

B Lymphoproliferative Neoplasms of Uncertain Biological Significance: Report from the IV Workshop of the Italian Group of Hematopathology and Review of the Literature

 , , ,
, , ,  , ,
, ,  ,
, 
 ,
,
Abstract
1. Introduction
2. Submitted Cases of ISFN and ISMCN Associated with Overt Lymphoma
2.1. Case n. 1
2.2. Case n. 2
2.3. Case n. 3
3. Submitted Cases of Early Lymphoproliferative Lesions Originating from the Germinal Center Other Than ISFN and ISMCN
3.1. Case n. 4
3.2. Case n. 5
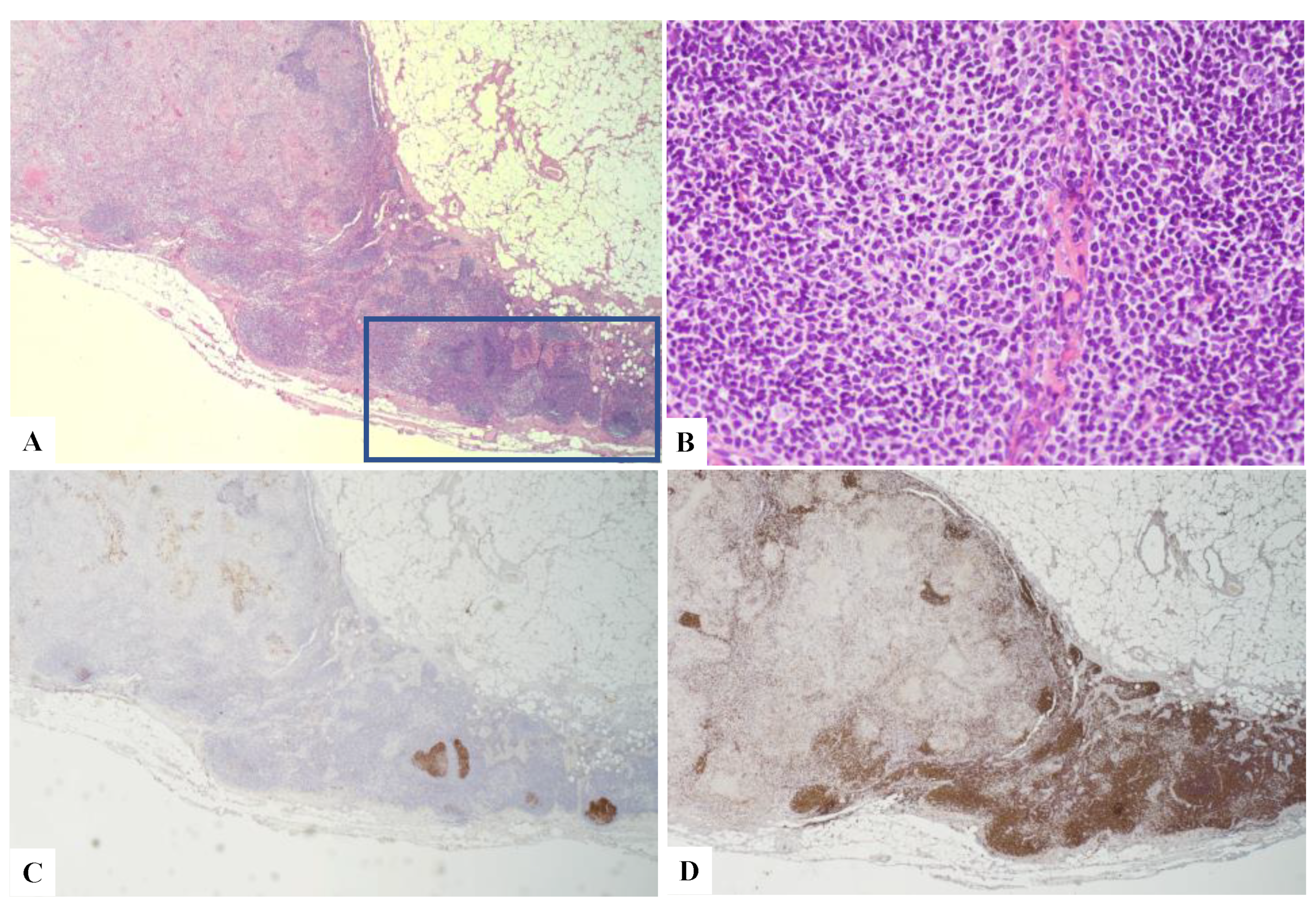
4. Submitted Cases of Early Lymphoproliferative Lesions Arising in the Setting of Monocytoid Hyperplasia
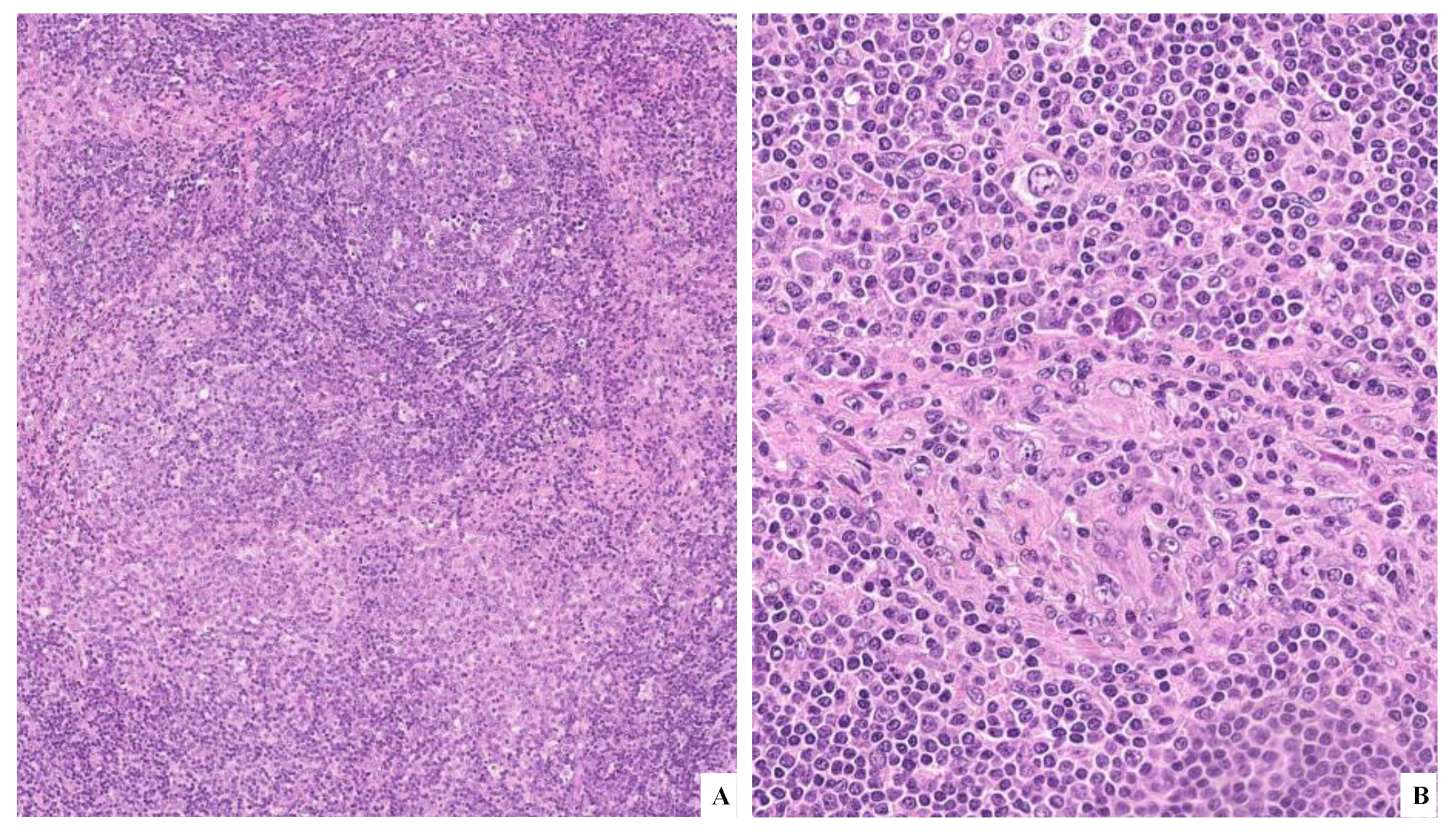
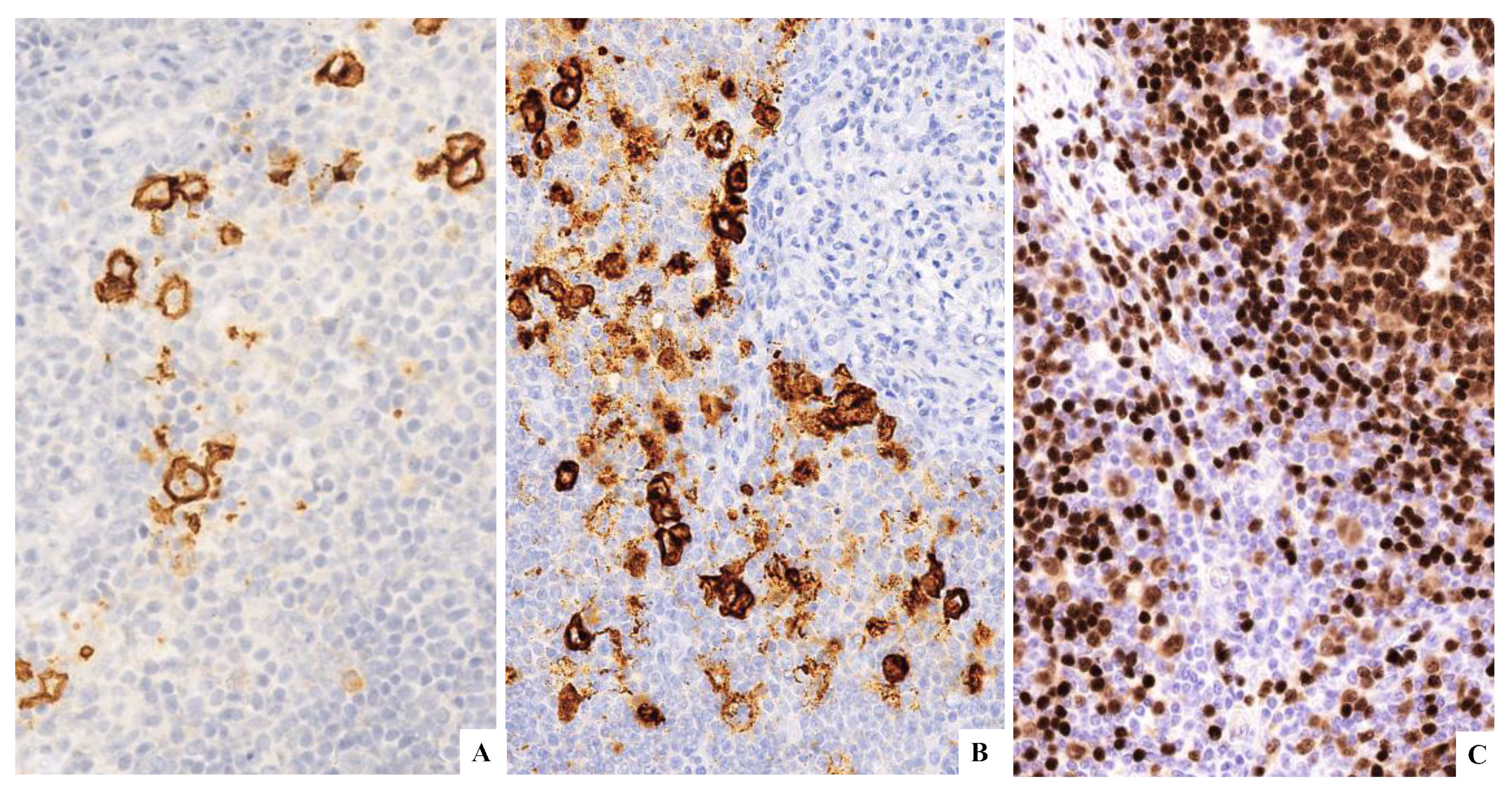
Case n. 6
5. Submitted Cases of Early Lymphoproliferative Lesions Associated with Infectious Diseases and Chronic Inflammation
5.1. Case n. 7
5.2. Case n. 8
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kyle, R.A.; Therneau, T.M.; Rajkumar, S.V.; Larson, D.R.; Plevak, M.F.; Offord, J.R.; Dispenzieri, A.; Katzmann, J.A.; Melton, L.J., 3rd. Prevalence of monoclonal gammopathy of undetermined significance. N. Engl. J. Med. 2006, 354, 1362–1369. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. (Eds.) WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues, 4th ed.; IARC: Lyon, France, 2017.
- Cong, P.; Raffeld, M.; Teruya-Feldstein, J.; Sorbara, L.; Pittaluga, S.; Jaffe, E.S. In situ localization of follicular lymphoma: Description and analysis by laser capture microdissection. Blood 2002, 99, 3376–3382. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Santoro, A. How I treat: Diagnosing and managing “in situ” lymphoma. Blood 2011, 117, 3954–3960. [Google Scholar] [CrossRef] [PubMed]
- Jegalian, A.G.; Eberle, F.C.; Pack, S.D.; Mirvis, M.; Raffeld, M.; Pittaluga, S.; Jaffe, E.S. Follicular lymphoma in situ: Clinical implications and comparisons with partial involvement by follicular lymphoma. Blood 2011, 118, 2976–3064. [Google Scholar] [CrossRef]
- Pillai, R.K.; Surti, U.; Swerdlow, S.H. Follicular lymphoma-like B cells of uncertain significance (in situ follicular lymphoma) may infrequently progress, but precedes follicular lymphoma, is associated with other overt lymphomas and mimics follicular lymphoma in flow cytometric studies. Haematologica 2013, 98, 1571–1580. [Google Scholar] [CrossRef]
- Carvajal-Cuenca, A.; Sua, L.F.; Silva, N.M.; Pittaluga, S.; Royo, C.; Song, J.Y.; Sargent, R.L.; Espinet, B.; Climent, F.; Jacobs, S.A.; et al. In situ mantle cell lymphoma: Clinical implications of an incidental finding with indolent clinical behavior. Haematologica 2012, 97, 270–278. [Google Scholar] [CrossRef]
