
Silicon-, Silica-, and Silicate-Toothpastes for Remineralization and Repair of Teeth: A Scoping Review

 , , ,
, , ,  and
and
Abstract
1. Introduction
1.1. Enamel Regeneration or Repair: Background and Definitions
1.2. Silicon, Silica, and Silicate Toothpastes
1.3. Rationale for the Review—Guiding Question
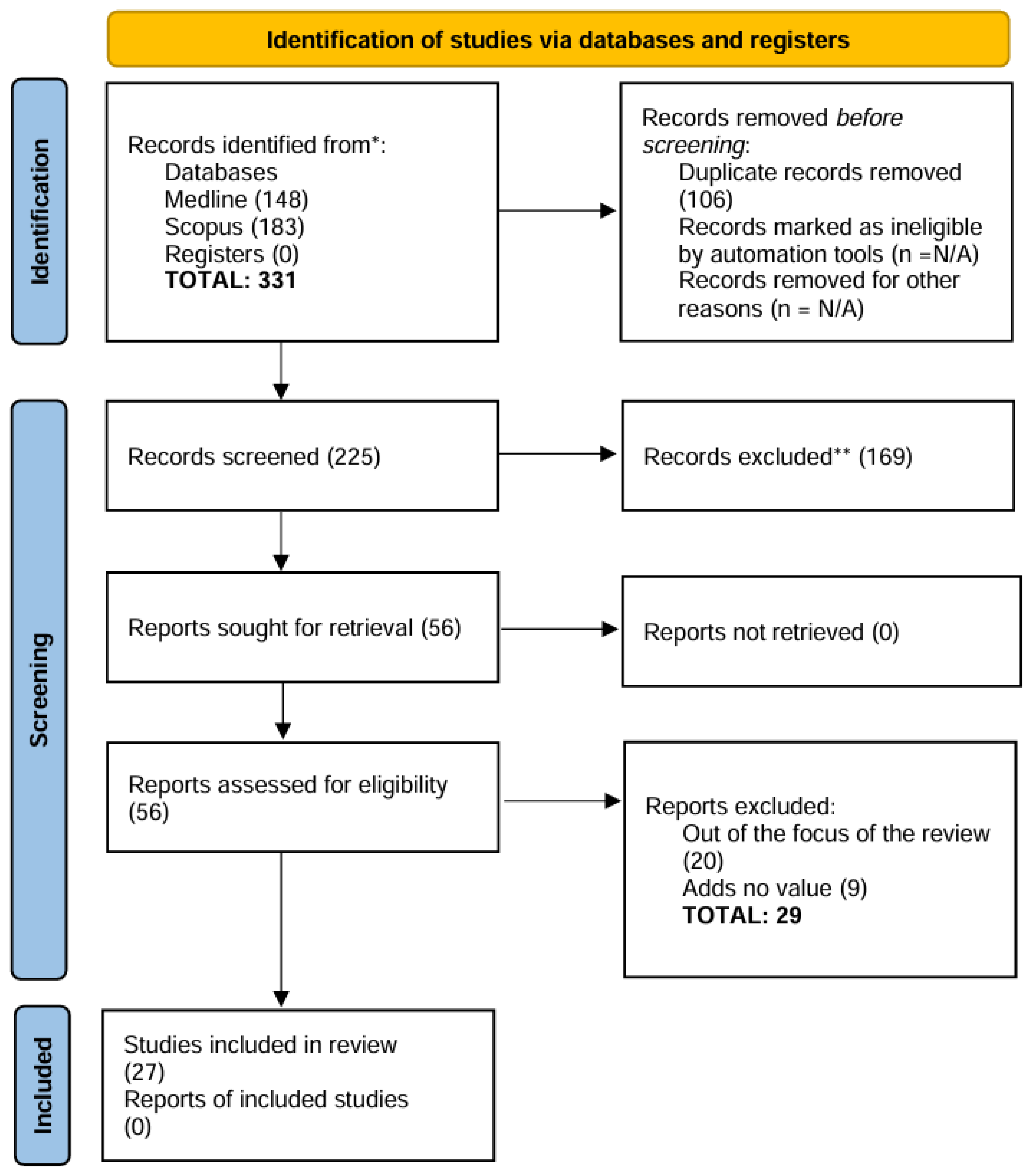
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M. Enhancing fluoride: Clinical human studies of alternatives or boosters for caries management. Caries Res. 2016, 50 (Suppl. S1), 22–37. [Google Scholar] [CrossRef]
- Sampaio, F.C.; Bonecker, M.; Paiva, S.M.; Martignon, S.; Ricomini Filho, A.P.; Pozos-Guillen, A.; Oliveira, B.H.; Bullen, M.; Naidu, R.; Guarnizo-Herreno, C.; et al. Dental caries prevalence, prospects, and challenges for Latin America and Caribbean countries: A summary and final recommendations from a Regional Consensus. Braz. Oral Res. 2021, 35, e056. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.L.S.; Silva, J.; de Sousa, E.B.G.; D’Alpino, P.H.P.; de Oliveira, A.F.B.; de Jong, E.J.; Sampaio, F.C. Effectiveness of fluoride-containing toothpastes associated with different technologies to remineralize enamel after pH cycling: An in vitro study. BMC Oral Health 2022, 22, 489. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.S.; Patel, A.N.; Al Botros, R.; Snowden, M.E.; McKelvey, K.; Unwin, P.R.; Ashcroft, A.T.; Carvell, M.; Joiner, A.; Peruffo, M. Measurement of the efficacy of calcium silicate for the protection and repair of dental enamel. J. Dent. 2014, 42 (Suppl. S1), S21–S29. [Google Scholar] [CrossRef] [PubMed]
- Joiner, A.; Schäfer, F.; Naeeni, M.M.; Gupta, A.K.; Zero, D.T. Remineralisation effect of a dual-phase calcium silicate/phosphate gel combined with calcium silicate/phosphate toothpaste on acid-challenged enamel in situ. J. Dent. 2014, 42, S53–S59. [Google Scholar] [CrossRef] [PubMed]
- Vilhena, F.V.; Grecco, S.D.S.; Gonzalez, A.H.M.; D’Alpino, P.H.P. Regenerative and protective effects on dental tissues of a fluoride-silicon-rich toothpaste associated with a calcium booster: An in vitro study. Dent. J. 2023, 11, 153. [Google Scholar] [CrossRef]
- Pandya, M.; Diekwisch, T.G.H. Enamel biomimetics-fiction or future of dentistry. Int. J. Oral Sci. 2019, 11, 8. [Google Scholar] [CrossRef]
- Philip, N. State of the art enamel remineralization systems: The next frontier in caries management. Caries Res. 2019, 53, 284–295. [Google Scholar] [CrossRef]
- Seong, J.; Newcombe, R.G.; Matheson, J.R.; Weddell, L.; Edwards, M.; West, N.X. A randomised controlled trial investigating efficacy of a novel toothpaste containing calcium silicate and sodium phosphate in dentine hypersensitivity pain reduction compared to a fluoride control toothpaste. J. Dent. 2020, 98, 103320. [Google Scholar] [CrossRef]
- Meyer, F.; Amaechi, B.T.; Fabritius, H.O.; Enax, J. Overview of calcium phosphates used in biomimetic oral care. Open Dent. J. 2018, 12, 406–423. [Google Scholar] [CrossRef] [PubMed]
- Vilhena, F.V.; de Oliveira, S.M.L.; Matochek, M.H.M.; Tomaz, P.L.S.; Oliveira, T.S.; D’Alpino, P.H.P. Biomimetic Mechanism of Action of Fluoridated Toothpaste Containing Proprietary REFIX Technology on the Remineralization and Repair of Demineralized Dental Tissues: An In Vitro Study. Eur. J. Dent. 2021, 15, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Regí, M.; Arcos, D. Silicon substituted hydroxyapatites. A method to upgrade calcium phosphate based implants. J. Mater. Chem. 2005, 15, 1509–1516. [Google Scholar] [CrossRef]
- Ten Cate, J.M.; Buzalaf, M.A.R. Fluoride Mode of Action: Once There Was an Observant Dentist. J. Dent. Res. 2019, 98, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Gibson, I.R.; Huang, J.; Best, S.M.; Bonfield, W. Enhanced in vitro cell activity and surface apatite layer formation on novel silicon-substituted hydroxyapatites. In Proceedings of the 12th International Symposium on Ceramics in Medicine, Nam, Japan, 8–11 October 1999. [Google Scholar]
- Patel, N.; Best, S.M.; Bonfield, W.; Gibson, I.R.; Hing, K.A.; Damien, E.; Revell, P.A. A comparative study on the in vivo behavior of hydroxyapatite and silicon substituted hydroxyapatite granules. J. Mater. Sci. Mater. Med. 2002, 13, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Luhrs, A.K.; Geurtsen, W. The application of silicon and silicates in dentistry: A review. Prog. Mol. Subcell. Biol. 2009, 47, 359–380. [Google Scholar] [CrossRef]
- Lippert, F. An introduction to toothpaste—Its purpose, history and ingredients. Monogr. Oral Sci. 2013, 23, 1–14. [Google Scholar] [CrossRef]
