
COVID-19 Outbreak Management and Vaccination Strategy in The United States of America

 ,
,  and
and 
Abstract
:1. Introduction
2. Case Presentation
2.1. Characteristics of the Country
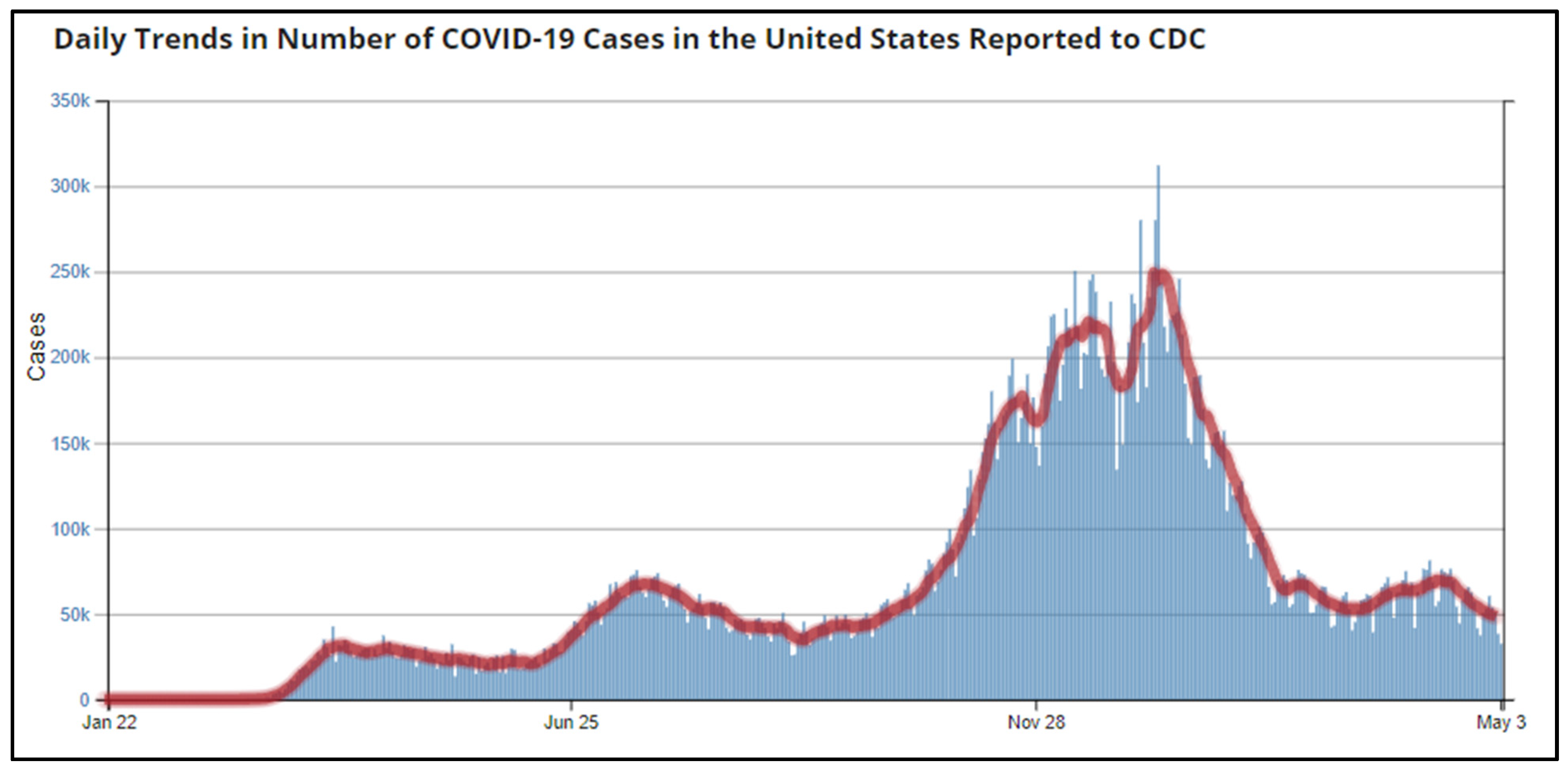
