
Posterior Spinal Fusion for Severe Kyphosis in a Child with Gaucher Disease: A Case Report and Review of the Literature

 ,
,
Abstract
1. Introduction
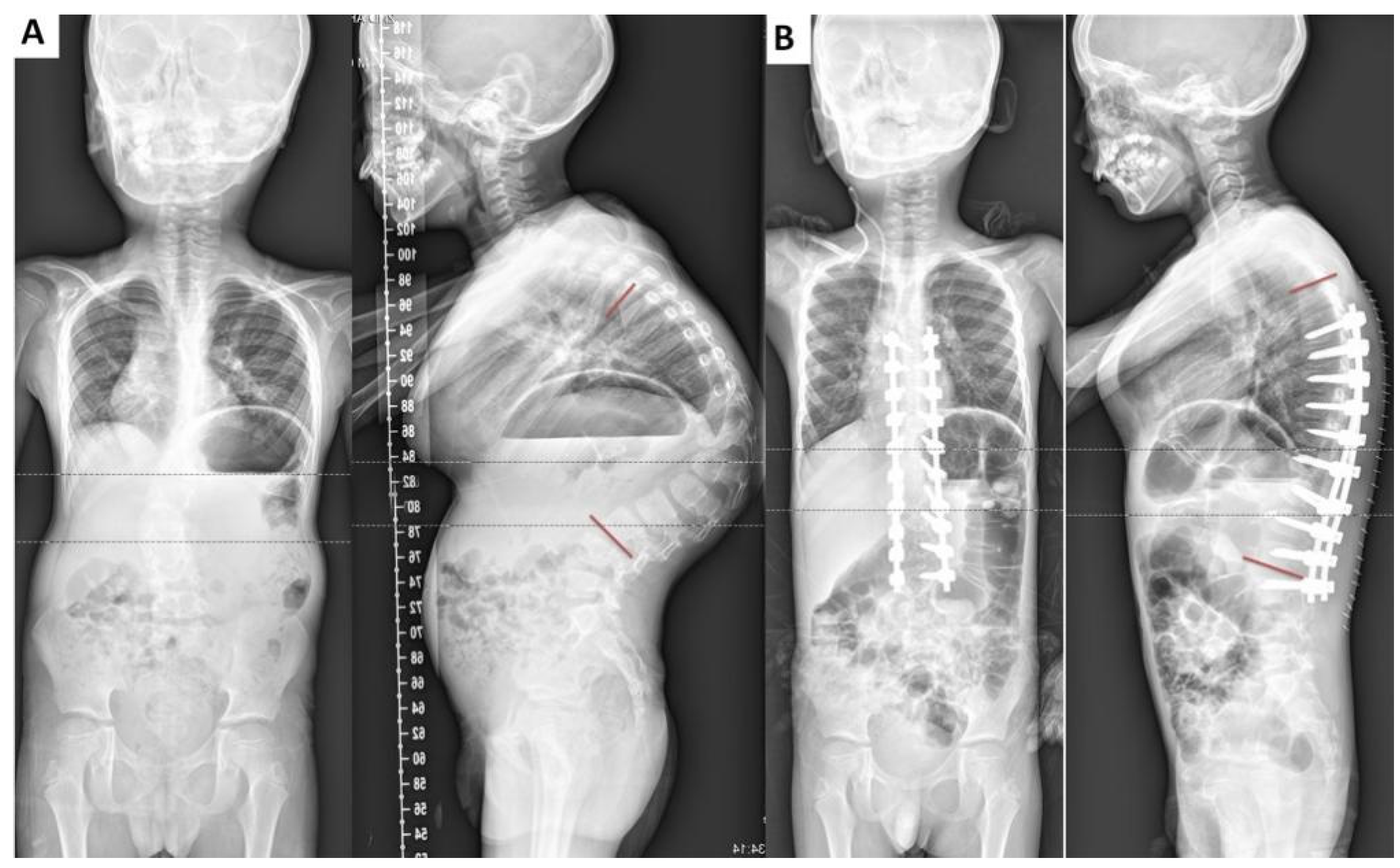
2. Case Presentation
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Report | Age (Years)/Sex | Disease Type | Presentation | Vertebrate Collapse (Site) | Complications | Treatment | Follow-Up | Outcome |
|---|---|---|---|---|---|---|---|---|
| Ruff et al., 1984 [10] | 12/F | Not available | Back pain | T11 | Progressive kyphosis of 64° | Anterior discectomies and T11 vertebrectomy, posterior spinal fusion of T8–L3 | Not available | Not available |
| Katz et al., 1993 [11] | 31/M | Not available | Back pain and lower extremity weakness | T12, L4 | Cord compression, hemorrhage | Laminectomy | 7 weeks | Died of gastric hemorrhage and bronchopneumonia |
| 17/M | Not available | Back pain | T5, T7, T12, L1–L5 | Kyphoscoliosis, cord compression | Brace, laminectomy, spinal fusion | Not available | Not available | |
| Kocher et al., 2000 [7] | 18/M | Type I | Lower extremity weakness and stumbling gait | T8–T12 | Cord compression and edema at the apex of the kyphosis | Anterior decompression and posterior fusion | 5 years | Good outcome |
| 11/M | Type 3 | Back pain and lower extremity weakness | Midthoracic spine | A thoracic kyphosis of ~120° and flattening of the cord | Anterior discectomies and fusion of T2–T11, posterior spinal fusion of T1–L3 | 19 months | Solid fusion with normal strength and sensation | |
| 13/M | Type 3 | Back pain | T6 and T10 | A thoracic kyphosis of 94° | Anterior discectomies and fusion of T8–L2, posterior spinal fusion of T5–L3 | 18 months | Maintenance of correction and solid fusion | |
| 15/F | Type 3 | Back pain | T5 and T10 | A thoracic kyphosis of 70° and slight cord impingement | Anterior discectomies and fusion of T8–T11, posterior spinal fusion of T2–L2 | 1 year | Good outcome and solid fusion | |
| Wiesner et al., 2003 [12] | 12/M | Type I | Back pain | T7–T9 | No complications | Ventral decompression with bone graft and fusion with TSRH(T5–L2) | 5 years | Good outcome |
| Ito et al., 2017 [17] | 10/F | Not available | Lower extremity weakness | No collapse | Kyphosis of 84° between T6 and L3 | T3–L3 posterior fusion with T12 osteotomy and anterior fusion from T12–L3 with bone grafts | 6 years | No progression of kyphosis, but suffered from fracture of limbs |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Goldblatt, J.; Sacks, S.; Beighton, P. The orthopedic aspects of Gaucher disease. Clin. Orthop. Relat. Res. 1978, 208–214. [Google Scholar] [CrossRef]
