Abstract
Background/Objectives: Orthopedic hip surgery has undergone advances driven by innovations in surgical techniques and improved patient care protocols. The aim was to synthesize and appraise all studies relevant to hip surgery published in Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA) in 2022–2023. Methods: The search included all studies published in KSSTA from 1 January 2022 to 31 December 2023. Quality assessment was performed using appropriate tools for randomized controlled trials (RCTs), non-RCTs, and systematic reviews. Due to the diverse nature of the included studies, a narrative synthesis approach was used. Results: A total of 33 primary studies were included in this narrative review, of which 10 were reviews (5 systematic reviews), 1 was an RCT, and 22 were non-RCTs. A total of 11 were from the UK, 10 studies were from the USA, and 5 were from Canada. Femoroacetabular impingement (FAI) was investigated in a total of 23 studies, followed by hip micro-instability in 7 studies, dysplasia in 5 studies, and gluteal and hamstring tears in 4 studies. The RCT had a low risk of bias. Of the 22 non-RCTs, 16 had a low risk of bias, 5 had a moderate risk of bias, and 1 had a high risk of bias. All systematic reviews were of moderate quality. Conclusions: Hip arthroscopy is an effective treatment for FAI with promising early outcomes, especially when combined with closed capsular repair and appropriate rehabilitation. Surgeons should tailor their approach to capsular management to optimize recovery, as closed capsular repair may enhance functional outcomes. Additionally, preoperative tools like the HAR Index can help identify patients at higher risk of requiring hip arthroplasty after surgery. The conclusions of the included primary studies align with current general recommendations and contribute valuable insights to the field of hip orthopedics.
1. Introduction
Orthopedic hip surgery has advanced significantly in recent years thanks to innovations in surgical techniques, implant technologies, and patient care protocols [1]. These improvements have expanded treatment options and improved outcomes for various hip conditions. With an aging population, the prevalence of hip-related problems such as osteoarthritis, hip fractures, and degenerative joint disease has risen, increasing the demand for effective surgical solutions [2]. Surgeons are challenged to manage these conditions while striving for faster recovery and improved long-term outcomes.
A significant shift towards minimally invasive approaches, such as hip arthroscopy, has reduced surgical trauma, minimized complications, and shortened recovery times [3]. These techniques, which allow smaller incisions and less tissue disruption, have improved the management of conditions such as femoroacetabular impingement (FAI), micro-instability, labral tears, and cartilage defects. FAI, in particular, has been recognized as a major cause of hip pain and early arthritis in younger patients, leading to the development of specialized surgical techniques [4].
Hip arthroscopy and direct anterior approaches (DAA) have changed the way surgeons access and treat the hip joint. Arthroscopy allows treatment with minimal tissue disruption, reducing the risk of complications, while DAA provides a muscle-sparing option for hip replacement surgery, improving recovery times [5]. These advances increase the precision of procedures and improve the overall patient experience by reducing hospital stays and promoting faster rehabilitation.
However, challenges remain in choosing the right surgical approach based on individual anatomy and pathology. While arthroscopy is effective for some conditions, it may not be appropriate for advanced degenerative disease. In addition, minimally invasive techniques require specialized training and equipment, which may limit their accessibility [6]. Ongoing research is essential to refine these techniques and better understand their long-term outcomes. As hip orthopedics is a rapidly developing area of research, a review would provide a comprehensive, up-to-date resource for both clinicians and researchers working in orthopedics.
In this narrative review, we aimed to synthesize and evaluate all studies relevant to hip surgery published in Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA) during the years 2022–2023. The thematic analysis allowed us to identify trends, gaps, and areas for future research in the field of hip surgery.
2. Materials and Methods
This review was conducted according to a pre-defined protocol, which was registered and published on the Open Science Framework on 30 September 2024. It is available at https://osf.io/hu596/files/osfstorage. In preparing this narrative review, we followed current recommendations [7]. As this narrative review used publicly available studies, ethical approval was not required. However, we adhered strictly to ethical guidelines in reporting and synthesizing the results to ensure transparency and integrity throughout the review process.
2.1. KSSTA
One of the influential journals in the orthopedic category is KSSTA, the official journal of the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA). It is a monthly, peer-reviewed, English-language orthopedic journal focusing on orthopedic surgery, particularly sports trauma and arthroscopy, with an Impact Factor of 3.3 (2023). A total of 765 articles were published in KSSTA in 2022 and 687 in 2023. KSSTA is indexed in all major medical databases such as Science Citation Index, PubMed/MEDLINE, Scopus, EMBASE, EBSCO databases, CINAHL, etc., and is recognized in orthopedic scientific circles for its reputation and credibility, specialization in the field, accessibility, and availability.
2.2. Search Strategy
A search was performed using PubMed to identify all articles published in the journal KSSTA from 2022 to 2023. The search term was limited to the full name of the journal: “Knee surgery, sports traumatology, arthroscopy: official journal of the ESSKA” [Journal], with the results filtered by year. We specifically used the search term ‘hip’ to capture all studies that addressed any aspect of hip surgery. The search was conducted on 1 October 2024 and included all studies published between 1 January 2022 and 31 December 2023.
2.3. Inclusion and Exclusion Criteria
All original research studies, case reports, reviews and clinical studies published in KSSTA in the two years period specified that focused on hip surgery were included. We excluded studies that did not have a primary focus on hip surgery, or that did not provide relevant clinical evidence. KSSTA does not publish articles about hip arthroplasty because they are out of the journal’s focus. In addition, commentaries, editorials, and animal or cadaveric studies were not considered for inclusion in this review.
2.4. Data Extraction and Analysis
To ensure accuracy and reduce bias, two independent reviewers conducted data extraction. Key information systematically gathered from each pertinent study included the authors, year and location of publication, study design, sample size, intervention specifics, measured outcomes, and primary findings relevant to hip surgery. Any disagreements during data extraction were addressed through discussion and mutual agreement among the reviewers.
2.5. Quality Assessment
To evaluate the quality of the included studies, the risk of bias (RoB) was assessed using the Cochrane RoB 2 tool [8] for randomized controlled trials (RCTs), the Risk of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool [9] for non-randomized studies and the revised Measurement Tool to Assess Systematic Reviews (AMSTAR 2) [10] for systematic reviews. Each study was rated based on criteria such as selection, comparability, and outcomes.
2.6. Synthesis of Included Studies
Given the diverse nature of the studies included, a narrative synthesis approach was employed to present the findings. We categorized the studies based on themes identified during the data extraction process, including hip pathologies and surgical techniques, allowing us to identify trends, gaps, and areas for future research in the field of hip surgery.
3. Results
3.1. Literature Search
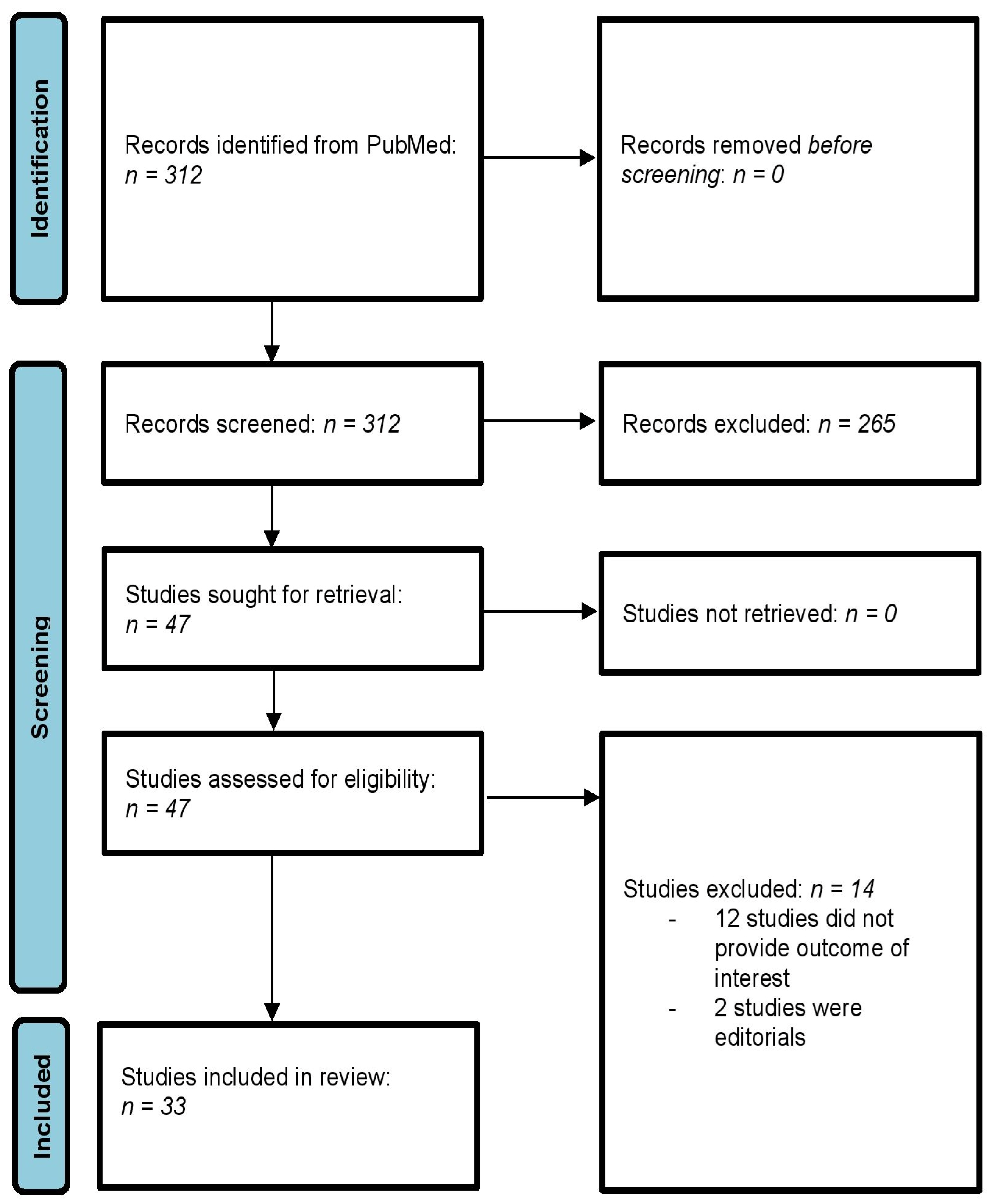
The systematic literature search using the above inclusion and exclusion criteria resulted in a total of 312 primary records. After title and abstract screening, 262 of the primary records were excluded. Of the remaining 47 studies [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57], 15 were excluded after full-text analysis. These 14 studies [44,45,46,47,48,49,50,51,52,53,54,55,56,57] were excluded for the following reasons: (1) 12 studies [44,45,46,48,49,50,51,52,53,54,55,57] did not have their primary focus on hip surgery and did not provide relevant clinical evidence on hip surgery, (2) 2 studies [47,56] were editorials. Finally, a total of 33 primary studies were included in this narrative review [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. The process of the literature search is illustrated in Figure 1.
