Abstract
Objective: This scoping review synthesized and mapped the breadth of the existing literature on technological resources used to support individuals undergoing hemodialysis treatment. Methods: Following the methodological guidelines of the Joanna Briggs Institute (JBI) for scoping reviews and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist, comprehensive searches were conducted across the following databases: MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Scopus, Scientific Electronic Library Online (SciELO), MedicLatina, and the Cochrane Central Register of Controlled Trials, with no time restrictions. Results: Thirty-nine studies conducted between 2003 and 2023 met the inclusion criteria. These studies covered a range of technological innovations developed specifically for hemodialysis treatment, including virtual reality, exergames, websites, and mobile applications. These technologies were designed with diverse objectives: to facilitate physical exercise, optimize dietary and medication management, improve disease adherence and management, and promote self-efficacy and self-care in patients. Conclusions: The review revealed a wide range of technological resources available to hemodialysis patients. These digital solutions show great potential to transform care by promoting more engaged and personalized health practices. Although this study did not directly assess the impact of these technologies, it provides a solid foundation for future investigations that can explore in-depth how such innovations contribute to effective disease management and improvement in clinical outcomes.
1. Introduction
Chronic kidney disease (CKD) is defined as abnormalities in kidney structure or function that have been present for at least three months and have implications for a person’s health [1]. This disease is classified based on its cause, the category of glomerular filtration rate (GFR), and the level of albuminuria [1,2]. The progression of CKD through its various grades culminates in kidney failure, known as grade 5 [1,3].
In 2021, a joint statement from the American Society of Nephrology, the European Renal Association, and the International Society of Nephrology pointed out that more than 850 million people suffer from some form of kidney disease, approximately double the number of people with diabetes, 20 times higher than the prevalence of cancer, and more than those living with AIDS/HIV [1].
Given the high prevalence and progressive nature of CKD, more appropriate and comprehensive patient monitoring is required to initiate renal replacement therapy, allowing for a transition to a new lifestyle [2]. There are three types of renal replacement therapies: peritoneal dialysis, hemodialysis (HD), and kidney transplantation [3]. Hemodialysis is the most common therapy, with treatment sessions lasting between 3 and 5 h [2].
Furthermore, it is important to highlight the significant impact of the symptoms associated with CKD, which directly affect patients’ quality of life [4,5]. CKD causes various symptoms, such as fatigue, pain, anxiety, and depression. Renal replacement therapies like hemodialysis may improve some of these symptoms but do not completely reverse them [5].
However, the treatment of kidney failure goes beyond hemodialysis sessions. Kidney failure involves a complex therapeutic regimen requiring considerable patient adherence. In addition to hemodialysis treatment, this regimen includes medication, fluid intake control, dietary restrictions, and vascular access maintenance [4]. These therapeutic demands result in substantial changes to the patient’s lifestyle and quality of life due to the challenging clinical and therapeutic management of the disease, as well as recurrent hospitalizations due to complications [6].
Considering the difficulties in adhering to hemodialysis, the need to implement new strategies that facilitate adaptation to dialysis treatment arises. The use of new technologies has been a topic of discussion within the scientific community in the healthcare field, particularly in research on the application and evaluation of health technologies for managing chronic kidney disease [7,8,9], with a focus on mobile applications [9].
Digital health is defined as encompassing not only eHealth but also digital consumers, smart devices, the Internet of Things, advanced computing, big data analytics, artificial intelligence including machine learning, and robotics [10]. Digital health technologies go beyond mobile apps and can be defined as a set of knowledge and practices related to developing and using digital technologies to improve health outcomes [10]. These tools can potentially provide diagnoses, treatment, prognoses, and disease management, reducing patient waiting times and travel. Additionally, they can lower costs for the healthcare system and patients, providing more comfort and enhancing self-efficacy [11]. Technological resources may exert distinct impacts across all stages of CKD, and they may support prevention and risk factor control to facilitate adherence to therapeutic regimens and self-management [8,9].
In this context, digital health interventions not only improve access to information but also promote the self-management of healthcare, thus contributing to better clinical outcomes [11,12,13]. Furthermore, the efficient and safe use of technological resources plays a crucial role in supporting healthcare services, disseminating health information, disease surveillance, health education, and facilitating knowledge production and scientific research [14,15], making them increasingly important tools for personalized healthcare [15].
Given the complex epidemiology of CKD and its significant impact on healthcare systems, professionals must invest not only in health promotion and preventive care but also in continuous innovation and research in their daily practices.
Hemodialysis is the most prevalent modality of kidney replacement therapy worldwide, encompassing most patients with end-stage chronic kidney disease [16]. Although other therapeutic options, such as peritoneal dialysis and kidney transplantation, also entail significant clinical and psychosocial challenges, HD is distinguished by its substantial burden in these domains, reflected in high morbidity rates and a five-year survival of less than 50% [17]. These specificities underscore the relevance of investigating and implementing technological resources tailored to this population. Patients undergoing hemodialysis face specific daily challenges, including lifestyle limitations, adherence to complex medication regimens, and nutritional adaptation [18]. Given these challenges, this investigation aims to explore how digital technologies, which are revolutionizing chronic disease care, can facilitate patient monitoring. Technological resources that may improve treatment adherence and enhance quality of life [8,19] are considered.
It is important to emphasize that the technological resources analyzed in this review are not designed to modify the fundamental nature of hemodialysis, but rather to alleviate its consequences. In this review, “technological resources” refers to digital or technology-based interventions developed to support patient care, education, monitoring, or rehabilitation, in the context of hemodialysis. These may include mobile health applications [7,9,18], websites and digital platforms [8,12], virtual reality environments and exergames [9], telehealth solutions [8], and wearable devices [10,15]. Such technologies can enable more effective health self-management by patients, potentially covering various aspects of adherence to the dialysis regimen. Self-efficacy, that is, the belief in one’s ability to manage these tasks, is crucial for improving health outcomes and reducing reliance on intensive medical interventions [19]. The existing literature on digital health has mainly focused on chronic disease management in general [7,12,13], leaving a clear gap regarding technological resources specifically directed at patients undergoing hemodialysis [18]. Therefore, the primary objective of this scoping review was to map the available scientific evidence on the use of technological resources to support patients undergoing hemodialysis. This review is guided by the following research question: “What types of technological resources are available for patients undergoing hemodialysis?”.
2. Methods
A scoping review was conducted following the Joanna Briggs Institute (JBI) guidelines for this type of study [20]. To structure all the information, we used the PRISMA-ScR extension (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) [21], which outlines the phases of the investigation. The research protocol was then registered on the Open Science Framework® platform (OSF: https://doi.org/10.17605/OSF.IO/VUFE3 accessed on: 9 June 2025).