- Nodit, L.; Bahler, D.W.; Jacobs, S.A.; Locker, J.; Swerdlow, S.H. Indolent mantle cell lymphoma with nodal involvement and mutated immunoglobulin heavy chain genes. Hum. Pathol. 2003, 34, 1030–1034. [Google Scholar] [CrossRef]
- Adam, P.; Schiefer, A.I.; Prill, S.; Henopp, T.; Quintanilla-Martínez, L.; Bösmüller, H.C.; Chott, A.; Fend, F. Incidence of preclinical manifestations of mantle cell lymphoma and mantle cell lymphoma in situ in reactive lymphoid tissues. Mod. Pathol. 2012, 25, 1629–1636. [Google Scholar] [CrossRef][Green Version]
- Nybakken, G.E.; Bala, R.; Gratzinger, D.; Jones, C.D.; Zehnder, J.L.; Bangs, C.D.; Cherry, A.; Warnke, R.A.; Natkunam, Y. Isolated follicles enriched for centroblasts and lacking t(14;18)/BCL2 in lymphoid tissue: Diagnostic and clinical implications. PLoS ONE 2016, 11, e0151735. [Google Scholar] [CrossRef]
- Granai, M.; Lazzi, S. Early pattern of large B-cell lymphoma with IRF4 rearrangement. Blood 2020, 136, 769. [Google Scholar] [CrossRef]
- Kumar, J.; Butzmann, A.; Wu, S.; Easly, S.; Zehnder, J.L.; Warnke, R.A.; Bangs, C.D.; Jangam, D.; Cherry, A.; Lau, J.; et al. Indolent in situ B-Cell neoplasms with MYC rearrangements show somatic mutations in MYC and TNFRSF14 by Next-generation Sequencing. Am. J. Surg. Pathol. 2019, 43, 1720–1725. [Google Scholar] [CrossRef] [PubMed]
- Knudson, A.G., Jr.; Meadows, A.T.; Nichols, W.W.; Hill, R. Chromosomal deletion and retinoblastoma. N. Engl. J. Med. 1976, 295, 1120–1123. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Ozkaya, N.; Hariharan, A. Novel insights into the early histopathogenesis of immunodeficiency-associated Burkitt lymphoma: A case report of Burkitt microlymphoma arising within HIV lymphadenitis. Histopathology 2016, 69, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Granai, M.; Lazzi, S.; Mancini, V.; Akarca, A.; Santi, R.; Vergoni, F.; Sorrentino, E.; Guazzo, R.; Mundo, L.; Cevenini, G.; et al. Burkitt lymphoma with a granulomatous reaction: An M1/Th1-polarised microenvironment is associated with controlled growth and spontaneous regression. Histopathology 2021, 80, 430–442. [Google Scholar] [CrossRef] [PubMed]
- Camacho, F.I.; Algara, P.; Mollejo, M.; Garcìa, J.F.; Montalba, C.; Martìnez, N.; Sánchez-Beato, M.; Piris, M.A. Nodal marginal zone B-cell lymphoma: A heterogenous tumor. A comprehensive analysis of a series of 27 cases. Am. J. Surg. Pathol. 2003, 27, 762–771. [Google Scholar] [CrossRef]