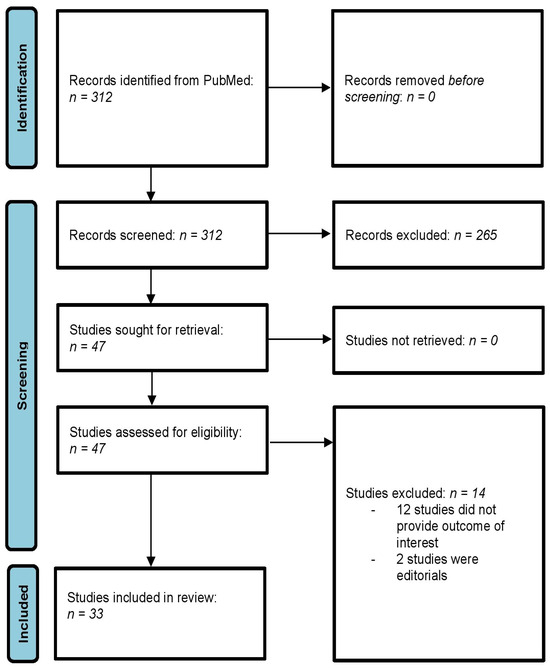
Figure 1.
Flowchart diagram of the literature search. 3.2. Characteristics of Included Studies.
3.2. Characteristics of Included Studies
Of the 33 included studies [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43], 10 were reviews [13,14,16,17,21,25,26,31,34,36], of which 5 [14,16,21,26,31] were systematic reviews, 1 study was an RCT [34], 1 study [43] was an experimental study, 1 was a diagnostic study [11], 9 were retrospective case series [24,27,28,30,32,39,40,41,42], 2 were retrospective cohort studies [19,29], 1 was a cross-sectional study [38], 4 were prospective cohort studies [12,15,18,37], and 4 were prospective case series [20,22,23,33].
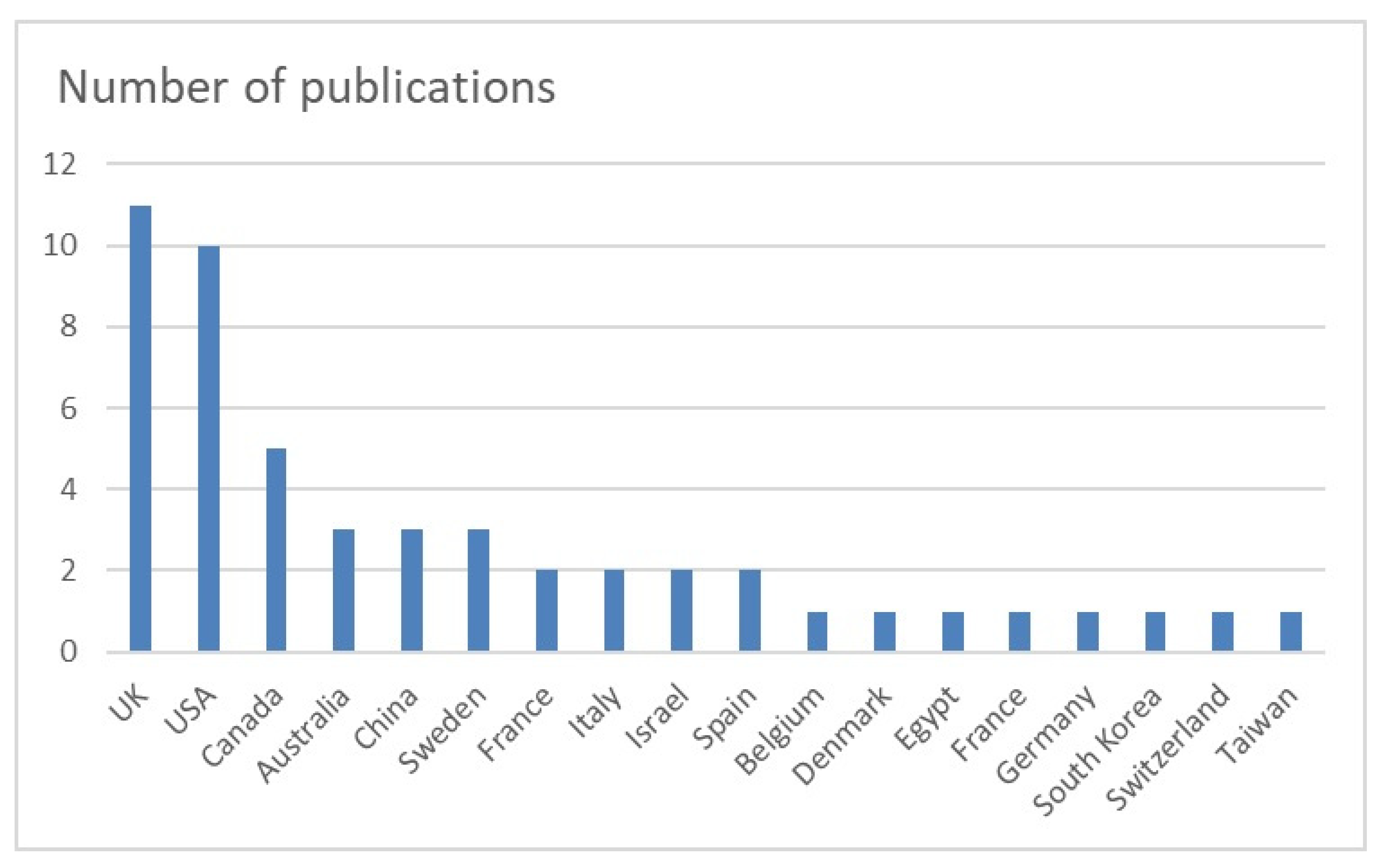
Overall, 11 studies were from the UK [12,17,21,25,26,27,28,36,39,40,41], 10 from the USA [12,16,19,24,25,26,27,28,31,34], 5 from Canada [13,14,21,26,35], 3 from Australia [25,39,41], China [11,22,32], and Sweden [23,37,40], and 2 from France [25,43], Italy [38,42], Israel [24,33], and Spain [15,20]. The countries of origin of the studies are shown in Figure 2. FAI was investigated in a total of 23 studies [11,12,13,14,15,16,17,18,19,20,21,22,23,24,27,28,29,31,32,33,34,35,36]. FAI was followed by hip micro-instability in 7 studies [15,25,26,27,28,31,36], dysplasia in 5 studies [11,25,30,31,36], gluteal and hamstring tears in 4 studies [39,40,41,42], osteoarthritis in 3 studies [11,17,31], and snapping hip in 2 studies [36,43].
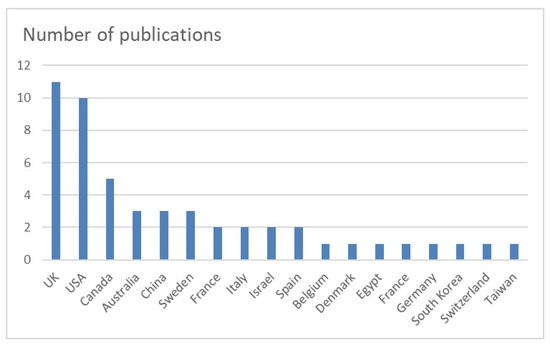
Figure 2.
Countries of origin of the included studies. UK: United Kingdom; USA: United States of America.
The most common procedure studied was hip arthroscopy in 23 studies [11,12,13,14,15,16,18,19,20,21,22,23,24,25,27,28,30,31,32,33,34,35,43], followed by total hip arthroplasty (THA) in 3 studies [14,19,20] and peri-articular endoscopy in 2 studies [42,43]. Of the included studies, 17 provided patient-reported outcome measures (PROMs) [12,13,14,16,17,18,19,20,21,26,31,33,34,36,39,41,42], and 8 reported minimal clinically important differences (MCIDs) [14,15,17,19,21,33,35,41]. The main topics of the publications were FAI, micro-instability, tendon injuries, groin pain in athletes, and bone morphology. Additional characteristics of the studies are presented in Table 1, Table 2, Table 3 and Table 4.

Table 1.
Details of study characteristics.
Table 2.
Details of study characteristics: continuation of Table 1.
Table 3.
Details of study characteristics.
Table 4.
Details of study characteristics: continuation of Table 3.
3.3. Quality Assessment
The quality of the included studies was assessed separately for RCTs using the Cochrane RoB 2 tool [8], for non-RCTs using the Risk of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool [9], and for systematic reviews using AMSTAR 2 [10]. The one RCT [35] had a low risk of bias. Of the 22 non-RCTs [11,12,15,18,19,20,22,23,24,27,28,29,30,32,33,37,38,39,40,41,42,43], 16 [12,15,18,20,22,27,28,29,30,32,33,37,38,39,41,42] had a low risk of bias, 5 [11,19,23,24,43] had a moderate risk of bias, and 1 [40] had a high risk of bias. All systematic reviews [14,16,21,26,31] were of moderate quality overall. All results of the quality assessment of the included studies are shown in Table 5.
Table 5.
Quality assessment of the included studies.