2.1. Search Strategy
A search was conducted in the following databases: MEDLINE (via PubMed, National Library of Medicine, Bethesda, MD, USA), Cumulative Index to Nursing and Allied Health Literature -CINAHL (EBSCOhost, Ipswich, MA, USA), PsycINFO (American Psychological Association, Washington, DC, USA), Scopus (Elsevier, Amsterdam, The Netherlands), Scientific Electronic Library Online-SciELO (São Paulo, Brazil), MedicLatina (EBSCOhost, Ipswich, MA, USA), and the Cochrane Central Register of Controlled Trials- CENTRAL (The Cochrane Library, London, UK), using specific syntax and indexing terms for each. The search strategies were jointly formulated and conducted by two investigators (AM, CF). All searches were carried out in December 2024. The search strategies for all databases are available in Appendix A.
2.2. Eligibility Criteria
The research question was formulated using the PCC (Population, Context, Concept) acronym. The population considered were patients, the context was hemodialysis, and the concept was technological resources. The concept of this review was “technological resources”. For the purposes of this study, technological resources were defined as digital or technology-based interventions designed to support, monitor, or enhance the management of patients undergoing hemodialysis, including mobile applications, websites, exergames, virtual reality, and wearable devices.
All articles published up to December 2024 were included. The search language was English, although articles published in Spanish, Portuguese, and French were also considered. Articles involving the development or use of technological resources to support patients undergoing hemodialysis treatment were deemed eligible, regardless of the period of use (inter- or intradialytic). Home hemodialysis was deliberately excluded. This decision was grounded in the observation that most technological resources reported in the literature are specifically designed for in-center hemodialysis. In addition, home hemodialysis remains a less commonly adopted modality worldwide, with technological requirements and patient experiences that differ substantially from those of in-center hemodialysis. Therefore, to maintain conceptual clarity and avoid conflating distinct patient populations, only studies involving in-center hemodialysis patients were included. All age groups were included. Articles that did not address health-related technological resources were excluded.
Eligible study designs comprised experimental studies (e.g., randomized controlled trials, pilot trials, quasi-experimental designs), observational studies (e.g., cross-sectional, cohort, descriptive prospective studies), qualitative studies (e.g., interviews, focus groups, thematic analyses), and mixed-methods studies. Reviews, protocols, and opinion papers were excluded. Additionally, any evidence that was not primary research related to the development and use of resources, such as conceptual articles, editorials, unpublished literature including theses and books, or studies in books, were also excluded.
Authors of studies with unavailable data were contacted for clarifications or additional information about their studies, as recommended by the JBI methodology [20]. Furthermore, the search for supplementary studies was expanded to include the examination of reference lists of all publications selected for inclusion in the review, a process known as “backward citation tracking”.
2.3. Data Extraction
The data extraction form was initially developed by two investigators, based on the predefined objectives and inclusion criteria of the study. To ensure accuracy and consistency, the form was subsequently pre-tested by two additional investigators. The results from each database search were imported into the Rayyan® software (web-based software; 2024, Qatar Computing Research Institute, Doha, Qatar) to assist with the development of the review. Duplicate references were removed, and two investigators performed the initial selection by reading the titles and abstracts according to the pre-defined inclusion/exclusion criteria. Subsequently, the full texts of the selected references were obtained to decide their inclusion or exclusion in the final study. Any discrepancies were discussed with a third investigator. The PRISMA-ScR framework was used to organize the information resulting from the selection process [21]. All scientific articles were coded with the letter (E) in the order they were reviewed.
2.4. Data Analysis
The selection, data extraction, and synthesis process were carried out independently by two investigators (AM, CF), with the involvement of a third investigator (MF) in the case of discrepancies. To synthesize the obtained data, a customized extraction table was developed, containing the following information: authors, year of publication, country, research objectives, methodology, participants, type of technology, purpose of the technology, duration of the intervention, assessment tools, and results. The data are presented in a descriptive manner (Table 1).

Table 1.
Characteristics of studies included in the scoping review.
3. Results
The search strategy identified 932 records. In line with the PRISMA 2020 statement, it is important to distinguish between records, reports, and studies when describing the evidence selection process. Records correspond to the bibliographic citations retrieved from databases prior to deduplication. Reports denote the full-text publications assessed for eligibility, which may consist of one or more records referring to the same investigation. Finally, studies constitute the primary unit of inclusion in this review and may be reported in single or multiple publications. This distinction enhances transparency and consistency in the reporting of systematic and scoping reviews [61]. After the different stages outlined in Figure 1, 39 studies were deemed eligible and included in the analysis.
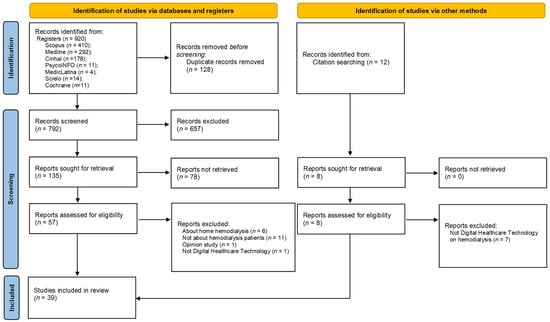
Figure 1.
Article identification and inclusion process.
3.1. Characteristics of the Included Studies
Table 1 summarizes the characteristics of the 39 studies included in this review, including authors, year, country, objectives, methodology, participants, type of technological resource, purpose of the technological resource, duration of the intervention, assessment tools, and results. A total of 39 articles published between 2003 and 2023 were selected for inclusion in the review [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]. The studies were conducted in various countries. The most frequent study design identified was the pilot study, representing 16 of the 39 included studies, followed by randomized controlled trials (n = 11), clinical trials (n = 4), and quasi-experimental studies (n = 5).
3.2. Characteristics of Participants
Regarding the participants, 2036 individuals were included in the analyzed studies, with adults predominating. However, study E16 involved children, study E11 was conducted with adolescents, and study E25 included both adolescents and children. In studies E18 and E19, both healthy individuals and patients undergoing hemodialysis were included. In study E14, healthy university students were used to assess the safety and efficacy of a virtual reality intervention in a context that could potentially be adapted for patients in the future.
3.3. Characteristics Technologies Resources
Regarding the types of technological resources developed in the included studies (Table 1), 12 studies used virtual reality technology. Of these, seven studies addressed non-immersive virtual reality (E3, E5, E7, E9, E17, E22, E23), while five studies used immersive virtual reality (E4, E6, E14, E15, E28). Three studies involved exergames (E1, E2, E8), and nineteen studies utilized mobile apps (E11, E12, E13, E18, E19, E20, E21, E24, E26, E27, E29, E31, E32, E33, E35, E36, E37, E38, E39). Additionally, five studies used other types of technologies, including a website (E10), two video games (E16, E25), a remote technology (E30), and a digital platform (E34) (Figure 2).
