
Impact of Physical Exercise on Quality of Life, Self-Esteem, and Depression in Breast Cancer Survivors: A Pilot Study


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Exercise Intervention
2.3. Participants
2.4. Measurements
- -
- Beck Depression Inventory:
- -
- Rosenberg Self-Esteem Scale (RSE):
- -
- Supplementary Questionnaire Breast Cancer Module (EORTC QLQ-BR23):
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oei, S.L.; Thronicke, A.; Matthes, H.; Schad, F. Assessment of integrative non-pharmacological interventions and quality of life in breast cancer patients using real-world data. Breast Cancer 2021, 28, 608–617. [Google Scholar] [CrossRef]
- Bruce, J.; Mazuquin, B.; Mistry, P.; Rees, S.; Canaway, A.; Hossain, A.; Williamson, E.; Padfield, E.J.; Lall, R.; Richmond, H.; et al. Exercise to prevent shoulder problems after breast cancer surgery: The PROSPER RCT. Health Technol. Assess. 2022, 26, 1–124. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Andrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K.; et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention. CA Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Zopf, E.M.; Zhang, X.; Schmitz, K.H. The Impact of Exercise on Cancer Mortality, Recurrence, and Treatment-Related Adverse Effects. Epidemiol. Rev. 2017, 39, 71–92. [Google Scholar] [CrossRef]
- Gilchrist, S.C.; Howard, V.J.; Akinyemiju, T.; Judd, S.E.; Cushman, M.; Hooker, S.P.; Diaz, K.M. Association of Sedentary Behavior With Cancer Mortality in Middle-aged and Older US Adults. JAMA Oncol. 2020, 6, 1210–1217. [Google Scholar] [CrossRef]
- Baumann, F.T.; Bieck, O.; Oberste, M.; Kuhn, R.; Schmitt, J.; Wentrock, S.; Zopf, E.; Bloch, W.; Schüle, K.; Reuss-Borst, M. Sustainable impact of an individualized exercise program on physical activity level and fatigue syndrome on breast cancer patients in two German rehabilitation centers. Support. Care Cancer 2016, 25, 1047–1054. [Google Scholar] [CrossRef]
- Leclerc, A.F.; Foidart-Dessalle, M.; Tomasella, M.; Coucke, P.; Devos, M.; Bruyère, O.; Bury, T.; Deflandre, D.; Jerusalem, G.; Lifrange, E.; et al. Multidisciplinary Rehabilitation Program after Breast Cancer: Benefits on Physical Function, Anthropometry and Quality of Life. Eur. J. Phys. Rehabil. Med. 2017, 53, 633–642. [Google Scholar] [CrossRef]
- Paulo, T.R.; Rossi, F.E.; Viezel, J.; Tosello, G.T.; Seidinger, S.C.; Simões, R.R.; De Freitas, R.; Freitas, I.F. The impact of an exercise program on quality of life in older breast cancer survivors undergoing aromatase inhibitor therapy: A randomized controlled trial. Health Qual. Life Outcomes 2019, 17, 17. [Google Scholar] [CrossRef]
- Wirtz, P.; Baumann, F.T. Physical Activity, Exercise and Breast Cancer—What Is the Evidence for Rehabilitation, Aftercare, and Survival? A Review. BRC 2018, 13, 92–100. [Google Scholar] [CrossRef]
- Dolan, L.B.; Barry, D.; Petrella, T.; Davey, L.; Minnes, A.; Yantzi, A.; Marzolini, S.; Oh, P. The Cardiac Rehabilitation Model Improves Fitness, Quality of Life, and Depression in Breast Cancer Survivors. J. Cardiopulm. Rehabil. Prev. 2018, 38, 246–252. [Google Scholar] [CrossRef]
