways or pass via the pharynx before entering the digestive tract [21]. The most extensively researched pathway is still the gastrointestinal system. Depending on ambient and dietary circumstances, reported daily intake rates range greatly, from milligrams to nanograms [17]. Enzymatic and mechanical mechanisms further break up the particles during digestion, which facilitates their interaction with intestinal mucus and the microbiota. These interactions have the potential to disrupt the gut–brain axis [20,21], promote biofilm development [19], and trigger dysbiosis [18]. The third and least investigated route is dermal exposure, particularly through MNP-containing cosmetics and packaging materials [22,23]. Clarifying these particles’ biological behavior and related hazards requires an understanding of their pharmacokinetics (PK), or ADME (Figure 1).
The majority of the information comes from isolated biological samples, while human research is still lacking and mostly descriptive. MNPs exhibit remarkable diversity in terms of size, content, and morphology (fragments, films, and fibers); human tissues have been found to contain at least 18 different polymeric monomers [24]. While the structures of polyethylene terephthalate (PET) are more complex than those of polypropylene (PP) or polyvinyl chloride (PVC), they all have characteristics such as limited reactivity, incomplete enzymatic breakdown, and chemical stability. Size-dependent absorption has been shown in animal models, with <0.36% for 6 µm particles and <1.7% for 0.05 µm ones [24].
Humans have been found to include MNPs in their blood [25], urine [26,27], milk [28,29], gastrointestinal tissue [30], stools [31], placenta [32], cardiac muscle [33], testis and semen [34], sputum [35], and even thrombi [36]. Larger polymers (>100 µm) are frequently trapped in mucus, while smaller particles (<10 µm) can pass through biological membranes, simulating gaseous diffusion and perhaps causing long-term subclinical damage. MNPs exposure may persist for years without causing any symptoms and can resemble long-term conditions including neurological, metabolic, or cardiovascular problems. This emphasizes the necessity of a single diagnostic system for Microplastics Syndrome (MP-Sy). The Chicago Cluster Evaluation System (CCES), a diagnostic and assessment model created to categorize and measure microplastics-related pathology across acute and chronic conditions, is thus introduced in the current study. It integrates toxicological, epidemiological, and clinical indicators to direct research, diagnostics, and the identification of possible therapeutic targets.
In conclusion, the present study aims to (i) characterize the clinical manifestations and diagnostic indicators of Microplastics Syndrome (MP-Sy), (ii) evaluate how well it aligns with current disease patterns, and (iii) validate the proposed CCES as an all-inclusive instrument for assessing disorders linked to MNPs.
2. Materials and Methods
2.1. Methodological Approach/Literature Search
A dual approach was adopted: (1) comprehensive examination of clinical evidence on the toxicity and bioaccumulation of MNPs in the literature; (2) an analysis of the Italian National Institute of Statistics’ (ISTAT) Standardized Mortality Rates (SMRs) for 44 diseases from 2003 to 2022. All authors reviewed and discussed the full contents of suitable publications. Additionally, to find other pertinent studies, the reference lists of the publications that were obtained were examined.
Research was conducted from 1 June 2025 to 30 September 2025, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement 2020 Checklist. To conduct the search, four different databases were consulted: PubMed, ISI Web of Science, Google Scholar, and Scopus. While many of the same articles were found in all databases, Google Scholar offered a wider selection of articles specifically on in vivo studies and was therefore used in both the initial and follow-up searches. The Google Scholar search used the terms “microplastics and nanoplastics”, “clinical trials”, “in vivo studies”, “human health”, “cytotoxicity”, “nanotoxicity/neurotoxicity”, “oxidative stress”, “biocorona”, “cell uptake”, “carcinogenesis”, “neurodegeneration”, and “inflammation”. The publication date was limited to the period between 1 January 2000, and 30 September 2025, yielding 992 results. For this study, only peer-reviewed English-language articles were taken into consideration. Figure 2 shows that 140 of the 992 documents that were retrieved were relevant to the clinical harm that MNPs produced between 2000 and 2025 (Table S1). At this stage, pertinent articles that focused on the following initially were taken into consideration: concentrations in different physiological fluids, organs, and tissues; oxidative stress, inflammation, and cellular damage; common threats to human health from MPs/NPs; biocorona formation; the toxicity of MPs/NPs to human health and carcinogenesis; more data on analytical techniques and source reduction strategies; and more information on the abundance of MPs/NPs (bioaccumulation) in the human body. For PRISMA Flow Diagram, see Figure S5 in Supplementary Materials.
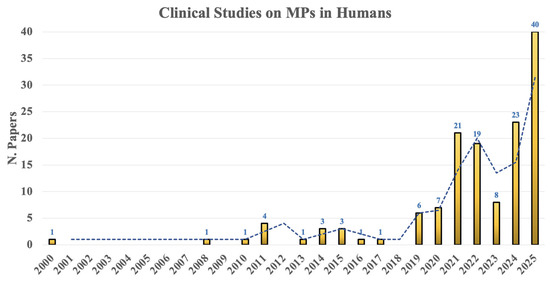
Figure 2.
N. articles reporting clinical effect of MNPs in humans (2000–2025).
The main components of the Preferred Reporting components for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement, modified for a non-systematic (narrative) synthesis, were followed in the carrying out and reporting of this narrative review. To improve reproducibility and reporting quality, the methodology—including database search, eligibility requirements, and selection procedure—was openly described in accordance with PRISMA’s guidelines. Despite the absence of exhaustive risk-of-bias assessment and quantitative synthesis, the review satisfies PRISMA guidelines’ reporting standards for narrative reviews.
Review publications, in vitro clinical studies, and animal clinical trials were excluded. Italy was used as an example for the retrospective examination. ISTAT official statistics [37] assessed the SMRs from 2003 to 2022 owing to 44 diseases in the 20 Regions (Figures S1–S3, Tables S2 and S5)
2.2. Statistics
The Tukey test was used to examine the difference between 2003 and 2022 after taking into account the SMRs of the 20 Italian regions.
A Binomial Model and Bayes Theorem were employed in accordance with this equation (Equation (1)) for the threshold determination of the number of symptoms necessary to attain a posterior diagnostic probability ≥95% [P(D/K ≥ k)], where k = 0…n for MNP-related disease.
where π: 0.05; S1 (k) and S0 (k′): cumulative tail probabilities of K in diseased and healthy individuals, respectively. The SAS Institute’s JMP Pro 14 (2019) software was used for the analysis.
3. Results
3.1. Clinical Findings
According to the analysis of the 20 main articles, there were indications of multiple illness associated with liver damage [32,38], atherosclerosis [34], vessels [35], thrombi [36], lung [39,40], brain [41,42,43], intestinal diseases [44,45], gallstones in young people [46], rhinosinusitis [47], other ocular diseases [48], and skin [22]. MNPs levels in blood [25,28], urine [26,27], and breastfeeding [29] were reported in five distinct articles.
MNPs were found to be at least largely responsible for the following diseases: gallstones, retinopathy, atherosclerosis, venous insufficiency, irritable bowel syndrome, and rhinosinusitis. The overall amount of SMRs decreased dramatically between 2003 and 2022. Nevertheless, 8 disease classes showed a considerable increase out of the 44 total (Table S2). Table 1 lists the data. With the exception of genito-urinary disorders, the increases were statistically significant.

Table 1.
SMRs of the type of diseases that increases in the 20 Italian Regions (2003–2022).