- Poppema, S.; Gilchrist, M. Monocytoid B cells and bcl-2 protein negative in contrast to marginal zone cells and monocytoid B-cell lymphoma. Int. J. Surg. Pathol. 1995, 2, 277. [Google Scholar]
- Kojima, M.; Nakamura, S.; Itoh, H.; Yoshida, K.; Shimizu, K.; Motoori, T.; Yamane, N.; Joshita, T.; Suchi, T. Occurrence of monocytoid B-cells in reactive lymph node lesions. Pathol. Res. Pract. 1998, 194, 559–565. [Google Scholar] [CrossRef]
- Mohrmann, R.L.; Nathwani, B.N.; Brynes, R.K.; Sheibani, K. Hodgkin’s disease occurring in monocytoid B-cell clusters. Am. J. Clin. Pathol. 1991, 95, 802–808. [Google Scholar] [CrossRef]
- Plank, L.; Hansmann, M.L.; Fischer, R. Monocytoid B-cells occurring in Hodgkin’s disease. Virchows Arch. 1994, 424, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, V.; Zen, Y.; Chan, J.K.; Yi, E.E.; Sato, Y.; Yoshino, T.; Klöppel, G.; Heathcote, J.G.; Khosroshahi, A.; Ferry, J.A.; et al. Consensus statement on the pathology of IgG4-related disease. Mod. Pathol. 2012, 25, 1181–1192. [Google Scholar] [CrossRef]
- Cheuk, W.; Yuen, H.K.L.; Chan, A.C.L.; Shih, L.Y.; Kuo, T.T.; Ma, M.W.; Lo, Y.F.; Chan, W.K.; Chan, J.K. Ocular adnexal lymphoma associated with IgG4+ chronic sclerosing dacryoadenitis: A previously undescribed complication of IgG4-related sclerosing disease. Am. J. Surg. Pathol. 2008, 32, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Ohshima, K.; Ichimura, K.; Sato, M.; Yamadori, I.; Tanaka, T.; Takata, K.; Morito, T.; Kondo, E.; Yoshino, T. Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathol. Int. 2008, 58, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Ferry, J.A. IgG4-related lymphadenopathy and IgG4-related lymphoma: Moving targets. Diagn. Histopathol. 2013, 19, 128–139. [Google Scholar] [CrossRef]
- Kanda, G.; Ryu, T.; Shirai, T.; Ijichi, M.; Hishima, T.; Kitamura, S.; Bandai, Y. Peripheral T-cell lymphoma that developed during the follow-up of IgG4-related disease. Intern. Med. 2011, 50, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Ishida, M.; Hodohara, K.; Yoshida, K.; Kagotani, A.; Iwai, M.; Yoshii, M.; Okuno, H.; Horinouchi, A.; Nakanishi, R.; Harada, A.; et al. Occurrence of anaplastic large cell lymphoma following IgG4-related autoimmune pancreatitis and cholecystitis and diffuse large B-cell lymphoma. Int. J. Clin. Exp. Pathol. 2013, 6, 2560–2568. [Google Scholar]
- Uehara, T.; Ikeda, S.; Hamano, H.; Kawa, S.; Moteki, H.; Matsuda, K.; Kaneko, Y.; Hara, E. A case of Mikulicz’s disease complicated by malignant lymphoma: A postmortem histopathological finding. Intern. Med. 2012, 51, 419–423. [Google Scholar] [CrossRef][Green Version]