- Thalakiriyawa, D.S.; Dissanayaka, W.L. Advances in Regenerative Dentistry Approaches: An Update. Int. Dent. J. 2024, 74, 25–34. [Google Scholar] [CrossRef]
- Luo, X.; Niu, J.; Su, G.; Zhou, L.; Zhang, X.; Liu, Y.; Wang, Q.; Sun, N. Research progress of biomimetic materials in oral medicine. J. Biol. Eng. 2023, 17, 72. [Google Scholar] [CrossRef]
- Volponi, A.A.; Zaugg, L.K.; Neves, V.; Liu, Y.; Sharpe, P.T. Tooth repair and regeneration. Curr. Oral Health Rep. 2018, 5, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Mann, S. The biomimetics of enamel: A paradigm for organized biomaterials synthesis. Ciba Found. Symp. 1997, 205, 261–269; discussion 269–274. [Google Scholar] [PubMed]
- Palmer, L.C.; Newcomb, C.J.; Kaltz, S.R.; Spoerke, E.D.; Stupp, S.I. Biomimetic systems for hydroxyapatite mineralization inspired by bone and enamel. Chem. Rev. 2008, 108, 4754–4783. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Yoon, M.; Choi, K.Y. Approaches for Regenerative Healing of Cutaneous Wound with an Emphasis on Strategies Activating the Wnt/beta-Catenin Pathway. Adv. Wound Care 2022, 11, 70–86. [Google Scholar] [CrossRef] [PubMed]
- Braga, R.R.; Habelitz, S. Current developments on enamel and dentin remineralization. Curr. Oral Health Rep. 2019, 6, 257–263. [Google Scholar] [CrossRef]
- Moradian-Oldak, J.; George, A. Biomineralization of Enamel and Dentin Mediated by Matrix Proteins. J. Dent. Res. 2021, 100, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Veis, A. Phosphorylated proteins and control over apatite nucleation, crystal growth, and inhibition. Chem. Rev. 2008, 108, 4670–4693. [Google Scholar] [CrossRef]
- Moradian-Oldak, J. Protein-mediated enamel mineralization. Front. Biosci. 2012, 17, 1996–2023. [Google Scholar] [CrossRef]
- Singer, L.; Fouda, A.; Bourauel, C. Biomimetic approaches and materials in restorative and regenerative dentistry: Review article. BMC Oral Health 2023, 23, 105. [Google Scholar] [CrossRef] [PubMed]
- Devadiga, D.; Shetty, P.; Hegde, M.N.; Reddy, U. Bioactive remineralization of dentin surface with calcium phosphate-based agents: An in vitro analysis. J. Conserv. Dent. JCD 2022, 25, 93–97. [Google Scholar] [CrossRef]
- Darvell, B.W.; Smith, A.J. Inert to bioactive—A multidimensional spectrum. Dent. Mater. 2022, 38, 2–6. [Google Scholar] [CrossRef]
- Hulbert, S.F.; Hench, L.L.; Forbers, D.; Bowman, L.S. History of bioceramics. Ceram. Int. 1982, 8, 131–140. [Google Scholar] [CrossRef]
- Al-Harbi, N.; Mohammed, H.; Al-Hadeethi, Y.; Bakry, A.S.; Umar, A.; Hussein, M.A.; Abbassy, M.A.; Vaidya, K.G.; Al Berakdar, G.; Mkawi, E.M.; et al. Silica-Based Bioactive Glasses and Their Applications in Hard Tissue Regeneration: A Review. Pharmaceuticals 2021, 14, 75. [Google Scholar] [CrossRef]
- Prasad, P.S.; Pasha, M.B.; Rao, R.N.; Rao, P.V.; Madaboosi, N.; Ozcan, M. A Review on Enhancing the Life of Teeth by Toothpaste Containing Bioactive Glass Particles. Curr. Oral Health Rep. 2024, 11, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, D. Bioglass at 50—A look at Larry Hench’s legacy and bioactive materials. Biomed. Glas. 2019, 5, 178–184. [Google Scholar] [CrossRef]
- Dai, L.L.; Mei, M.L.; Chu, C.H.; Lo, E.C.M. Mechanisms of Bioactive Glass on Caries Management: A Review. Materials 2019, 12, 4183. [Google Scholar] [CrossRef] [PubMed]
- El-Wassefy, N.A. Remineralizing effect of cold plasma and/or bioglass on demineralized enamel. Dent. Mater. J. 2017, 36, 157–167. [Google Scholar] [CrossRef]
- Ramadoss, R.; Padmanaban, R.; Subramanian, B. Role of bioglass in enamel remineralization: Existing strategies and future prospects—A narrative review. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int. J. Mol. Sci. 2019, 20, 5960. [Google Scholar] [CrossRef] [PubMed]
- Vilhena, F.V.; Lonni, A.A.S.G.; D’Alpino, P.H.P. Silicon-enriched hydroxyapatite formed induced by REFIX-based toothpaste on the enamel surface. Braz. Dent. Sci. 2021, 24, 1–7. [Google Scholar] [CrossRef]
- Alonso, R.C.B.; Oliveira, L.d.; Silva, J.A.B.; Santos, W.B.B.d.; Ferreira, L.R.d.S.L.; Guiraldo, R.D.; Vilhena, F.V.; D’Alpino, P.H.P. Effectiveness of Bioactive Toothpastes against Dentin Hypersensitivity Using Evaporative and Tactile Analyses: A Randomized Clinical Trial. Oral 2024, 4, 36–49. [Google Scholar] [CrossRef]
- Zangrando, M.S.R.; Silva, G.F.F.; Bigotto, M.L.B.; Cintra, F.M.R.N.; Damante, C.A.; Sant’Ana, A.C.P.; Vilhena, F.V. Blocking tubules technologies for dentin hypersensitivity in periodontal patients—Pilot study. Res. Soc. Dev. 2021, 10, e35101320398. [Google Scholar] [CrossRef]