Finally, only five disease types were added: pancreatic and central nervous system (CNS) tumors, neurodegenerative diseases, psychiatric/behavioral disorders, and endocrine system diseases (apart from diabetes).
3.2. Map of the Organ/System Affected by MNPs
Considering the fate of MNPs and the diseases that have been identified, a rough map may be created that shows the organs and systems on one side and the symptoms and laboratory values on the other (Table 2).
Table 2.
Organ symptoms and laboratory abnormality due to MNPs damage.
Inflammatory indicators and ultrasound imaging are essential components of medical diagnosis. The thorax, brain, vascular system, pelvis, and abdomen are among the areas where ultrasound can identify important pathological and anatomical changes that have clinical significance.
According to the SMR differences between 2003 and 2022 and the literature documenting clinical damages caused by MNPs, 29 variables (lab, semeiotic, ultrasound) can be altered by the presence of MNPs in the body in Italy. Figure 3 summarizes data (CCES: Cardiovascular, Hematological, Intestinal (duodenum, pancreas, colon and dysbiosis), Cerebral, Andrological, Gynecological, Oncological, Connective tissue, Liver, Urinary, Sensorial system (ear, eye, nose, mouth, balance disorders), Thyroid, Endocrine system, Respiratory system. CCES is an acronym for a systematic framework that includes important clinical domains for classifying diseases. According to the references for each letter of the acronym, the variables shown in Table 1 and Figure 3 were obtained from a thorough analysis of the literature. Table S1 and Figure S4 in the Supplementary Materials provide details on the corresponding references. These variables are representative of common diagnostic tests and systems/organs that doctors use to identify and characterize illness phenotypes.
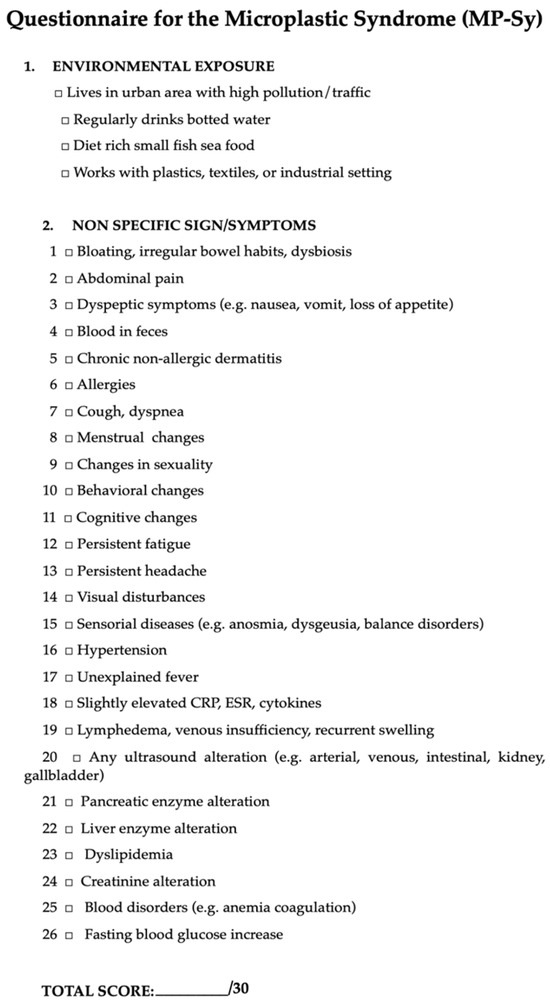
Figure 3.
Questionnaire for MP-Sy.
3.3. MNPs Syndrome (MP-Sy)
Approximately 89% of the participants had MNPs in their blood, according to some authors [28], indicating that these pollutants are essentially a part of the human body whether or not they are causing illnesses. Depending on their concentrations and the kind of polymer, one could think that they could become poisonous.
Since MNPs levels were shown to be highest in the brain, it stands to reason that symptoms of these pollutants would either precede or accompany other organs (Table 2).
It may be able to recognize an MP-Sy in a complex protean landscape by combining the signs and symptoms. Figure 3 shows a questionnaire with 30 questions (CCES) that may be used to tentatively identify MP-Sy based on the information presented in Table 1 and Table 2.
The following factors were considered for consideration for the questionnaire’s binomial distribution: n = 30 total symptoms, p1 = 0.65 (probability of a symptom occurring in affected individuals), p0 = 0.10 (probability in healthy individuals) and π = 0.05 (prevalence of the disease).
Figure 4 shows the results of the posterior probability P(D/K ≥ k) for k = 0…n, which was computed using Equation (1).
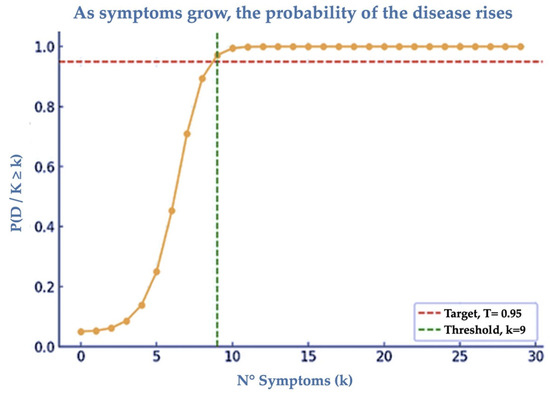
Figure 4.
P(D/K ≥ k) as a Diagnostic Probability as a function of the minimum symptoms. where: Number of symptoms (k) from 0 to 30. Probability . Curve (orange): from ~0.05 for k = 0 up to ≈1 for k > 12. Horizontal green line: target T = 0.95. Vertical red line: minimum threshold k = 9 which is equal to 0.97.
Interpretation of the score: from 0 to 4 points no risk of MS; from 5 to 8 points: moderate risk of MS; >8 points high risk of MS. Thus, for a posterior probability of ≥0.95 to indicate that a person has MS, at least 9 symptoms are required to be evident. Major depressive disorders, Parkinson’s disease, Alzheimer’s disease, and COPD are just a few of the chronic illnesses that exhibit at least six CCES signs and symptoms. These variables may surpass the 8 criterion and need to be added to environmental variables (Tables S3 and S5). This also holds true for a number of acute illnesses (such as diverticulosis, deep vein thrombosis, and gastroenteritis) (Tables S4 and S5).
4. Discussion
MNPs have been detected globally in water, air, and soil, indicating widespread environmental contamination across multiple ecosystems. In 2003, a study published in the Annals of Global Health [18] summarized “the increased risk of leukemia, lymphoma, hepatic angiocarcinoma, brain cancer, breast cancer, mesothelioma, neurotoxic damage, and lower fertility for those who produce plastic. An increasing number of workers who produce plastic fabrics pass away from interstitial lung disease, bladder cancer, lung cancer, and mesothelioma. Workers who recycle plastic are more likely to suffer from lung cancer, neuropathy, toxic metal toxicity, and cardiovascular disease. Living close to plastic manufacturing facilities or landfills puts nearby residents at higher risk for lung cancer, low birth weight, asthma, pediatric leukemia, cardiovascular illness, and chronic obstructive pulmonary disease”.