3.4. Femoroacetabular Impingement (FAI)
In a diagnostic study, Bai et al. [11] investigated the thickness and intra-substance changes of the anterior hip capsule, comparing capsular characteristics across 30 patients with varying levels of hip stability. The average anterior capsule thickness in patients with hip dysplasia was 3.2 ± 0.5 mm, notably thinner than that observed in the borderline hip dysplasia and FAI groups (4.5 ± 0.8 mm and 4.7 ± 0.6 mm, respectively). Findings suggest that patients with hip dysplasia show a significantly reduced capsular thickness on MRI, along with delamination of the anterior joint capsule, which may be linked to instability. In a prospective cohort study involving 4963 cases from the UK Non-Arthroplasty Hip Registry (NAHR), Holleyman et al. [12] assessed early outcomes of hip arthroscopy for FAI and factors influencing these outcomes. The study found hip arthroscopy to be an effective surgical option for individuals with symptomatic FAI, leading to statistically significant improvements in PROMs that were sustained over a 12-month follow-up period. In a citation analysis, Abdel Khalik et al. [13] reviewed 10 RCTs published between 2013 and 2023 that examined surgical management approaches for FAI. These studies show considerable variation in clinical uptake, as indicated by citation density, and appear across journals with diverse impact factors. Overall, high-quality evidence on FAI arthroscopy remains largely confined to studies conducted in the USA and Europe.
In a systematic review and meta-analysis of 36 studies involving 4744 patients, Cohen et al. [14] analyzed various capsular management techniques and their outcomes in hip arthroscopy for FAI. Findings showed that closing an interportal capsulotomy led to improved postoperative Harris Hip Scores (HHS). In a prospective cohort study, Tahoun et al. [15] investigated the impact of capsular management on functional outcomes following arthroscopic treatment of FAI and labral tears. They compared outcomes between closed and open capsulotomy in 42 patients. At the 5-year follow-up, patients who underwent arthroscopic treatment with full capsular closure demonstrated significantly better functional results, as assessed by the Non-Arthritic Hip Score (NAHS) and Hip Outcome Score (HOS), compared to those with open capsulotomy. Early follow-up data suggested that closed capsular repair may enhance sports-specific outcomes. Additionally, controlled capsulotomy, limited to the zona orbicularis, did not result in any postoperative instability. Both groups showed comparable rates of achieving MCID and similar reoperation frequencies. George et al. [16], in a systematic review of 11 studies involving 440 patients, assessed the use of orthobiologics in treating FAI. Both platelet-rich plasma (PRP) and cell-based therapies have been commonly utilized during hip arthroscopy, particularly for labral repair and acetabular chondral lesions. The cell-based therapy groups reported better PROM outcomes at final follow-up in comparison to the control group. Andronic et al. [17] conducted a scoping review of 24 studies to evaluate the outcomes of non-operative treatments for FAI, irrespective of the level of degeneration. Their findings indicate no evidence of poorer outcomes in cases of FAI with concomitant Tönnis grade 2 or higher managed conservatively. Hip-specific physiotherapy, incorporating activity modification and core strengthening, alongside adjunctive measures such as corticosteroid injections and non-steroidal anti-inflammatory drugs (NSAIDs) use, may help delay the necessity for surgical intervention. Dippmann et al. [18], in a prospective cohort study utilizing data from the Danish Hip Arthroscopy Registry (DHAR), analyzed the outcomes of arthroscopic treatment for FAI in 4914 patients, comparing those with and without radiographic signs of acetabular retroversion. Their findings showed no significant differences in outcomes between the two groups at 1- and 2-year follow-ups.
In a retrospective cohort study, Shankar et al. [19] examined the influence of age on the time to achieve MCID, Substantial Clinical Benefit (SCB), and Patient Acceptable Symptom State (PASS) following primary hip arthroscopy in 285 patients with FAI. They found that PASS, but not MCID or SCB, was achieved later in patients aged 50–75 compared to those aged 20–34. Seijas et al. [20], in a prospective case series, introduced a new tool to predict the risk of conversion to THA after hip arthroscopy in 584 patients with FAI. Four factors—age, Body Mass Index (BMI), Tönnis grade, and acetabular labral disruption—were associated with an elevated risk of THA conversion. Cut-off points were established for each variable, forming the Hip Arthroplasty Risk Index (HAR Index), a 0–4 point scale assigning binary scores (0 or 1) based on whether thresholds were met. The corresponding THA risk percentages for HAR Index scores were 1.1%, 6.2%, 17.9%, 55.1%, and 79.3%. The HAR Index demonstrated strong predictive accuracy, with an area under the ROC curve of 0.89, offering a practical tool for clinicians to better assess arthroscopy suitability in FAI patients. Zhu et al. [21], in a systematic review of 6 studies involving 213 patients (231 hips), evaluated hip arthroscopy for FAI in the context of generalized ligamentous laxity. Their findings indicated that arthroscopy effectively reduced pain and improved function, showing statistically significant improvements across all PROMs in this patient group. Yang et al. [22], in a prospective case series, analyzed the femoral neck-shaft angle (NSA) using computer tomography scans in 150 FAI patients, exploring its correlation with anterior capsule thickness. They observed that a 1° decrease in NSA was linked to a 0.24 mm increase in anterior capsule thickness. Sjövall Anari et al. [23] conducted a prospective case series to assess return-to-sport (RTS) rates in 83 elite soccer players following hip arthroscopy for FAI. They reported that 85.5% of players successfully returned to sport within the first or second season post-surgery. Marom et al. [24], in a retrospective case series, investigated RTS outcomes in 87 competitive soccer players (119 hips) after hip arthroscopy for FAI and identified factors influencing RTS. Among these players, 65 (74.7%) resumed sport, with 49% returning to or exceeding their pre-injury performance levels. Pain/discomfort (50%) and fear of re-injury (31.8%) were the most cited reasons for not returning. The mean time to RTS was 33.1 ± 26.3 weeks. Of the 22 players who did not return, 14 (63.6%) expressed satisfaction with the surgery. Multivariable logistic regression revealed that female players (OR = 0.27; CI = 0.083 to 0.872; p = 0.029) and older players (OR = 0.895; 95% CI = 0.832 to 0.963; p = 0.003) were less likely to return to sport. These findings can help guide clinicians and soccer players in setting realistic expectations for arthroscopic FAI management.
3.5. Micro-Instability of the Hip
Khanduja et al. [25] used the Delphi method to develop the first expert consensus on diagnosing hip micro-instability. The resulting diagnostic tool highlights the complexity clinicians face when making this diagnosis. Cohen et al. [26], in a systematic review of 9 studies involving 189 patients (193 hips), outlined the common causes, diagnostic characteristics, treatment approaches, and outcomes for hip micro-instability. The most frequently reported symptom was anterior hip pain, while physical examination commonly revealed pain during extension and external rotation of the hip. With appropriate treatment tailored to the underlying cause, patients typically experience improved outcomes.
In a retrospective case series, Curtis et al. [27] examined the degree of distractibility in 464 patients undergoing hip arthroscopy, comparing those with and without micro-instability. They found that hip micro-instability, whether accompanied by FAI or not, correlated with reduced axial traction required for hip distraction. Patients with isolated micro-instability needed a median of 6.9 rotations, those with instability and FAI required 8.8 rotations, and patients with isolated FAI needed 19.1 rotations. These findings suggest that intraoperative ease of distraction may help identify patients with micro-instability of the hip. In another retrospective case series, Curtis et al. [28] investigated factors influencing the ease of hip distraction during arthroscopy in 453 patients. Univariate analysis revealed associations between sex, race, BMI, range of motion, hyperextension-external rotation (HEER) test, abduction-extension-external rotation test, and lateral center edge angle (LCEA) with the number of traction rotations required for distraction. Multivariable analysis showed that lower LCEA (p = 0.002), female sex (p < 0.001), and a positive HEER test (p = 0.045) were independently associated with fewer rotations needed for adequate distraction. Since easier distraction correlates with hip micro-instability, these findings could assist in preoperative identification, counseling, risk stratification, and planning for capsular management.
3.6. Bone Morphology of the Hip
In a retrospective cohort study, Kwon et al. [29] examined the relationship between acetabular labral tears and sagittal pelvic parameters in 365 patients (449 hips). They found that the pelvic incidence was significantly higher in the labral tear group compared to the non-labral tear group (52.3° vs. 47.1°). After adjusting for potential confounders, older age, FAI, and high pelvic incidence were independently associated with acetabular labral tears. When analyzing only patients without FAI (308 hips), they found that higher age and high pelvic incidence were independently associated with acetabular labral tears. These findings suggest that acetabular labral tears are linked to high pelvic incidence, regardless of FAI morphology. In a retrospective case series of 133 patients (138 hips), Huang et al. [30] explored the connection between capsular stiffness and acetabular coverage by evaluating the distension of the anterior and posterior joint recesses using hip CT arthrography. They observed significantly greater posterior capsule distension in acetabular dysplasia. A significant, albeit weak, negative correlation was also found between posterior and anterior capsule distension, indicating that a looser posterior capsule is present in dysplastic hips. Curley et al. [31] conducted a systematic review of 7 studies involving 151 hips (148 patients) to evaluate the outcomes of periacetabular osteotomy following failed hip arthroscopy. The review found that periacetabular osteotomy after failed hip arthroscopy was performed in a diverse patient population, frequently including hips with moderate to severe dysplasia and minimal osteoarthritis. Regardless of hip morphology or accompanying procedures, all studies reporting postoperative outcomes showed significant improvements in PROMs after the periacetabular osteotomy.
3.7. Expectation and Outcome After Hip Arthroscopy
In a retrospective case series, Yin et al. [32] explored the connection between muscle volume, LCEA, alpha angle (AA), BMI, and Beighton score with stiffness coefficient in 36 patients, assessing how varying physical conditions of the hip joint capsule impact traction force. Findings revealed that hip joint capsule condition affects traction force and that muscle volume, more so than BMI, serves as a reliable indicator for estimating preoperative traction force. LCEA has been shown to influence traction, unlike AA and Beighton scores. Muscle volume measurements could aid in determining the optimal traction force for individual patients. In a prospective case series involving 69 patients, Factor et al. [33] examined the expectations of patients undergoing hip arthroscopy and the association of these expectations with patient-reported outcome measures (PROMs) and satisfaction, utilizing machine learning (ML) algorithms. The results showed that violations of patient expectations significantly predict PROMs and patient satisfaction and are linked to patients’ willingness to consider repeat surgery. In a review study, Martin et al. [34] analyzed data from 5581 patients in the DHAR database to evaluate whether ML could develop a clinically useful tool for forecasting the likelihood of revision surgery after an initial hip arthroscopy. The ML analysis produced a model that moderately predicted revision surgery risk following primary hip arthroscopy; however, its clinical applicability may be limited despite considering all available factors in the registry. In an RCT, Degen et al. [35] assessed 132 patients to determine if different multimodal analgesia regimens could lower pain scores postoperatively, costs, length of hospital stay, and opioid consumption after hip arthroscopy. The findings indicated that the routine administration of celecoxib, zopiclone, and gabapentin did not significantly enhance postoperative pain management or shorten hospital stay, suggesting these medications are not advisable for standard postoperative pain management following hip arthroscopy.