- Dieli-Conwright, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Sami, N.; Lee, K.; Sweeney, F.C.; Stewart, C.; Buchanan, T.A.; Spicer, D.; Tripathy, D.; et al. Aerobic and resistance exercise improves physical fitness, bone health, and quality of life in overweight and obese breast cancer survivors: A randomized controlled trial. Breast Cancer Res. 2018, 20, 124. [Google Scholar] [CrossRef]
- Blount, D.S.; McDonough, D.J.; Gao, Z. Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review. J. Clin. Med. 2021, 10, 2015. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Pekarek, L.; Guijarro, L.G.; Castellanos, A.J.; Sanchez-Trujillo, L.; García-Honduvilla, N.; Álvarez-Mon, M.; Buján, J.; et al. Physical Activity as an Imperative Support in Breast Cancer Management. Cancers 2021, 13, 55. [Google Scholar] [CrossRef]
- Liska, T.M.; Kolen, A.M. The role of physical activity in cancer survivors’ quality of life. Health Qual. Life Outcomes 2020, 18, 197. [Google Scholar] [CrossRef] [PubMed]
- del-Rosal-Jurado, A.; Romero-Galisteo, R.; Trinidad-Fernández, M.; González-Sánchez, M.; Cuesta-Vargas, A.; Ruiz-Muñoz, M. Therapeutic Physical Exercise Post-Treatment in Breast Cancer: A Systematic Review of Clinical Practice Guidelines. J. Clin. Med. 2020, 9, 1239. [Google Scholar] [CrossRef] [PubMed]
- García-Chico, C.; López-Ortiz, S.; Peñín-Grandes, S.; Pinto-Fraga, J.; Valenzuela, P.L.; Emanuele, E.; Ceci, C.; Graziani, G.; Fiuza-Luces, C.; Lista, S.; et al. Physical Exercise and the Hallmarks of Breast Cancer: A Narrative Review. Cancers 2023, 15, 324. [Google Scholar] [CrossRef]
- Zagalaz-Anula, N.; Mora-Rubio, M.J.; Obrero-Gaitán, E.; Del-Pino-Casado, R. Recreational physical activity reduces breast cancer recurrence in female survivors of breast cancer: A meta-analysis. Eur. J. Oncol. Nurs. 2022, 59, 102162. [Google Scholar] [CrossRef]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of Community-Based Research: Assessing Partnership Approaches to Improve Public Health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Lippincott, Williams & Wilkins: Baltimore, MD, USA, 2010; pp. 228–232. ISBN 9780781769020. [Google Scholar]
- Blanchard, C.M.; Courneya, K.S.; Stein, K. American cancer society’s SCS II. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef]
- Ballard-Barbash, R.; George, S.; Alfano, C.; Schmitz, K. Physical activity across the cancer continuum. Oncology 2013, 27, 589–592. [Google Scholar]
- Courneya, K.S.; Mackey, J.R.; McKenzie, D.C. Exercise for breast cancer survivors: Research evidence and clinical guidelines. Physician Sportsmed. 2002, 30, 33–42. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Vaz Serra, A.S.; Abreu, J.L. Aferição dos quadros clínicos depressivos: Ensaio de aplicação do inventário depressivo de Beck a uma amostra portuguesa de doentes deprimidos. Sep. Coimbra Méd. 1973, 20, 623–644. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Garbin, M.G. Psychometric properties of the beck depression inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Santos, P.J. Validação da Rosenberg Self-Esteem Scale Numa Amostra de Estudantes do Ensino Superior; III Conferência Internacional Avaliação Psicológica; Formas e Contextos: Braga, Portugal, 2008. [Google Scholar]