- Takahashi, N.; Ghazale, A.H.; Smyrk, T.C.; Mandrekar, J.N.; Chari, S.T. Possible association between IgG4-associated systemic disease with or without autoimmune pancreatitis and non-Hodgkin lymphoma. Pancreas 2009, 38, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Takahashi, H.; Tabeya, T.; Suzuki, C.; Naishiro, Y.; Ishigami, K.; Yajima, H.; Shimizu, Y.; Obara, M.; Yamamoto, H.; et al. Risk of malignancies in IgG4- related disease. Mod. Rheumatol. 2012, 22, 414–418. [Google Scholar] [CrossRef]
- Gupta, R.; Khosroshahi, A.; Shinagare, S.; Fernandez, C.; Ferrone, C.; Lauwers, G.Y.; Stone, J.H.; Deshpande, V. Does autoimmune pancreatitis increase the risk of pancreatic carcinoma? a retrospective analysis of pancreatic resections. Pancreas 2013, 42, 506–510. [Google Scholar] [CrossRef]
- Kussick, S.J.; Kalnoski, M.; Braziel, R.M.; Wood, B.L. Prominent clonal B-cell populations identified by flow cytometry in histologically reactive lymphoid proliferations. Am. J. Clin. Pathol. 2004, 121, 464–472. [Google Scholar] [CrossRef]
- Vivian, L.F.; Magnoli, F.; Campiotti, L.; Chini, C.; Calabrese, G.; Sessa, F.; Tibiletti, M.G.; Uccella, S. Composite follicular lymphoma and “early” (in situ and mantle zone growth pattern) mantle cell neoplasia: A rare entity with peculiar cytogenetic and clinical features. Pathol. Res. Pract. 2020, 216, 153067. [Google Scholar] [CrossRef] [PubMed]
- Fend, F.; Quintanilla-Martinez, L.; Kumar, S.; Beaty, M.W.; Blum, L.; Sorbara, L.; Jaffe, E.S.; Raffeld, M. Composite low grade B-cell lymphomas with two immunophenotypically distinct cell populations are true biclonal lymphomas. A molecular analysis using laser capture microdissection. Am. J. Pathol. 1999, 154, 1857–1866. [Google Scholar] [CrossRef]
- Criel, A.; Michaux, L.; de Wolf-Peeters, C. The concept of typical and atypical chronic lymphocytic leukaemia. Leuk. Lymphoma 1999, 33, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Matutes, E.; Oscier, D.; Garcia-Marco, J.; Ellis, J.; Copplestone, A.; Gillingham, R.; Hamblin, T.; Lens, D.; Swansbury, G.J.; Catovsky, D. Trisomy 12 defines a group of CLL with atypical morphology: Correlation between cytogenetic, clinical and laboratory features in 544 patients. Br. J. Haematol. 1996, 92, 382–388. [Google Scholar] [CrossRef]
- Lazzi, S.; Granai, M.; Capanni, M.; Fend, F. Unusual presentation of extra-nodal double-hit follicular lymphoma: A case report. BMC Gastroenterol. 2022, 22, 254. [Google Scholar] [CrossRef]