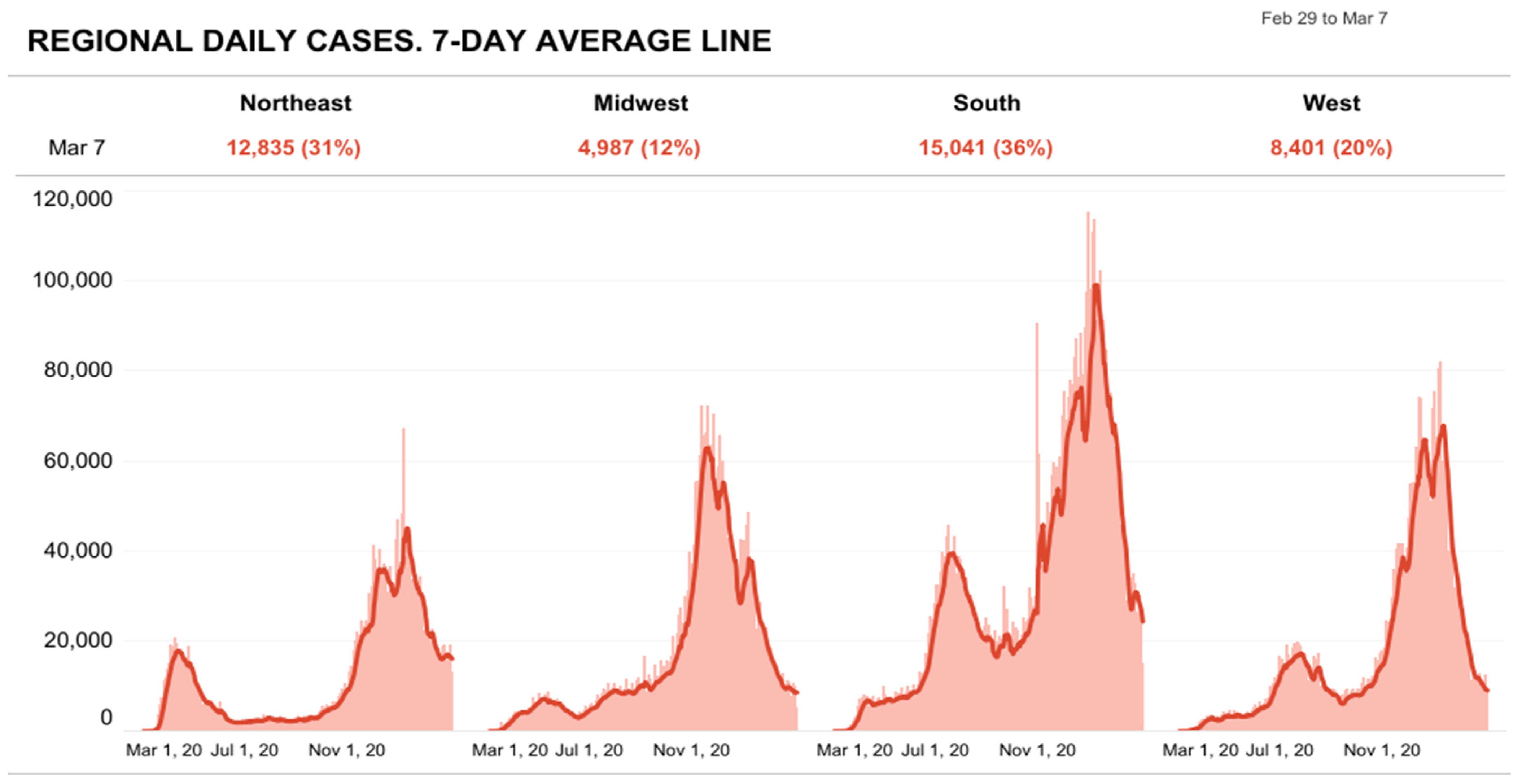
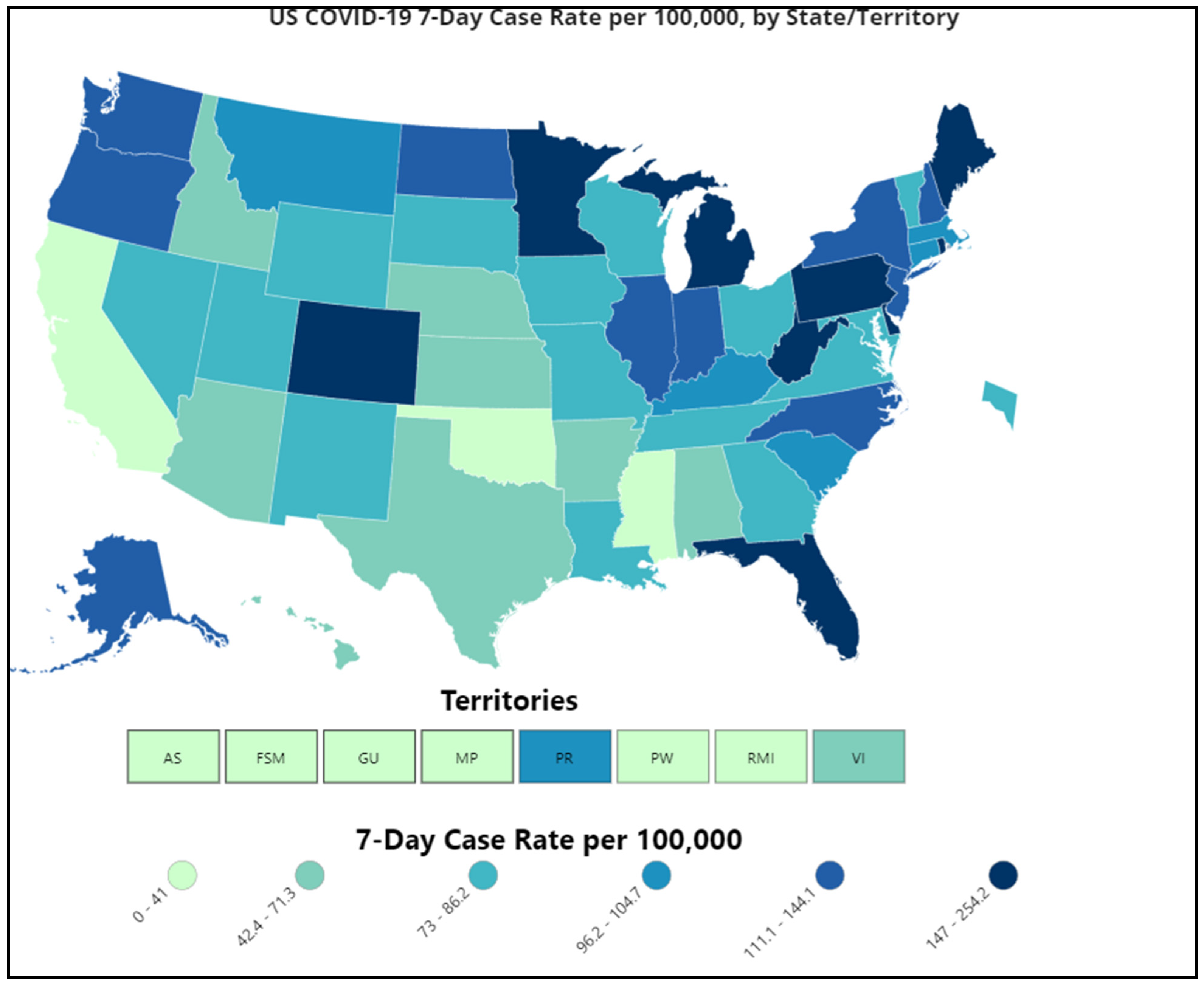
