
Will the Artificial Intelligence Touch Substitute for the Human Touch?


{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
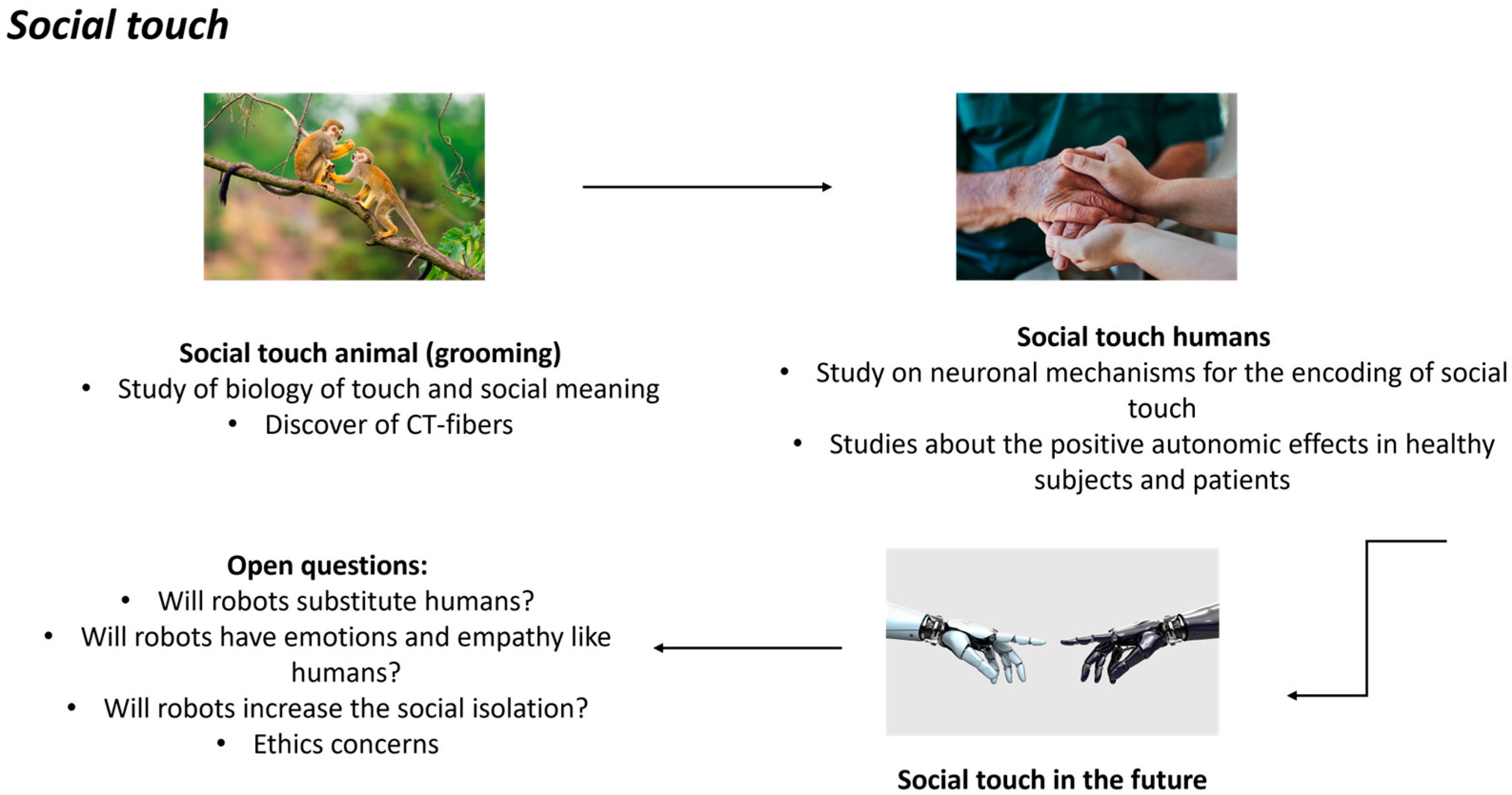
3.1. Social Touch
3.2. The Importance of Social Touch
3.3. Artificial Intelligence for Social Touch
3.4. Robots and Artificial Intelligence
3.5. Ethical Concerns of AI and Robots
4. Discussion
Funding
Acknowledgments
Conflicts of Interest
References
- Hertenstein, M.J.; Keltner, D.; App, B.; Bulleit, B.A.; Jaskolka, A.R. Touch communicates distinct emotions. Emotion 2006, 6, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Suvilehto, J.T.; Cekaite, A.; Morrison, I. The why, who and how of social touch. Nat. Rev. Psychol. 2023, 2, 606–621. [Google Scholar] [CrossRef]
- Castiello, U.; Becchio, C.; Zoia, S.; Nelini, C.; Sartori, L.; Blason, L.; D’Ottavio, G.; Bulgheroni, M.; Gallese, V. Wired to be social: The ontogeny of human interaction. PLoS ONE 2010, 5, e13199. [Google Scholar] [CrossRef] [PubMed]
- Gliga, T.; Farroni, T.; Cascio, C.J. Social touch: A new vista for developmental cognitive neuroscience? Dev. Cogn. Neurosci. 2019, 35, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Morrison, I.; Bjornsdotter, M.; Olausson, H. Vicarious responses to social touch in posterior insular cortex are tuned to pleasant caressing speeds. J. Neurosci. 2011, 31, 9554–9562. [Google Scholar] [CrossRef] [PubMed]
- Floyd, K. Relational and health correlates of affection deprivation. West. J. Commun. 2014, 78, 383–403. [Google Scholar] [CrossRef]
- Meijer, L.L.; Hasenack, B.; Kamps, J.C.C.; Mahon, A.; Titone, G.; Dijkerman, H.C.; Keizer, A. Affective touch perception and longing for touch during the COVID-19 pandemic. Sci. Rep. 2022, 12, 3887. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, M.; Mamaev, I.; Ditzen, B.; Sailer, U. Calming Effects of Touch in Human, Animal, and Robotic Interaction-Scientific State-of-the-Art and Technical Advances. Front. Psychiatry 2020, 11, 555058. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ishikura, T.; Kitamura, Y.; Sato, W.; Takamatsu, J.; Yuguchi, A.; Cho, S.-G.; Ding, M.; Yoshikawa, S.; Ogasawara, T. Pleasant Stroke Touch on Human Back by a Human and a Robot. Sensors 2023, 23, 1136. [Google Scholar] [CrossRef]
- Feng, C.; Zhou, S.; Qu, Y.; Wang, Q.; Bao, S.; Li, Y.; Yang, T. Overview of Artificial Intelligence Applications in Chinese Medicine Therapy. Evid. Based Complement. Altern. Med. 2021, 2021, 6678958. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhang, P.; Liang, C.; Shi, Y. A portable back massage robot based on traditional Chinese medicine. Technol. Health Care 2018, 26, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Li, J.; Huang, Q.; Souères, P. Anthropomorphic robotic arm with integrated elastic joints for TCM remedial massage. Robotica 2015, 33, 348–365. [Google Scholar] [CrossRef]