Due to extensive biological and environmental infiltration, MNPs have been found in soil, water, air, and human tissues all over the world [30]. Physicochemical properties, particularly surface charge and the development of a biocorona made up of proteins, lipids, nucleic acids, and metabolites, determine particle absorption once it enters the body [34,35]. Bioactivity, immunological recognition, and circulation time are all regulated by this corona. Positively charged particles, even in non-phagocytic cells, have a higher affinity for membranes, which increases intracellular uptake [1]. After intake, absorbed particles are carried to the liver and other organs via portal and lymphatic circulation, while MNPs travel to the gut, where a fraction is eliminated [30]. The greatest amounts of accumulation are seen in the brain and liver, then the kidneys. Milk (12 µm) [29], kidney (29 µm), urine (15 µm), and cirrhotic liver (30 µm) [33] are among the human organs that contain MNPs up to 30 µm. Interestingly, there were no detectable MNPs in healthy livers or kidneys [38], indicating a pathogenic correlation. Toxic metals, phthalates, and bisphenols are examples of endocrine-disrupting chemicals (EDCs) that are present in or adsorbable by MNPs. These chemicals can covalently bind to polymers and increase toxicity. These interactions add to vascular damage, oxidative stress, cytokine release, and hormonal instability, underscoring the complex ways in which MNPs cause systemic damage.
According to recent post-mortem studies, MNPs were found in high amounts in the liver and brain but not in the kidneys, indicating persisting neurohepatic retention despite prolonged renal elimination [49]. Its dependence on the glymphatic system and poor lymphatic clearance seem to make the brain especially vulnerable [50]. The most often found polymer was polyethylene (PE) [51]. Cognitive decline on the Mini-Mental State Examination (MMSE) was correlated with significantly lower levels of amyloid-β peptide (Aβ42) in cerebrospinal fluid (CSF) in Alzheimer’s patients (<600 pg/mL) than in healthy individuals, which highlights the neurotoxic implications [42]. The idea that MNPs might disrupt amyloid metabolism and exacerbate neurodegenerative processes is supported by this new finding.
The prevalence of MNPs in human biology is becoming more and more evident from clinical research. In certain cohorts, measurable MNPs were found in the circulation of about 89% of participants, indicating that these pollutants are now inherent to the human body regardless of clinical presentation [28]. The kind and concentration of polymers, however, determine their potential for toxicity. Since the brain has the greatest levels of MNP, neurological symptoms including mood swings, exhaustion, or cognitive deterioration could occur before or alongside systemic manifestations in other organs (Table 2). The identification of a unique, multisystemic entity—the MP-Sy—is supported by the convergence of symptoms and indicators from the neurological, cardiovascular, metabolic, and endocrine domains.
A standardized diagnostic and assessment framework that integrates toxicological, epidemiological, and clinical criteria, the CCES was proposed in the current study in response to the complex clinical presentation of MP-Sy. The pathology linked to MNPs can be categorized and measured by academics and physicians using this system for both acute and chronic disease spectrums. CCES has demonstrated remarkable efficacy in verifying MNP-associated pathology and assessing its diagnostic sensitivity and repeatability, according to the data presented. Its multifaceted structure makes it possible to identify discrete clinical clusters, which aids in distinguishing coincidental comorbidities from MNP-induced syndromic patterns.
As a useful diagnostic framework for recognizing and describing the complex clinical patterns that may be connected to MP-Sy, the current findings support the CCES. It is an exceptional methodological advancement to combine epidemiological, clinical, and toxicological information into a single analytical matrix. The CCES offers a quantitative, repeatable framework that may connect the load of MNPs to particular clinical characteristics, in contrast to earlier descriptive studies. It has been confirmed that plastic particles are now a quasi-physiological element of the human body, with MNPs identified in the bloodstream of about 89% of the participants in the analysis [28]. This extensive internalization highlights the necessity of a diagnostic approach that is multisystemic. With thirty laboratory, semeiotic, and imaging variables spanning the cardiovascular, hepatic, neurological, endocrine, and immunological domains, the CCES’s multifaceted architecture is its strongest point. The identification of small, overlapping syndromic manifestations that would otherwise go unnoticed in clinical settings is made possible by this integrative power.
4.1. Clinical and Epidemiological Outcomes
Significant correlations with the possible impacts of MNPs were found in an investigation of SMRs from 2003 to 2022. The most important discoveries included pancreatic cancers, central nervous system (CNS) tumors, and brain disorders, none of which were reported in the clinical studies examined, with the exception of Alzheimer’s disease [42,49].
In contrast, metabolic diseases, pancreatic tumors, and CNS cancers continue to be the three conditions most consistently associated with MNPs exposure. The COVID-19 outbreak between 2019 and 2022 was found to increase SMRs of neurological, hematopoietic, genitourinary, and undefined diseases [52], which suggests a negative interaction between viral infection and MNPs toxicity. Only mental disorders and Parkinson’s disease remained significantly elevated when comparing data from 2003 and 2019.
4.2. Pathophysiological Processes
MNPs have been related to a variety of brain damage, including tumors, degenerative diseases, and behavioral and mental issues [53]. The brain has a disproportionately high concentration of MNPs, an order of magnitude more than that found in the liver and kidneys, which seems to account for these clinical symptoms.
On the pancreas, tumors appear to be a reflection of localized toxicity brought on by MNPs enterohepatic circulation. This phenomenon produces toxic consequences that are specific to a given place, and the pancreas is especially sensitive because of its close proximity to other organs [54].
Inflammatory cytokines are produced as a result of increased OS within cellular structures, which is the known molecular basis for the inflammatory response to MNPs [9]. Immune surveillance cells like macrophages are drawn to the chemotactic milieu that these cytokines create in the arterial, venous, and lymphatic vasculature damage. This approach promotes advancement by keeping the lesion in “active” condition. The OS/inflammation/lesion cascade is sufficiently deactivated by disruption of this pathway to stop future progression and improve organ and vascular function.
The system’s translational potential is demonstrated by its capacity to reflect the complex nature of MNP toxicity, which includes everything from endothelial damage and oxidative stress to metabolic and neuroinflammatory disorders. Organ-specific clinical correlates of pathophysiological processes (OS, cytokine activation, and endocrine disturbance) are matched by the CCES (Table 2). Based on binomial modeling, its probabilistic design determines an empirically defined threshold of nine positive variables for a diagnostic probability of MP-Sy ≥ 0.95. Between clinical medicine and environmental toxicology, this quantitative criterion offers an operational interface. Neurological signs may precede or accompany other systemic effects, according to the greater MNP concentrations seen in brain tissues. The neurological cluster of CCES may therefore use cognitive impairment, behavioral abnormalities, and exhaustion as early signs. By combining vascular, hepatic, and endocrine clusters into a single model, cross-domain correlation is made possible, providing a comprehensive clinical picture that is in line with a syndrome brought on by systemic xenobiotics.
4.3. Effects on Therapy and Prevention
There are currently no treatment approaches to get rid of MNPs from tissues. Reducing intake and absorption, however, can stop them from building up and essentially “freeze” the tissue damage that has already been caused [55]. Accordingly, it has been proposed that product labels reveal the levels of MNPs found in food.
4.4. Proposal for Diagnostics and Limitations
Significant increases in neurological, pancreatic, and endocrine illnesses were found in the retrospective analysis of Standardized Mortality Rates (SMRs) from 2003 to 2022, which lends credence to the possibility of an MNP-related burden. These epidemiological tendencies were successfully reflected in the CCES framework, which validated its diagnostic reasoning internally. Through the mapping of documented patterns in mortality and morbidity to the respective clusters—particularly vascular, pancreatic, and cerebral—the CCES creates an empirical connection between clinical manifestation and population-level statistical data. Additionally, the CCES facilitates a tiered diagnostic strategy that may be applied to both clinical and research contexts by integrating laboratory biomarkers, self-reported symptoms, and ultrasound imaging. Its promise as a universal screening and monitoring tool for MNP exposure and effect is strengthened by its repeatability across both acute and chronic illnesses (i.e., dementia, Parkinson’s disease, deep vein thrombosis-DVT, and gastroenteritis).