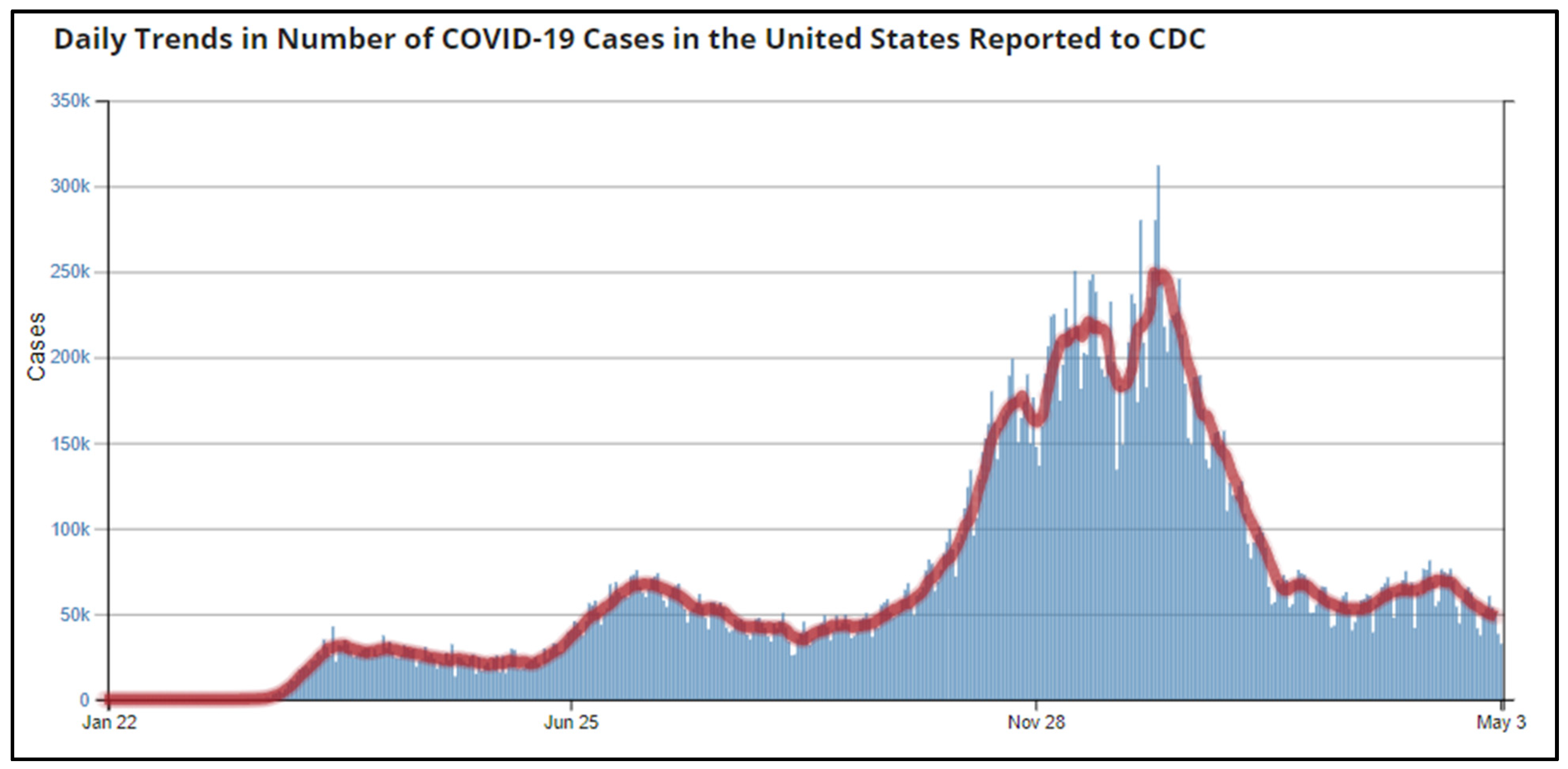
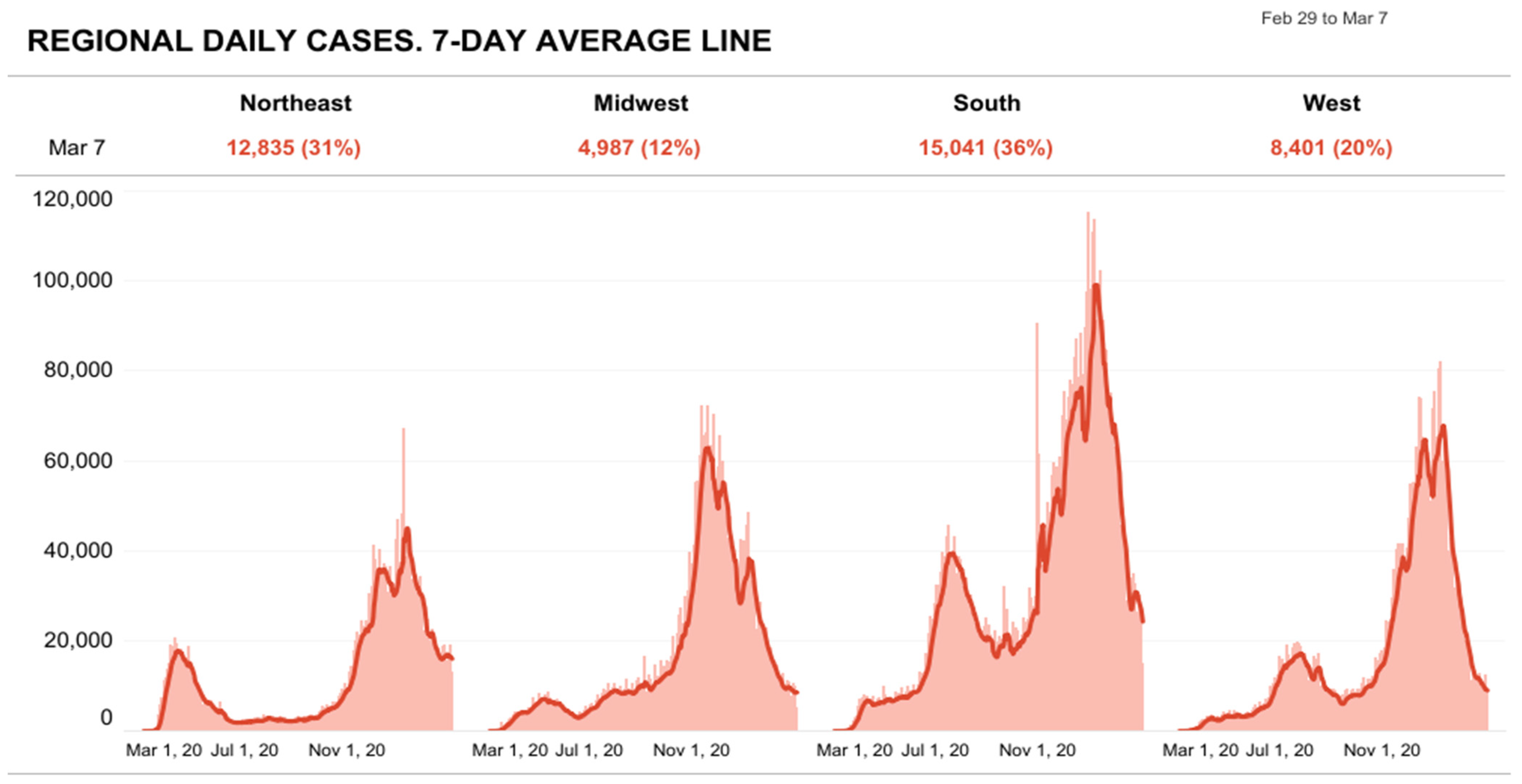