- Robotic fingers get touchy-feely. Nature 2018, 555, 289. [CrossRef] [PubMed]
- Wettels, N.; Loeb, G.E. Haptic feature extraction from a biomimetic tactile sensor: Force, contact location and curvature. In Proceedings of the 2011 IEEE International Conference on Robotics and Biomimetics, Karon Beach, Thailand, 7–11 December 2011; pp. 2471–2478. [Google Scholar]
- Fishel, J.A.; Santos, V.J.; Loeb, G.E. A robust micro-vibration sensor for biomimetic fingertips. In Proceedings of the IEEE International Conference on Biomedical Robotics and Biomechatronics, (Scottsdale, AZ), Scottsdale, AZ, USA, 19–22 October 2008; pp. 659–663. [Google Scholar]
- Lin, C.H.; Erickson, T.W.; Fishel, J.A.; Wettels, N.; Loeb, G.E. Signal processing and fabrication of a biomimetic tactile sensor array with thermal, force and microvibration modalities. In Proceedings of the IEEE International Conference on Robotics and Biomimetics, Guilin, China, 19–23 December 2009; pp. 129–134. [Google Scholar]
- Su, Z.; Fishel, J.A.; Yamamoto, T.; Loeb, G.E. Use of tactile feedback to control exploratory movements to characterize object compliance. Front. Neurorobotics 2012, 6, 7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grandi, L.C. From sweeping to caress: Similarities and discrepancies between human and non-human primates’ pleasant touch. Front. Psychol. 2016, 7, 1371. [Google Scholar] [CrossRef] [PubMed]
- Olausson, H.; Lamarre, Y.; Backlund, H.; Morin, C.; Wallin, B.G.; Starck, G.; Ekholm, S.; Strigo, I.; Worsley, K.; Vallbo, Å.B.; et al. Unmyelinated tactile afferents signal touch and project to insular cortex. Nat. Neurosci. 2002, 5, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Olausson, H.; Wessberg, J.; Morrison, I.; McGlone, F.; Vallbo, A.B. The Neurophysiology of Unmyelinated Tactile Afferents. Neurosci. Biobehav. Rev. 2010, 34, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Olausson, H.; Cole, J.; Vallbo, A.B.; McGlone, F.; Elam, M.; Kramer, H.H.; Rylander, K.; Wessberg, J.; Elam, M.; Bushnell, M.C. Unmyelinated tactile afferents have opposite effects on insular and somatosensory cortical processing. Neurosci. Lett. 2008, 436, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Ang, J.Y.; Lua, J.L.; Mathur, A.; Thomas, R.; Asmar, B.I.; Savasan, S.; Buck, S.; Long, M.; Shankaran, S. A randomized pla-cebo-controlled trial of massage therapy on the immune system of preterm infants. Pediatrics 2012, 130, e1549–e1558. [Google Scholar] [CrossRef] [PubMed]
- Kymre, I.G.; Bondas, T. Balancing preterm infants’ developmental needs with parents’ readiness for skin-to-skin care: A phenomenological study. Int. J. Qual. Stud. Health Well-Being 2013, 8, 21370. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Field, T. Social touch, CT touch and massage therapy: A narrative review. Dev. Rev. 2019, 51, 123–145. [Google Scholar] [CrossRef]