- Rosenberg, M. Conceiving the Self; Basic Books: New York, NY, USA, 1979. [Google Scholar]
- Fayers, P.M.; Aaraonson, N.; Bjordal, K.; Curran, D.; Groevold, M. EORTC QLQ-C30. In Scoring Manual, 2nd ed.; European Organization for Research and Treatment of Cancer Quality of Life Study Group: Brussels, Portugal, 1999. [Google Scholar]
- Pestana, M.; Gageiro, L. Análise de Dados para Ciências Sociais. In A Complementaridade Do SPSS, 5th ed.; Edições Silabo: Lisboa, Portugal, 2005. [Google Scholar]
- Courneya, K.S.; Segal, R.J.; Mackey, J.R.; Gelmon, K.; Reid, R.D.; Friedenreich, C.M.; McKenzie, D.C. Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. J. Clin. Oncol. 2007, 25, 4396–4404. [Google Scholar] [CrossRef] [PubMed]
- Valenti, M.; Porzio, G.; Aielli, F.; Verna, L.; Cannita, K.; Manno, R.; Masedu, F.; Marchetti, P.; Ficorella, C. Physical exercise and quality of life in breast cancer survivors. Int. J. Sci. 2008, 5, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Pinto, B.M.; Frierson, G.M.; Rabin, C.; Trunzo, J.J.; Marcus, B.H. Home-based physical activity intervention for breast cancer patients. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 3577–3587. [Google Scholar] [CrossRef]
- Sprod, L.K.; Hsieh, C.C.; Hayward, R.; Schneider, C.M. Three versus Six Months of Exercise Training in Breast Cancer Survivors. Breast Cancer Res. Treat. 2010, 121, 413–419. [Google Scholar] [CrossRef]
- Steindorf, K.; Schmidt, M.E.; Klassen, O.; Ulrich, C.M.; Oelmann, J.; Habermann, N.; Potthoff, K. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: Results on cancer-related fatigue and quality of life. Ann. Oncol. 2014, 25, 2237–2243. [Google Scholar] [CrossRef]
- Burgess, C.; Cornelius, V.; Love, S.; Graham j Richards, M.; Ramirez, A. Depression and anxiety in women with early breast cancer: Five-year observational cohort study. BMJ 2005, 330, 702. [Google Scholar] [CrossRef]
- Krebber, A.M.; Buffart, L.M.; Kleijn, G.; Riepma, I.C.; De Bree, R.; Leemans, C.R.; Becker, A.; Brug, J.; Van Straten, A.; Cuijpers, P.; et al. Prevalence of depression in cancer patients: A meta- analysis of diagnostic interviews and self-report instruments. Psycho-Oncol. 2014, 23, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.I.; Scherer, R.W.; Geigle, P.M.; Berlanstein, T.O.; Gotay, C.C.; Snyder, C. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database Syst. Rev. 2012, 15, CD007566. [Google Scholar]
- Travier, N.; Velthuis, M.J.; Steins Bisschop, C.N.; van den Buijs, B.; Monninkhof, E.M.; Backx, F.; Los, M.; Erdkamp, F.; Bloemendal, H.J.; Rodenhuis, C.; et al. Effects of an 18-week exercise programme started early during breast cancer treatment: A randomised controlled trial. BMC Med. 2015, 13, 121. [Google Scholar] [CrossRef]
- Ramos, A.S.; Patrão, I. Imagem corporal da mulher com cancro de mama: Impacto na qualidade do relacionamento conjugal e na satisfação sexual. Anál. Psicol. 2005, 3, 295–304. [Google Scholar] [CrossRef]
- Shobeiri, F.; Masoumi, S.Z.; Nikravesh, A.; Moghadam, R.H.; Karami, M. The impact of aerobic exercise on quality of life in women with breast cancer: A randomized controlled trial. J. Res. Health Sci. 2016, 16, 127–132. [Google Scholar]