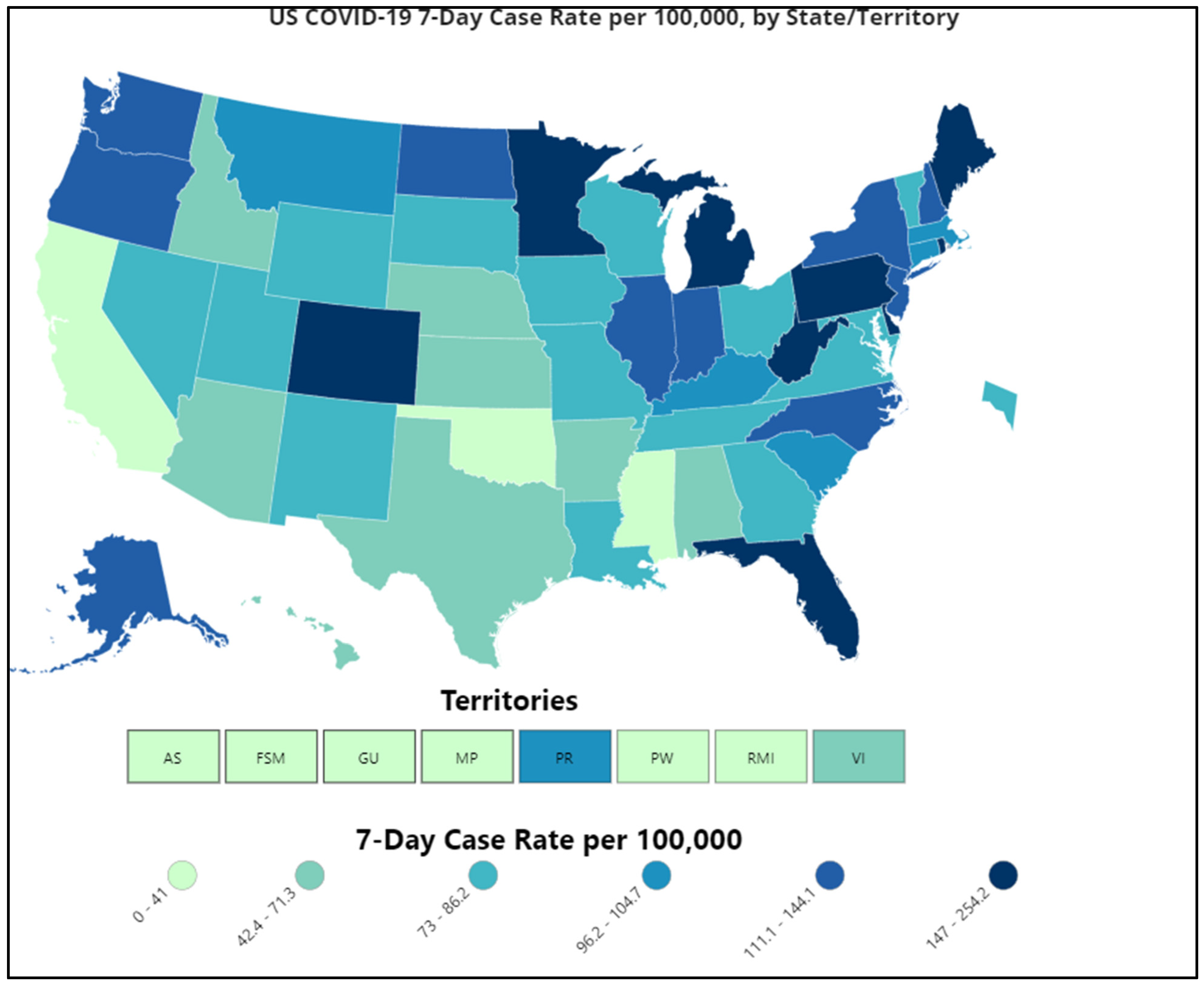
2.2. Epidemiological Situation
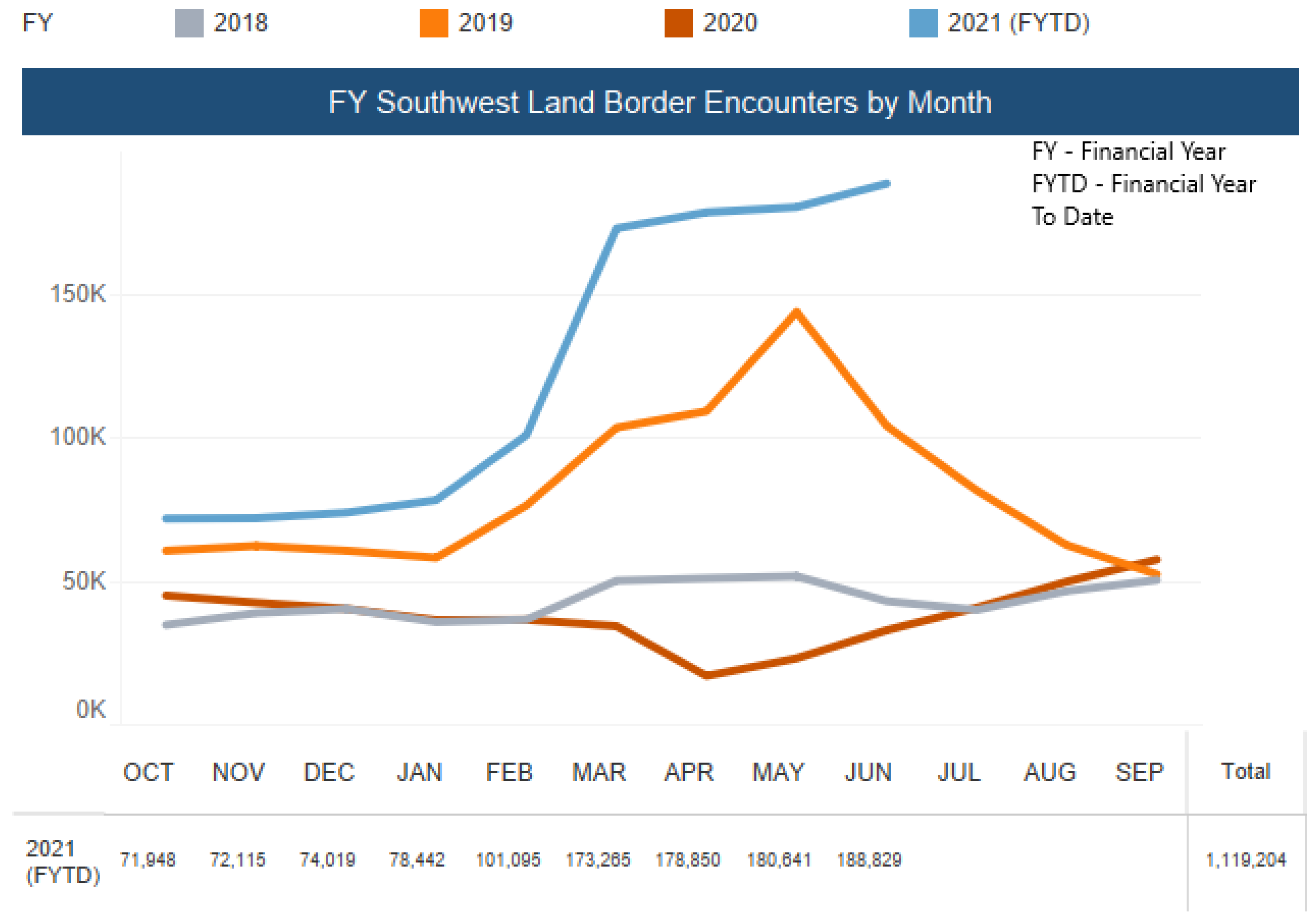