- Cassileth, B.R.; Vickers, A.J. Massage therapy for symptom control: Outcome study at a major cancer center. J. Pain Symptom Manag. 2004, 28, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Billhult, A.; Lindholm, C.; Gunnarsson, R.; Stener-Victorin, E. The effect of massage on immune function and stress in women with breast cancer—A randomized controlled trial. Auton. Neurosci. 2009, 150, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Garner, B.; Phillips, L.J.; Schmidt, H.M.; Markulev, C.; O’Connor, J.; Wood, S.J.; Berger, G.E.; Burnett, P.; McGorry, P.D. Pilot study evaluating the effect of massage therapy on stress, anxiety and aggression in a young adult psychiatric inpatient unit. Aust. N. Z. J. Psychiatry 2008, 42, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, B.; Doig, J.; Premkumar, K. The effects of massage therapy on multiple sclerosis patients’ quality of life and leg function. Evid. Based Complement. Altern. Med. 2014, 2014, 640916. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, Q.; Zhang, Q.; Kou, J.; Zhang, Y.; Cui, H.; Wernicke, J.; Montag, C.; Becker, B.; Kendrick, K.M.; et al. The Effects of Intranasal Oxytocin on Neural and Behavioral Responses to Social Touch in the Form of Massage. Front. Neurosci. 2020, 14, 589878. [Google Scholar] [CrossRef] [PubMed]
- Morrison, I.; Löken, L.S.; Olausson, H. The skin as a social organ. Exp. Brain Res. 2009, 204, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Triscoli, C.; Croy, I.; Steudte-Schmiedgen, S.; Olausson, H.; Sailer, U. Heart rate variability is enhanced by long-lasting pleasant touch at CT-optimized velocity. Biol. Psychol. 2017, 128, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Nordin, M. Low-threshold mechanoreceptive and nociceptive units with unmyelinated (C) fibers in the human supraor-bital nerve. J. Physiol. 1990, 426, 229–240. [Google Scholar] [CrossRef]
- McGlone, F.; Kelly, E.F.; Trulsson, M.; Francis, S.T.; Westling, G.; Bowtell, R. Functional neuroimaging studies of human somatosensory cortex. Behav. Brain Res. 2002, 135, 147–158. [Google Scholar] [CrossRef] [PubMed]
- McGlone, F.; Vallbo, A.B.; Olausson, H.; Loken, L.; Wessberg, J. Discriminative touch and emotional touch. Can. J. Exp. Psychol. Can. Psychol. Exp. 2007, 61, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Gordon, I.; Voos, A.C.; Bennett, R.H.; Bolling, D.Z.; Pelphrey, K.A.; Kaiser, M.D. Brain mechanisms for processing affective touch. Hum. Brain Mapp. 2013, 34, 914–922. [Google Scholar] [CrossRef]
- McGlone, F.; Wessberg, J.; Olausson, H. Discriminative and affective touch: Sensing and feeling. Neuron 2014, 82, 737–755. [Google Scholar] [CrossRef] [PubMed]
- Fagundes, C.P.; Glaser, R.; Kiecolt-Glaser, J.K. Stressful early life experiences and immune dysregulation across the lifespan. Brain Behav. Immun. 2013, 27, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Gallace, A.; Spence, C. The science of interpersonal touch: An overview. Neurosci. Biobehav. Rev. 2010, 34, 246–259. [Google Scholar] [CrossRef]