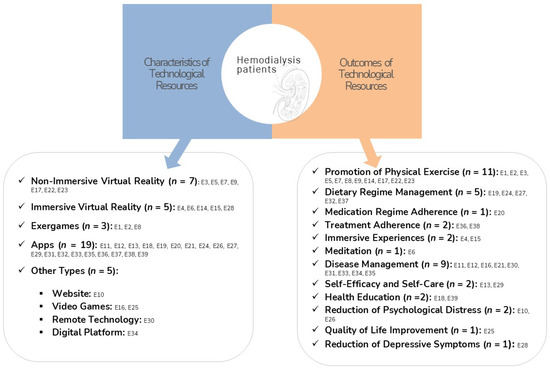
Figure 2.
Distribution of technologies resources.
3.4. Outcomes of the Technologies Resources
The outcomes of the technologies were as follows: eleven promoted physical exercise (E1, E2, E3, E5, E7, E8, E9, E14, E17, E22, E23), five focused on dietary regimen management (E19, E24, E27, E32, E37), one aimed at medication adherence (E20), two focused on treatment adherence (E36, E38), two provided immersive experiences (E4, E15), one offered meditation (E6), nine focused on disease management (E11, E12, E16, E21, E30, E31, E33, E34, E35), two aimed at increasing self-efficacy and self-care (E13, E29), two focused on health education (E18, E39), two aimed to reduce psychological distress (E10, E26), one aimed to improve quality of life (E25), and one aimed to reduce depressive symptoms (E28).
4. Discussion
In this scoping review, 39 studies conducted between 2003 and 2023 were analyzed, investigating the use of 39 different technological resources in treating hemodialysis patients. This review spans an extended period to provide a comprehensive view of technological advancements in this field. The types of technological resources discussed in this context include virtual reality systems, mobile applications, interactive websites, and digital platforms, each tailored to enhance the management and treatment of hemodialysis patients.
4.1. Mobile Applications (Apps)
According to the analysis of the studies, the use of mobile applications was explored in 19 studies [32,41,42]. Mobile applications were developed to assist in dietary regimen management [40,42,53], medication adherence [41], disease management [33,52,54,56], promotion of self-efficacy and self-care [32,34,50], health education [39,60], treatment adherence [57,59], and reduction in psychological distress [47]. Mobile applications are essential in supporting both patients and healthcare professionals, allowing for the storage and sharing of information that fosters a collaborative approach to patient care. However, the development of these tools must include all end-users to ensure efficient design [62].
According to the included studies, the apps provided practical support for monitoring health indicators, such as weight, potassium, phosphorus, iron, and albumin levels in the blood [48,53,58]. They also offered spaces for food diaries and tracking fluid and mineral levels [40,45]. Dietary and fluid intake restrictions require constant management by patients, making it one of the most challenging aspects of dialysis treatment. In this regard, mobile health applications can be valuable tools to facilitate self-management of these patients’ nutritional and dietary plans [63].
In one study, a mobile application was developed for phosphate control, incorporating educational videos and interactive features that allowed for dietary self-management. The use of this app resulted in reductions in serum phosphate levels and phosphate intake, improving patients’ knowledge and adherence to phosphate binders [58].
Another study developed a dietary self-management app that allowed patients to monitor nutrients such as protein, calories, and minerals in their food. After 12 weeks of use, the app resulted in reductions in phosphorus and potassium levels [53]. Hemodialysis patients often need to make significant dietary adjustments. Mobile applications focused on nutrition tend to improve adherence to dietary changes compared to traditional methods [64]. Additionally, these interventions facilitate the daily recording of food and fluid intake, making them accessible tools for dietary self-management in hemodialysis patients [65].
In addition to nutritional aspects, an app focused on medication adherence incorporated features such as medication reminders for hemodialysis patients [41]. Seven other applications concentrated on self-management, self-efficacy, and self-care, offering information on hemodialysis, nutrition, infection prevention, and preventive measures, positively impacting patients’ self-care and self-efficacy [32,33,34,50]. The need to integrate features such as education, goal setting, self-monitoring, and interactive feedback into health apps was emphasized [66]. Moreover, one application allowed for the monitoring of interdialytic weight and diet adherence, providing real-time feedback, and showed significant improvements in patients’ self-efficacy and behavior [50].
4.2. Virtual Reality
After analysis, 12 studies addressed virtual reality (VR), with a predominant use of non-immersive virtual reality [39,43,44] compared to immersive VR [27,36,49], which offers more immersive experiences [67]. These technologies showed significant improvements in patients’ functional capacity, mobility, balance, and flexibility [28,38,43], positively impacting hemodynamic parameters and stress levels during treatment [36,44].
In addition to its physical benefits, virtual reality (VR) has been shown to reduce negative emotions and enhance psychological well-being by serving as a distractive intervention that alleviates physical and psychological symptoms such as pain, nausea, and anxiety [28,36,49,68]. Both immersive and non-immersive VR are regarded as safe and effective during hemodialysis sessions, without inducing adverse effects such as nausea or virtual disruptions [27,35,38]. These findings are complemented by studies that assessed the cost-effectiveness of these technologies, demonstrating that virtual reality-based interventions can significantly reduce healthcare costs, including expenses for laboratory tests, radiology exams, and outpatient consultations [30]. These discoveries highlight VR’s potential not only to improve the quality of life of hemodialysis patients but also to optimize healthcare resources.
4.3. Exergames
Exergames, games that track user movements and integrate them into an engaging environment, are noted for their ability to encourage active participation during hemodialysis [69]. Three studies in the exergame category [22,23,29] have adopted this technology to promote physical activity by merging exercise with digital game components. These studies have demonstrated significant improvements in areas such as gait speed and motor control, in addition to helping reduce depressive symptoms [23,70]. It is important to highlight that engaging in physical exercise through exergames during hemodialysis can offer multiple benefits: optimizing time spent at the dialysis center, enhancing the treatment experience, alleviating the monotony of the treatment, and significantly contributing to the mental health promotion of patients [26].
4.4. Other Health Information Technologies
In the context of hemodialysis treatment, besides technologies like VR, mobile apps, and exergames, other modalities were explored, including two video games [37,46], one website [31], one digital platform [55], and one remote technology [51]. These innovations not only diversified therapeutic options but also enriched the patient experience. The video games, specifically designed for children and adolescents undergoing hemodialysis, provided a three-dimensional virtual environment that allowed users to interact in a virtual city, promoting socialization and creativity [37]. One such game, a Role-Playing Game (RPG) called Nefro Hero®, was created to enhance the quality of life through interactive narratives that encouraged problem-solving and reflection, addressing the experiences of young patients [46].
Additionally, a website was developed to offer online cognitive behavioral therapy, focusing on challenges and the associated psychosocial changes [31]. A digital platform also stood out by providing educational programs about the disease, showing improvements in patient self-management and knowledge [55]. These digital platforms proved to be valuable resources in health management and psychological support for patients, facilitating ongoing education and active involvement in their treatment.