3.8. Groin Pain in Athletes
In a scoping review of 35 studies covering 1655 ballet dancers, Singh et al. [36] investigated whether ballet dancers exhibit a higher prevalence of hip morphology abnormalities and injury-related pathologies compared to the general population, as well as any specific risk factors contributing to an increased rate of hip injuries. The review suggests that ballet dancers experience elevated rates of chondro-labral damage and hip degeneration. Unlike other sports, intra-articular lesions in ballet are often located in the postero-superior hip region. In a prospective cohort study including 462 soccer players, Sonesson et al. [37] analyzed injury prevalence, patterns, and baseline risk factors in adolescent and adult amateur soccer players of both sexes. Male players reported 95 injuries (totaling 262 injury weeks, with a weekly prevalence of 18.0% (95% CI 16.1–20.1)), while female players reported 350 injuries (totaling 1206 injury weeks, with a weekly prevalence of 23.9% (95% CI 22.8–25.1)). Gradual-onset injuries comprised 57% of male injuries and 66% of female injuries. For men, the most frequent substantial injuries were in the hip/groin (weekly prevalence of 3.8%), ankle (2.1%), posterior thigh (2.0%), and knee (2.0%), while in women, these were in the knee (4.3%), ankle (2.5%), and lower leg/Achilles tendon (2.0%). Significant injury risk factors included older age (rate ratio for men 1.05 per year increase (95% CI 1.02–1.08), women 1.03 (95% CI 1.01–1.05)) and pre-existing injuries at the start of the season (men 1.92 (95% CI 1.27–2.89), women 1.58 (95% CI 1.19–2.09)). On average, one in five male and one in four female amateur players reported new or ongoing injuries weekly. Hip/groin injuries were more prevalent among males, while females had a higher incidence of knee injuries. Older players and those with prior injuries were more likely to sustain new injuries during the season, emphasizing the importance of addressing pre-season injuries to reduce injury risk in amateur soccer. In a cross-sectional study, Mercurio et al. [38] examined the seasonal prevalence of groin pain and average time lost per injury in 600 team sport athletes. Groin pain was reported by up to one in four team sport athletes over a season, with the highest prevalence among soccer players (32.5%), followed by futsal (25.5%), basketball (25.2%), water polo (17.6%), and volleyball players (13.6%). Professional players in soccer, futsal, and basketball reported higher groin pain rates than non-professional athletes (p = 0.02, p = 0.005, and p = 0.004, respectively). Average time lost due to groin pain was 60.3 ± 66 days in soccer, 41.1 ± 16.6 days in futsal, 31.5 ± 18 days in water polo, 37.2 ± 14.2 days in basketball, and 50.8 ± 24.6 days in volleyball. The Copenhagen Hip and Groin Outcome Score (HAGOS) appears to be an effective tool for assessing groin pain, correlating with both sports absence duration and coexisting injuries among athletes.
3.9. Tendon Injuries and Soft Tissue Procedures Around the Hip
In a retrospective case series involving 10 patients (11 injuries), Aujla et al. [39] assessed RTS outcomes and re-injury rates after surgical repair of first-time, high-grade, intramuscular hamstring tendon injuries in elite athletes. The surgical repair of these high-grade intramuscular biceps femoris tendon injuries led to a high RTS rate, with athletes resuming pre-injury activity on average within 3.1 ± 1.0 months, and no cases of re-injury were reported. Given these findings, the intramuscular tendon should be evaluated when diagnosing hamstring injuries in elite athletes, and surgery should be considered for high-grade cases. Ekstrand et al. [40], in a retrospective case series, investigated perceptions of risk factors for hamstring injuries and compared these perceptions across teams with varying hamstring injury rates. Findings indicated that most hamstring injury risk factors are extrinsic, linked to the club, team, and coaching practices rather than the players themselves. In another retrospective case series, Ebert et al. [41] examined clinical outcomes, patient satisfaction, re-injury, and