- Harlow, H.F.; Zimmermann, R.R. The development of affectional responses in infant monkeys. Proc. Am. Philos. Soc. 1958, 102, 501–509. [Google Scholar]
- Harlow, H.F.; Zimmermann, R.R. Affectional responses in the infant monkey; orphaned baby monkeys develop a strong and persistent attachment to inanimate surrogate mothers. Science 1959, 130, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Disarbois, E.; Duhamel, J.R. Virtual social grooming in macaques and its psychophysiological effects. Sci. Rep. 2024, 14, 11697. [Google Scholar] [CrossRef] [PubMed]
- Hooker, D. Early human fetal activity. Anat. Rec. 1952, 113, 503–504. [Google Scholar] [PubMed]
- Kisilevsky, B.S.; Muir, D.W.; Low, J.A. Maturation of human fetal responses to vibroacoustic stimulation. Child Dev. 1992, 63, 1497–1508. [Google Scholar] [CrossRef] [PubMed]
- Marx, V.; Nagy, E. Fetal behavioral responses to the touch of the mother’s abdomen: A frame-by-frame analysis. Infant Behav. Dev. 2017, 47, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Marx, V.; Nagy, E. Fetal Behavioural Responses to Maternal Voice and Touch. PLoS ONE 2015, 10, e0129118. [Google Scholar] [CrossRef] [PubMed]
- Bremner, A.J.; Spence, C. The development of tactile perception. Adv. Child Dev. Behav. 2017, 52, 227–268. [Google Scholar]
- Carlson, M.; Earls, F. Psychological and neuroendocrinological sequelae of early social deprivation in institutionalized children in Romania. In The Integrative Neurobiology of Affiliation; Carter, C.S., Lederhendler, I.I., Kirkpatrick, B., Eds.; New York Academy of Sciences: New York, NY, USA, 1997; pp. 419–428. [Google Scholar]
- Diego, M.A.; Field, T.; Hernandez-Reif, M. Preterm infant weight gain is increased by massage therapy and exercise via different underlying mechanisms. Early Hum. Dev. 2014, 90, 137–140. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Field, T.M.; Schanberg, S.M.; Scafidi, F.; Bauer, C.R.; Vega-Lahr, N.; Garcia, R.; Nystrom, J.; Kuhn, C.M. Tac-tile/kinesthetic stimulation effects on preterm neonates. Pediatrics 1986, 77, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Neu, M.; Laudenslager, M.L.; Robinson, J. Coregulation in salivary cortisol during maternal holding of premature infants. Biol. Res. Nurs. 2008, 10, 226–240. [Google Scholar] [CrossRef] [PubMed]
- International Workshop on Kangaroo Mother Care. 2009. Available online: https://kangaroomothercare.org/ (accessed on 6 May 2024).
- Nyqvist, K.H.; Anderson, G.C.; Bergman, N.; Cattaneo, A.; Davanzo, R.; Ewald, U.; Ludington-Hoe, S.; Mendoza, S.; Pallas-Allonso, C. State of the art and recommendations. Kangaroo mother care; application in a high-tech environment. Acta Paediatr. 2010, 99, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.donatoridicoccole.it/ (accessed on 6 May 2024).