It is important to consider this study as an initial effort to identify a possible MP-Sy. In order to achieve this, consideration was given to the signs, symptoms, and laboratory tests that are most frequently utilized in medical outpatient visits. Our suggested diagnostic method is based on the structure of a typical outpatient assessment, in which lab tests are used to detect and track clinical symptoms.
Nevertheless, are significant drawbacks, including the lack of methods to properly evaluate MNPs’ effects on the human body, the uneven clinical evidence about their effects, and the paucity of a systematic attempt to establish a syndrome—assuming that is even possible.
4.5. Compared to Other Syndromes
The 30 variables identified for MS include some of the characteristics of the metabolic syndrome as defined by ATP III [56], including dyslipidemia, hypertension, and hyperglycemia, but they fall short of the crucial threshold of nine elements. The threshold can be met or exceeded, though, when taking into account ancillary factors that are commonly seen in these patients, such as drinking from plastic containers, eating fish or shellfish, living in situations where microplastics are present, having high inflammatory markers, abnormal arterial ultrasound findings, elevated creatinine levels, and coagulation disorders. This implies that metabolic syndrome could be regarded as a subset of the MP-Sy spectrum in specific individuals. In supplementary Table S3 and Table S4 report, respectively, chronic and acute diseases that may fall within the MP-Sy.
Theoretically, the CCES provides the first systematic effort to identify a syndromic identity for microplastic toxicity, similar to the identification of metabolic or endocrine syndromes in earlier decades. It offers an outline for differentiating between direct impacts of MNP and secondary or co-factor phenomena, including oxidative stress or viral amplifications. In the clinical setting, it enables hypothesis-driven patient categorization, directing imaging, laboratory testing, and potentially treatment strategies. Since MNPs have been observed to generate varied pathology in almost every examined tissue, including the brain, placenta, blood, and gastrointestinal tract, the CCES may be used as a prediction framework for susceptibility assessment. Integrating the model with new biomarkers, including proteomic or metabolomic signs of biocorona development, is also made possible by its modularity.
4.6. Concluding Remarks
This study represents a first step toward the clinical systematization of a potential MP-Sy. Recent study evidence indicates that MNPs are physiologically active substances that can cause tissue injury and pathophysiological disturbance rather than just being passive xenobiotics [57,58,59,60]. MNPs seem to play a role as co-factors, if not initiators, in a variety of disease processes, rather than being inert pollutants. Numerous studies have linked their extensive distribution in human organs—such as the liver, placenta, gastrointestinal tract, cardiovascular system, and lungs—to cellular malfunction, OS, and localized inflammation. It is commonly acknowledged that these reactions are early indicators of cancer and chronic illness, and they are not coincidental [25,56].
MNPs have been shown in vitro to impede cellular repair mechanisms, activate pro-inflammatory signaling pathways (such as NF-κB and NLRP3), change redox balance, and impair mitochondrial function. These kinds of interactions foster an environment that is favorable to the development of both acute and chronic diseases. It is significant to note that MNPs have the potential to both intensify the beginning of subclinical damage that occurs prior to overt clinical signs and worsen pre-existing pathological disorders [1]. Evidence currently available supports MNPs’ involvement as active participants in pathogenesis rather than passive observers, even if injured tissues may show higher retention of MNPs. Significantly, the pro-oxidative and pro-inflammatory environment that MNPs produce closely resembles the molecular environment seen in the early phases of carcinogenesis, highlighting their possible significance for long-term health effects [1,56].
The CCES’s suggested diagnostic probability criteria are amenable to prospective validation in the form of interventional and longitudinal research. Future multicenter studies could include it to help determine whether MP-Sy is a convergent phenotype of chronic pollution exposure or a separate clinical illness. Additionally, it may make therapeutic monitoring and the assessment of detoxifying or barrier-protective therapies easier by quantifying symptom clusters. In summary, an environmental toxicological problem is converted into a clinically quantifiable construct using the CCES. By bridging the fields of epidemiology, molecular pathology, and medical diagnostics, it provides a scalable, testable, and standard model for examining the MP-Sy theory. With its implementation, one of the most widespread emergent health hazards of the twenty-first century may move from anecdotal observation to evidence-based characterization. These findings support the CCES as a valuable exploratory tool to direct future in vivo and epidemiological research on the health impacts of MNPs and highlight the possible relevance of MNPs in disease pathways.
5. Putative Limitations and Methodological Considerations
This study has some limitations. The concept of MP-Sy was introduced to promote in vivo research exploring the link between MNPs and both chronic and acute diseases. MNPs have been found in multiple human organs, complicating the identification of specific pathogenic mechanisms. While experimental studies suggest that MNPs induce oxidative stress and inflammation [56], it remains unclear whether they act as causal agents or disease byproducts. The lack of longitudinal clinical data and the variability in particle size, polymer type, and detection methods limit exposure–response assessments. Although the CCES diagnostic tool may involve some classification variability, it provides a useful framework for exploring potential associations in the absence of standardized biomarkers.
Confounders such as comorbidities, smoking, and changing diagnostic criteria may affect standardized mortality ratio (SMR)-based analyses. Additionally, a ~2.5-year increase in life expectancy from 2003 to 2022 [38] and the impact of the COVID-19 pandemic [57,61,62,63] may influence mortality patterns. Finally, the lack of validated protocols for detecting MNPs in human tissues limits comparability. These findings should therefore be considered hypothesis-generating, requiring confirmation through prospective studies.
6. Future Directions
Many previous international studies have shown that the widespread accumulation of MNPs in the environment has been linked to toxicological effects at many levels of biological organization. New data points to possible effects on human health, which, along with growing public anxiety, has already spurred preliminary legislative actions. Legal harmonization is desperately needed to protect human health. Strategies to reduce MNPs emissions and those to eliminate them should be clearly distinguished in such frameworks. The basis for evidence-based regulation must be the latest scientific developments in the detection of MNPs in the air, water, and soil matrices as well as in the creation of efficient mitigation procedures [64].
Research will be used to both identify the hazards of MNPs exposure and to direct the development of successful therapies. According to previous studies, for example, cationic fibers, like chitosan made from Procambarus clarkii, which has a high binding affinity for MNPs, may improve the intestine removal of MNPs [65,66,67,68,69,70,71,72,73]. The next stage will be to determine whether these methods could also have an impact on the “microplastic-related syndrome” that has been postulated.
This issue is still within the realm of plausible theories at this period. Clinical observations and prospective research that can offer more accurate insights into causality, processes, and possible treatment approaches will be necessary for definitive advancement.
7. Conclusions
MNPs are alarmingly proliferating throughout ecosystems as a result of the exponential increase in plastic manufacture since 2003. These particles have become widespread environmental contaminants, and there is mounting evidence that they can harm tissues including brain, lungs, liver, gastrointestinal tract, kidneys, blood vessels, skin, and eyes. There are significant human health implications. A promising first step is provided by a recently created diagnostic instrument consisting of CCES (30 items). According to preliminary research, receiving more than 8 responses might be a sign of the existence of what is now known as an MP-Sy. These findings highlight the urgent need for worldwide attention to plastic pollution, both as an environmental emergency and as a serious human health concern.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/microplastics4040093/s1. Figure S1: Main SMR values of the different diseases in Italy (2003–2022); Figure S2: Main SMR values for cancer types in Italy (2003–2022); Figure S3: Main SMR values of the other types of disease evaluated in Italy (2003–2022); Figure S4: Chicago Cluster; Figure S5: PRISMA 2020 Flow Diagram; Table S1: Main in vivo studies (2000–2025); Table S2: SMRs for residents in Italy (1 × 104), (Test HSD de Tukey: p < 0.05); Table S3: Chronic diseases with at least 6 Chicago Cluster signs/symptoms; Table S4: Acute diseases with at least 6 Chicago Cluster signs/symptoms; Table S5: Merck Manual Seventeenth Edition (1999) MediCom Milan-Italy [74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99].