- Moras, C.G.; Acharya, S.R.; Adarsh, U.K.; Unnikrishnan, V.K. Regenerative biomineralization potential of commercially available remineralizing agents as a preventive treatment approach for tooth erosion—An in vitro laser-induced breakdown spectroscopy analysis. J. Conserv. Dent. JCD 2023, 26, 165–169. [Google Scholar] [CrossRef]
- Rahman, B.; El-Damanhoury, H.M.; Sheela, S.; Ngo, H.C. Effect Of Calcium Silicate, Sodium Phosphate, and Fluoride on Dentinal Tubule Occlusion and Permeability in Comparison to Desensitizing Toothpaste: An In Vitro Study. Oper. Dent. 2021, 46, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Mc Gowan, J.; Straus, S.; Moher, D.; Langlois, E.V.; O’Brien, K.K.; Horsley, T.; Aldcroft, A.; Zarin, W.; Garitty, C.M.; Hempel, S.; et al. Reporting scoping reviews-PRISMA ScR extension. J. Clin. Epidemiol. 2020, 123, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Athanasiadou, D.; Eymael, D.; Hajhamid, B.; Carneiro, K.M.M.; Prakki, A. Chemical and Ultrastructural Characterization of Dentin Treated with Remineralizing Dentifrices. J. Funct. Biomater. 2024, 15, 25. [Google Scholar] [CrossRef]
- Tomaz, P.L.S.; Sousa, L.A.; Aguiar, K.F.; Oliveira, T.S.; Matochek, M.H.M.; Polassi, M.R.; D’Alpino, P.H.P. Effects of 1450-ppm fluoride-containing toothpastes associated with boosters on the enamel remineralization and surface roughness after cariogenic challenge. Eur. J. Dent. 2020, 14, 161–170. [Google Scholar] [CrossRef]
- Fernandes, N.L.S.; Juliellen, L.D.C.; Andressa, F.B.O.; D’Alpino, H.P.P.; Sampaio, C.F. Resistance against erosive challenge of dental enamel treated with 1,450-PPM fluoride toothpastes containing different biomimetic compounds. Eur. J. Dent. 2021, 15, 433–439. [Google Scholar] [CrossRef]
- Poggio, C.; Gulino, C.; Mirando, M.; Colombo, M.; Pietrocola, G. Preventive effects of different protective agents on dentin erosion: An in vitro investigation. J. Clin. Exp. Dent. 2017, 9, e7–e12. [Google Scholar] [CrossRef]
- Altan, H.; Goztas, Z.; Kahraman, K.; Kus, M.; Tosun, G. Inhibition Effects of Different Toothpastes on Demineralisation of Incipient Enamel Lesions. Oral Health Prev. Dent. 2019, 17, 179–185. [Google Scholar] [CrossRef]
- El-Damanhoury, H.M.; Elsahn, N.A.; Sheela, S.; Bastaty, T. In Vitro Enamel Remineralization Efficacy of Calcium Silicate-Sodium Phosphate-Fluoride Salts versus NovaMin Bioactive Glass, Following Tooth Whitening. Eur. J. Dent. 2021, 15, 515–522. [Google Scholar] [CrossRef]
- Chalas, R.; Wojcik-Checinska, I.; Zamoscinska, J.; Bachanek, T. Assessment of Pain Intensity in Patients with Dentin Hypersensitivity After Application of Prophylaxis Paste Based on Calcium Sodium Phosphosilicate Formula. Med. Sci. Monit. 2015, 21, 2950–2955. [Google Scholar] [CrossRef] [PubMed]
- Zang, P.; Parkinson, C.; Hall, C.; Wang, N.; Jiang, H.; Zhang, J.; Du, M. A Randomized Clinical Trial Investigating the Effect of Particle Size of Calcium Sodium Phosphosilicate (CSPS) on the Efficacy of CSPS-containing Dentifrices for the Relief of Dentin Hypersensitivity. J. Clin. Dent. 2016, 27, 54–60. [Google Scholar] [PubMed]
- Sufi, F.; Hall, C.; Mason, S.; Shaw, D.; Milleman, J.; Milleman, K. Efficacy of an experimental toothpaste containing 5% calcium sodium phosphosilicate in the relief of dentin hypersensitivity: An 8-week randomized study (Study 2). Am. J. Dent. 2016, 29, 101–109. [Google Scholar]
- Hall, C.; Mason, S.; Cooke, J. Exploratory randomised controlled clinical study to evaluate the comparative efficacy of two occluding toothpastes—A 5% calcium sodium phosphosilicate toothpaste and an 8% arginine/calcium carbonate toothpaste—For the longer-term relief of dentine hypersensitivity. J. Dent. 2017, 60, 36–43. [Google Scholar] [CrossRef]
- Fu, Y.; Sufi, F.; Wang, N.; Young, S.; Feng, X. An Exploratory Randomised Study to Evaluate the Efficacy of an Experimental Occlusion-based Dentifrice in the Relief of Dentin Hypersensitivity. Oral Health Prev. Dent. 2019, 17, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Bhowmik, E.; Pawar Chandrashekhar, D.; Sharma Hareesha, M. Comparative evaluation of fluorinol and calcium sodium phosphosilicate-containing toothpastes in the treatment of dentin hypersensitivity. Int. J. Dent. Hyg. 2021, 19, 421–428. [Google Scholar] [CrossRef]
- Arshad, S.; Zaidi, S.J.A.; Farooqui, W.A. Comparative efficacy of BioMin-F, Colgate Sensitive Pro-relief and Sensodyne Rapid Action in relieving dentin hypersensitivity: A randomized controlled trial. BMC Oral Health 2021, 21, 498. [Google Scholar] [CrossRef] [PubMed]