- von Mohr, M.; Kirsch, L.P.; Fotopoulou, A. Social touch deprivation during COVID-19: Effects on psychological wellbeing and craving interpersonal touch. R. Soc. Open Sci. 2021, 8, 210287. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- MacLean, K. The impact of institutionalization on child development. Dev. Psychopathol. 2003, 15, 853–884. [Google Scholar] [CrossRef] [PubMed]
- Haggarty, C.J.; Malinowski, P.; McGlone, F.P.; Walker, S.C. Autistic traits modulate cortical responses to affective but not discriminative touch. Eur. J. Neurosci. 2020, 51, 1844–1855. [Google Scholar] [CrossRef] [PubMed]
- Kang, Z.; Xing, H.; Lin, Q.; Meng, F.; Gong, L. Effectiveness of therapeutic massage for improving motor symptoms in Park-inson’s disease: A systematic review and meta-analysis. Front. Neurol. 2022, 13, 915232. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baumgart, S.B.; Baumbach-Kraft, A.; Lorenz, J. Effect of Psycho-Regulatory Massage Therapy on Pain and Depression in Women with Chronic and/or Somatoform Back Pain: A Randomized Controlled Trial. Brain Sci. 2020, 10, 721. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grandi, L.C.; Bruni, S. Social Touch: Its Mirror-like Responses and Implications in Neurological and Psychiatric Diseases. NeuroSci 2023, 4, 118–133. [Google Scholar] [CrossRef]
- Mintz, Y.; Brodie, R. Introduction to artificial intelligence in medicine. Minim. Invasive Ther. Allied Technol. 2019, 28, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.R.; Lu, L.; Zhang, J.Y.; Huo, T.T.; Liu, S.X.; Ye, Z.W. Application of Artificial Intelligence in Medicine: An Overview. Curr. Med. Sci. 2021, 41, 1105–1115. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hamet, P.; Tremblay, J. Artificial intelligence in medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef]
- Alberdi, A.; Aztiria, A.; Basarab, A. On the early diagnosis of Alzheimer’s Disease from multimodal signals: A survey. Artif. Intell. Med. 2016, 71, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.; Villa, R.; Ugga, L.; Romeo, V.; Stanzione, A.; Cuocolo, R. Artificial intelligence applied to neuroimaging data in Parkinsonian syndromes: Actuality and expectations. Math. Biosci. Eng. 2021, 18, 1753–1773. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bejnordi, B.E.; Lin, J.; Glass, B.; Mullooly, M.; Gierach, G.L.; Sherman, M.E.; Karssemeijer, N.; van der Laak, J.; Beck, A.H. Deep learning-based assessment of tumor-associated stroma for diagnosing breast cancer in histopathology images. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, VIC, Australia, 18–21 April 2017; pp. 929–932. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Available online: https://www.therobotreport.com/6-ways-ai-and-robotics-are-improving-healthcare/ (accessed on 6 May 2024).
- Available online: https://starship.co/ (accessed on 6 May 2024).
- Available online: https://www.nasa.gov/artificial-intelligence/ (accessed on 6 May 2024).
- Available online: https://www.techopedia.com/nasas-2024-tech-ai-robots-space-exploration;https://www.esa.int/Enabling_Support/Preparing_for_the_Future/Discovery_and_Preparation/Artificial_intelligence_in_space (accessed on 6 May 2024).
- A soft touch for robots. Nat. Mach. Intell. 2022, 4, 415. [CrossRef]
- Massari, L.; Fransvea, G.; D’abbraccio, J.; Filosa, M.; Terruso, G.; Aliperta, A.; D’alesio, G.; Zaltieri, M.; Schena, E.; Palermo, E.; et al. Functional mimicry of Ruffini receptors with fibre Bragg gratings and deep neural networks enables a bio-inspired large-area tactile-sensitive skin. Nat. Mach. Intell. 2022, 4, 425–435. [Google Scholar] [CrossRef]
- Jiminez, M.C.; Fishel, J.A. Evaluation of force, vibration and thermal tactile feedback in prosthetic limbs. In Proceedings of the IEEE International Conference on Haptic Interfaces for Virtual Environment and Teleoperator Systems (Haptics), Houston, TX, USA, 23–26 February 2014; pp. 437–441. [Google Scholar]
- Huang, S.; Wu, H. Texture Recognition Based on Perception Data from a Bionic Tactile Sensor. Sensors 2021, 21, 5224. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- SynTouch. Available online: https://syntouchinc.com (accessed on 6 May 2024).