Author Contributions
U.C.: Conceptualization, methodology, validation, visualization, formal analysis, investigation, supervision, writing—original draft preparation, writing—review and editing; C.C.: Conceptualization, methodology, validation, visualization, investigation, writing—original draft preparation, writing—review and editing; G.B.: Validation, visualization, writing—review and editing; M.R.C.: Validation, visualization, writing—review and editing; S.M.: Validation, visualization, writing—review and editing; M.R. (Mariangela Rondanelli): Data curation, stastical analysis, visualization, writing—review and editing; M.R. (Martino Recchia): Data curation, software, statistical analysis; G.Z.: Validation, visualization, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
The authors had no financial support.
Data Availability Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request. Umberto Cornelli can provide all data in Excel files upon request.
Acknowledgments
The authors express their gratitude to ISTAT for enabling the analysis of SMRs.
Conflicts of Interest
The authors Giovanni Belcaro and Maria Rosaria Cesarone were employed by IRVINE3 Labs and OOLEX Project. The remaining authors declare that this research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript and Supplementary Materials:
| ADME | Absorption, Distribution, Metabolism, and Excretion |
| AIDS | Acquired Immune Deficiency Syndrome |
| CCES | Chicago Cluster Evaluation System |
| CSF | Cerebrospinal Fluid |
| CNS | Central Nervous System |
| COPD | Chronic Obstructive Pulmonary Diseases |
| CRP | C-Reactive Protein |
| DVT | Deep Vein Thrombosis |
| EDCs | Endocrine-Disrupting Chemicals |
| GI | Gastrointestinal |
| ISTAT | Italian National Institute of Statistics |
| MMSE | Mini-Mental State Examination |
| MNPs | Micro-Nanoplastics |
| MPs | Microplastics |
| MP-Sy | Microplastic Syndrome |
| Mt | Metric Tons |
| NPs | Nanoplastics |
| OS | Oxidative Stress |
| PCOS | Polycystic Ovary Syndrome |
| PET | Polyethylene Terephthalate |
| PK | Pharmacokinetics |
| PP | Polypropylene |
| PS | Polystyrene |
| PVC | Polyvynil Chloride |
| SMRs | Standardized Mortality Rates |
| TBC | Tuberculosis |
| WHO | World Health Organization |
References
- Casella, C.; Ballaz, S.J. Genotoxic and neurotoxic potential of intracellular nanoplastics: A review. J. Appl. Toxicol. 2024, 44, 1657–1678. [Google Scholar] [CrossRef]
- Plastic Europe 2024 Plastics—The Fast Facts 2024 Plastics Europe. 2024. Available online: https://plasticseurope.org/knowledge-hub/plastics-the-fast-facts-2024/ (accessed on 1 August 2025).
- Haque, M.K.; Uddin, M.; Kormoker, T.; Ahmed, T.; Zaman, M.R.U.; Rahman, M.S.; Tsang, Y.F. Occurrences, sources, fate and impacts of plastic on aquatic organisms and human health in global perspectives: What Bangladesh can do in future? Environ. Geochem. Health 2023, 45, 5531–5556. [Google Scholar] [CrossRef]
- Li, P.; Liu, J. Micro (nano) plastics in the human body: Sources, occurrences, fates, and health risks. Environ. Sci. Technol. 2024, 58, 3065–3078. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, G.; Abdulkadhim, M.; Joshi, K.; Wankhede, L.; Das, R.K.; Brar, S.K. Exposure Pathways, Systemic Distribution, and Health Implications of Micro-and Nanoplastics in Humans. Appl. Sci. 2025, 15, 8813. [Google Scholar] [CrossRef]
- Feng, Y.; Tu, C.; Li, R.; Wu, D.; Yang, J.; Xia, Y.; Luo, Y. A systematic review of the impacts of exposure to micro-and nano-plastics on human tissue accumulation and health. Eco-Environ. Health 2023, 2, 195–207. [Google Scholar] [CrossRef]
- Bossio, S.; Ruffolo, S.A.; Lofaro, D.; Perri, A.; La Russa, M.F. Endocrine Toxicity of Micro-and Nanoplastics, and Advances in Detection Techniques for Human Tissues: A Comprehensive Review. Endocrines 2025, 6, 23. [Google Scholar] [CrossRef]
- Laganà, A.; Visalli, G.; Facciolà, A.; Saija, C.; Bertuccio, M.P.; Baluce, B.; Di Pietro, A. Sterile inflammation induced by respirable micro and nano polystyrene particles in the pathogenesis of pulmonary diseases. Toxicol. Res. 2024, 13, tfae138. [Google Scholar] [CrossRef]
- Mahmud, F.; Sarker, D.B.; Jocelyn, J.A.; Sang, Q.X.A. Molecular and cellular effects of microplastics and nanoplastics: Focus on inflammation and senescence. Cells 2024, 13, 1788. [Google Scholar] [CrossRef]
- Panizzolo, M.; Martins, V.H.; Ghelli, F.; Squillacioti, G.; Bellisario, V.; Garzaro, G.; Bergamaschi, E. Biomarkers of oxidative stress, inflammation, and genotoxicity to assess exposure to micro-and nanoplastics. A literature review. Ecotoxicol. Environ. Saf. 2023, 267, 115645. [Google Scholar] [CrossRef]
- Casella, C.; Cornelli, U.; Ballaz, S.; Zanoni, G.; Merlo, G.; Ramos-Guerrero, L. Plastic Smell: A Review of the Hidden Threat of Airborne Micro and Nanoplastics to Human Health and the Environment. Toxics 2025, 13, 387. [Google Scholar] [CrossRef]
- Vasse, G.F.; Melgert, B.N. Microplastic and plastic pollution: Impact on respiratory disease and health. Eur. Respirat. Rev. 2024, 33, 230226. [Google Scholar] [CrossRef] [PubMed]
- Basaran, B.; Özçifçi, Z.; Akcay, H.T.; Aytan, Ü. Microplastics in branded milk: Dietary exposure and risk assessment. J. Food Compos. Anal. 2023, 123, 105611. [Google Scholar] [CrossRef]
- Diaz-Basantes, M.F.; Conesa, J.A.; Fullana, A. Microplastics in honey, beer, milk and refreshments in Ecuador as emerging contaminants. Sustainability 2020, 12, 5514. [Google Scholar] [CrossRef]
