Abstract
Background: Bone tissue decalcification is essential for histopathological evaluation, but conventional methods using inorganic acids degrade nucleic acids, limiting molecular testing. EDTA is known to better preserve DNA, but its suitability for next-generation sequencing (NGS) in clinical settings remains to be validated. Methods: This retrospective study evaluated 752 formalin-fixed paraffin-embedded (FFPE) tissue samples undergoing NGS between January 2022 and October 2024. Of these, 31 were decalcified using EDTA (Osteosoft, Merck, Germany). DNA was extracted using the Qiagen AllPrep® kit and quantified using Qubit and NanoDrop. Libraries were prepared with a custom 30-gene Ampliseq panel and sequenced on the Ion Torrent platform. Sequencing was deemed suboptimal if <95% of target regions reached ≥250X depth. Results were compared to 721 non-decalcified FFPE samples. Results: Suboptimal sequencing occurred in 9.7% of EDTA-decalcified and 9.0% of non-decalcified cases (p = 0.9). DNA concentration (Qubit) and NanoDrop 260/280 ratios were not significantly different (p = 0.4 and p = 0.8, respectively), though EDTA cases had lower DNA concentrations (NanoDrop, p = 0.006) and 260/230 ratios (p = 0.002). Mutation detection in decalcified samples was consistent with known mutation profiles for respective tumor types. Conclusions: EDTA-decalcified FFPE bone tissues produce NGS results comparable to non-decalcified specimens, with similar sequencing success rates and acceptable DNA quality. These findings support the use of EDTA as a suitable decalcification method for molecular diagnostics, enabling broader inclusion of bone specimens in clinical testing.
1. Introduction
Bone tissue decalcification methods utilizing inorganic acids such as hydrochloric acid are effective in removing calcium but compromise the integrity of DNA and RNA, which are critical for molecular analyses [1]. This limitation restricts the diagnostic utility of bone specimens in malignancies, where accurate genetic testing is essential for diagnosis and therapeutic decision-making. EDTA is known to be superior in preserving nucleic acids, allowing for the feasibility of genetic studies [2]. With the advent of more complex NGS testing, there is a greater need for good DNA quality and quantity to produce optimal results. We endeavor to confirm that EDTA is a suitable agent for tissue decalcification that is compatible with NGS testing in our laboratory by comparing the quality and quantity of DNA and the rate of suboptimal NGS test results.
2. Methods
This is a retrospective study investigating formalin-fixed paraffin-embedded (FFPE) bone tissue that has undergone EDTA decalcification (Osteosoft, Merck, Germany) and subsequent NGS testing from January 2022 to October 2024. The duration of EDTA decalcification is not fixed and depends on the size of the specimen. This varies from a short duration to overnight cycles.
Genomic DNA was extracted using the Qiagen AllPrep® DNA/RNA FFPE Kit (QIAGEN GmbH, Hilden, Germany). DNA quality and quantity were assessed using a NanoDrop ND-2000 spectrophotometer and Qubit Quantification Assay (Thermo Fisher Scientific Inc., Darmstadt, Germany). Libraries were prepared using the Ion Torrent Ampliseq 2.0 kit(Thermofisher, Carlsbad, CA, USA) with primer pairs targeting a locally developed, customized NGS panel of around 30 genes, which includes all types of common clinically relevant mutations detected in routine anatomical pathology departments including Single-Nucleotide Variants (SNVs) and indels including those that result in MET exon skipping. Template preparation and sequencing were performed on the Ion Torrent platform. Sequencing was considered optimal if at least 95% of the regions covered obtained a sequencing depth of at least 250X, while a value of 80–95% was considered suboptimal. The results were compared with samples without decalcification that underwent NGS in 2024.
Statistical comparisons were performed using Pearson’s Chi-squared test for categorical variables and the Wilcoxon rank-sum test for continuous variables.
3. Results
During the 3-year study period, 752 cases underwent NGS: 31 bone tissue with EDTA decalcification and 721 without any decalcification. Amongst the 31 types of specimens, 22 were lung adenocarcinoma, 4 were breast carcinoma, 2 were melanoma, 1 was mastocytosis, and 1 was carcinoma of unknown primary origin; all 30 were found in bone specimens, and 1 case of GIST was heavily calcified (Table 1). The frequency of gene-specific mutations was high and expected for decalcified specimens, with 19/22 lung adenocarcinomas having mutations like EGFR, KRAS, TP53, and BRAF. All melanomas and GISTs had KIT exon 11, and one breast carcinoma had a PIK3CA mutation. Finally, the mastocytosis had KIT exon 17 (Table 1).

Table 1.
Summary of bone tissue with EDTA.
The time treated with EDTA ranges from 1 to 5 days with an average of 2.4 days. Suboptimal sequencing coverage was observed in 3 (9.7%) of the EDTA-decalcified cases and 65 (9.0%) of the non-decalcified cases (Figure 1). The three cases with suboptimal sequencing coverage were treated in EDTA for 2, 3, and 4 days, respectively.