- Katsushima, H.; Fukuhara, N.; Konosu-Fukaya, S.; Himuro, M.; Kitawaki, Y.; Ichikawa, S.; Ishizawa, K.; Sasano, H.; Harigae, H.; Ichinohasama, R. Does double-hit follicular lymphoma with translocations of MYC and BCL2 change the definition of transformation? Leuk. Lymphoma 2018, 59, 758–762. [Google Scholar] [CrossRef]
- Miyaoka, M.; Kikuti, Y.Y.; Carreras, J.; Ikoma, H.; Hiraiwa, S.; Ichiki, A.; Kojima, M.; Ando, K.; Yokose, T.; Sakai, R.; et al. Clinicopathological and genomic analysis of double-hit follicular lymphoma: Comparison with high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements. Mod. Pathol. 2018, 31, 313–326. [Google Scholar] [CrossRef]
- Miao, Y.; Hu, S.; Lu, X.; Li, S.; Wang, W.; Medeiros, L.J.; Lin, P. Double-hit follicular lymphoma with MYC and BCL2 translocations: A study of 7 cases with a review of literature. Hum. Pathol. 2016, 58, 72–77. [Google Scholar] [CrossRef]
- Tomita, N.; Tokunaka, M.; Nakamura, N.; Takeuchi, K.; Koike, J.; Motomura, S.; Miyamoto, K.; Kikuchi, A.; Hyo, R.; Yakushijin, Y.; et al. Clinicopathological features of lymphoma/leukemia patients carrying both BCL2 and MYC translocations. Haematologica 2009, 94, 935–943. [Google Scholar] [CrossRef]
- Christie, L.; Kernohan, N.; Levison, D.; Sales, M.; Cunningham, J.; Gillespie, K.; Batstone, P.; Meiklejohn, D.; Goodlad, J. C-MYC translocation in t(14;18) positive follicular lymphoma at presentation: An adverse prognostic indicator? Leuk. Lymphoma 2008, 49, 470–476. [Google Scholar] [CrossRef]
- Landgren, O.; Albitar, M.; Ma, W.; Abbasi, F.; Hayes, R.B.; Ghia, P.; Marti, G.E.; Caporaso, N. B-cell clones as early markers for chronic lymphocytic leukemia. N. Engl. J. Med. 2009, 360, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Nann, D.; Ramis-Zaldivar, J.E.; Müller, I.; Gonzalez-Farre, B.; Schmidt, J.; Egan, C.; Salmeron-Villalobos, J.; Clot, G.; Mattern, S.; Otto, F.; et al. Follicular lymphoma t(14;18)-negative is genetically a heterogeneous disease. Blood Adv. 2020, 4, 5652–5665. [Google Scholar] [CrossRef] [PubMed]
- Nam-Cha, S.H.; San-Millan, B.; Mollejo, M.; Garcia-Cosio, M.; Garijo, G.; Gomez, M.; Warnke, R.A.; Jaffe, E.S.; Piris, M.A. Light-chain-restricted germinal centres in reactive lymphadenitis: Report of eight cases. Histopathology 2008, 52, 436–444. [Google Scholar] [CrossRef]
- Attygalle, A.D.; Liu, H.; Shirali, S.; Diss, T.C.; Loddenkemper, C.; Stein, H.; Dogan, A.; Du, M.Q.; Isaacson, P.G. Atypical marginal zone hyperplasia of mucosa-associated lymphoid tissue: A reactive condition of childhood showing immunoglobulin lambda light-chain restriction. Blood 2004, 104, 3343–3348. [Google Scholar] [CrossRef]