- Visentin, E.; Niero, G.; Benetti, F.; Perini, A.; Zanella, M.; Pozza, M.; De Marchi, M. Preliminary characterization of microplastics in beef hamburgers. Meat Sci. 2024, 217, 109626. [Google Scholar] [CrossRef] [PubMed]
- Alberghini, L.; Truant, A.; Santonicola, S.; Colavita, G.; Giaccone, V. Microplastics in fish and fishery products and risks for human health: A review. Int. J. Environ. Res. Public Health 2022, 20, 789. [Google Scholar] [CrossRef]
- Heo, S.J.; Moon, N.; Kim, J.H. A systematic review and quality assessment of estimated daily intake of microplastics through food. Rev. Environ. Health 2025, 40, 371–392. [Google Scholar] [CrossRef]
- Ibrahim, Y.S.; Tuan Anuar, S.; Azmi, A.A.; Wan Mohd Khalik, W.M.A.; Lehata, S.; Hamzah, S.R.; Landrigan, P.J.; Raps, H.; Cropper, M.; Bald, C.; et al. The Minderoo-Monaco commission on plastics and human health. Ann. Glob. Health 2023, 89, 23. [Google Scholar] [CrossRef]
- Tamargo, A.; Molinero, N.; Reinosa, J.J.; Alcolea-Rodriguez, V.; Portela, R.; Bañares, M.A.; Moreno-Arribas, M.V. PET microplastics affect human gut microbiota communities during simulated gastrointestinal digestion, first evidence of plausible polymer biodegradation during human digestion. Sci. Rep. 2022, 12, 528. [Google Scholar] [CrossRef]
- Sofield, C.E.; Anderton, R.S.; Gorecki, A.M. Mind over microplastics: Exploring microplastic-induced gut disruption and gut-brain-axis consequences. Curr. Issues Mol. Biol. 2024, 46, 4186–4202. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhi, F. Lower level of bacteroides in the gut microbiota is associated with inflammatory bowel disease: A meta-analysis. BioMed Res. Int. 2016, 2016, 5828959. [Google Scholar] [CrossRef]
- Aristizabal, M.; Jiménez-Orrego, K.V.; Caicedo-León, M.D.; Páez-Cárdenas, L.S.; Castellanos-García, I.; Villalba-Moreno, D.L.; Gold, M. Microplastics in dermatology: Potential effects on skin homeostasis. J. Cosmet. Dermatol. 2024, 23, 766–772. [Google Scholar] [CrossRef]
- Yee, M.S.L.; Hii, L.W.; Looi, C.K.; Lim, W.M.; Wong, S.F.; Kok, Y.Y.; Leong, C.O. Impact of microplastics and nanoplastics on human health. Nanomaterials 2021, 11, 496. [Google Scholar] [CrossRef]
- Prata, J.C. Microplastics and human health: Integrating pharmacokinetics. Crit. Rev. Environ. Sci. Technol. 2023, 53, 1489–1511. [Google Scholar] [CrossRef]
- Leslie, H.A.; Van Velzen, M.J.; Brandsma, S.H.; Vethaak, A.D.; Garcia-Vallejo, J.J.; Lamoree, M.H. Discovery and quantification of plastic particle pollution in human blood. Environ. Int. 2022, 163, 107199. [Google Scholar] [CrossRef]
- Pironti, C.; Notarstefano, V.; Ricciardi, M.; Motta, O.; Giorgini, E.; Montano, L. First evidence of microplastics in human urine, a preliminary study of intake in the human body. Toxics 2022, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Rotchell, J.M.; Austin, C.; Chapman, E.; Atherall, C.A.; Liddle, C.R.; Dunstan, T.S.; Guinn, B.A. Microplastics in human urine: Characterisation using μFTIR and sampling challenges using healthy donors and endometriosis participants. Ecotoxicol. Environ. Saf. 2024, 274, 116208. [Google Scholar] [CrossRef]
- Lee, D.W.; Jung, J.; Park, S.A.; Lee, Y.; Kim, J.; Han, C.; Hong, Y.C. Microplastic particles in human blood and their association with coagulation markers. Sci. Rep. 2024, 14, 30419. [Google Scholar] [CrossRef]
- Ragusa, A.; Notarstefano, V.; Svelato, A.; Belloni, A.; Gioacchini, G.; Blondeel, C.; Giorgini, E. Raman microspectroscopy detection and characterisation of microplastics in human breastmilk. Polymers 2022, 14, 2700. [Google Scholar] [CrossRef]
- Wibowo, A.T.; Nugrahapraja, H.; Wahyuono, R.A.; Islami, I.; Haekal, M.H.; Fardiansyah, Y.; Luqman, A. Microplastic contamination in the human gastrointestinal tract and daily consumables associated with an Indonesian farming community. Sustainability 2021, 13, 12840. [Google Scholar] [CrossRef]
- Schwabl, P.; Köppel, S.; Königshofer, P.; Bucsics, T.; Trauner, M.; Reiberger, T.; Liebmann, B. Detection of various microplastics in human stool: A prospective case series. Ann. Int. Med. 2019, 171, 453–457. [Google Scholar] [CrossRef]
- Braun, T.; Ehrlich, L.; Henrich, W.; Koeppel, S.; Lomako, I.; Schwabl, P.; Liebmann, B. Detection of microplastic in human placenta and meconium in a clinical setting. Pharmaceutics 2021, 13, 921. [Google Scholar] [CrossRef]
- Yang, Y.; Xie, E.; Du, Z.; Peng, Z.; Han, Z.; Li, L.; Yang, X. Detection of various microplastics in patients undergoing cardiac surgery. Environ. Sci. Technol. 2023, 57, 10911–10918. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Zhu, L.; Weng, J.; Jin, Z.; Cao, Y.; Jiang, H.; Zhang, Z. Detection and characterization of microplastics in the human testis and semen. Sci. Total Environ. 2023, 877, 162713. [Google Scholar] [CrossRef]
- Huang, S.; Huang, X.; Bi, R.; Guo, Q.; Yu, X.; Zeng, Q.; Guo, P. Detection and analysis of microplastics in human sputum. Environ. Sci. Technol. 2022, 56, 2476–2486. [Google Scholar] [CrossRef]
- Wu, D.; Feng, Y.; Wang, R.; Jiang, J.; Guan, Q.; Yang, X.; Luo, Y. Pigment microparticles and microplastics found in human thrombi based on Raman spectral evidence. J. Adv. Res. 2023, 49, 141–150. [Google Scholar] [CrossRef]
- ISTAT. 2023. Available online: https://www.istat.it/wp-content/uploads/2023/05/2022-SDGS-Report_Inglese.pdf (accessed on 1 August 2025).