4.5. Impact of Technological Resources on Health Outcomes
The objectives of technologies reflected in the study outcomes span a wide range of applications, underscoring the diversity and potential of technology in chronic disease management. A significant focus is placed on promoting physical activity, with 11 technologies specifically aimed at this purpose [22,23,24,25]. Intradialytic exercise could enhance the quality of life across various domains for patients undergoing hemodialysis [71]. Dietary management [40,45] and disease management [32,33] are other prevalent areas highlighted by the study findings, illustrating the importance and complexity of these interventions in the patient care continuum. While information or knowledge about the different aspects of therapy is critical for building awareness, it alone is insufficient to effect or sustain behavioral change [72,73].
An important consideration concerns whether the integration of technological resources in HD represents a technology-driven (push) or a patient-driven (pull) process. Evidence from patient-reported outcomes remains limited, and few surveys have systematically explored the priorities and expectations of individuals undergoing HD regarding such technologies. Nevertheless, available data indicate that patients highly value interventions that address depression [23,26], enhance dietary and medication adherence [22,38], and improve psychological well-being [31,47]. Thus, while auxiliary technological resources offer promising support, their benefits must be interpreted within the broader and often conflicting clinical and psychosocial trade-offs that characterize the HD experience.
Hemodialysis prolongs survival but imposes a profound burden on patients’ daily lives [74]. The impact extends across physical, psychological, social, and financial domains [75,76]. Patients frequently report debilitating symptoms, including persistent fatigue, muscle cramps, pruritus, sleep disturbances, gastrointestinal complaints, and anorexia, in addition to a high burden of cardiovascular complications [77]. Moreover, strict dietary and fluid restrictions represent ongoing challenges, often exacerbating frustration and emotional distress [76]. Within this context, technological resources emerge as promising adjuncts, with potential to mitigate symptom burden, enhance treatment adherence, and ultimately improve patients’ quality of life.
In summary, the resources analyzed in our review study emerge as crucial for enhancing the patient experience during hemodialysis, encouraging them to take an active role in managing their health. These resources have the potential to significantly increase patient engagement in their own care [62], with an observed increase in recent years [78,79]. However, while these solutions serve many well, younger patients, especially those in the early stages of the disease, may require more advanced technological approaches focused on primary prevention and improving treatment adherence [78]. For future developments, it is crucial to recognize that the chronic kidney disease population is diverse in terms of digital health literacy, suggesting that standardized approaches may not be effective for everyone [78,79].
4.6. Limitations
As a scoping review, this study offers a comprehensive overview of the available literature, but it has several important limitations. One such limitation is language restriction, as only studies in four languages were included. Relevant studies published in other languages were not considered, potentially limiting the generalizability of the results. Another significant limitation of this type of review is that, unlike systematic reviews, a scoping review does not assess the methodological quality of the included studies. This means the results might encompass studies with lower scientific rigor, preventing a deeper critical analysis of the strength of the evidence. These characteristics limit the ability to distinguish between technologies’ proven effects and those that may have been positively reported due to potential biases in the original studies.
Furthermore, implementing technology in hemodialysis treatment faces challenges, such as adapting technological resources to the diverse needs of patients, who vary in terms of age, medical conditions, and cognitive ability. Adopting a user-centered design methodology is crucial to overcome these barriers and ensure that devices are useful and accessible [70,79,80,81]. Finally, the effective implementation of technologies in dialysis centers requires that they be integrated in a way that does not disrupt existing workflows and that patient data is handled with the utmost security to ensure privacy and compliance with legal standards. Acceptance by healthcare professionals and adequate training is essential for the successful and sustainable adoption of technological solutions.
5. Conclusions
This study provided a comprehensive overview of the technologies applied in supporting patients undergoing hemodialysis, mapping a variety of tools, ranging from VR to mobile applications, developed and evaluated over the past two decades. Among the technologies cataloged, mobile apps and VR technologies stood out due to their prevalence, highlighting their potential to assist in disease management, self-management, and improving patients’ quality of life. These technologies primarily focused on promoting physical exercise, managing diet and medication regimens, and other essential aspects of patient self-care and self-efficacy. The development of these technologies reflects a growing trend toward integrative approaches in hemodialysis, with a strong emphasis on personalizing treatment to meet patients’ specific needs.
Despite challenges related to safety, adaptation, and implementation, these technologies emerge as valuable tools for healthcare professionals to develop more effective support strategies. To maximize the potential of these innovations, it is recommended that healthcare professionals maintain a continuous and evolving dialog with patients, ensuring that interventions are tailored to individual needs and effectively promote treatment adherence.
For future research, it is essential to adopt a multidisciplinary approach, integrating knowledge from fields such as medicine, engineering, design, and information technology. This collaborative effort could result in developing even more effective and personalized solutions. Moreover, it is crucial to explore the integration of patient feedback to continuously assess the applicability and safety of implemented technologies, adjusting them as necessary to ensure that interventions are both safe and beneficial.
In summary, although the study did not directly assess the impact of these technologies, its compilation offers a solid foundation for future investigations, which may explore in depth how these innovations can continue to transform hemodialysis, significantly improving treatment outcomes and patients’ lives.