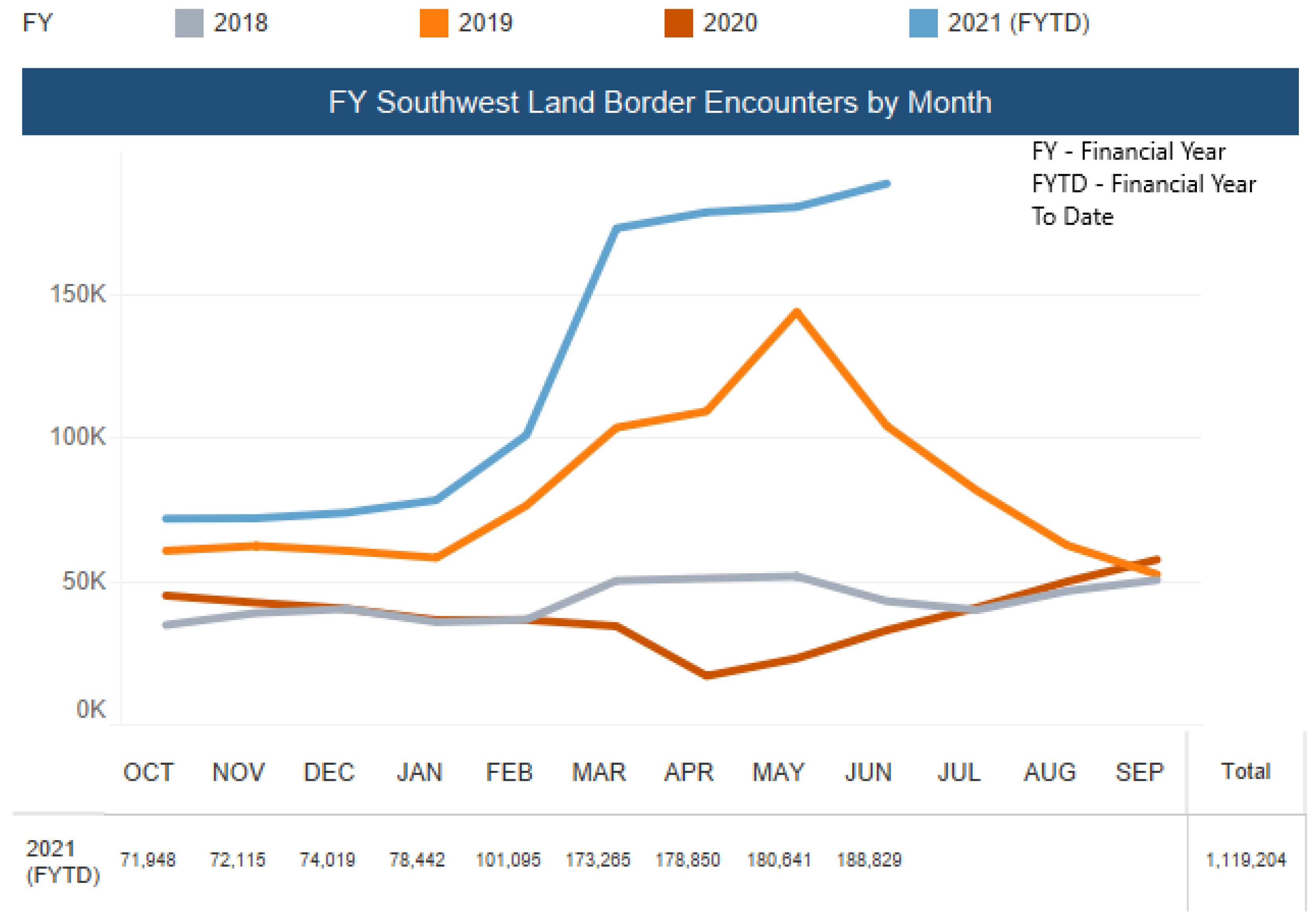
2.3. Immigration Crisis