- Horvatits, T.; Tamminga, M.; Liu, B.; Sebode, M.; Carambia, A.; Fischer, L.; Fischer, E.K. Microplastics detected in cirrhotic liver tissue. EBioMedicine 2022, 82, 104147. [Google Scholar] [CrossRef]
- Cao, J.; Yang, Q.; Jiang, J.; Dalu, T.; Kadushkin, A.; Singh, J.; Li, R. Coronas of micro/nano plastics: A key determinant in their risk assessments. Part. Fibre Toxicol. 2022, 19, 55. [Google Scholar] [CrossRef]
- Dawson, A.L.; Bose, U.; Ni, D.; Nelis, J.L.D. Unravelling protein corona formation on pristine and leached microplastics. Microplast. Nanoplast. 2024, 4, 9. [Google Scholar] [CrossRef]
- Rotchell, J.M.; Jenner, L.C.; Chapman, E.; Bennett, R.T.; Bolanle, I.O.; Loubani, M.; Palmer, T.M. Detection of microplastics in human saphenous vein tissue using μFTIR: A pilot study. PLoS ONE 2023, 18, e0280594. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Wang, F.; Xi, G.; Li, Y.; Wang, F.; Wang, H.; Shi, Y. Association of microplastics in human cerebrospinal fluid with Alzheimer’s disease-related changes. J. Hazard. Mater. 2025, 494, 138748. [Google Scholar] [CrossRef]
- Landrigan, P.; Symeonides, C.; Raps, H.; Dunlop, S. The global plastics treaty: Why is it needed? Lancet 2023, 402, 2274–2276. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, Y.S.; Tuan Anuar, S.; Azmi, A.A.; Wan Mohd Khalik, W.M.A.; Lehata, S.; Hamzah, S.R.; Lee, Y.Y. Detection of microplastics in human colectomy specimens. JGH Open 2021, 5, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Liu, Y.; Zhang, T.; Zhang, F.; Ren, H.; Zhang, Y. Analysis of microplastics in human feces reveals a correlation between fecal microplastics and inflammatory bowel disease status. Environ. Sci. Technol. 2021, 56, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Wu, C.; Liu, Y.; Li, W.; Li, S.; Peng, L.; Huang, H. Microplastics are detected in human gallstones and have the ability to form large cholesterol-microplastic heteroaggregates. J. Hazard. Mater. 2024, 467, 133631. [Google Scholar] [CrossRef]
- Taş, B.M.; Tuna, A.; Başaran Kankılıç, G.; Koçak, F.M.; Şencan, Z.; Cömert, E.; Bayar Muluk, N. Role of microplastics in chronic rhinosinusitis without nasal polyps. Laryngoscope 2024, 134, 1077–1080. [Google Scholar] [CrossRef]
- Zhong, Y.; Yang, Y.; Zhang, L.; Ma, D.; Wen, K.; Cai, J.; Huang, Z. Revealing new insights: Two-center evidence of microplastics in human vitreous humor and their implications for ocular health. Sci. Total Environ. 2024, 921, 171109. [Google Scholar] [CrossRef]
- Nihart, A.J.; Garcia, M.A.; El Hayek, E.; Liu, R.; Olewine, M.; Kingston, J.D.; Campen, M.J. Bioaccumulation of microplastics in decedent human brains. Nat. Med. 2025, 31, 1114–1119. [Google Scholar] [CrossRef]
- Jessen, N.A.; Munk, A.S.F.; Lundgaard, I.; Nedergaard, M. The glymphatic system: A beginner’s guide. Neurochem. Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef]
- Ma, Q.; Lei, J.; Pang, Y.; Shen, Y.; Zhang, T. Neurotoxicity of Micro-and Nanoplastics: A Comprehensive Review of Central Nervous System Impacts. Environ. Health 2025. [Google Scholar] [CrossRef]
- Cornelli, U.; Algeri, F.; Brignoli, A. The increase of chronic diseases death during COVID-19 outbreak in Italy: The effect of vaccinations. Eur. J. Appl. Sci. 2024, 16, 622–629. [Google Scholar] [CrossRef]
- Li, L.; Yang, J.; Wang, Y.; Liu, T.; Yao, C.; Huang, L.; Liu, N. Environmental neurotoxicity revisited: Evaluating microplastics as a potential risk factor for autism spectrum disorder. Innov. Med. 2025, 3, 100156. [Google Scholar] [CrossRef]
- Wang, Y.F.; Wang, X.Y.; Chen, B.J.; Yang, Y.P.; Li, H.; Wang, F. Impact of microplastics on the human digestive system: From basic to clinical. World J. Gastroenterol. 2025, 31, 100470. [Google Scholar] [CrossRef] [PubMed]
- Casella, C.; Cornelli, U.; Ballaz, S.; Recchia, M.; Zanoni, G.; Ramos-Guerrero, L. Preliminary Study on PCC-Chitosan’s Ability to Enhance Microplastic Excretion in Human Stools from Healthy Volunteers. Foods 2025, 14, 2190. [Google Scholar] [CrossRef]
- Mishra, S.K.; Sanyal, T.; Kundu, P.; Kumar, R.; Ghosh, D.; Chakrabarti, G.; Das, A. Microplastics as emerging carcinogens: From environmental pollutants to oncogenic drivers. Mol. Cancer 2025, 24, 248. [Google Scholar] [CrossRef]
- Dobrowolski, P.; Prejbisz, A.; Kuryłowicz, A.; Baska, A.; Burchardt, P.; Chlebus, K.; Bogdański, P. Metabolic syndrome—A new definition and management guidelines. Arter. Hypertens. 2022, 26, 99–121. [Google Scholar] [CrossRef]
- Ragusa, A.; Svelato, A.; Santacroce, C.; Catalano, P.; Notarstefano, V.; Carnevali, O.; Giorgini, E. Plasticenta: First evidence of microplastics in human placenta. Environ. Int. 2021, 146, 106274. [Google Scholar] [CrossRef] [PubMed]
- Ragusa, A.; Matta, M.; Cristiano, L.; Matassa, R.; Battaglione, E.; Svelato, A.; Nottola, S.A. Deeply in plasticenta: Presence of microplastics in the intracellular compartment of human placentas. Int. J. Environ. Res. Public Health 2022, 19, 11593. [Google Scholar] [CrossRef]
- Ali, N.; Katsouli, J.; Marczylo, E.L.; Gant, T.W.; Wright, S.; De La Serna, J.B. The potential impacts of micro-and-nano plastics on various organ systems in humans. EBioMedicine 2022, 99, 104901. [Google Scholar] [CrossRef] [PubMed]
- Amiri, H.; Moradalizadeh, S.; Jahani, Y.; Nasiri, A. Biomonitoring of microplastics in saliva and hands of young children in kindergartens: Identification, quantification, and exposure assessment. Environ. Monit. Assess. 2025, 197, 859. [Google Scholar] [CrossRef]
- Tiwari, B.R.; Lecka, J.; Pulicharla, R.; Brar, S.K. Microplastic pollution and associated health hazards: Impact of COVID-19 pandemic. Curr. Opin. Environ. Sci. Health 2023, 34, 100480. [Google Scholar] [CrossRef]
- Torres-Agullo, A.; Karanasiou, A.; Moreno, T.; Lacorte, S. Overview on the occurrence of microplastics in air and implications from the use of face masks during the COVID-19 pandemic. Sci. Total Environ. 2021, 800, 149555. [Google Scholar] [CrossRef] [PubMed]
- Casella, C.; Vadivel, D.; Dondi, D. The current situation of the legislative gap on microplastics (MPs) as new pollutants for the environment. Water Air Soil Pollut. 2024, 235, 778. [Google Scholar] [CrossRef]
- Casella, C.; Cornelli, U.; Zanoni, G.; Moncayo, P.; Ramos-Guerrero, L. Health Risks from Microplastics in Intravenous Infusions: Evidence from Italy, Spain, and Ecuador. Toxics 2025, 13, 597. [Google Scholar] [CrossRef]