- Majji, P.; Murthy, K.R. Clinical efficacy of four interventions in the reduction of dentinal hypersensitivity: A 2-month study. Indian J. Dent. Res. 2016, 27, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Gallob, J.; Sufi, F.; Amini, P.; Siddiqi, M.; Mason, S. A randomised exploratory clinical evaluation of dentifrices used as controls in dentinal hypersensitivity studies. J. Dent. 2017, 64, 80–87. [Google Scholar] [CrossRef]
- Salah, R.; Afifi, R.R.; Kehela, H.A.; Aly, N.M.; Rashwan, M.; Hill, R.G. Efficacy of novel bioactive glass in the treatment of enamel white spot lesions: A randomized controlled trial. J. Evid. Based Dent. Pract. 2022, 22, 101725. [Google Scholar] [CrossRef]
- Hamdi, K.; Hamama, H.H.; Motawea, A.; Fawzy, A.; Mahmoud, S.H. Long-term evaluation of early-enamel lesions treated with novel experimental tricalcium silicate paste: A 2-year randomized clinical trial. J. Esthet. Restor. Dent. 2022, 34, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Mollabashi, V.; Heydarpour, M.; Farhadifard, H.; Alafchi, B. DIAGNOdent pen quantification of the synergy of NovaMin(R) in fluoride toothpaste to remineralize white spot lesions in patients with fixed orthodontic appliances: A double-blind, randomized, controlled clinical trial. Int. Orthod. 2022, 20, 100632. [Google Scholar] [CrossRef] [PubMed]
- Michaelis, L.; Ebel, M.; Bekes, K.; Klode, C.; Hirsch, C. Influence of caries and molar incisor hypomineralization on oral health-related quality of life in children. Clin. Oral Investig. 2021, 25, 5205–5216. [Google Scholar] [CrossRef] [PubMed]
- Weerheijm, K.L. Molar incisor hypomineralisation (MIH). Eur. J. Paediatr. Dent. 2003, 4, 114–120. [Google Scholar] [PubMed]
- Jalevik, B.; Klingberg, G. Treatment outcomes and dental anxiety in 18-year-olds with MIH, comparisons with healthy controls—A longitudinal study. Int. J. Paediatr. Dent. 2012, 22, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Jälevik, B.; Sabel, N.; Robertson, A. Can molar incisor hypomineralization cause dental fear and anxiety or influence the oral health-related quality of life in children and adolescents?—A systematic review. Eur. Arch. Paediatr. Dent. 2022, 23, 65–78. [Google Scholar] [CrossRef]
- Raposo, F.; de Carvalho Rodrigues, A.C.; Lia, É.N.; Leal, S.C. Prevalence of Hypersensitivity in Teeth Affected by Molar-Incisor Hypomineralization (MIH). Caries Res. 2019, 53, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Rodd, H.D.; Graham, A.; Tajmehr, N.; Timms, L.; Hasmun, N. Molar Incisor Hypomineralisation: Current Knowledge and Practice. Int. Dent. J. 2021, 71, 285–291. [Google Scholar] [CrossRef]

{kind=link}
| Technology | Dentifrice | pH | Bioactive Si-Compounds | Fluoride Compound and Concentration |
|---|---|---|---|---|
| NovaMin | Sensodyne Repair & Protect—Haleon | 8.63 | Bioglass | 1.420 ppm F- (MFP *) |
| NR5 | Regenerate—UNILEVER | 8.92 | Calcium Silicate/Sodium Phosphate | 1.450 ppm F- (NaF and MFP) |
| REFIX | Regenerator Sensitive—Dentalclean | 4.72 | Silica/Sodium Phosphate and Phosphoric Acid | 1.450 ppm F- (NaF) |
| Inclusion | Exclusion |
|---|---|
| All geographical areas but published in English language | Language other than English |
| Experimental studies (in vitro and in vivo) | Literature reviews, opinions, dissertations, conference presentations, discussion papers |
| Peer reviewed articles | Not peer reviewed |
| Published in the last 10 years | More than 10-year publication |
| Bioactive Si-toothpastes | Silica as abrasive component or incorporated in dental materials or other oral health products |
| Author (Year) | Study Aim | Outcome Measurement | Sample Size (SS), Follow-Up (FU) | Material(s) or Technology (ies) Used | Active Agent(s) | Primary Results |
|---|---|---|---|---|---|---|
| [49] Poggio et al. (2017) Italy | Evaluate effects of protective agents on dentin erosion by soft drinks. | Percent weight loss, SEM imaging | SS: 70 human dentin specimens FU: 32 min total immersion in Coca-Cola | Remin Pro | Hydroxyapatite | Biorepair and regenerate significantly reduced dentin weight loss, showing greater resistance to acid erosion compared to other agents. Remin Pro and MI Paste Plus showed results similar to the control group, while Tooth Mousse and Biorepair Plus increased dentin demineralization. |
| MI Paste Plus | CPP-ACPF and fluoride | |||||
| Tooth Mousse | CPP-ACP and fluoride | |||||
| Biorepair | Zinc hydroxyapatite, silica and tetrapotassiumpyrophospate | |||||
| Biorepair Plus | Zinc hydroxyapatite, silica and tetrapotassiumpyrophospate | |||||