- Matulevich, B.; Pandit, V.; Lin, C.H.; Loeb, G.E.; Fishel, J.A. Utility of contact detection and compliant fingertips in prosthetic hand control. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 4741–4746. [Google Scholar]
- Zhang, M.L.; Shi, Z.X. Structure design and analysis of end-effector for traditional Chinese medical massage manipulator. J. Mech. Transm. 2020, 44, 73–77. [Google Scholar]
- Motamedi, N. Keep in touch: A tactile-vision intimate interface. In Proceedings of the 1st International Conference on Tangible and Embedded Interaction (TEI ’07); Association for Computing Machinery: New York, NY, USA, 2007; pp. 21–22. [Google Scholar] [CrossRef]
- Mueller, F.; Vetere, F.; Gibbs, M.R.; Kjeldskov, J.; Pedell, S.; Howard, S. Hug over a distance. In Proceedings of the CHI’05 Extended Abstracts on Human Factors in Computing Systems, Portland, OR, USA, 2–7 April 2005; pp. 1673–1676. [Google Scholar]
- Available online: https://cutecircuit.com/hugshirt/ (accessed on 6 May 2024).
- Petersen, S.; Houston, S.; Qin, H.; Tague, C.; Studley, J. The Utilization of Robotic Pets in Dementia Care. J. Alzheimer’s Dis. 2017, 55, 569–574. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Velde, B.P.; Cipriani, J.; Fisher, G. Resident and therapist views of animal-assisted therapy: Implications for occupational therapy practice. Aust. Occup. Ther. J. 2005, 52, 43–50. [Google Scholar] [CrossRef]
- Broekens, J.; Heerink, M.; Rosendal, H. Assistive social robots in elderly care: A review. Gerontechnology 2009, 8, 94–103. [Google Scholar] [CrossRef]
- Shibata, T.; Wada, K. Robot therapy: A new approach for mental healthcare of the elderly—A mini-review. Gerontology 2011, 57, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T. Human-entrained embodied interaction and communication technology. Emot. Eng. 2011, 9, 161–177. [Google Scholar] [CrossRef]
- Giannopulu, I.; Terada, K.; Watanabe, T. Emotional empathy as a mechanism of synchronization in child–robot interaction. Front. Psychol. 2018, 9, 1852. [Google Scholar] [CrossRef]
- Kozima, H.; Michalowski, M.P.; Nakagawa, C. Keepon. Int. J. Soc. Robot. 2008, 1, 3–18. [Google Scholar] [CrossRef]
- Giannopulu, I.; Pradel, G. Multimodal interactions in free game play of children with autism and a mobile toy robot. NeuroRehabilitation 2010, 27, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Elendu, C.; Amaechi, D.C.; Elendu, T.C.; Jingwa, K.A.; Okoye, O.K.; John Okah, M.; Ladele, J.A.; Farah, A.H.; Alimi, H.A. Ethical implications of AI and robotics in healthcare: A review. Medicine 2023, 102, e36671. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Emanuel, E.J.; Wachter, R.M. Artificial intelligence in health care: Will the value match the hype? JAMA 2019, 321, 2281–2282. [Google Scholar] [CrossRef] [PubMed]
- Henschel, A.; Laban, G.; Cross, E.S. What Makes a Robot Social? A Review of Social Robots from Science Fiction to a Home or Hospital Near You. Curr. Robot. Rep. 2021, 2, 9–19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Available online: https://furhatrobotics.com/ (accessed on 6 May 2024).
- Pandey, A.K.; Gelin, R. A Mass-Produced Sociable Humanoid Robot: Pepper: The First Machine of Its Kind. IEEE Robot. Autom. Mag. 2018, 25, 40–48. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grandi, L.C.; Bruni, S. Will the Artificial Intelligence Touch Substitute for the Human Touch? NeuroSci 2024, 5, 254-264. https://doi.org/10.3390/neurosci5030020
Grandi LC, Bruni S. Will the Artificial Intelligence Touch Substitute for the Human Touch? NeuroSci. 2024; 5(3):254-264. https://doi.org/10.3390/neurosci5030020
Chicago/Turabian StyleGrandi, Laura Clara, and Stefania Bruni. 2024. "Will the Artificial Intelligence Touch Substitute for the Human Touch?" NeuroSci 5, no. 3: 254-264. https://doi.org/10.3390/neurosci5030020
APA StyleGrandi, L. C., & Bruni, S. (2024). Will the Artificial Intelligence Touch Substitute for the Human Touch? NeuroSci, 5(3), 254-264. https://doi.org/10.3390/neurosci5030020