Author Contributions
Conceptualization, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; methodology, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; validation, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; formal analysis, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; investigation, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; data curation, A.R.M., M.C.F. and C.S.F.; writing—original draft preparation, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; writing—review and editing, A.R.M., M.T.M., A.L., S.F., M.C.F. and C.S.F.; supervision, C.S.F.; project administration, C.S.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Search Strategies According to the Database
| Database | Research Strategy |
| MEDLINE | (((MH “Patients”) OR (MH “Patient Education as Topic”) OR (“Patient*”) OR (“Adult*”) OR (“Person”) OR (“Aged”)) AND ((MH “Educational Technology”) OR (MH “Digital Technology”) OR (MH “Games, Recreational”) OR (MH “Video Games”) OR (MH “Gamification”) OR (MH “Play and Playthings”) OR (MH “Mobile Applications”) OR (MH “Digital Technology”) OR (MH “Technology”) OR (MH “virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“APPs”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND ((MH “Renal Dialysis”) OR (MH “Kidneys, Artificial”) OR (MH “Intermittent Renal Replacement Therapy”) OR (MM “Renal Insufficiency, Chronic”) OR (MH “hemodialysis Units, Hospital”) OR (MH “Renal Replacement Therapy”) OR (MH “Dialysis”) OR (“hemodialysis”) OR (“hemodialysis”) OR (“Renal Dialysis”) OR (“Renal Insufficiency”) OR (“Kidney Failure”))) |
| CINAHL | (((MH “Patients”) OR (MH “Patient Education”) OR (MH “Dialysis Patients”) OR (“Patient*”) OR (“Adult*”) OR (“Person”) OR (“Aged”)) AND ((MH “Educational Technology”) OR (MH “Digital Technology”) OR (MH “Games, Recreational”) OR (MH “Video Games”) OR (MH “Gamification”) OR (MH “Play and Playthings”) OR (MH “Mobile Applications”) OR (MH “Technology”) OR (MH “virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“APPs”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND (((MH “hemodialysis”) OR (MH “hemodialysis Therapy (Iowa NIC)”) OR (MH “Dialysis Centers”) OR (MH “Renal Replacement Therapy”) OR (MH “Kidney Failure, Chronic”) OR (“hemodialysis”) OR (“hemodialysis”) OR (“Renal Dialysis”) OR (“Renal Insufficiency”) OR (“Kidney Failure”))) |
| PsycINFO | ((DE “PATIENTS”) OR (DE “PATIENT care”) OR (DE “PATIENT education”) OR (DE “hemodialysis patients”) OR (“Patient Education”) OR (“Dialysis Patients”) OR (“Patient*”) OR (“Adult*”) OR (“Person”) OR (“Aged”) AND (DE “GAMIFICATION”) OR (DE “GAMES”) OR (DE “GAMES & technology”) OR (DE “GAMES -- Therapeutic use”) OR (DE “EDUCATIONAL games”) OR (DE “VIDEO game software”) OR (DE “VIDEO games”) OR (DE “TECHNOLOGY”) OR (DE “EDUCATIONAL technology”) OR (“Educational Technology”) OR (“Digital Technology”) OR (“Games Recreational”) OR (“Video Games”) OR (“Gamification”) OR (“APPS”) OR (“Play and Playthings”) OR (“Mobile Applications”) OR (“Technology”) OR (“virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND ((DE “KIDNEY disease treatments”) OR (DE “RENAL replacement therapy”) OR (DE “HEMODIALYSIS”) OR (DE “KIDNEY disease treatments”) |
| Scopus | (TITLE-ABS-KEY ((“Patient Education”) OR (“Dialysis Patients”)) AND TITLE-ABS-KEY ((“Educational Technology”) OR (“Digital Technology”) OR (“Games Recreational”) OR (“Video Games”) OR (“Gamification”) OR (“APPS”) OR (“Play and Playthings”) OR (“Mobile Applications”) OR (“Technology”) OR (“virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND TITLE-ABS-KEY ((“Renal Dialysis”) OR (“Kidneys Artificial”) OR (“Renal Therapy”) OR (“hemodialysis Units”) OR (“Dialysis”) OR (“hemodialysis”) OR (“hemodialysis”) OR (“Renal Insufficiency”))) |
| SciELO | (((“Patient Education”) OR (“Dialysis Patients”)) AND ((“Educational Technology”) OR (“Digital Technology”) OR (“Games Recreational”) OR (“Video Games”) OR (“Gamification”) OR (“APPS”) OR (“Play and Playthings”) OR (“Mobile Applications”) OR (“Technology”) OR (“virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND ((“Renal Dialysis”) OR (“Kidneys Artificial”) OR (“Renal Therapy”) OR (“hemodialysis Units”) OR (“Dialysis”) OR (“hemodialysis”) OR (“hemodialysis”) OR (“Renal Insufficiency”))) |
| MedicLatina | (((“Patient Education”) OR (“Dialysis Patients”)) AND ((“Educational Technology”) OR (“Digital Technology”) OR (“Games Recreational”) OR (“Video Games”) OR (“Gamification”) OR (“APPS”) OR (“Play and Playthings”) OR (“Mobile Applications”) OR (“Technology”) OR (“virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND ((“Renal Dialysis”) OR (“Kidneys Artificial”) OR (“Renal Therapy”) OR (“hemodialysis Units”) OR (“Dialysis”) OR (“hemodialysis”) OR (“hemodialysis”) OR (“Renal Insufficiency”))) |
| Cochrane Library | (((“Patient Education”) OR (“Dialysis Patients”)) AND ((“Educational Technology”) OR (“Digital Technology”) OR (“Games Recreational”) OR (“Video Games”) OR (“Gamification”) OR (“APPS”) OR (“Play and Playthings”) OR (“Mobile Applications”) OR (“Technology”) OR (“virtual reality”) OR (“Game*”) OR (“Gamification”) OR (“Video Game*”) OR (“virtual reality”) OR (“Boardgame”) OR (“Digital Technology”) OR (“Mobile Application”) OR (“Web System”)) AND ((“Renal Dialysis”) OR (“Kidneys Artificial”) OR (“Renal Therapy”) OR (“hemodialysis Units”) OR (“Dialysis”) OR (“hemodialysis”) OR (“hemodialysis”) OR (“Renal Insufficiency”))) |
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024, 105, S117–S314. [Google Scholar] [CrossRef]
- Daugirdas, J.; Blake, P.; Ing, T. Handbook of Dialysis, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2015. [Google Scholar]
- Luyckx, V.; Tonelli, M.; Stanifer, J. The global burden of kidney disease and the sustainable development goals. Bull. World Health Organ. 2018, 96, 414–422D. [Google Scholar] [CrossRef]
- Chironda, G.; Bhengu, B. Contributing Factors to Non-Adherence among Chronic Kidney Disease (CKD) Patients: A Systematic Review of Literature. Med. Clin. Rev. 2016, 2, 29. [Google Scholar] [CrossRef]
- Farinha, A. Symptom control in End Stage Renal Disease. Port. J. Nephrol. Hypertens. 2017, 31, 192–199. [Google Scholar]
- Sułkowski, L.; Rynkowski, W.; Szyszkowska, A.; Rezmerska, L.; Krajewska, M. Social Support and Quality of Life in Hemo-dialysis Patients: A Comparative Study with Healthy Controls. Healthcare 2024, 12, 1219. [Google Scholar] [CrossRef]
- Scott, I.; Scuffham, P.; Gupta, D.; Harch, T.; Borchi, J.; Richards, B. Going digital: A narrative overview of the effects, quality and utility of mobile apps in chronic disease self-management. Aust. Health Rev. 2020, 44, 62–82. [Google Scholar] [CrossRef]
- Diamantidis, C.J.; Becker, S. Health information technology (IT) to improve the care of patients with chronic kidney disease (CKD). BMC Nephrol. 2014, 15, 7. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, H.; Qazi, H.; Morita, P. Intervention and Evaluation of Mobile Health Technologies in Management of Patients Undergoing Chronic Dialysis: Scoping Review. JMIR Mhealth Uhealth 2020, 8, e15549. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Digital Health 2020–2025. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/344249/9789240020924-eng.pdf (accessed on 9 June 2025).