| Regenerate | Calcium silicate, sodium phosphate, sodium monofluorophosphate (1450 ppm fluoride) | |||||
| [50] Altan et al. (2019) Turkey | Evaluate inhibition of demineralization in enamel lesions. | SEM imaging, EDX with weight percentage of mineral changes (Ca, P, Na, Si) | SS: 50 human enamel blocks FU: 5 days pH cycling | Arginine | Arginine | All toothpaste groups showed a statistically significant increase in Ca and P compared to the control group (p < 0.05). CPP-ACP showed the highest increase in Ca and P. NovaMin increased Na and Si significantly. |
| Fluoride | Sodium monofluorophosphate (fluoride) | |||||
| CPP-ACP | CPP-ACP | |||||
| Novamin | NaF, calcium sodium phosphosilicate 5% (NovaMin) | |||||
| [12] Vilhena et al. (2021) Brazil | Assess mineral content and surface and cross-sectional morphology of enamel and dentin tissues treated with REFIX technology. | SEM imaging, with an energy-dispersive X-ray spectroscopy (EDS). | SS: Bovine enamel blocks (n = 5) FU: 7 days of pH cycling | REFIX technology | NaF, tetrasodium pyrophosphate, silica | REFIX created a silicon-enriched layer on enamel and occluded dentin tubules after 7 days. |
| [47] Tomaz et al. (2020) Brazil | Investigate remineralization of enamel with fluoride-containing toothpastes with different active remineralization agents. | Surface hardness recovery (% SHR), surface enamel roughness (Ra), pH, %weight of particles, zeta potential, and polydispersity index of toothpaste | SS: Bovine enamel blocks (n = 8/per group) FU: 7 days of pH cycling | REFIX | 1450 ppm F− (as sodium fluoride), tetrasodium pyrophosphate, silica | Elmex Sensitive and REFIXshowed more effective remineralization; higher surface roughness when treatedwith REFIX, and NR-5 after a cariogenic challenge. |
| NR-5 | 1450 ppm F− (as sodium fluoride and sodium monofluorophosphate), calcium silicate and sodium phosphate | |||||
| Colgate Total 12 Daily Repair | 1450 ppm F− (as sodium fluoride), tetrasodium pyrophosphate, arginine | |||||
| Bianco Pro Clinical | 1450 ppm F− (as sodium fluoride) 3% tricalcium phosphate (β-TCP) | |||||
| Elmex Sensitive | 1450 ppm F− (as sodium monofluorophosphate), β-TCP and tetrasodium pyrophosphate | |||||
| [51] El-Damanhoury et al. (2021) United Arab Emirates | Evaluate the effect of in-office bleaching on enamel surface and compare the efficacy of calcium silicate–sodium phosphate–fluoride (CS) and NovaMin bioactive glass (NM) in remineralizing bleached enamel. | Surface microhardness, surface roughness, SEM/EDX elemental analysis | SS: 40 human premolars (n = 10) FU: 7 days pH cycling | NovaMin | NaF, calcium sodium phosphosilicate 5% | CS and CS + NR-5 were more effective in remineralization and reducing roughness compared to NovaMin. CS and CS + NR-5 were more effective in restoring hardness and smoothness. |
| NR-5 (CS) | 1450 ppm F− (as sodium fluoride and sodium monofluorophosphate), calcium silicate and sodium phosphate | |||||
| Additional treatment with NR-5 boosting serum (CS + NR-5) | Calcium silicate, sodium phosphate, and sodium monoflourophosphate | |||||
| [48] Fernandes et al. (2021) Brazil | Assess enamel superficial and subsurface morphology treated with fluoridated gels containing different biomimetic compounds after erosive challenge. | SEM imaging, with an energy-dispersive X-ray spectros- copy (EDS). | SS: Bovine enamel blocks (n = 5/per group) FU: 6 days of pH cycling | NR-5 | 1450 ppm F− (as sodium fluoride and sodium monofluorophosphate), calcium silicate and sodium phosphate | REFIX provided smoother enamel surface and higher resistance to erosion. |
| REFIX | 1450 ppm F− (as sodium fluoride), tetrasodium pyrophosphate, silica | |||||
| NovaMin | NaF, calcium sodium phosphosilicate 5% | |||||
| [44] Rahman et al. (2021) United Arab Emirates | Compare dentinal tubule occlusion and permeability of a calcium silicate-, sodium phosphate-, and fluoride-based (CSSPF) toothpaste. | SEM imaging, with an energy-dispersive X-ray spectros- copy (EDS). | SS: 78 human dentin discs FU: 7 days | NR-5 | Sodium monofluorophosphate (1450 ppm fluoride), calcium silicate, trisodium phosphate | Regenerate showed highest occlusion and calcium deposition, followed by NovaMin. Signal Sensitive Expert showed a less effective tubule occlusion and permeability reduction. |
| NovaMin | NaF, calcium sodium phosphosilicate 5% | |||||
| Potassium Nitrate (Signal Sensitive Expert) | Hydrated silica, potassium nitrate and NaF | |||||