re-operation rates in 146 patients 7–10 years post-augmented hip abductor tendon repair. Results showed favorable clinical outcomes, high patient satisfaction, and an acceptable re-injury rate, indicating that this repair approach generally maintains effectiveness over time. In a series of 22 patients, Della Rocca et al. [42] reported on mid-term follow-up outcomes following endoscopic gluteus medius repair combined with systematic gluteus maximus tendon release. Patient feedback was largely positive, with 11 (50%) rating the outcome as excellent, 7 (32%) as good, and 2 (9%) each as fair and poor. In an experimental study, Coulomb et al. [43] compared an ultrasound-guided iliotibial band release method to a similar endoscopic approach in 10 cadavers (20 hips). Results suggested that the ultrasound-guided technique is comparable in safety and effectiveness to the endoscopic technique, with a shorter operative time (average of 12.3 ± 6.0 min) for ultrasound-trained surgeons and lower disposable costs than the endoscopic method, which had an operative time of 21.0 ± 10.7 min (p = 0.04).
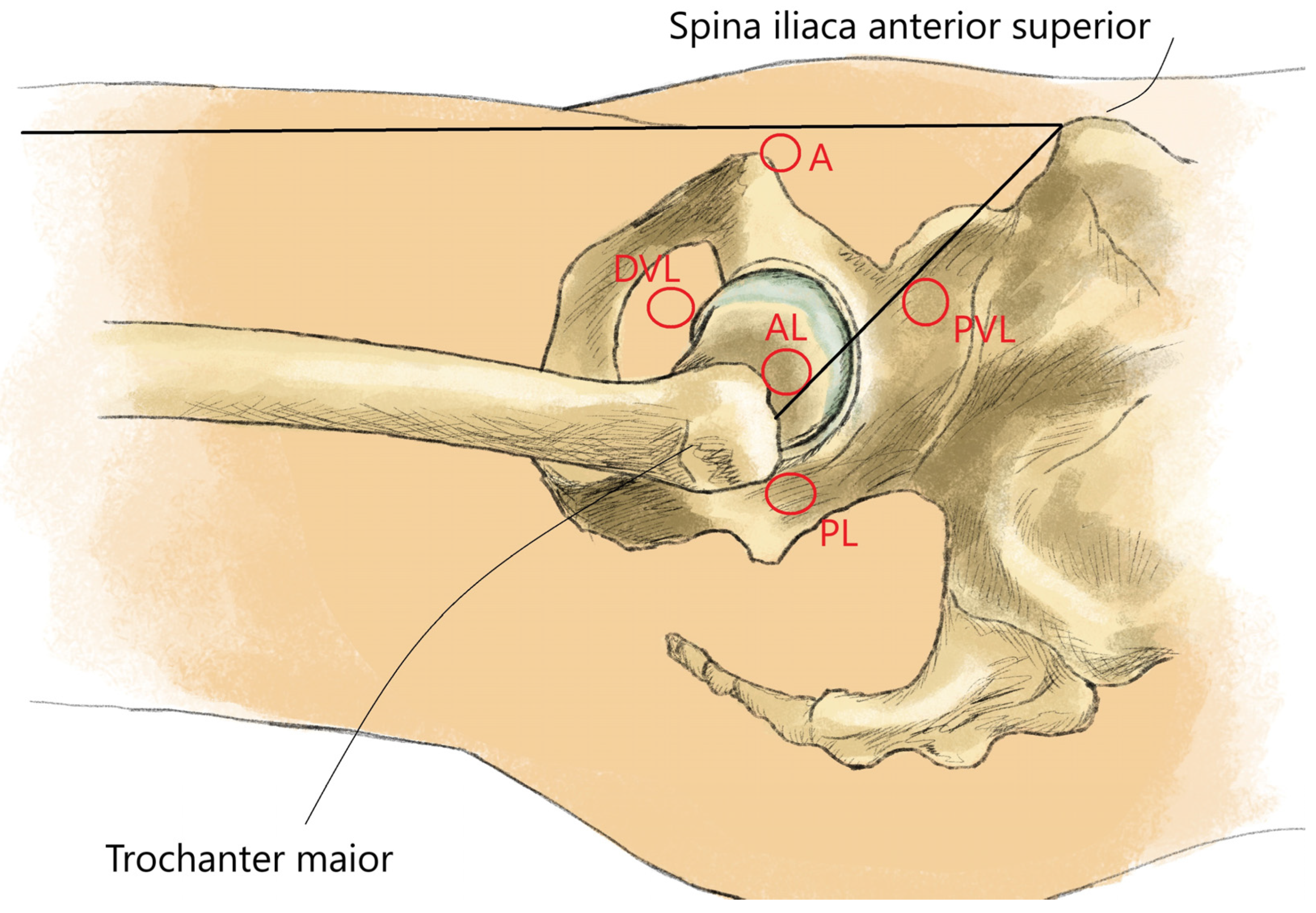
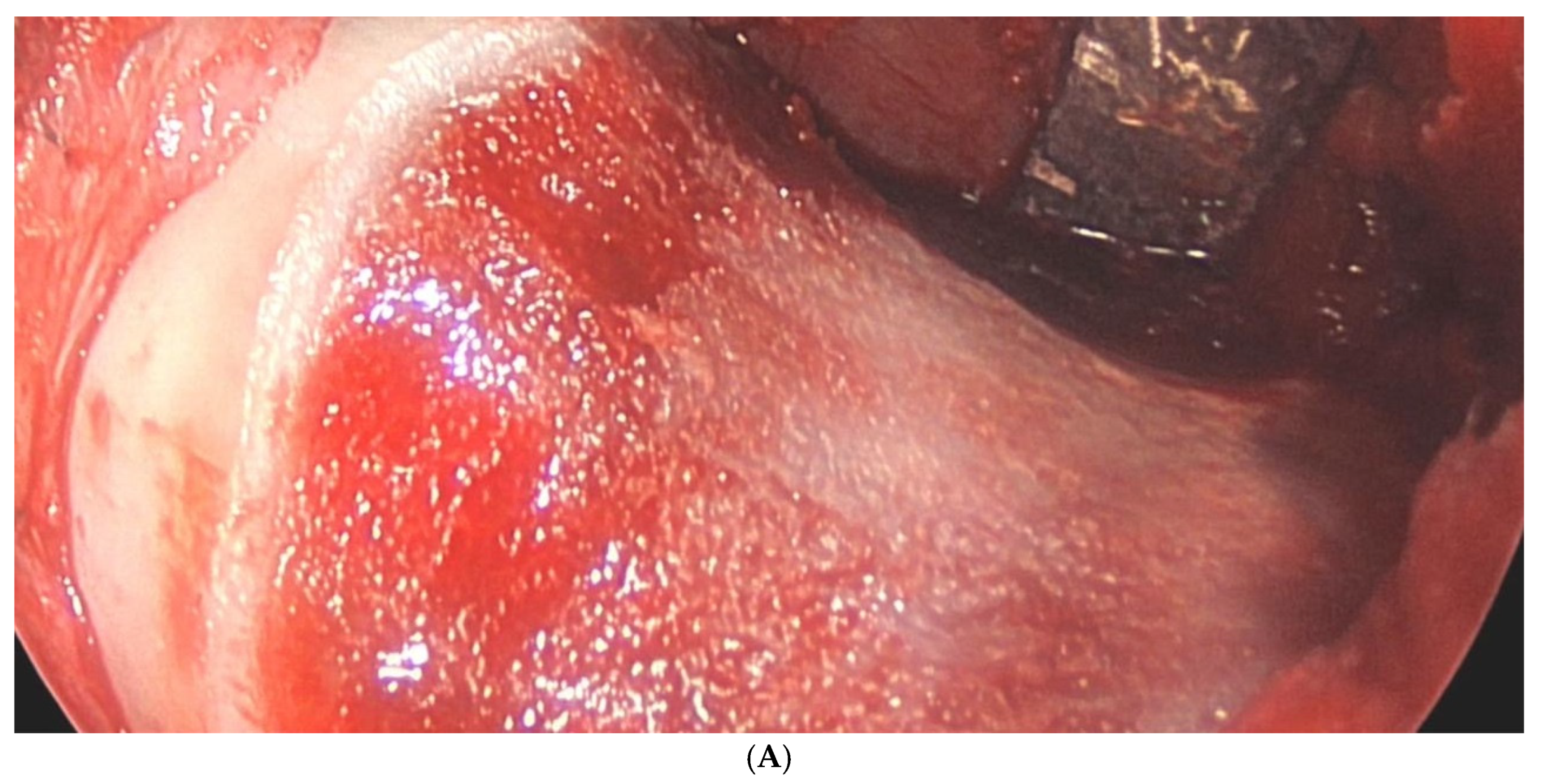
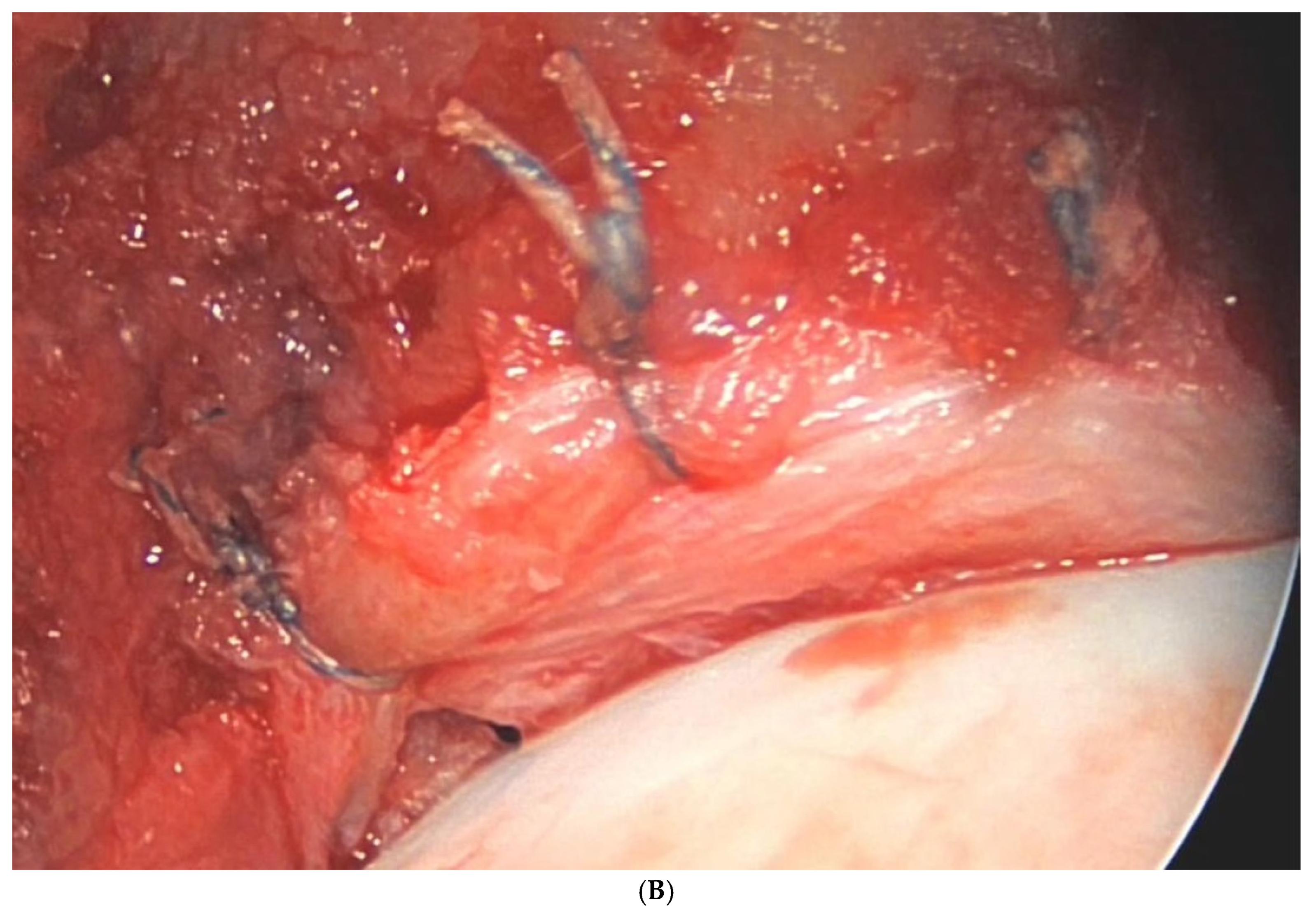
The main results of each included primary study [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] are summarized in Table 6. Figure 3 shows the arthroscopic portals to the hip joint (Figure 3). Figure 4 shows intraoperative photographs of FAI surgery (Figure 4A,B).
Table 6.
Summary of main findings.
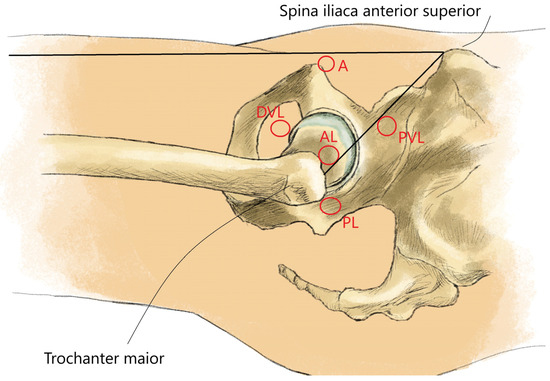
Figure 3.
Arthroscopic portals to the hip joint. A: anterior portal; AL: anterolateral portal; DVL: distal ventrolateral portal; PL: posterolateral portal; PVL: proximal ventrolateral portal.
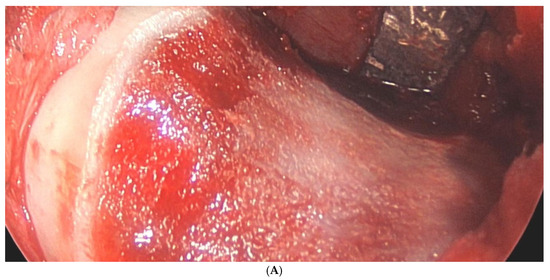
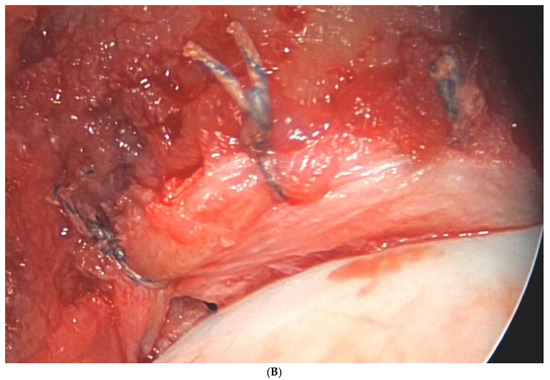
Figure 4.
(A) Intraoperative photograph of a femoral neck after cam resection. (B) Intraoperative photograph of a labral refixation.
4. Discussion
4.1. Femoroacetabular Impingement (FAI)
The management of femoroacetabular impingement (FAI) has undergone significant evolution over the past decade, shaped by emerging research, technological advancements, and a growing understanding of hip anatomy and biomechanics. A key factor in this evolution has been the shift from open surgery to minimally invasive approaches, which prioritize patient recovery and reduce surgical trauma. While hip arthroscopy has become a cornerstone treatment modality, the interplay between surgical and non-operative strategies, as well as the influence of patient expectations and anatomical considerations, invites a nuanced discussion on optimizing care. Recent studies reinforce the effectiveness of hip arthroscopy in treating FAI, demonstrating significant improvements in PROMs post-surgery. Holleyman et al. [12] provided compelling evidence of sustained benefits through 12 months, affirming the role of arthroscopy as a first-line intervention for symptomatic FAI. This evidence is in line with the wider trend towards using less invasive procedures for earlier intervention, with the aim of delaying or preventing severe degenerative changes that would require more invasive surgery. However, the findings of Abdel Khalik et al. [13] raise critical questions regarding the quality and geographical distribution of evidence. The concentration of high-quality RCTs in the USA and Europe suggests a need for broader, multicentric studies that include diverse populations to ensure the generalizability of results. Additionally, the exploration of capsular management strategies, as indicated by Cohen et al. [14], highlights the complexity of surgical techniques in influencing outcomes. This complexity is compounded by variations in surgical experience and equipment, which can lead to differences in patient outcomes between healthcare settings. The improved postoperative HHS following interportal capsulotomy closure reflects the significance of the meticulous surgical practice. This leads to a broader implication: as surgical techniques evolve, the need for standardized protocols becomes paramount to maximize patient outcomes across different settings.