- Weniger, M.A.; Küppers, R. Molecular biology of Hodgkin lymphoma. Leukemia 2021, 35, 968–981. [Google Scholar] [CrossRef] [PubMed]
- Gilroy, D.; Sherigar, J. Concurrent small bowel lymphoma and mycobacterial infection: The use of adesonosine deaminase activity and polymerase chain reaction to facilitated rapid diagnosis and treatment. Eur. J. Gastroenterol. Hepatol. 2006, 18, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Ouedraogo, M.; Ouedraogo, S.M.; Cisse, R.; Lougue, C.; Badoum, G.; Sigani, A.; Drabo, Y.J. Active tuberculosis in a patient with Hodgkin’s disease. A case report. Rev. Pneumol. Clin. 2000, 56, 33–35. [Google Scholar] [PubMed]
- Audebert, F.; Schneidewind, A.; Hartmann, P.; Kullmann, F.; Schölmerich, J. Lymph node tuberculosis as primary manifestation of Hodgkin’s disease. Med. Klin. 2006, 101, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Klein, T.O.; Soll, B.A.; Issel, B.F.; Fraser, C. Bronchus-associated lymphoid tissue lymphoma and mycobacterium tuberculosis infection: An unusual case and a review of the literature. Respir. Care 2007, 52, 755–758. [Google Scholar]
- Inadome, Y.; Ikezawa, T.; Oyasu, R.; Noguchi, M. Malignant lymphoma of bronchus-associated lymphoid tissue (BALT) coexistent with pulmonary tuberculosis. Pathol. Int. 2001, 51, 807–811. [Google Scholar] [CrossRef]
- Centkowski, P.; Sawczuk-Chabin, J.; Prochorec, M.; Warzocha, K. Hodgkin’s lymphoma and tuberculosis coexistence in cervical lymph nodes. Leuk. Lymphoma 2005, 46, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Bellido, M.C.; Martino, R.; Martínez, C.; Sureda, A.; Brunet, S. Extrapulmonary tuberculosis and non- Hodgkin’s lymphoma: Coexistence in an abdominal lymph node. Haematologica 1995, 80, 482–483. [Google Scholar] [PubMed]
- Fanourgiakis, P.; Mylona, E.; Androulakis, I.I.; Eftychiou, C.; Vryonis, E.; Georgala, A.; Skoutelis, A.; Aoun, M. Non-Hodgkin’s lymphoma and tuberculosis coexistence in the same organs: A report of two cases. Postgrad. Med. J. 2008, 84, 276–277. [Google Scholar] [CrossRef]
- Gaur, S.; Trayner, E.; Aish, L.; Weinstein, R. Bronchus-associated lymphoid tissue lymphoma arising in a patient with bronchiectasis and chronic Mycobacterium avium infection. Am. J. Hematol. 2004, 77, 22–25. [Google Scholar] [CrossRef]
- Geyer, J.T.; Niesvizky, R.; Jayabalan, D.S.; Mathew, S.; Subramaniyam, S.; Geyer, A.I.; Orazi, A.; Ely, S.A. IgG4 plasma cell myeloma: New insights into the pathogenesis of IgG4-related disease. Mod. Pathol. 2014, 27, 375–381. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GC Involvement | Non-GC Involvement | Histologic Characteristics | Suggested Procedures When Lymphoproliferative Neoplasms of Uncertain Biological Significance Are Encountered | |