| [40] Vilhena et al. (2021) Brazil | Characterize mineral content and morphology of enamel treated with REFIX toothpaste. | SEM imaging, with an energy-dispersive X-ray spectros- copy (EDS). | SS: Bovine enamel blocks (n = 5) FU: 7 days of pH cycling | REFIX | 1450 ppm F− (as sodium fluoride), tetrasodium pyrophosphate, silica | EDS demonstrated the presence of Si (silicon), Na (sodium), P (phosphorus), andF (fluorine), among others. REFIX formed a 14 μm thick mineral layer enriched with silicon on enamel surface. |
| [4] Fernandes et al. (2022) Brazil | Evaluate fluoride-containing toothpastes with different technologies in remineralizing artificial enamel caries. | Surface microhardness recovery (%SMHR), fluorescence recovery (ΔFRE) with quantitative light-induced fluorescence, SEM imaging, with an energy-dispersive X-ray spectros- copy (EDS). | SS: Bovine enamel blocks (n = 12/per group) FU: 6 days of pH cycling | REFIX | 1450 ppm F− (as sodium fluoride), tetrasodium pyrophosphate, silica | REFIX promoted enamel surface microhardness enamel recovery and the formation of a silicon-enriched mineral layer. |
| NR-5 | 1450 ppm F− (as sodium fluoride and sodium monofluorophosphate), calcium silicate and sodium phosphate | |||||
| NovaMin | NaF, calcium sodium phosphosilicate 5% | |||||
| [43] Moras et al. (2023) India | Compare the surface remineralization potential of SAP P11-4 (self-assembling peptide) and CSSP (calcium silicate plus sodium phosphate) on sound and demineralized enamel. | Laser-induced breakdown spectroscopy (LIBS) | SS:32 human enamel samples (16 intact, 16 demineralized) FU: 30 days pH cycling | SAP P11-4 (CURODONT™ PROTECT) | SAP P11-4, sodium monoflourophosphate and silica | Both agents significantly increased Ca and P levels; no significant difference between intact and demineralized enamel. |
| CSSP (REGENERATE™ Enamel Science™ Advanced Toothpaste and Serum) | Calcium silicate, sodium phosphate, and sodium monoflourophosphate | |||||
| [7] Vilhena et al. (2023) Brazil | Assess regenerative and protective effects of a fluoride–silicon-rich toothpaste combined with a calcium booster on dental tissues. | SEM imaging, with an energy-dispersive X-ray spectroscopy (EDS) | SS: 5 bovine enamel and 5 bovine dentin blocks FU: Immediate and after 5 days | Fluoride–silicon-rich toothpaste with calcium booster—REFIX technology | NaF, tetrasodiumpyrophosphate, silica, calcium carbonate, and tricalcium phosphate | Mineralized layer formed on enamel and dentin, significant remineralization after treatment with increasing calcium and silicon signals after immediate treatment, and occlusion of dentin tubules. |
| [46] Athanasiadou et al. (2024) Canada | Investigate chemical and ultrastructural changes in dentin with remineralizing toothpastes. | Atomic force microscopy (AFM), SEM imaging, with an energy-dispersive X-ray spectroscopy (EDS), transmissionelectron microscopy (TEM), and selected area electron diffraction (SAED). | SS: 12 human dentin blocks (n = 3 per group) FU: 14 days of toothbrushing | REFIX | 1450 ppm F− (as sodium fluoride), tetrasodium pyrophosphate, silica | All evaluated dentifrices led to successful formation of hydroxyapatite andincreased dentin stiffness. |
| REFIX + Booster | NaF, tetrasodiumpyrophosphate, silica, calcium carbonate, and tricalcium phosphate | |||||
| NovaMin | NaF, calcium sodium phosphosilicate 5% |
| Author (Year) | Study Design | Study Aim | Outcome Measurement | Sample Size (SS), Follow-Up (FU) | Material(s) or Technology(ies) Used | Active Agent(s) | Primary Results |
|---|---|---|---|---|---|---|---|
| [52] Chalas (2015) Poland | Longitudinal study | Effectiveness of single application for dentin hypersensitivity. | Pain assessed using VAS after air and tactile stimuli. | SS: 92 teeth with hypersensitivity FU: Baseline, and after 1 week | NUPRO® Sensodyne® Prophylaxis Paste | Calcium sodium | NovaMin reduced dentin sensitivity in 1 week. |
| Dentsply (NovaMin Formula) | Phosphosilicate (CSPS) | ||||||
| [53] Zang (2016) China | Randomized clinical trial | To compare the efficacy in dentin hypersensitivity relief. | Hypersensitivity measured using Yeaple probe and Schiff scale. | SS: 133 subjects FU: Baseline, and after 1, 2, 4, and 8 weeks | Vitryxx® (NaF and <5% CSPS) | NaF and CSPS | No significant CSPS (calcium sodium phosphosilicate) treatment benefit found. |
| NovaMin® (NaF or SMFP and 5% CSPS) | Sodium monofluorophosphate (SMFP) and CSPS | ||||||
| Regular fluoride toothpaste | Fluoride | ||||||