While surgical options dominate discussions surrounding FAI, non-operative management should not be overlooked. Andronic et al. [17] highlighted the potential of physiotherapy and conservative measures to delay surgical intervention, particularly in early-stage FAI. These non-surgical options offer a way forward for patients who are not ideal surgical candidates or who prefer conservative approaches. This is especially relevant given the increasing recognition of the importance of a tailored, multidisciplinary approach to care. Non-operative strategies can serve as essential adjuncts, enabling patients to maintain function and quality of life while mitigating symptoms. However, the absence of evidence supporting non-operative outcomes in patients with Tönnis grade 2 or higher degenerative changes raises concerns about the appropriate timing and selection of interventions. Identifying thresholds for surgical intervention could prevent unnecessary procedures while still effectively treating progressive symptoms. Further research is warranted to delineate the threshold at which surgical intervention becomes necessary, particularly in the context of degenerative changes.
In summary, the management of FAI is at a pivotal juncture, characterized by a blend of surgical innovation, a renewed focus on non-operative interventions, and a deeper appreciation for patient-centered care. This multidimensional approach requires collaboration between surgical, rehabilitation, and research disciplines to ensure that patients receive optimal treatment at each stage of FAI progression. While hip arthroscopy remains a vital component of treatment, the complex interplay of factors influencing outcomes necessitates a comprehensive approach that integrates anatomical insights, patient expectations, and evidence-based practices. Continued research and collaboration across disciplines will be essential to refine treatment strategies, enhance patient outcomes, and ultimately advance the field of hip arthroscopy for FAI.
4.2. Micro-Instability of the Hip
Hip micro-instability has gained recognition as a distinct clinical entity, yet its complexity poses challenges in diagnosis and management. Recent studies underscore that this condition, characterized by symptoms such as anterior hip pain and mechanical instability, requires a multifaceted approach for effective treatment. Cohen et al. [26] highlighted anterior hip pain as the hallmark symptom of micro-instability. This symptom profile highlights the delicate balance between stability and mobility in the hip joint, which is easily disturbed by even minor structural changes. This pain, often exacerbated during hip extension and external rotation, reflects the dynamic nature of the hip joint and the strain placed on its soft tissues. However, the overlap of symptoms with other hip conditions, such as femoroacetabular impingement (FAI), complicates diagnosis. The study by Khanduja et al. [25] emphasizes the difficulty clinicians face in establishing a definitive diagnosis, pointing to the need for a consensus on diagnostic criteria. A more standardized framework would help differentiate micro-instability from other disorders, facilitating timely and appropriate intervention. Such standardization is critical because the effectiveness of treatment often depends on accurate early diagnosis. The diversity in treatment options for hip micro-instability reflects the condition’s multifactorial nature. Curtis et al. found in two different studies [27,28] that the degree of distractability during hip arthroscopy can serve as an indicator of micro-instability. In clinical practice, this intra-operative assessment could guide surgeons in real-time, allowing for tailored treatment modifications based on joint laxity. This insight is significant because it suggests that intraoperative assessment can guide surgical decision-making, allowing for tailored interventions. The importance of identifying the underlying cause of micro-instability cannot be overstated, as appropriate treatment based on etiology is crucial for optimizing outcomes.
The implications of hip micro-instability are particularly pronounced in specific athletic populations, as shown in the scoping review of ballet dancers by Singh et al. [36]. This group experiences a higher prevalence of chondrolabral damage, highlighting the need for targeted injury prevention strategies. The physical demands of ballet often lead to increased stress on the hip joint, suggesting that specific training regimens may be necessary to mitigate the risk of developing micro-instability and related pathologies. The complexity of diagnosing and treating hip micro-instability emphasizes the need for ongoing research. Establishing clear diagnostic protocols, as advocated by Khanduja et al. [25], will enhance clinician confidence in identifying this condition. Moreover, further studies examining the long-term outcomes of various treatment strategies, including the role of conservative management, are essential to inform best practices.
In summary, hip micro-instability is a multifaceted condition that necessitates a comprehensive understanding of its clinical presentation, underlying causes, and the effectiveness of various treatment modalities. As research progresses, the refinement of diagnostic criteria and the exploration of tailored interventions will be vital in improving patient outcomes and quality of life.
4.3. Bone Morphology of the Hip
A nuanced understanding of hip anatomy is critical for optimizing surgical outcomes. Variations in bone morphology, even within a small cohort of patients, can have a significant impact on both surgical planning and patient outcomes, highlighting the need for individualized approaches. The associations found by Kwon et al. [29] and Yang et al. [22] between pelvic parameters, femoral neck-shaft angle, and surgical outcomes underscore the importance of preoperative imaging and assessment. Accurate preoperative assessment is particularly important in complex cases, where even small variations in bone structure can affect joint stability and mobility. These anatomical considerations can inform surgical planning and technique, particularly in complex cases involving dysplasia or concomitant conditions. The findings from Yin et al. [32] regarding muscle volume as a predictor of traction force introduce an intriguing dimension to preoperative evaluations. As the physical properties of the hip joint capsule influence the surgical approach, integrating advanced imaging and biomechanical assessments into routine practice could enhance surgical precision and outcomes. Furthermore, the findings of Curley et al. [31] regarding periacetabular osteotomy following failed hip arthroscopy illustrate that even in challenging cases, surgical intervention can yield positive results. This adaptability highlights the need for a flexible approach to complex cases, allowing surgeons to pivot when standard techniques may not be sufficient. This is particularly relevant for patients with varying hip morphologies, as it suggests that adaptability in surgical techniques is necessary to address the unique needs of each patient. Improved PROMs following such procedures indicate that, despite previous treatment failures, patients can achieve significant functional recovery.
4.4. Expectation and Outcome After Hip Arthroscopy
The influence of patient expectations on surgical outcomes is a growing area of interest. Patients with high expectations of recovery are more likely to comply with postoperative guidelines, suggesting that expectation management may improve the quality of recovery. Factor et al. [33] demonstrated that unmet expectations correlate with lower satisfaction rates, underscoring the necessity for comprehensive preoperative counseling. This discussion highlights a shift towards patient-centered care, where aligning surgical goals with individual patient expectations is crucial. Aligning these goals may also reduce the risk of revision surgery, as patients with realistic expectations may be less likely to seek additional procedures. Understanding patient psychology and communication strategies could play a pivotal role in enhancing satisfaction and reducing the rates of revision surgeries. Factor et al. [33] utilized ML algorithms to investigate the relationship between patient expectations and postoperative outcomes. Their findings revealed that expectation violation significantly impacts PROMs and satisfaction. This suggests that managing patient expectations could play a crucial role in enhancing satisfaction and reducing the likelihood of repeat surgeries. Furthermore, Martin et al. [34] explored ML applications in predicting revision surgery risks using data from the DHAR. While their model showed moderate accuracy, it highlights the potential of ML to inform clinical decision-making. ML’s potential to predict outcomes based on patient expectations, demographics, and procedural data could enable highly personalized patient care in the future. However, the limited clinical utility calls for further refinement and validation to ensure practical applications in everyday clinical settings. Together, these studies emphasize the growing importance of ML in improving surgical training and enhancing patient-centered care in hip arthroscopy.
4.5. Groin Pain in Athletes
The results of the three studies highlight important patterns in injury prevalence and risk factors in different sports, reflecting the complex interplay between sport-specific demands and athlete health. Each sport presents unique biomechanical challenges, making groin pain a common yet complex symptom to manage. Firstly, the higher incidence of hip injuries in ballet dancers, particularly in relation to chondrolabral damage, suggests that the unique biomechanics of ballet—such as extreme ranges of motion and repetitive loading—may predispose dancers to specific pathologies. This raises questions about the adequacy of current training and rehabilitation practices in ballet and suggests a potential need for specific interventions that address these unique risk factors. In football, the differentiation in injury patterns between the sexes provides an opportunity for targeted injury prevention programs. The fact that older athletes and those with a history of previous injury are at higher risk highlights the importance of comprehensive pre-season assessment. Such assessments may need to include basic strength and flexibility tests to better understand individual susceptibility to groin injury. Integrating strength and conditioning programs that focus on injury prevention, particularly in the hip and knee regions, may help to reduce these risks. Mercurio et al.’s [38] findings on the prevalence of groin pain in different team sports add another layer, highlighting the common vulnerabilities of athletes involved in high-intensity, dynamic movements. The correlation between time lost due to groin pain and the use of the HAGOS tool highlights the need for standardized assessments in injury management. The adoption of standardized assessment tools across sports could provide more accurate data for tracking and managing groin pain. Taken together, these studies highlight the need for a multifaceted approach to injury prevention and rehabilitation that takes into account the unique physical demands of each sport and individual athlete profile to optimize health and performance outcomes. Integrating the evidence from these studies into practice could improve the longevity and overall well-being of athletes in different sports.
4.6. Tendon Injuries and Soft Tissue Procedures Around the Hip
Hamstring and gluteal ruptures are prevalent injuries among athletes, and recent findings shed light on their management and recovery outcomes. These injuries often pose a risk of long-term functional limitations if not managed promptly and effectively. Aujla et al. [39] demonstrated that surgical repair of high-grade intramuscular tendon injuries in elite athletes results in excellent return-to-sport rates without re-injury. This highlights the critical need for accurate assessment of intramuscular tendon involvement, as misclassification could lead to suboptimal treatment strategies. The study advocates for surgical intervention in high-grade cases, suggesting that early and appropriate surgical repair may mitigate long-term complications and facilitate a quicker return to competitive performance. This emphasis on early surgical intervention reflects the high functional demands placed on elite athletes. The work of Della Rocca et al. [42] complements this by presenting the Polesello technique for endoscopic gluteus medius repair. This approach not only addresses full-thickness tears effectively but also integrates systematic release of the gluteus maximus, reflecting an evolving understanding of tendon dynamics. Techniques such as these are essential in restoring function and preventing secondary complications. Such surgical techniques are essential for restoring function and may influence long-term outcomes by preserving the integrity of surrounding structures. Ebert et al. [41] provide a longitudinal perspective by evaluating outcomes seven to ten years post-augmented hip abductor tendon repair. The durability of surgical interventions is crucial for patient satisfaction and overall quality of life. Their findings indicate that satisfactory outcomes can be maintained over time, reinforcing the idea that effective surgical management can lead to lasting improvements in function and well-being. The long-term success demonstrated by these results may help to justify surgery over conservative management in certain cases. Coulomb et al. [43] examined the efficacy of an ultrasound-guided iliotibial band release technique compared to a similar endoscopic method. Their experimental study revealed that the ultrasound-guided approach is not only effective but also offers the advantage of lower disposable costs and reasonable operative times for trained surgeons. This finding is particularly relevant in the context of gluteal injuries, as iliotibial band tightness can contribute to hip dysfunction. By providing an effective and cost-efficient alternative, this technique could enhance surgical options available to clinicians. Having low-cost options can widen access to patients who may not be able to afford more expensive procedures. Finally, the study by Ekstrand et al. [40] underscores the extrinsic risk factors associated with hamstring injuries, emphasizing the role of team dynamics, coaching strategies, and training environments over individual athlete characteristics. This broader perspective encourages a more holistic approach to injury prevention, where interventions can be tailored not only to the athlete but also to the organizational context.