- Remondes-Costa, S.; Jimenéz, F.; Pais-Ribeiro, J. Imagem corporal, sexualidade e qualidade de vida no cancro da mama. Psicol. Saúde Doenças 2012, 13, 327–339. [Google Scholar]
- Pinto, B.M.; Clark, M.M.; Maruyama, N.C.; Feder, S.I. Psychological and fitness changes associated with exercise participation among women with breast cancer. Psycho-Oncol. 2003, 12, 118–126. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Ligibel, J. Lifestyle factors in cancer survivorship. JCO 2012, 30, 3697–3704. [Google Scholar] [CrossRef]
- Hayes, S.; Spence, R.R.; Galvão, D.; Newton, R. Australian association for exercise and sport science position stand: Optimizing cancer outcomes through exercise. J. Sci. Med. Sport 2009, 12, 428–434. [Google Scholar] [CrossRef]
- Vallance, J.; Courneya, K.; Plotnikoff, R.; Mackey, J. Analyzing theoretical mechanisms of physical activity behavior change in breast cancer surviviors: Results from the activity promotion (action) trail. Ann. Behav. Med. 2008, 35, 150–158. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Pre-Test (n = 13) | Post-Test (n = 13) | Mean Difference ± SD | p | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
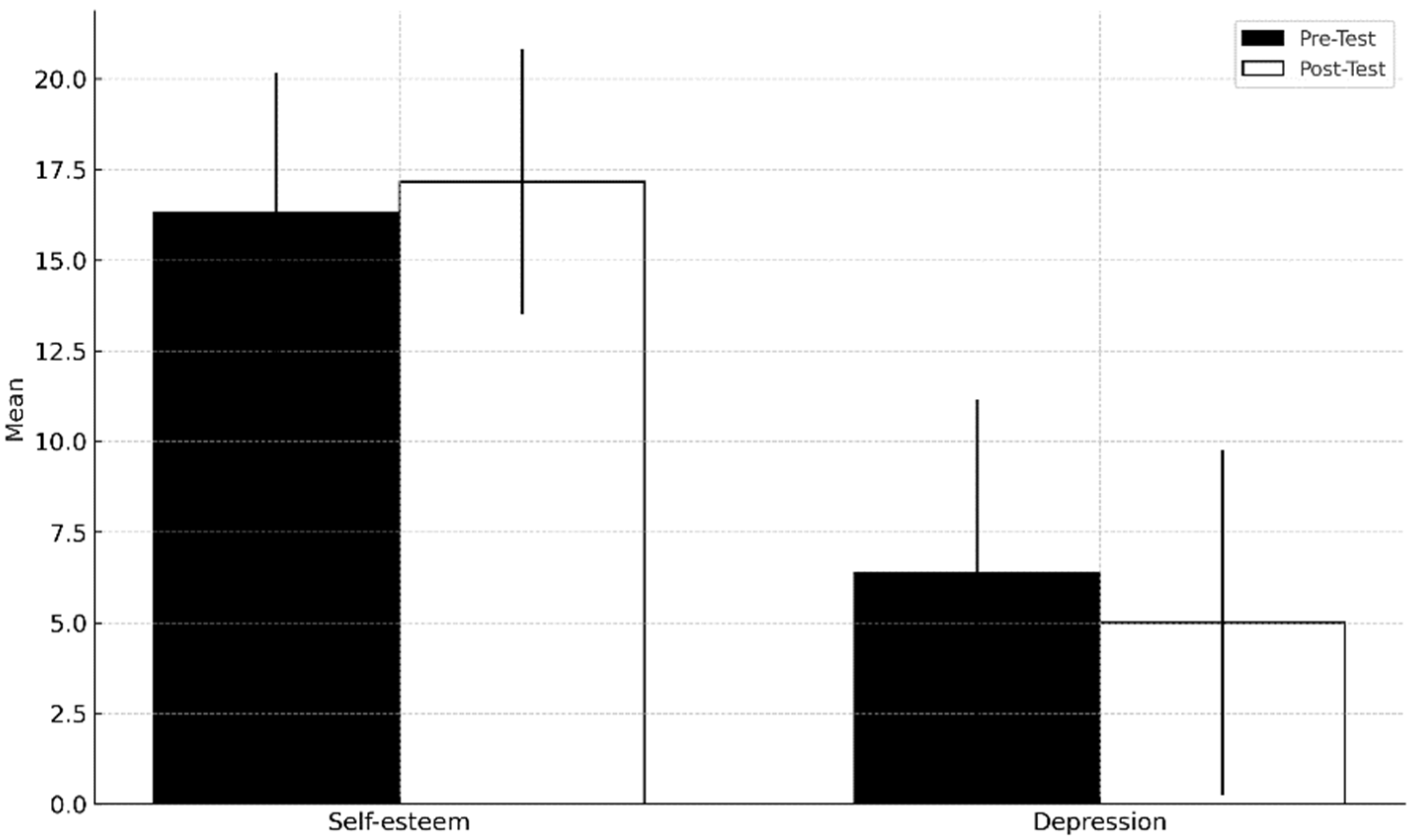
| Self-esteem | 16.31 | ±3.86 | 17.16 | ±3.67 | 0.85 ± 0.52 | 0.004 * |
| Depression | 6.39 | ±4.75 | 5.00 | ±4.75 | −1.39 ± 1.29 | 0.080 |
| Pre-Test (n = 13) | Post-Test (n = 13) | Mean Difference ± SD | p | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Functional Scale | ||||||
| -Body image | 1.23 | ±0.37 | 1.31 | ±0.74 | 0.08 ± 0.37 | 0.746 |
| -Sexual function | 1.65 | ±0.88 | 1.73 | ±0.90 | 0.08 ± 0.32 | 0.436 |
| -Sexual pleasure | 2.33 | ±1.12 | 2.10 | ±1.10 | −0.23 ± 0.42 | 0.436 |
| -Future health prospect | 2.69 | ±1.11 | 2.15 | ±0.80 | −0.54 ± 0.31 | 0.047 * |
| Symptom Scale | ||||||
| -Chemotherapy Side-Effects | 1.55 | ±0.52 | 1.45 | ±0.38 | −0.10 ± 0.20 | 0.324 |
| -Breast symptoms | 1.38 | ±0.40 | 1.19 | ±0.23 | −0.19 ± 0.27 | 0.127 |
| -Arm symptoms | 1.87 | ±0.73 | 1.49 | ±0.48 | −0.38 ± 0.35 | 0.015 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, E.M.R.T.d.C.; Mendes, H.I.A.; Varajidás, C.A.; Fonseca, S.C.F. Impact of Physical Exercise on Quality of Life, Self-Esteem, and Depression in Breast Cancer Survivors: A Pilot Study. Onco 2024, 4, 207-216. https://doi.org/10.3390/onco4030015
Coelho EMRTdC, Mendes HIA, Varajidás CA, Fonseca SCF. Impact of Physical Exercise on Quality of Life, Self-Esteem, and Depression in Breast Cancer Survivors: A Pilot Study. Onco. 2024; 4(3):207-216. https://doi.org/10.3390/onco4030015
Chicago/Turabian StyleCoelho, Eduarda Maria Rocha Teles de Castro, Helena Isabel Azevedo Mendes, Carla Afonso Varajidás, and Sandra Celina Fernandes Fonseca. 2024. "Impact of Physical Exercise on Quality of Life, Self-Esteem, and Depression in Breast Cancer Survivors: A Pilot Study" Onco 4, no. 3: 207-216. https://doi.org/10.3390/onco4030015
APA StyleCoelho, E. M. R. T. d. C., Mendes, H. I. A., Varajidás, C. A., & Fonseca, S. C. F. (2024). Impact of Physical Exercise on Quality of Life, Self-Esteem, and Depression in Breast Cancer Survivors: A Pilot Study. Onco, 4(3), 207-216. https://doi.org/10.3390/onco4030015