| [54] Sufi (2016) UK | Randomized clinical trial | To compare the efficacy in relieving dentin hypersensitivity. | Dentin hypersensitivity assessed using tactile and evaporative stimuli, and OHIP-14. | SS: 137 subjects FU: Baseline, and after 4 and 8 weeks | Experimental toothpaste w/5% CSPS | Calcium sodium phosphosilicate (CSPS) | 5% CSPS (calcium sodium phosphosilicate) significantly reduced sensitivity at 4 and 8 weeks. |
| Placebo abrasivity matched 0% CSPS with additional abrasive silica | No active ingrident | ||||||
| Two control fluoride toothpastes | Fluoride | ||||||
| [55] Hall (2017) UK | Randomized clinical trial | To compare the efficacyin relieving dentine hypersensitivity. | Sensitivity assessed using Schiff scale/VAS and tactile threshold. | SS: 135 subjects FU: Baseline, and after 1, 2, 4, 6, and 11 weeks | Sensodyne Repair & Protect (5% CSPS) | Calcium sodium phosphosilicate (CSPS) | 5% CSPS and 8% ACP equally reduced DH over 11 weeks. |
| Colgate Sensitive Pro-Relief (8% arginine and calcium carbonate) | Arginine and calcium carbonate | ||||||
| Colgate Triple Protection (1450 ppm fluoride) | Fluoride | ||||||
| [56] Fu (2019) China | Randomized clinical trial | To compare the efficacyin relieving dentine hypersensitivity. | Hypersensitivity assessed using Schiff scale/VAS and tactile threshold. | SS: 147 subjects FU: Baseline, and after 1, 2, 4, and 8 weeks | 2.5% calcium sodium phosphosilicate toothpaste | Calcium sodium phosphosilicate (CSPS) | No significant difference between CSPS and arginine dentifrices. |
| 8% arginine toothpaste | Arginine | ||||||
| Negative control toothpaste | Fluoride | ||||||
| [16] Patel (2019) India | Randomized clinical trial | To compare the efficacyin relieving dentine hypersensitivity. | Hypersensitivity assessed using tactile and evaporative stimuli (VAS). | SS: 75 subjects FU: Baseline, 15 days, and 1 month | BioMin-F (5% FCPS) | FCPS | 5% FCPS (fluorocalciumphosphosilicate) toothpaste is most effective for reducing DH symptoms. |
| Pro-Argin (8% arginine and calcium carbonate) | Arginine and calcium carbonate | ||||||
| Placebo | Fluoride | ||||||
| [57] Bhowmik (2020) India | Randomized clinical trial | Comparison of fluorinol and sodium calcium phosphosilicate for dentin hypersensitivity. | Sensitivity assessed using VAS for tactile, evaporative, and cold stimuli. Gingival and plaque indices recorded. OHIP-14 used for quality of life. | SS: 30 subjects FU: Baseline, 2nd week, 3rd week, 4th week | Fluorinol-containing Elgydium Sensitive toothpaste | Fluorinol | Both groups reduced DH, but no significant differences were found. |
| 7.5% calcium sodium phosphosilicate-containing Shy-NM toothpaste | Sodium calciumphosphosilicate | ||||||
| [58] Arshad (2021) Pakistan | Randomized clinical trial | Compared Pro-Argin™, strontium acetate, and FCPS dentifrices for immediate DH pain relief. | Sensitivity assessed using SCASS and VAS for airblast, mechanical, and waterjet stimuli. | SS: 128 participants FU: 1 min, 3 days, 2, 4, and 6 weeks | BioMinF® | Fluoro-calcium-phospho-silicates (FCPS) | All groups reduced DH, with Pro-Argin™ and FCPS showing superior efficacy. |
| Colgate® Sensitive Pro-Relief™ | Pro-Argin™ with 8.0% arginine and 1450 ppm fuorides as sodium monofluoro-phosphate in calcium carbonate base | ||||||
| Sensodyne Rapid Action™ | 8% strontium acetate, 1040 ppm fluorides as sodium fuoride | ||||||
| Colgate® Total (Placebo) | NaF, sodium monofluorophosphate, dicalcium phosphate with 1150 ppm F | ||||||
| [59] Majji (2016) India | Randomized clinical trial | To compare the efficacyin reduction of dentinal hypersensitivity. | Dentin hypersensitivity measured using VAS for tactile, thermal, and evaporative stimuli. | SS: 160 subjects FU: Baseline, after 2 weeks, and after 12 months | Toothpaste with 5% potassium nitrate | Potassium nitrate | CSPS (calcium sodium phosphosilicate) toothpaste most effective for dentin sensitivity. |
| NovaMin toothpaste (CSPS) | CSPS, strontium chloride | ||||||
| 10% strontium chloride, herbal formulation | Hekla lava, calendula, kresote, andplantago | ||||||
| [60] Gallob (2017) USA | Randomized clinical trial | To compare the efficacyin relieving dentine hypersensitivity. | Dentin hypersensitivity assessed using tactile and evaporative stimuli, and VRS. | SS: 249 subjects FU: After 4 and 8 weeks | US Sensodyne® Freshmint Maximum Strength | 5% potassium nitrate and fluoride in silica base | Negative controls essential for DH dentifrice evaluation. |
| US Crest® Pro-Health™ Healthy Fresh | Stannous fluoride in silica base | ||||||
| US Colgate® Cavity Protection | Sodium mono fluorophosphate in dicalcium phosphate base | ||||||