In summary, the management of hamstring and gluteal ruptures requires a nuanced understanding of both surgical and non-surgical options. By considering individual and team-level factors, clinicians can develop more robust injury prevention programs tailored to different athlete populations. By integrating insights from these studies, clinicians can adopt a more personalized approach to treatment, balancing the benefits of surgical repair with the potential for successful conservative management, ultimately enhancing recovery outcomes for athletes across various demographics. Continued research is essential to refine these strategies and develop comprehensive protocols that address both the immediate and long-term needs of this patient population.
5. Conclusions
This narrative review of primary studies published in the journal KSSTA in 2022 and 2023 summarized the results of 33 studies on hip conditions, particularly FAI. Based on the evidence reviewed, hip arthroscopy remains an effective treatment for FAI, with promising early outcomes, particularly when combined with closed capsular repair and appropriate postoperative rehabilitation strategies. It is recommended that surgeons adapt their approach to capsular management to improve postoperative outcomes, as studies suggest that closed capsular repair may improve functional recovery. In addition, preoperative assessment tools such as the HAR Index should be used to identify patients at higher risk of requiring hip arthroplasty after hip arthroscopy. In summary, the conclusions of the included primary studies align with current general recommendations and contribute valuable insights to the field of hip orthopedics.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/surgeries5040089/s1, Table S1: Raw data extraction set.
Author Contributions
Conceptualization: N.R. and R.P.; Methodology: N.R. and M.V.; Software: N.R.; Validation: N.R. and R.P.; Formal analysis: N.R. and J.L.; Investigation: N.R. and M.V.; Resources: N.R.; Data curation: N.R. and M.V.; Writing—original draft preparation: N.R.; Writing—review and editing: R.B., A.K. and K.K.; Visualization: N.R.; Supervision: R.B.; Project administration: N.R. and R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable as this is a narrative review.
Informed Consent Statement
Not applicable as this is a narrative review.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| 3D | three-dimensional |
| AA | alpha angle |
| AMSTAR 2 | A Measurement Tool to Assess Systematic Reviews |
| BMI | body mass index |
| CI | confidence interval |
| CT | computed tomography |
| COVID-19 | Coronavirus disease 2019 |
| DAA | direct anterior approaches |
| DHAR | Danish Hip Arthroscopy Registry |
| ERAS | enhanced recovery after surgery |
| ESSKA | European Society of Sports Traumatology, Knee Surgery and Arthroscopy |
| HAGOS | Copenhagen Hip and Groin Outcome Score |
| HAR Index | Hip Arthroplasty Risk Index |
| HHS | Harris Hip Score |
| HEER | hyperextension-external rotation |
| HOS | Hip Outcome Score |
| IQR | interquartile range |
| KSSTA | Knee Surgery, Sports Traumatology, Arthroscopy |
| LCEA | lateral center edge angle |
| ML | machine learning |
| MCID | minimal clinically important difference |
| MRI | magnetic resonance imaging |
| NAHR | Non-Arthroplasty Hip Registry |
| NAHS | Non-Arthritic Hip Score |
| NSA | neck-shaft angle |
| NSAIDs | non-steroidal anti-inflammatory drugs |
| PASS | Patient Acceptable Symptom State |
| PROM | patient-reported outcome measure |
| PROMIS | Patient-Reported Outcomes Measurement Information System |
| PRP | platelet-rich plasma |
| OR | odds ratio |
| RTS | return to sport |
| RoB | risk of bias |
| ROBINS-I | Risk of Bias in Non-Randomized Studies of Interventions |
| ROC curve | receiver-operating characteristic curve |
| SCB | Substantial Clinical Benefit |
| THA | total hip arthroplasty |
| UK | United Kingdom |
| USA | United States of America |
| WOMAC | Western Ontario and McMaster Universities Osteoarthritis Index |
References
- Blakeney, W.G.; Kuster, M. Advances in Hip Replacement Surgery. J. Clin. Med. 2023, 12, 3439. [Google Scholar] [CrossRef] [PubMed]
- Dhanwal, D.K.; Dennison, E.M.; Harvey, N.C.; Cooper, C. Epidemiology of Hip Fracture: Worldwide Geographic Variation. Indian J. Orthop. 2011, 45, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Kyin, C.; Maldonado, D.R.; Go, C.C.; Shapira, J.; Lall, A.C.; Domb, B.G. Mid- to Long-Term Outcomes of Hip Arthroscopy: A Systematic Review. Arthroscopy 2021, 37, 1011–1025. [Google Scholar] [CrossRef] [PubMed]
- Addai, D.; Zarkos, J.; Pettit, M.; Sunil Kumar, K.H.; Khanduja, V. Outcomes Following Surgical Management of Femoroacetabular Impingement: A Systematic Review and Meta-Analysis of Different Surgical Techniques. Bone Jt. Res. 2021, 10, 574–590. [Google Scholar] [CrossRef] [PubMed]
- Ramadanov, N.; Bueschges, S.; Liu, K.; Lazaru, P.; Marintschev, I. Direct and Indirect Comparisons in Network Meta-Analysis of SuperPATH, Direct Anterior, and Posterior Approaches in Total Hip Arthroplasty. Sci. Rep. 2022, 12, 16778. [Google Scholar] [CrossRef]
- Mehta, N.; Chamberlin, P.; Marx, R.G.; Hidaka, C.; Ge, Y.; Nawabi, D.H.; Lyman, S. Defining the Learning Curve for Hip Arthroscopy: A Threshold Analysis of the Volume-Outcomes Relationship. Am. J. Sports Med. 2018, 46, 1284–1293. [Google Scholar] [CrossRef]
- Sukhera, J. Narrative Reviews in Medical Education: Key Steps for Researchers. J. Grad. Med. Educ. 2022, 14, 418–419. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Bai, H.; Fu, Y.Q.; Ayeni, O.R.; Yin, Q.F. The Anterior Hip Capsule Is Thinner in Dysplastic Hips: A Study Comparing Different Young Adult Hip Patients. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Holleyman, R.; Sohatee, M.A.; Lyman, S.; Malviya, A.; Khanduja, V.; NAHR User Group. Hip Arthroscopy for Femoroacetabular Impingement Is Associated with Significant Improvement in Early Patient-Reported Outcomes: Analysis of 4963 Cases from the UK Non-Arthroplasty Registry (NAHR) Dataset. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Abdel Khalik, H.; Lameire, D.L.; Park, L.J.; Ayeni, O.R. The Impact of Surgical Randomised Controlled Trials on the Management of FAI Syndrome: A Citation Analysis. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 6006–6019. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Comeau-Gauthier, M.; Khan, A.; Kay, J.; Slawaska-Eng, D.; Simunovic, N.; Ayeni, O.R. A higher proportion of patients may reach the MCID with capsular closure in patients undergoing arthroscopic surgery for femoroacetabular impingement: A systematic review and meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2425–2456. [Google Scholar] [CrossRef] [PubMed]
- Tahoun, M.F.; Lizano-Díez, X.; Soler, B.C.; Pons, M.T. Superior outcomes after arthroscopic treatment of femoroacetabular impingement and labral tears with closed versus open capsule. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 4501–4509. [Google Scholar] [CrossRef]
- George, T.; Curley, A.J.; Saeed, S.K.; Kuhns, B.D.; Parsa, A.; Domb, B.G. Orthobiologics as an adjunct in treatment of femoroacetabular impingement syndrome: Cell-based therapies facilitate improved postoperative outcomes in the setting of acetabular chondral lesions—A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 6020–6038. [Google Scholar] [CrossRef]
- Andronic, O.; Claydon-Mueller, L.S.; Cubberley, R.; Karczewski, D.; Lu, V.; Khanduja, V. No evidence exists on outcomes of non-operative management in patients with femoroacetabular impingement and concomitant Tönnis Grade 2 or more hip osteoarthritis: A scoping review. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2103–2122. [Google Scholar] [CrossRef]
- Dippmann, C.; Siersma, V.; Overgaard, S.; Krogsgaard, M.R. Acetabular retroversion does not affect outcome in primary hip arthroscopy for femoroacetabular impingement. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3535–3543. [Google Scholar] [CrossRef]
- Shankar, D.S.; Rao, N.; Colasanti, C.A.; Lan, R.; Essilfie, A.A.; Youm, T. Patients aged 50–75 years take longer to achieve the patient-acceptable symptom state than patients aged 20–34 years following primary hip arthroscopy for femoroacetabular impingement syndrome. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 4510–4518. [Google Scholar] [CrossRef]
- Seijas, R.; Barra-López, M.E.; López-de-Celis, C.; Laiz, P.; Ferré-Aniorte, A.; Barastegui, D.; Cugat, R. The HAR-index: A reliable method for evaluating the risk of total hip arthroplasty conversion after hip arthroscopy for femoroacetabular impingement. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2730–2738. [Google Scholar] [CrossRef]
- Zhu, X.M.; Toobaie, A.; Iansavichene, A.; Khan, M.; Degen, R.M. Improvement in pain and patient-related outcome measures following hip arthroscopy in patients with femoroacetabular impingement syndrome and concomitant generalized ligamentous laxity: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3907–3915. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Zhang, Z.; Zhang, X.; Huang, H.; Wang, J. Femoral neck-shaft angle can predict the anterior capsular thickness in patients with femoroacetabular impingement syndrome. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2716–2720. [Google Scholar] [CrossRef] [PubMed]
- Sjövall Anari, S.; Olsson, A.; Öhlin, A.; Desai, N.; Senorski, E.H.; Sansone, M.; Lindman, I. High-level soccer players have a low rate of return to performance after hip arthroscopy for femoroacetabular impingement syndrome. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2071–2078. [Google Scholar] [CrossRef] [PubMed]
- Marom, N.; Olsen, R.; Burger, J.A.; Dooley, M.S.; Coleman, S.H.; Ranawat, A.S.; Kelly, B.T.; Nawabi, D.H. Majority of competitive soccer players return to soccer following hip arthroscopy for femoroacetabular impingement: Female and older-aged players are less likely to return to soccer. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2721–2729. [Google Scholar] [CrossRef]