Figure 1.
Comparison of the frequency of suboptimal sequencing results in EDTA-treated cases to that in non-decalcified cases.
There was no significant association between the presence or absence of EDTA decalcification and the quality of sequencing results (p = 0.9). Notably, no cases with poor sequencing coverage were observed in either group (Figure 1).
For EDTA-decalcified cases, the DNA concentration measured by Qubit showed a median of 31.60 ng/µL (IQR: 16.09–60.50). NanoDrop measurements for these cases revealed a higher median concentration of 116.80 ng/µL (IQR: 63.70–178.05). The NanoDrop 260/280 ratio for EDTA-decalcified cases had a median of 1.89 (IQR: 1.86–1.93), while the 260/230 ratio had a median of 1.86 (IQR: 1.53–2.06). The results are shown in Table 2 and Figure 1 and Figure 2.
Table 2.
Summary of results.
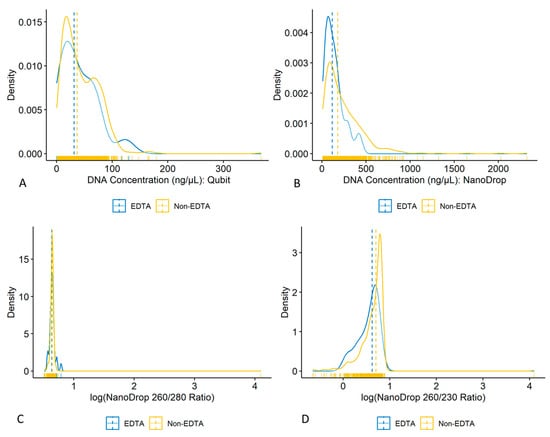
Figure 2.
(A) DNA concentration measured by Qubit (ng/µL); (B) DNA concentration measured by NanoDrop (ng/µL); (C) log of NanoDrop 260/280 ratio; (D) log of NanoDrop 260/230 ratio.
In comparison, non-decalcified cases showed slightly higher DNA concentrations. Qubit measurements had a median of 37.00 ng/µL (IQR: 18.14–66.80), which was not significantly different from EDTA-treated cases (p = 0.4). NanoDrop measurements for these cases were notably higher, with a median of 180.40 ng/µL (IQR: 88.30–343.60), significantly different from EDTA-treated cases (p = 0.006). The NanoDrop 260/280 ratio for non-decalcified cases was comparable (median 1.90; IQR: 1.87–1.92; p = 0.8 vs. EDTA-treated cases). In contrast, the 260/230 ratio was significantly higher for non-decalcified cases (median 2.02; IQR: 1.72–2.21; p = 0.002 vs. EDTA cases). Of note, the lower 260/230 ratio in EDTA-decalcified cases did not result in more library preparation failure or required sample repetition.
The median tumor content and tumor area were also compared between optimal and suboptimal cases (Table 3). Although optimal cases showed higher median tumor content and tumor area, this difference did not reach statistical significance, likely due to low statistical power from the small number of suboptimal cases (n = 3), rather than a true lack of difference between the groups.
Table 3.
Comparing median tumor content and tumor area.
4. Discussion
As molecular profiling becomes increasingly integrated into cancer diagnosis and treatment planning, the preservation of genetic material through optimal decalcification methods is paramount. This would be important in bone biopsies from metastases and primary bone tumors, especially if this was the only site of metastasis or the only place accessible. However, it is time-consuming and adds 1 to 5 days to the delivery of the results.
EDTA has emerged as a preferred agent for decalcifying FFPE tissue due to its ability to preserve nucleic acid integrity for molecular studies [2]. Studies have compared different decalcification agents such as formic acid, hydrochloric acid, and EDTA. EDTA and formic acid were shown to have significantly more DNA yield than hydrochloric acid [3]. In our study, we sought to find out if EDTA-decalcified FFPE tissue was indeed suitable for molecular NGS testing and compared its DNA quality/quantity and sequencing results against non-calcified tissue. We found that EDTA-treated FFPE tissue had significantly lower DNA concentrations as measured by NanoDrop and lower 260/230 nm ratios compared to non-decalcified tissue. However, the DNA concentrations measured by Qubit and NanoDrop 260/280 nm ratios in EDTA-treated tissue were not significantly different from non-decalcified tissue. EDTA-treated tissue also had a similar rate of suboptimal NGS results compared to non-decalcified tissue. Similarly, Miquelstorena-Standley et al. found that DNA concentration was lower in EDTA-decalcified samples (96.7 ± 35.6, p = 0.009) than in non-decalcified samples (237.4 ± 57.6 ng/µL) [1]. Comparable with our results, their NanoDrop 260/280 nm ratios were not significantly different (1.7 ± 0.07) in non-decalcified tissue compared to 1.6 ± 0.13 (p = 0.017) in EDTA-decalcified tissues [1].