- Moulaei, K.; Moulaei, R.; Bahaadinbeigy, K. Barriers and facilitators of using health information technologies by women: A scoping review. BMC Med. Inform. Decis. Mak. 2023, 23, 176. [Google Scholar] [CrossRef]
- Agarwal, P.; Gordon, D.; Griffith, J.; Kithulegoda, N.; Witteman, H.; Bhatia, R.; Kushniruk, A.; Borycki, E.; Lamothe, L.; Springall, E.; et al. Assessing the quality of mobile applications in chronic disease management: A scoping review. NPJ Digit. Med. 2021, 4, 46. [Google Scholar] [CrossRef]
- Kessel, R.; Wong, B.; Clemens, T.; Brand, H. Digital health literacy as a super determinant of health: More than simply the sum of its parts. Internet Interv. 2022, 27, 100500. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. eHealth. 2022. Available online: https://www.emro.who.int/health-topics/ehealth/ (accessed on 9 June 2025).
- World Health Organization. MHealth: Use of Appropriate Digital Technologies for Public Health. 2018. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_20-en.pdf (accessed on 9 June 2025).
- Lee, H.J.; Son, Y.J. Prevalence and Associated Factors of Frailty and Mortality in Patients with End-Stage Renal Disease Undergoing hemodialysis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3471. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Flythe, J.E.; Watnick, S. Dialysis for Chronic Kidney Failure: A Review. JAMA 2024, 332, 1559–1573. [Google Scholar] [CrossRef] [PubMed]
- Siddique, A.B.; Krebs, M.; Alvarez, S.; Greenspan, I.; Patel, A.; Kinsolving, J.; Koizumi, N. Mobile Apps for the Care Management of Chronic Kidney and End-Stage Renal Diseases: Systematic Search in App Stores and Evaluation. JMIR Mhealth Uhealth 2019, 7, e12604. [Google Scholar] [CrossRef]
- Verweel, L.; Newman, A.; Michaelchuck, W.; Packham, T.; Goldstein, R.; Brooks, D. The effect of digital interventions on related health literacy and skills for individuals living with chronic diseases: A systematic review and meta-analysis. Int. J. Med. Inform. 2023, 177, 105114. [Google Scholar] [CrossRef]
- Aromataris, E.; Lockwood, C.; Porritt, K.; Pilla, B.; Jordan, Z. JBI Manual for Evidence Synthesis. JBI. 2024. Available online: https://synthesismanual.jbi.global (accessed on 9 June 2025). [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Martínez-Olmos, F.J.; Gómez-Conesa, A.A.; García-Testal, A.; Ortega-Pérez-de-Villar, L.; Valtueña-Gimeno, N.; Gil-Gómez, J.A.; Garcia-Maset, R.; Segura-Ortí, E. An intradialytic non-immersive virtual reality exercise programme: A crossover randomized controlled trial. Nephrol. Dial. Transplant. 2022, 37, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Al-Ali, F.; Kang, G.E.; Hamad, A.I.; Ibrahim, R.A.; Talal, T.K.; Najafi, B. Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms. Sensors 2020, 20, 1571. [Google Scholar] [CrossRef]
- Meléndez-Oliva, E.; Sánchez-Romero, E.A.; Segura-Ortí, E.; Gil-Gómez, J.A.; Soto-Goñi, X.A.; Poveda-Pagán, E.J. Effect of a virtual reality Exercise on Patients Undergoing Haemodialysis: A Randomised Controlled Clinical Trial Research Protocol. Int. J. Environ. Res. Public Health 2023, 20, 4116. [Google Scholar] [CrossRef]
- Smyth, W.; McArdle, J.; Body-Dempsey, J.; Manickam, V.; Swinbourne, A.; Lee, I.; Holdsworth, J.; Omonaiye, O.; Nagle, C. Immersive virtual reality in a northern Queensland haemodialysis unit: Study protocol for a cross-over randomized controlled feasibility trial (ACTRN12621000732886). Contemp. Clin. Trials Commun. 2022, 28, 100956. [Google Scholar] [CrossRef] [PubMed]
- Turoń-Skrzypińska, A.; Tomska, N.; Mosiejczuk, H.; Rył, A.; Szylińska, A.; Marchelek-Myśliwiec, M.; Ciechanowski, K.; Nagay, R.; Rotter, I. Impact of virtual reality exercises on anxiety and depression in hemodialysis. Sci. Rep. 2023, 13, 12435. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.; Burrows, B.; Browning, M.H.; Solai, K.; Fast, D.; Litbarg, N.O.; Wilund, K.R.; Moskowitz, J.T. Mindfulness-based virtual reality Intervention in hemodialysis Patients: A Pilot Study on End-user Perceptions and Safety. Kidney360 2021, 2, 435–444. [Google Scholar] [CrossRef]
- Maynard, L.G.; de Menezes, D.L.; Lião, N.S.; de Jesus, E.M.; Andrade, N.L.S.; Santos, J.C.D.; da Silva Júnior, W.M.; Bastos, K.; Barreto Filho, J.A.S. Effects of Exercise Training Combined with virtual reality in Functionality and Health-Related Quality of Life of Patients on hemodialysis. Games Health J. 2019, 8, 339–348. [Google Scholar] [CrossRef]
- Finco, M.G.; Najafi, B.; Zhou, H.; Hamad, A.; Ibrahim, R.; Al-Ali, F. Game-based intradialytic non-weight-bearing exercise training on gait speed and balance in older adults with diabetes: A single-blind randomized controlled trial. Sci. Rep. 2023, 13, 14225. [Google Scholar] [CrossRef]
- García-Testal, A.; Martínez-Olmos, F.J.; Gil-Gómez, J.A.; Villalón-Coca, J.; Ortiz-Ramón, R.; Cana-Poyatos, A.; García-Maset, R.; Segura-Ortí, E. Impact of an intradialysis virtual-reality-based exercise program on healthcare resources expenditure: A micro-costing analysis. BMC Nephrol. 2022, 23, 230. [Google Scholar] [CrossRef]
- Hudson, J.L.; Moss-Morris, R.; Game, D.; Carroll, A.; McCrone, P.; Hotopf, M.; Yardley, L.; Chilcot, J. Improving distress in dialysis (iDiD): A feasibility two-arm parallel randomised controlled trial of an online cognitive behavioural therapy intervention with and without therapist-led telephone support for psychological distress in patients undergoing haemodialysis. BMJ Open 2016, 6, e011286. [Google Scholar] [CrossRef]
- Santana, C.; Freitas, A.; Oliveira Barreto, G.; Sousa De Avelar, I.; Mazaro-Costa, R.; Bueno, G.; Ribeiro, D.; Damasceno Silva, G.; Naghettini, A. Serious Game on a Smartphone for Adolescents Undergoing hemodialysis: Development and Evaluation. JMIR Serious Games 2020, 8, e17979. [Google Scholar] [CrossRef]
- Hayashi, A.; Yamaguchi, S.; Waki, K.; Fujiu, K.; Hanafusa, N.; Nishi, T.; Tomita, H.; Kobayashi, H.; Fujita, H.; Kadowaki, T.; et al. Testing the feasibility and usability of a novel smartphone-based self-management support system for dialysis patients: A pilot study. JMIR Res. Protoc. 2017, 6, e63. [Google Scholar] [CrossRef]