- Grabowski, G.A. Phenotype, diagnosis, and treatment of Gaucher’s disease. Lancet 2008, 372, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Erdos, M.; Hodanova, K.; Taskó, S.; Palicz, A.; Stolnaja, L.; Dvorakova, L.; Hrebicek, M.; Maródi, L. Genetic and clinical features of patients with Gaucher disease in Hungary. Blood Cells Mol. Dis. 2007, 39, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Abrahamov, A.; Elstein, D.; Gross-Tsur, V.; Farber, B.; Glaser, Y.; Hadas-Halpern, I.; Ronen, S.; Tafakjdi, M.; Horowitz, M.; Zimran, A. Gaucher’s disease variant characterised by progressive calcification of heart valves and unique genotype. Lancet 1995, 346, 1000–1003. [Google Scholar] [CrossRef] [PubMed]
- Patterson, M.C.; Horowitz, M.; Abel, R.B.; Currie, J.N.; Yu, K.T.; Kaneski, C.; Higgins, J.J.; O’Neill, R.R.; Fedio, P.; Pikus, A.; et al. Isolated horizontal supranuclear gaze palsy as a marker of severe systemic involvement in Gaucher’s disease. Neurology 1993, 43, 1993–1997. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.; Mikosch, P.; Belmatoug, N.; Carubbi, F.; Cox, T.; Goker-Alpan, O.; Kindmark, A.; Mistry, P.; Poll, L.; Weinreb, N.; et al. Gaucher Disease in Bone: From Pathophysiology to Practice. J. Bone Miner. Res. 2019, 34, 996–1013. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Hall, J.E. Surgical management of spinal involvement in children and adolescents with Gaucher’s disease. J. Pediatr. Orthop. 2000, 20, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, P.; Andersson, H.C.; Kacena, K.A.; Yee, J.D. The clinical and demographic characteristics of nonneuronopathic Gaucher disease in 887 children at diagnosis. Arch. Pediatr. Adolesc. Med. 2006, 160, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Stirnemann, J.; Belmatoug, N.; Camou, F.; Serratrice, C.; Froissart, R.; Caillaud, C.; Levade, T.; Astudillo, L.; Serratrice, J.; Brassier, A.; et al. A Review of Gaucher Disease Pathophysiology, Clinical Presentation and Treatments. Int. J. Mol. Sci. 2017, 18, 441. [Google Scholar] [CrossRef] [PubMed]
- Ruff, M.E.; Weis, L.D.; Kean, J.R. Acute thoracic kyphosis in Gaucher’s disease. A case report. Spine 1984, 9, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Katz, K.; Sabato, S.; Horev, G.; Cohen, I.J.; Yosipovitch, Z. Spinal involvement in children and adolescents with Gaucher disease. Spine 1993, 18, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, L.; Niggemeyer, O.; Kothe, R.; Meiss, L. Severe pathologic compression of three consecutive vertebrae in Gaucher’s disease: A case report and review of the literature. Eur. Spine J. 2003, 12, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.; Li, Y.; Yu, Z. Prevalence and Consequences of the Proximal Junctional Kyphosis after Spinal Deformity Surgery: A Meta-Analysis. Medicine 2016, 95, e3471. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Chen, Z.H.; Qiu, Y.; Zhu, Z.Z.; Li, S.; Xu, L.; Sun, X. Proximal Junctional Kyphosis after Posterior Spinal Instrumentation and Fusion in Young Children With Congenital Scoliosis: A Preliminary Report on its Incidence and Risk Factors. Spine 2017, 42, E1197–E1203. [Google Scholar] [CrossRef] [PubMed]