|---|---|---|---|---|
| Entities accepted in the 4th WHO edition | ||||
| “In situ” follicular neoplasia (ISFN) | Yes | No | Lack of polarization, closely packed centrocytes with few centroblast. | Exclude pFL and a composite form with appropriate immunohistochemistry. Suggest a complete staging workup to rule out an overt lymphoma in another site. |
| “In situ” mantle cell neoplasia (ISMCN) | No | Yes | Cyclin D1-expressing B-cells in non-expanded mantle zones of otherwise morphologically reactive lymph node. | Exclude a MCLGP and composite form with appropriate immunohistochemistry. Suggest a complete staging workup to rule out an overt lymphoma in another site. |
| Entities not included in the in the 4th WHO edition | ||||
| Atypical GC BCL2-negative | Yes | No | Isolated follicles with GC composed of aggregates of large centroblast with atypical mitosis without centrocytes and BCL2 negative by immunohistochemistry and FISH analysis. | Apply immunohistochemestry to confirm the presence of follicular dendritic networks and the GC origin of the B cell population. Occurrence of strong and diffuse immunoreactivity for IRF4, BCL2, and c-MYC must be assessed. In addition, FISH analysis for IRF4, BCL2, c-MYC rearrangements is advisable. Exclusion of an overt disease with a complete staging workup is mandatory. |
| Early pattern of large B-cell lymphoma (LBCL) with IRF4 rearrangement | Yes | No | Atypical GC enriched with centroblasts, without tingible body macrophages or polarization with strong IRF4 positivity and IRF4 rearrangement. | |
| Single extranodal involvement of “double hit” Follicular lymphoma (DH-FL) | Yes | No | Atypical GC B-cell population with follicular dendritic networks and BCL-2 + c-MYC rearrangements. | |
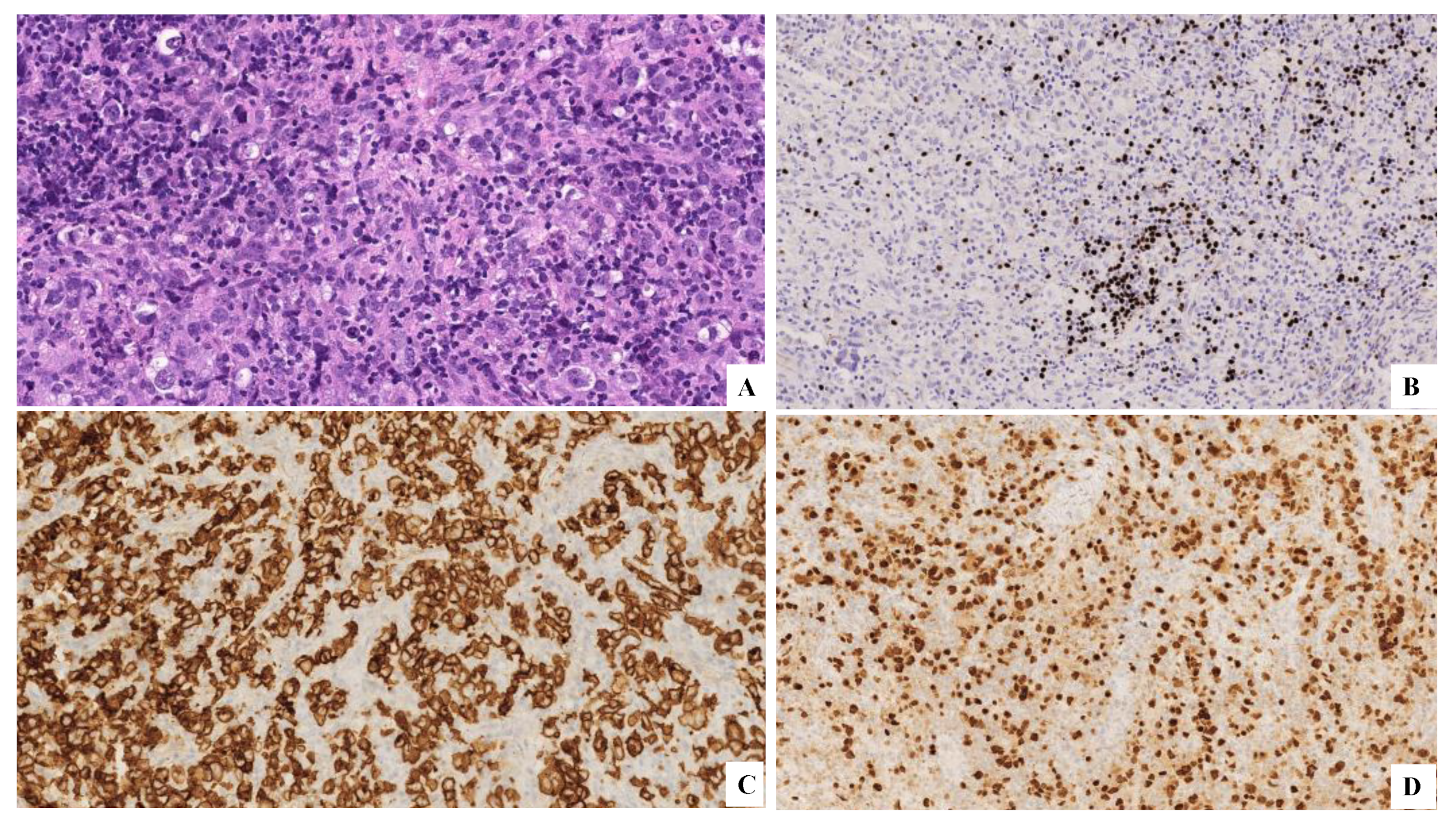
| Early Burkitt lymphoma (BL) | No | Yes | Aggregates composed of medium-sized lymphoid cells morphologically and phenotipically consistent with BL cells along with mitotic figures and apoptotic bodies | Apply immunohistochemical analysis to characterize the medium size population with BL features added to FISH to identify c-MYC rearrengement |
| Early classic Hodgkin lymphoma (cHL) | No | Yes | Presence of RS and HL cells in perifollicular areas with preserved lymph node architecture. | Evaluation of the preserved lymph node architecture. Investigate the scattered atypical RS- and HL-cells by immunohistochemistry. Exclusion of an overt disease with a complete staging workup is mandatory. |