| US Colgate® Triple Action | NaF (different concentrations) in silica base and different ppm fluoride concentrations | ||||||
| US Crest® Cavity Protection | Sodium fluoride in silica base and Fluoride | ||||||
| Three toothpastes with non-marketed formulation | Sodium mono fluorophosphate in a silica base and different concentrations of abrasive silica | ||||||
| [41] Alonso et al. (2024) Brazil | Open clinical treatment trial | Evaluated efficacy of new toothpaste for dentin hypersensitivity. | Hypersensitivity assessed using tactile and evaporative stimuli (VAS). | SS: 62 subjects FU: Baseline, immediately after treatment, 1-week treatment | Dentifrice-containing REFIX technology (Regenerador + Sensitive DentalClean, Rabbit Corp, Londrina, PR, Brazil). | Fluoride Tetrasodiumpyrophosphate Silica | Immediate and sustained pain reduction after first use. |
| [10] Seong (2020) UK | Double-blind parallel study | Compared CSSP and fluoride toothpaste for DH pain reduction. | Sensitivity assessed using Schiff/VAS, Yeaple probe, and OHQoL. | SS: 247 subjects FU: Baseline, 14, and 28 days, and at 29 days, 12 h after last productapplication. | Calcium silicate and sodium phosphate toothpaste (CSSP) | Calcium silicate and sodium phosphate (CSSP) | CSSP significantly reduced DH symptoms compared to control. |
| Negative control toothpaste | 1450 ppm fluoride as sodiummonofluorophosphate | ||||||
| [61] Salah (2022) Egypt | Randomized controlled trial | Compared bioactive glass and CPP-ACP for orthodontically-induced WSLs. | WSL dimensions assessed using digital intraoral photos and DIAGNOdent. | SS: 60 subjects FU: Assessment before treatment (T0) and at 1 week (T1), 1 month (T2), 3 months (T3), and 6 months (T4), follow up | BioMinF® (Bio-BAG, Glaxo SmithKline, UK) | Bioactive glass 45S5, Calcium fluoride (3 mol%) | Bio-BAG significantly reduced WSL compared to control. |
| NovaMin (N-BAG, BioMin Technologies Ltd., UK) | Bioactive glass 45S5 | ||||||
| Recaldent (CPP-ACP, GC Corporation, Japan) | Casein phospho-peptide-amorphous calciumphosphate | ||||||
| [62] Hamdi (2022) Egypt | Randomized clinical trial | To compare remineralization potential of TCS, SDF-KI, and CPP-ACP. | Lesions were evaluated clinically using DIAGNOdent. | SS: 45 patients and 92 teeth FU: Immediately, and after 3, 6, 12, and 24 months of treatment | Riva star silver fluoride + potassium iodide | SDF-KI | SDF-KI is more effective than CPP-ACP or TCS for remineralization. |
| Tooth Mousse (CPP-ACP) | Casein phosphopeptide-amorphous calcium phosphate | ||||||
| Tri-calcium silicate paste | TCS | ||||||
| [63] Mollabashi (2022) Iran | Randomized clinical trial | Evaluated NovaMin’s effect on WSL remineralization in orthodontic patients | DIAGNOdent pen was used to score the WSLs | SS: 38 subjects FU: Baseline, and then after usage for 1 and 3 months | Fluoride toothpaste (Sensodyne® Rapid Relief, England) | Fluoride-hydrated silica | DIAGNOdent readings reduced significantly in both groups. |
| NovaMin (Sensodyne® Repair & Protect, England). | Sodium monofluorophosphate (SMFP) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampaio, F.C.; Oliveira, A.F.B.d.; Fernandes, N.L.S.; Gentile, A.C.C.; Marinho, G.B.; Bönecker, M.J.S.; Paschoal, M.A.B.; D’Alpino, P.H.P.; Vilhena, F.V. Silicon-, Silica-, and Silicate-Toothpastes for Remineralization and Repair of Teeth: A Scoping Review. Oral 2024, 4, 467-486. https://doi.org/10.3390/oral4040038
Sampaio FC, Oliveira AFBd, Fernandes NLS, Gentile ACC, Marinho GB, Bönecker MJS, Paschoal MAB, D’Alpino PHP, Vilhena FV. Silicon-, Silica-, and Silicate-Toothpastes for Remineralization and Repair of Teeth: A Scoping Review. Oral. 2024; 4(4):467-486. https://doi.org/10.3390/oral4040038
Chicago/Turabian StyleSampaio, Fabio Correia, Andressa Feitosa Bezerra de Oliveira, Nayanna Lana Soares Fernandes, Ana Carolina Cheron Gentile, Giovanna Bueno Marinho, Marcelo José Strazzeri Bönecker, Marco Aurelio Benini Paschoal, Paulo Henrique Perlatti D’Alpino, and Fabiano Vieira Vilhena. 2024. "Silicon-, Silica-, and Silicate-Toothpastes for Remineralization and Repair of Teeth: A Scoping Review" Oral 4, no. 4: 467-486. https://doi.org/10.3390/oral4040038
APA StyleSampaio, F. C., Oliveira, A. F. B. d., Fernandes, N. L. S., Gentile, A. C. C., Marinho, G. B., Bönecker, M. J. S., Paschoal, M. A. B., D’Alpino, P. H. P., & Vilhena, F. V. (2024). Silicon-, Silica-, and Silicate-Toothpastes for Remineralization and Repair of Teeth: A Scoping Review. Oral, 4(4), 467-486. https://doi.org/10.3390/oral4040038