- Hosseini, A.; Jackson, A.C.; Chegini, N.; Dehghan, M.F.; Mazloum, D.; Haghani, S.; Bahramnezhad, F. The effect of an educational app on hemodialysis patients’ self-efficacy and self-care: A quasi-experimental longitudinal study. Chronic Illn. 2023, 19, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.; Yabe, H.; Hibino, T.; Morishita, S.; Watanabe, M.; Nishioka, K.; Ishikawa, H. The study of exercise therapy using a virtual reality system on healthy subjects assuming hospital use and intradialytic exercise. Nagoya J. Med. Sci. 2023, 85, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Li, D. Understanding how virtual reality forest experience promote physiological and psychological health for patients undergoing hemodialysis. Front. Psychiatry 2022, 13, 1007396. [Google Scholar] [CrossRef]
- Bers, M.U.; Gonzalez-Heydrich, J.; Demaso, D.R. Use of a computer-based application in a pediatric hemodialysis unit: A pilot study. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Segura-Ortí, E.; Pérez-Domínguez, B.; Ortega-Pérez de Villar, L.; Meléndez-Oliva, E.; Martínez-Gramage, J.; García-Maset, R.; Gil-Gómez, J.A. Virtual reality exercise intradialysis to improve physical function: A feasibility randomized trial. Scand. J. Med. Sci. Sports 2019, 29, 89–94. [Google Scholar] [CrossRef]
- Feizalahzadeh, H.; Tafreshi, M.Z.; Moghaddasi, H.; Farahani, M.A.; Khosrovshahi, H.T.; Zareh, Z.; Mortazavi, F. Development and validation of a theory-based multimedia application for educating Persian patients on hemodialysis. Comput. Inform. Nurs. 2014, 32, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Agapito, G.; Simeoni, M.; Calabrese, B.; Caré, I.; Lamprinoudi, T.; Guzzi, P.; Pujia, A.; Fuiano, G.; Cannataro, M. DIETOS: A dietary recommender system for chronic diseases monitoring and management. Comput. Methods Programs Biomed. 2018, 153, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Chettati, M.; Bouchemla, N.; Fadili, W.; Laouad, I. Use of the TestObs mobile application for the evaluation of therapeutic adherence in chronic hemodialysis patients: Technological monitoring model of treatment adherence and determining factors. Nephrol. Ther. 2022, 18, 557–564. [Google Scholar] [CrossRef]
- Chiang, Y.; Chang, Y.; Lin, S.; Lin, C.; Hsu, P.; Hsu, Y.; Wu, T. Effects of Individualized Dietary Phosphate Control Program With a Smartphone Application in hemodialysis Patients in Taiwan. Biol. Res. Nurs. 2021, 23, 375–381. [Google Scholar] [CrossRef]
- Cho, H.; Sohng, K. The effect of a virtual reality exercise program on physical fitness, body composition, and fatigue in hemodialysis patients. J. Phys. Ther. Sci. 2014, 26, 1661–1665. [Google Scholar] [CrossRef]
- Chou, H.; Chen, S.; Yen, T.; Han, H. Effect of a virtual reality-Based Exercise Program on Fatigue in Hospitalized Taiwanese End-Stage Renal Disease Patients Undergoing hemodialysis. Clin. Nurs. Res. 2020, 29, 368–374. [Google Scholar] [CrossRef]
- Connelly, K.; Siek, K.; Chaudry, B.; Jones, J.; Astroth, K.; Welch, J. An offline mobile nutrition monitoring intervention for varying-literacy patients receiving hemodialysis: A pilot study examining usage and usability. J. Am. Med. Inform. Assoc. 2012, 19, 705–712. [Google Scholar] [CrossRef]
- Costa, F.; Delage, P.; Santana, M.; Nascimento, M.; Teixeira, E. Alfa test of a gamified technology for children and adolescents in hemodialysis. Anna Nery Sch. J. Nurs. Esc. Anna Nery Rev. Enferm. 2021, 25, e20200514. [Google Scholar] [CrossRef]
- Dingwall, K.; Sweet, M.; Cass, A.; Hughes, J.; Kavanagh, D.; Howard, K.; Barzi, F.; Brown, S.; Sajiv, C.; Majoni, S.; et al. Effectiveness of Wellbeing Intervention for Chronic Kidney Disease (WICKD): Results of a randomised controlled trial. BMC Nephrol. 2021, 22, 136. [Google Scholar] [CrossRef]
- Khoury, C.; Crutzen, R.; Schols, J.; Halfens, R.; Karavetian, M. A Dietary Mobile App for Patients Undergoing hemodialysis: Prospective Pilot Study to Improve Dietary Intakes. J. Med. Internet Res. 2020, 22, e17817. [Google Scholar] [CrossRef]
- Hernandez, R.; Wilund, K.; Solai, K.; Tamayo, D.; Fast, D.; Venkatesan, P.; Lash, J.; Lora, C.; Martinez, L.; Alemañy, G.; et al. Positive Psychological Intervention Delivered Using virtual reality in Patients on hemodialysis with Comorbid Depression: Protocol and Design for the Joviality Randomized Controlled Trial. JMIR Res. Protoc. 2023, 12, e45100. [Google Scholar] [CrossRef]
- Min, Y.; Park, M. Effects of a Mobile-App-Based Self-Management Support Program For Elderly hemodialysis Patients. Healthc. Inform. Res. 2020, 26, 93–103. [Google Scholar] [CrossRef]
- Minatodani, D.; Berman, S. Home telehealth in high-risk dialysis patients: A 3-year study. Telemed. e-Health 2013, 19, 520–522. [Google Scholar] [CrossRef]
- Ong, S.; Jassal, S.; Miller, J.; Porter, E.; Cafazzo, J.; Seto, E.; Thorpe, K.; Logan, A. Integrating a Smartphone-Based Self-Management System into Usual Care of Advanced CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 1054–1062. [Google Scholar] [CrossRef]
- Pack, S.; Lee, J. Randomised controlled trial of a smartphone application-based dietary self-management program on haemodialysis patients. J. Clin. Nurs. 2021, 30, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Park, O.; Kim, S. Integrated self-management program effects on hemodialysis patients: A quasi-experimental study. Jpn. J. Nurs. Sci. 2019, 16, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Ren, Q.; Lian, M.; Liu, Y.; Thomas-Hawkins, C.; Zhu, L.; Shen, Q. Effects of a transtheoretical model-based WeChat health education programme on self-management among haemodialysis patients: A longitudinal experimental intervention study. J. Adv. Nurs. 2019, 75, 3554–3565. [Google Scholar] [CrossRef] [PubMed]
- Rocco, M.; Rigaud, M.; Ertel, C.; Russell, G.; Zemdegs, J.; Vecchio, M. Fluid Intake Management in Maintenance hemodialysis Using a Smartphone-Based Application: A Pilot Study. Kidney Med. 2023, 5, 100703. [Google Scholar] [CrossRef] [PubMed]