- Piantoni, L.; Remondino, R.G.; Tello, C.A.; Wilson, I.A.F.; Galaretto, E.; Noel, M.A. Proximal junction kyphosis after posterior spinal fusion for early-onset scoliosis. Spine Deform. 2020, 8, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Mika, A.P.; Mesfin, A.; Rubery, P.T.; Molinari, R.; Kebaish, K.M.; Menga, E.N. Proximal Junctional Kyphosis: A Pediatric and Adult Spinal Deformity Surgery Dilemma. JBJS Rev. 2019, 7, e4. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Kawakami, N.; Tsuji, T.; Ohara, T.; Saito, T.; Tauchi, R.; Morishita, K. Corrective surgery for kyphosis in a case of Gaucher’s disease without history of vertebral compression fractures. Spine Surg. Relat. Res. 2017, 1, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; King, A.B.; Boachie-Adjei, O. Incidence, risk factors, and natural course of proximal junctional kyphosis: Surgical outcomes review of adult idiopathic scoliosis. Minimum 5 years of follow-up. Spine 2012, 37, 1479–1489. [Google Scholar] [CrossRef] [PubMed]
- Messelodi, D.; Bertuccio, S.N.; Indio, V.; Strocchi, S.; Taddia, A.; Serravalle, S.; Bandini, J.; Astolfi, A.; Pession, A. iPSC-Derived Gaucher Macrophages Display Growth Impairment and Activation of Inflammation-Related Cell Death. Cells 2021, 10, 2822. [Google Scholar] [CrossRef] [PubMed]
- Kacher, Y.; Futerman, A.H. Impaired IL-10 transcription and release in animal models of Gaucher disease macrophages. Blood Cells Mol. Dis. 2009, 43, 134–137. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, T.; Zhang, N.; Chen, L.; Li, J.; Chen, Q.; Li, F. Posterior Spinal Fusion for Severe Kyphosis in a Child with Gaucher Disease: A Case Report and Review of the Literature. Surgeries 2024, 5, 619-626. https://doi.org/10.3390/surgeries5030049
Zhao T, Zhang N, Chen L, Li J, Chen Q, Li F. Posterior Spinal Fusion for Severe Kyphosis in a Child with Gaucher Disease: A Case Report and Review of the Literature. Surgeries. 2024; 5(3):619-626. https://doi.org/10.3390/surgeries5030049
Chicago/Turabian StyleZhao, Tengfei, Ning Zhang, Linwei Chen, Jun Li, Qixin Chen, and Fangcai Li. 2024. "Posterior Spinal Fusion for Severe Kyphosis in a Child with Gaucher Disease: A Case Report and Review of the Literature" Surgeries 5, no. 3: 619-626. https://doi.org/10.3390/surgeries5030049
APA StyleZhao, T., Zhang, N., Chen, L., Li, J., Chen, Q., & Li, F. (2024). Posterior Spinal Fusion for Severe Kyphosis in a Child with Gaucher Disease: A Case Report and Review of the Literature. Surgeries, 5(3), 619-626. https://doi.org/10.3390/surgeries5030049