- Ashim, J.; Ji, S.; Kim, H.Y.; Lee, S.W.; Jang, S.; Kim, W.; Yu, W. Protein Microplastic Coronation Complexes Trigger Proteome Changes in Brain-Derived Neuronal and Glial Cells. Environ. Sci. Technol. 2025, 59, 14993–15004. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Zhang, Q.; Wang, L.; Li, S.; Wang, K.; Xu, Y.; Qiu, Y. Take-out containers as nano-and microplastics reservoirs: Diet-driven gut dysbiosis in university students. Environ. Pollut. 2025, 384, 126985. [Google Scholar] [CrossRef]
- Guo, Y.; Rong, M.; Fan, Y.; Teng, X.; Jin, L.; Zhao, Y. The Presence of Microplastics in Human Semen and Their Associations with Semen Quality. Toxics 2025, 13, 566. [Google Scholar] [CrossRef]
- Hu, D.; Liu, H.; Guo, Y.; Zhang, H.; Qiu, M.; Yang, Z.; Zhang, M. Microplastics promote chemoresistance by mediating lipid metabolism and suppressing pyroptosis in colorectal cancer. Apoptosis 2025, 30, 2287–2300. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, J.; Shen, X.; Yang, L.; Jia, Y.; Song, F.; Ma, G. Microplastics in stools and their influencing factors among young adults from three cities in China: A multicenter cross-sectional study. Environ. Pollut. 2025, 364, 125168. [Google Scholar] [CrossRef]
- Xie, R.; Xiao, X.; Zhao, W.; Zhong, Y.; Wu, D.; Dou, J.; Liu, Y. Association between long-term exposure of polystyrene microplastics and exacerbation of seizure symptoms: Evidence from multiple approaches. Ecotoxicol. Environ. Saf. 2025, 302, 118741. [Google Scholar] [CrossRef]
- Xu, J.; Qu, J.; Jin, H.; Mao, W. Associations between Microplastics in Human Feces and Colorectal Cancer Risk. J. Hazard. Mater. 2025, 495, 139099. [Google Scholar] [CrossRef]
- Zheng, D.; Wang, D.; Zhang, S.; Liu, Y.; Xi, Q.; Weng, Y. Impact of urinary microplastic exposure on cognitive function in primary school children. Ecotoxicol. Environ. Saf. 2025, 302, 118532. [Google Scholar] [CrossRef]
- Marfella, R.; Prattichizzo, F.; Sardu, C.; Fulgenzi, G.; Graciotti, L.; Spadoni, T.; Paolisso, G. Microplastics and nanoplastics in atheromas and cardiovascular events. N. Eng. J. Med. 2024, 390, 900–910. [Google Scholar] [CrossRef]
- Jenner, L.C.; Rotchell, J.M.; Bennett, R.T.; Cowen, M.; Tentzeris, V.; Sadofsky, L.R. Detection of microplastics in human lung tissue using μFTIR spectroscopy. Sci. Total Environ. 2022, 831, 154907. [Google Scholar] [CrossRef]
- Tsokos, G.C. The immunology of systemic lupus erythematosus. Nat. Immunol. 2024, 25, 1332–1343. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Costa, F. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef]
- Ordás, I.; Eckmann, L.; Talamini, M.; Baumgart, D.C.; Sandborn, W.J. Ulcerative colitis. Lancet 2012, 380, 1606–1619. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Agusti, A. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Gabbay, R.A. Introduction and methodology: Standards of care in diabetes—2023. Diabetes Care 2022, 46 (Suppl 1), S1. [Google Scholar] [CrossRef] [PubMed]
- Jurado-Priego, L.N.; Cueto-Ureña, C.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Fibromyalgia: A review of the pathophysiological mechanisms and multidisciplinary treatment strategies. Biomedicines 2024, 12, 1543. [Google Scholar] [CrossRef]
- Lea, A.S.; Khurana, J.K. Medical Reference Tools and Pharmaceutical Promotion: A History of Entanglement. Ann. Int. Med. 2025, 178, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Váradi, C. Clinical features of Parkinson’s disease: The evolution of critical symptoms. Biology 2020, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, P.; Elia, G.; Ragusa, F.; Paparo, S.R.; Patrizio, A.; Balestri, E.; Ferrari, S.M. Thyroid autoimmunity and SARS-CoV-2 infection. J. Clin. Med. 2023, 12, 6365. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Assessing National Capacity for the Prevention and Control of Noncommunicable Diseases: Report of the 2021 Global Survey; World Health Organization: Cambridge, MA, USA, 2023; Available online: https://books.google.es/books?hl=es&lr=&id=OaIOEQAAQBAJ&oi=fnd&pg=PR5&dq=Fact+sheet:+noncommunicable+diseases+2023&ots=p15J-xsQck&sig=fLqXvRb4JunM0GSC_J57jjZFKQo#v=onepage&q=Fact%20sheet%3A%20noncommunicable%20diseases%202023&f=false (accessed on 12 October 2025).
- MSD Manual. Clinical Reference. 2025. Available online: https://www.msdmanuals.com/professional (accessed on 12 October 2025).
- Mehra, A.; Khanna, J.; Singh, G.; Sachdeva, V.; Bedi, N. A Comprehensive Review on Major Depressive Disorder: Exploring Etiology, Pathogenesis and Clinical Approaches. Curr. Behav. Neurosci. Rep. 2025, 12, 18. [Google Scholar] [CrossRef]
- Mayo Clinic. Health Information Resource. 2025. Available online: https://monument.health/mayo-clinic-health-information-library/ (accessed on 12 October 2025).
- Puledda, F.; Silva, E.M.; Suwanlaong, K.; Goadsby, P.J. Migraine: From pathophysiology to treatment. J. Neurol. 2023, 270, 3654–3666. [Google Scholar] [CrossRef]
- Shenot, P.J. Thomas Jefferson University Hospital. 2023. Available online: https://www.merckmanuals.com/en-ca/home/kidney-and-urinary-tract-disorders/disorders-of-urination/control-of-urination (accessed on 12 October 2025).
- Nguyen, N.N.; Tissot-Dupont, H.; Brouqui, P.; Gautret, P. Post-COVID syndrome in symptomatic COVID-19 patients: A retrospective cohort study. BMC Infect Dis. 2025, 25, 1099. [Google Scholar] [CrossRef]
- World Health Organization. Fact Sheet: Infectious Diseases. 2025. Available online: https://www.who.int/news-room/fact-sheets (accessed on 12 October 2025).
- Cecchetti, M.; Scarallo, L.; Lionetti, P.; Ooi, C.Y.; Terlizzi, V. Impact of highly effective modulator therapy on gastrointestinal symptoms and features in people with cystic fibrosis. Paediat. Respir. Rev. 2025, 54, 70–75. [Google Scholar] [CrossRef]
- Neves, F.S.; Pereira, I.A.; Sztajnbok, F.; Rosa Neto, N.S. Sarcoidosis: A general overview. Adv. Rheumatol. 2024, 64, 57. [Google Scholar] [CrossRef]
- Porsteinsson, A.P.; Isaacson, R.S.; Knox, S.; Sabbagh, M.N.; Rubino, I. Diagnosis of early Alzheimer’s disease: Clinical practice in 2021. J. Prev. Alzheimer Dis. 2021, 8, 371–386. [Google Scholar] [CrossRef]
- Amar, S.; Binet, A.; Téteau, O.; Desmarchais, A.; Papillier, P.; Lacroix, M.Z.; Elis, S. Bisphenol S impaired human granulosa cell steroidogenesis in vitro. Int. J. Mol. Sci. 2020, 21, 1821. [Google Scholar] [CrossRef]
- Abdelouahab, N.; Langlois, M.F.; Lavoie, L.; Corbin, F.; Pasquier, J.C.; Takser, L. Maternal and cord-blood thyroid hormone levels and exposure to polybrominated diphenyl ethers and polychlorinated biphenyls during early pregnancy. Am. J. Epidemiol. 2013, 178, 701–713. [Google Scholar] [CrossRef]
- Lu, K.; Zhan, D.; Fang, Y.; Li, L.; Chen, G.; Chen, S.; Wang, L. Microplastics, potential threat to patients with lung diseases. Front. Toxicol. 2022, 4, 958414. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).