- Saadatifar, B.; Sharifi, S.; Faghihi, H.; Googhary, N. Effect of mHealth Training on Treatment Adherence in hemodialysis Patients. Med. Surg. Nurs. J. 2022, 11, e134851. [Google Scholar] [CrossRef]
- Teong, L.; Khor, B.; Ng, H.; Sahathevan, S.; Purba, K.; Narayanan, S.; Gafor, A.; Goh, B.; Bee, B.; Yahya, R.; et al. Effectiveness of a Nutritional Mobile Application for Management of Hyperphosphatemia in Patients on hemodialysis: A Multicenter Open-Label Randomized Clinical Trial. J. Pers. Med. 2022, 12, 961. [Google Scholar] [CrossRef]
- Khah, M.; Farsi, Z.; Sajadi, S. Comparing the effects of mHealth application based on micro-learning method and face-to-face training on treatment adherence and perception in haemodialysis patients: A randomised clinical trial. BMJ Open 2023, 13, e071982. [Google Scholar] [CrossRef] [PubMed]
- Willis, M.; Hein, L.; Hu, Z.; Saran, R.; Argentina, M.; Bragg-Gresham, J.; Krein, S.; Gillespie, B.; Zheng, K.; Veinot, T. Usability evaluation of a tablet-based intervention to prevent intradialytic hypotension in dialysis patients during in-clinic dialysis: Mixed methods study. JMIR Hum. Factors 2021, 8, e26012. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Kosa, S.; Monize, J.; D’Souza, M. Nutritional Mobile APPlications for CKD Patients: Systematic Review. Kidney Int. Rep. 2018, 4, 399–407. [Google Scholar] [CrossRef]
- Russell, C.; Zigan, C.; Wozniak, K.; Soni, K.; Gallant, K.; Friedman, A. A Systematic Review and Qualitative Analysis of Existing Dietary Mobile Applications for People With Chronic Kidney Disease. J. Ren. Nutr. 2022, 32, 382–388. [Google Scholar] [CrossRef]
- Stevenson, J.K.; Campbell, Z.C.; Webster, A.C. E-Health interventions for people with chronic kidney disease. Cochrane Database Syst. Rev. 2019, 8, CD012379. [Google Scholar] [CrossRef]
- Campbell, J.; Porter, J. Dietary mobile apps and their effect on nutritional indicators in chronic renal disease: A systematic review. Nephrology 2015, 20, 744–751. [Google Scholar] [CrossRef]
- Chen, J.F.; Wu, L.L.; Chou, S.C. Effects of Journaling Dietary Intake App on the Health Outcomes of Chronic Kidney Disease Stage 3B-5. In Proceedings of the 2016 49th Hawaii International Conference on System Sciences, Koloa, HI, USA, 5–8 January 2016; pp. 3379–3388. [Google Scholar] [CrossRef]
- Shen, H. Electronic Health Self-Management Interventions for Patients With Chronic Kidney Disease: Systematic Review of Quantitative and Qualitative Evidence. J. Med. Internet Res. 2019, 21, e12384. [Google Scholar] [CrossRef] [PubMed]
- Ventura, S.; Brivio, E.; Riva, G.; Baños, R.M. Immersive versus non-immersive experience: Exploring the feasibility of memory assessment through 360° technology. Front. Psychol. 2019, 10, 2509. [Google Scholar] [CrossRef]
- Burrai, F.; Othman, S.; Brioni, E.; Silingardi, M.; Micheluzzi, V.; Luppi, M.; Apuzzo, L.; La Manna, G. Virtual reality in dialysis: A new perspective on care. J. Ren. Care 2018, 44, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, C.S.; Magalhães, B.; Gomes, J.A.; Santos, C. Exergames to improve Rehabilitation after Anterior Cruciate Ligament Injury: Systematic review and GRADE evidence synthesis. Int. J. Orthop. Trauma Nurs. 2022, 44, 100917. [Google Scholar] [CrossRef] [PubMed]
- Perez, F.M.; Henrique, P.P.; Marchi, A.C. Kinesiotherapeutic intervention protocol with exergames for muscle strength and balance in elderly—A systematic literature review. Res. Soc. Dev. 2021, 10, e113101321063. [Google Scholar] [CrossRef]
- Hu, H.; Liu, X.; Chau, P.H.; Choi, E.P.H. Effects of intradialytic exercise on health-related quality of life in patients undergoing maintenance haemodialysis: A systematic review and meta-analysis. Qual. Life Res. 2022, 31, 1915–1932. [Google Scholar] [CrossRef]
- Sabate, E. Adherence to Long-Term Therapies: Evidence for Action; Report of WHO Adherence to Longterm Therapies Project; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Martins, A.R.; Ferreira, M.C.; Fernandes, C.S. Emerging technologies for supporting patients during hemodialysis: A scoping review. Int. J. Med. Inform. 2024, 181, 105664. [Google Scholar] [CrossRef]
- Shahgholian, N.; Yousefi, H. The lived experiences of patients undergoing hemodialysis with the concept of care: A phenomenological study. BMC Nephrol. 2018, 19, 338. [Google Scholar] [CrossRef] [PubMed]
- Sukartini, T.; Efendi, F.; Putri, N.S. A phenomenological study to explore patient experience of fluid and dietary restrictions imposed by hemodialysis. J. Vasc. Nurs. 2022, 40, 105–111. [Google Scholar] [CrossRef]
- Kim, S.; Lee, H.Z. The lived self-care experiences of patients undergoing long-term haemodialysis: A phenomenological study. Int. J. Environ. Res. Public Health 2023, 20, 4690. [Google Scholar] [CrossRef]
- Murali, K.M.; Mullan, J.; Roodenrys, S.; Hassan, H.C.; Lambert, K.; Lonergan, M. Strategies to improve dietary, fluid, dialysis or medication adherence in patients with end stage kidney disease on dialysis: A systematic review and meta-analysis of randomized intervention trials. PLoS ONE 2019, 14, e0211479. [Google Scholar] [CrossRef] [PubMed]
- Bonner, A.; Gillespie, K.; Campbell, K.L.; Corones-Watkins, K.; Hayes, B.; Harvie, B.; Kelly, J.T.; Havas, K. Evaluating the prevalence and opportunity for technology use in chronic kidney disease patients: A cross-sectional study. BMC Nephrol. 2018, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Sobrinho, A.; da Silva, L.D.; Perkusich, A.; Pinheiro, M.; Cunha, P. Design and evaluation of a mobile application to assist the self-monitoring of the chronic kidney disease in developing countries. BMC Med. Inform. Decis. Mak. 2018, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Gulliksen, J.; Göransson, B.; Boivie, I.; Blomkvist, S.; Persson, J.; Cajander, A. Key principles for user-centred systems design. Behav. Inf. Technol. 2003, 22, 397–409. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).