- Khanduja, V.; Darby, N.; O’Donnell, J.; Bonin, N.; Safran, M.R. International Microinstability Expert Panel. Diagnosing hip microinstability: An international consensus study using the Delphi methodology. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 40–49. [Google Scholar] [CrossRef]
- Cohen, D.; Jean, P.O.; Patel, M.; Aravinthan, N.; Simunovic, N.; Duong, A.; Safran, M.R.; Khanduja, V.; Ayeni, O.R. Hip microinstability diagnosis and management: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 16–32. [Google Scholar] [CrossRef]
- Curtis, D.M.; Pullen, W.M.; Murray, I.R.; Money, A.J.; Segovia, N.; Safran, M.R. Female gender, decreased lateral center edge angle, and a positive hyperextension-external rotation test are associated with ease of hip distractibility at the time of hip arthroscopy. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2188–2194. [Google Scholar] [CrossRef]
- Curtis, D.M.; Pullen, W.M.; Murray, I.R.; Money, A.; Safran, M. The diagnosis of hip microinstability is correlated with ease of intraoperative hip distraction. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 33–39. [Google Scholar] [CrossRef]
- Kwon, H.M.; Cho, B.W.; Kim, S.; Yang, I.H.; Park, K.K.; Son, N.H.; Lee, W.S. Acetabular labral tear is associated with high pelvic incidence with or without femoroacetabular impingement morphology. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3526–3534. [Google Scholar] [CrossRef]
- Huang, Y.Y.; Chen, I.J.; Wu, C.T.; Chan, Y.S.; Chen, D.W.; Tang, H.C. The Posterior Capsule Is Distended in Dysplastic Hips, but the Anterior Capsule Is Not. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 79–85. [Google Scholar] [CrossRef]
- Curley, A.J.; Engler, I.D.; Ruh, E.R.; Mauro, C.S.; McClincy, M.P. Periacetabular Osteotomy After Failed Hip Arthroscopy Demonstrates Improved Outcomes in a Heterogeneous Patient Population: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2090–2102. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Xue, S.; Zhang, X.; Yang, G.; Xu, Y.; Wang, J.; Huang, H. The Traction Force of the Pulled Limb in Hip Arthroscopic Surgery Is Determined by Stiffness Coefficient, Which Is Significantly Related to Muscle Volume. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2708–2715. [Google Scholar] [CrossRef] [PubMed]
- Factor, S.; Neuman, Y.; Vidra, M.; Shalom, M.; Lichtenstein, A.; Amar, E.; Rath, E. Violation of Expectations Is Correlated with Satisfaction Following Hip Arthroscopy. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2023–2029. [Google Scholar] [CrossRef]
- Martin, R.K.; Wastvedt, S.; Lange, J.; Pareek, A.; Wolfson, J.; Lund, B. Limited Clinical Utility of a Machine Learning Revision Prediction Model Based on a National Hip Arthroscopy Registry. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2079–2089. [Google Scholar] [CrossRef] [PubMed]
- Degen, R.M.; Firth, A.; Sehmbi, H.; Martindale, A.; Wanlin, S.; Chen, C.; Marsh, J.D.; Willits, K.; Bryant, D. Multimodal Analgesia Did Not Improve Post-Operative Pain Scores, Reduce Opioid Consumption, or Reduce Length of Stay Following Hip Arthroscopy. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 4016–4026. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.; Pettit, M.; El-Hakeem, O.; Elwood, R.; Norrish, A.; Audenaert, E.; Khanduja, V. Understanding Hip Pathology in Ballet Dancers. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3546–3562. [Google Scholar] [CrossRef]
- Sonesson, S.; Lindblom, H.; Hägglund, M. Higher Age and Present Injury at the Start of the Season Are Risk Factors for In-Season Injury in Amateur Male and Female Football Players: A Prospective Cohort Study. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 4618–4630. [Google Scholar] [CrossRef]
- Mercurio, M.; Corona, K.; Galasso, O.; Cerciello, S.; Morris, B.J.; Guerra, G.; Gasparini, G. Soccer Players Show the Highest Seasonal Groin Pain Prevalence and the Longest Time Loss from Sport Among 500 Athletes from Major Team Sports. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2149–2157. [Google Scholar] [CrossRef]
- Aujla, R.S.; Cecchi, S.; Koh, E.; D’Alessandro, P.; Annear, P. Surgical treatment of high-grade acute intramuscular hamstring tendon injuries in athletes leads to predictable return to sports and no re-injuries. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 4601–4606. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hallén, A.; Marin, V.; Gauffin, H. Most modifiable risk factors for hamstring muscle injury in women’s elite football are extrinsic and associated with the club, the team, and the coaching staff and not the players themselves: The UEFA Women’s Elite Club Injury Study. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2550–2555. [Google Scholar] [CrossRef]
- Ebert, J.R.; Jain, M.; Janes, G.C. Good clinical outcomes, a high level of patient satisfaction and an acceptable re-operation rate are observed 7–10 years after augmented hip abductor tendon repair. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2131–2139. [Google Scholar] [CrossRef] [PubMed]
- Della Rocca, F.; Di Francia, V.; Giuffrida, A.; Rosolani, M.; D’Ambrosi, R.; D’Addona, A. Satisfactory results after endoscopic gluteus medius repair combined with selective gluteus maximus reflected tendon release for the treatment of a full-thickness tear of gluteus medius. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2038–2045. [Google Scholar] [CrossRef] [PubMed]
- Coulomb, R.; Cascales, V.; Mares, O.; Bertrand, M.M.; Marchand, P.; Kouyoumdjian, P. A percutaneous ultrasound-guided iliotibial band release technique reduces surgical time and costs compared to an endoscopic technique. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2754–2761. [Google Scholar] [CrossRef] [PubMed]
- Cai, B.; Duan, S.; Yi, J.; Bay, B.H.; Huang, J.; Huang, W.; Hu, N.; Chen, C. A three-dimensional (3D) printed simulator as a feasible assessment tool for evaluating hip arthroscopy skills. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Efrima, B.; Amar, E.; Rotman, D.; Elias, A.; Ejnisman, L.; Bonin, N.; Albagli, A.; Benady, A.; Segal, O.; Rath, E. Inter- and intra-observer agreement of the 3-dimensional CT-based anterior inferior iliac spine classification system shows fair-to-moderate agreement among high-volume hip surgeons. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 50–57. [Google Scholar] [CrossRef]
- Hinz, M.; Lutter, C.; Mueller-Rath, R.; Niemeyer, P.; Miltner, O.; Tischer, T. The German Arthroscopy Registry DART: What has happened after 5 years? Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 102–109. [Google Scholar] [CrossRef]
- Jean, P.O.; Safran, M.R.; Ayeni, O.R. Hip microinstability: Fact or fiction? Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 1–3. [Google Scholar] [CrossRef]
- Kanakamedala, A.C.; Rynecki, N.D.; Mojica, E.S.; Markus, D.H.; Song, M.Y.; Gonzalez-Lomas, G.; Strauss, E.J.; Youm, T.; Jazrawi, L.M. No difference in clinical outcomes between operative and nonoperative management of minimally retracted proximal hamstring ruptures. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2739–2745. [Google Scholar] [CrossRef]
- Kaveeshwar, S.; Rocca, M.P.; Oster, B.A.; Schneider, M.B.; Tran, A.; Kolevar, M.P.; Adib, F.; Henn, M., III; Meredith, S.J. Depression and anxiety are associated with worse baseline function in hip arthroscopy patients. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3563–3569. [Google Scholar] [CrossRef]
- Kim, S.G.; Jun, J.B.; Bae, I.W.; Lee, D.H. Changes in ankle and hip joints following medial opening-wedge high tibial osteotomy affect knee joint line obliquity. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 5420–5427. [Google Scholar] [CrossRef]
- Matsumoto, T.; Nakano, N.; Ishida, K.; Maeda, T.; Tachibana, S.; Kuroda, Y.; Hayashi, S.; Matsushita, T.; Kuroda, R. Targeting the neutral hip-to-calcaneus axis in kinematically aligned total knee arthroplasty is feasible with fewer alignment outliers for varus osteoarthritic patients. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 3880–3888. [Google Scholar] [CrossRef] [PubMed]
- Mullins, K.; Filan, D.; Carton, P. High survivorship and excellent 5-year outcomes in patients older than 40 years undergoing arthroscopy for femoroacetabular impingement. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2123–2130. [Google Scholar] [CrossRef] [PubMed]
- Prill, R.; Królikowska, A.; de Girolamo, L.; Becker, R.; Karlsson, J. Checklists, risk of bias tools, and reporting guidelines for research in orthopedics, sports medicine, and rehabilitation. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 3029–3033. [Google Scholar] [CrossRef] [PubMed]
- Pullen, W.M.; Curtis, D.M.; Jamero, C.; Segovia, N.; Safran, M.R. Gadolinium injected concurrently with anesthetic can result in false-negative diagnostic intra-articular hip injections. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Schatz, C.; Leidl, R.; Plötz, W.; Bredow, K.; Buschner, P. Preoperative patients’ health decreases moderately, while hospital costs increase for hip and knee replacement due to the first COVID-19 lockdown in Germany. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3304–3310. [Google Scholar] [CrossRef]
- Sienko, A.; Ekhtiari, S.; Khanduja, V. The growth of hip preservation as a specialty. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 2540–2543. [Google Scholar] [CrossRef]
- Tarassoli, P.; Wood, J.A.; Chen, D.B.; Griffiths-Jones, W.; Bellemans, J.; MacDessi, S.J. Arithmetic hip-knee-ankle angle and stressed hip-knee-ankle angle: Equivalent methods for estimating constitutional lower limb alignment in kinematically aligned total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2980–2990. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).