| Case | Gender | Age | Diagnosis | Presence of Overt Lymphoma | Type of Overt Lymphoma |
|---|---|---|---|---|---|
| Case n. 1 | F | 75 y | FL and ISMCN | Yes | FL |
| Case n. 2 | M | 45 y | ISMCN and SLL | Yes | MCL in previous biopsy |
| Case n. 3 | M | 45 y | CLL with atypical phenotype and ISFN | Yes | CLL on bone marrow |
| Case n. 4 | M | 77 y | FL, 3A with focal localization on the contralateral lymph node | Yes | FL, 3A |
| Case n. 5 | F | 72 y | Extranodal FL with BCL2 and c-MYC rearrangement | No | |
| Case n. 6 | F | 61 y | Early cHL in monocytoid hyperplasia | Yes | cHL, mixed cellularity |
| Case n. 7 | M | 76 y | Necrotizing granulomatous lymphadenitis associated with ISFN | No | |
| Case n. 8 | M | 77 y | IgG4-RD with ISFN | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stefano, G.; Magnoli, F.; Granai, M.; Vittone, F.; Santi, R.; Ferrara, D.; Boveri, E.; Florena, A.M.; Fend, F.; Sabattini, E.; et al. B Lymphoproliferative Neoplasms of Uncertain Biological Significance: Report from the IV Workshop of the Italian Group of Hematopathology and Review of the Literature. Hemato 2022, 3, 634-649. https://doi.org/10.3390/hemato3040043
Di Stefano G, Magnoli F, Granai M, Vittone F, Santi R, Ferrara D, Boveri E, Florena AM, Fend F, Sabattini E, et al. B Lymphoproliferative Neoplasms of Uncertain Biological Significance: Report from the IV Workshop of the Italian Group of Hematopathology and Review of the Literature. Hemato. 2022; 3(4):634-649. https://doi.org/10.3390/hemato3040043
Chicago/Turabian StyleDi Stefano, Gioia, Francesca Magnoli, Massimo Granai, Federico Vittone, Raffaella Santi, Domenico Ferrara, Emanuela Boveri, Ada M. Florena, Falko Fend, Elena Sabattini, and et al. 2022. "B Lymphoproliferative Neoplasms of Uncertain Biological Significance: Report from the IV Workshop of the Italian Group of Hematopathology and Review of the Literature" Hemato 3, no. 4: 634-649. https://doi.org/10.3390/hemato3040043
APA StyleDi Stefano, G., Magnoli, F., Granai, M., Vittone, F., Santi, R., Ferrara, D., Boveri, E., Florena, A. M., Fend, F., Sabattini, E., Paulli, M., Ponzoni, M., Lazzi, S., Pileri, S. A., Leoncini, L., & the Italian Group of Hematopathology. (2022). B Lymphoproliferative Neoplasms of Uncertain Biological Significance: Report from the IV Workshop of the Italian Group of Hematopathology and Review of the Literature. Hemato, 3(4), 634-649. https://doi.org/10.3390/hemato3040043