Miquelstorena-Standley et al. showed that the use of EDTA and short-term formic acid decalcification did not alter antigenicity for the detection of gene mutations, amplifications, or fusions using Pyrosequencing, PyroMark PCR kit (Qiagen, Hilden, Germany), and RT-PCR; DNA was sequenced using the Truseq FFPE DNA Library Prep QC Kit (Illumina) [1]. However, these technologies were only used to detect six genes in total, compared to NGS, where hundreds of genes are sequenced and read simultaneously, and the amount and quality of DNA required are higher. Boureille et al. looked at 26 cases of EDTA-treated and 8 cases of formic acid-treated non-small-cell lung carcinoma samples and performed NGS and Idylla™ EGFR assays. However, the results are limited as Idylla only covers EGFR, while only nine of the samples contained EGFR mutations according to NGS. Furthermore, the authors mentioned that NGS failed in 58.8% of cases and required Sanger sequencing but did not elaborate as to why the NGS failed, whereas we demonstrated comparable success rates between EDTA-decalcified samples compared with non-decalcified samples using the same NGS platform.
They only performed NGS on seven DNA samples; unfortunately, none of the samples could be qualified in theory as they failed to achieve a quality control DCt score of more than 6, and they required a cover of 100% with a 600x depth read. Of the seven cases, four samples were decalcified using EDTA and had a quality score of up to 95.4%, and two of the cases had 100% interpretable regions. Comparatively, out of our 31 EDTA cases, only 3 (9%) were suboptimal.
Other studies have compared various decalcification agents and focused on multiple ancillary studies such as immunohistochemistry, in situ hybridization, comparative genomic hybridization, and RT-PCR [3,4,5]. Our study, however, focuses on nucleic acid yield and quality and compares the rate of suboptimal NGS results against the standard of non-decalcified cases. One limitation of our study was that we did not look at RNA concentration and quality, nor did we investigate the effect of EDTA decalcification on other types of molecular diagnostic assays like hybridization-based methods. It was also important to note that other factors such as small sample size compared to the total cohort, formalin fixation, and tissue block size could impact DNA quality and quantity. Finally, it is not possible to obtain paired non-bone specimens from the same tumor.
5. Conclusions
We found that EDTA-treated FFPE bone tissue did not have a significantly higher rate of suboptimal sequencing results on NGS compared to non-decalcified tissue. Although there were some quality parameters where EDTA-treated tissue fared poorer, there were others (such as DNA concentration as measured by Qubit and NanoDrop 260/280 nm ratios) where EDTA-treated tissue was not significantly different from non-decalcified tissue. These factors, coupled with the non-inferior sequencing results obtained, showed that EDTA is a suitable decalcification agent for tissue that is needed for downstream NGS testing. This would also provide evidence to support the inclusion of patients who only have decalcified specimens in clinical trials. Future potential validation of these findings could be performed using other sequencing platforms, like long-read sequencing.
Author Contributions
Conceptualization, F.H.X.Y. and T.K.Y.T.; methodology, F.H.X.Y., J.-H.S. and J.W.K.N.; software, J.W.K.N.; validation, T.K.Y.T., F.H.X.Y. and C.P.Y.; formal analysis, H.A.K.; investigation, F.H.X.Y. and T.K.Y.T.; resources, F.H.X.Y.; data curation, F.H.X.Y. and H.A.K.; writing—original draft preparation, F.H.X.Y.; writing—review and editing, J.-H.S., J.W.K.N., H.A.K. and T.K.Y.T.; visualization, H.A.K.; supervision, T.K.Y.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Miquelestorena-Standley, E.; Jourdan, M.-L.; Collin, C.; Bouvier, C.; Larousserie, F.; Aubert, S.; Gomez-Brouchet, A.; Guinebretière, J.-M.; Tallegas, M.; Brulin, B.; et al. Effect of decalcification protocols on immunohistochemistry and molecular analyses of bone samples. Mod. Pathol. 2020, 33, 1505–1517. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.E.; Hong, S.W.; Yoon, S.O. Proposal of an appropriate decalcification method of bone marrow biopsy specimens in the era of expanding genetic molecular study. J. Pathol. Transl. Med. 2015, 49, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.M.; Salunga, R.C.; Huang, V.J.; Tran, Y.; Erlander, M.; Plumlee, P.; Peterson, M.R. Analysis of the effect of various decalcification agents on the quantity and quality of nucleic acid (DNA and RNA) recovered from bone biopsies. Ann. Diagn. Pathol. 2013, 17, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.S.; Edwards, J.; Bartlett, J.W.; Jones, C.; Dogan, A. Routine acid decalcification of bone marrow samples can preserve DNA for FISH and CGH studies in metastatic prostate cancer. J. Histochem. Cytochem. 2002, 50, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Alers, J.C.; Krijtenburg, P.J.; Vissers, K.J.; van Dekken, H. Effect of bone decalcification procedures on DNA in situ hybridization and comparative genomic hybridization. EDTA is highly preferable to a routinely used acid decalcifier. J. Histochem. Cytochem. 1999, 47, 703–710. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).