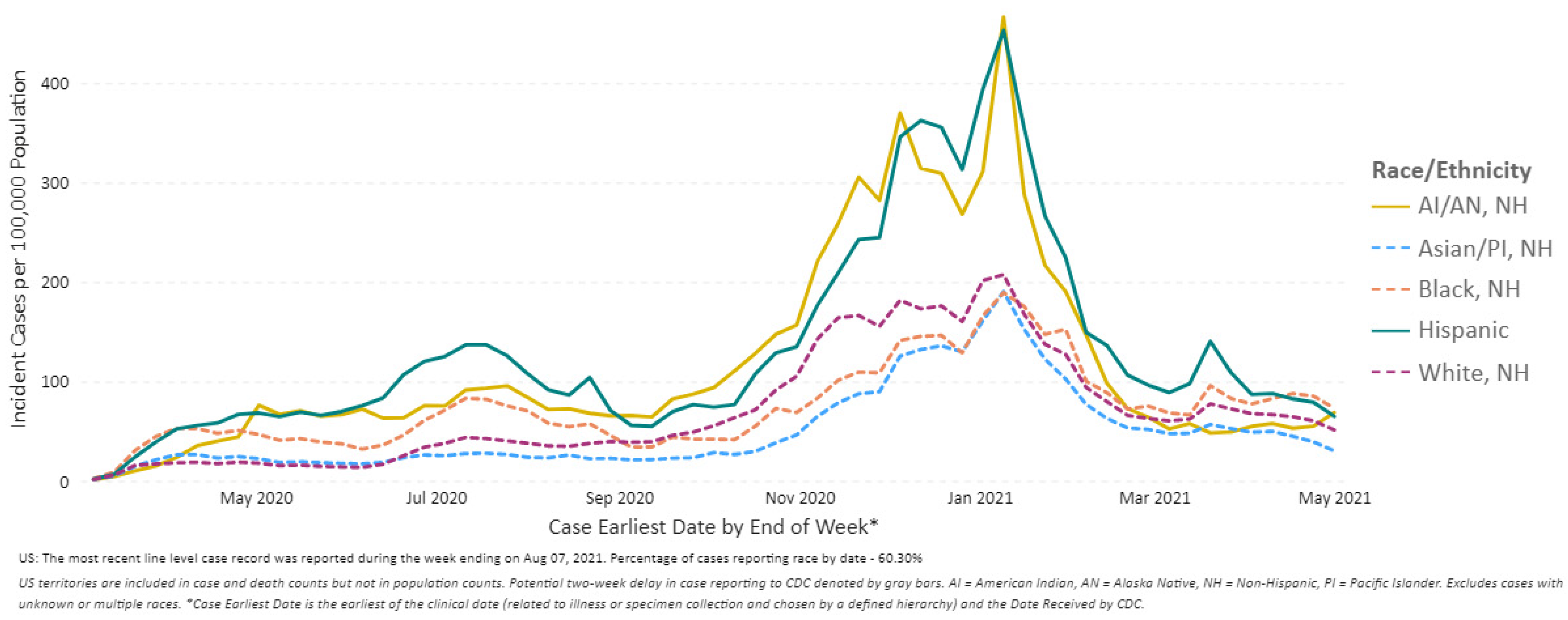
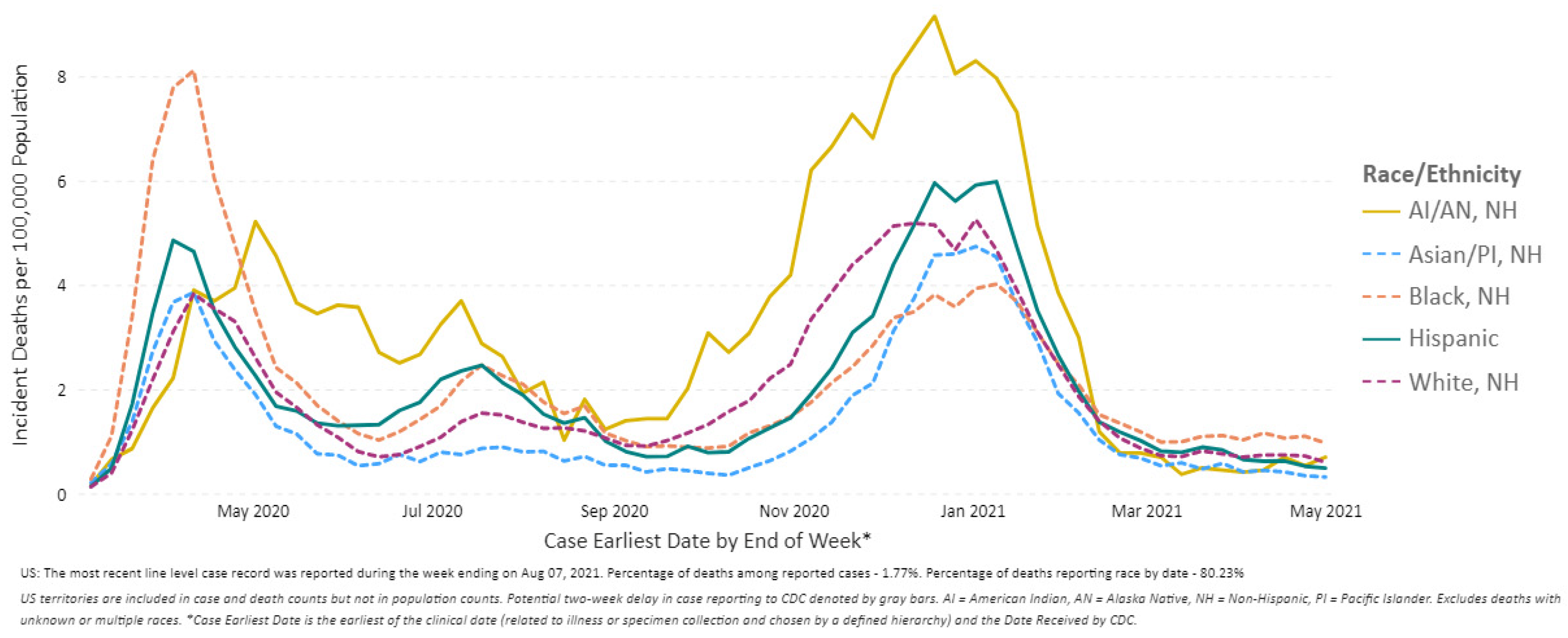
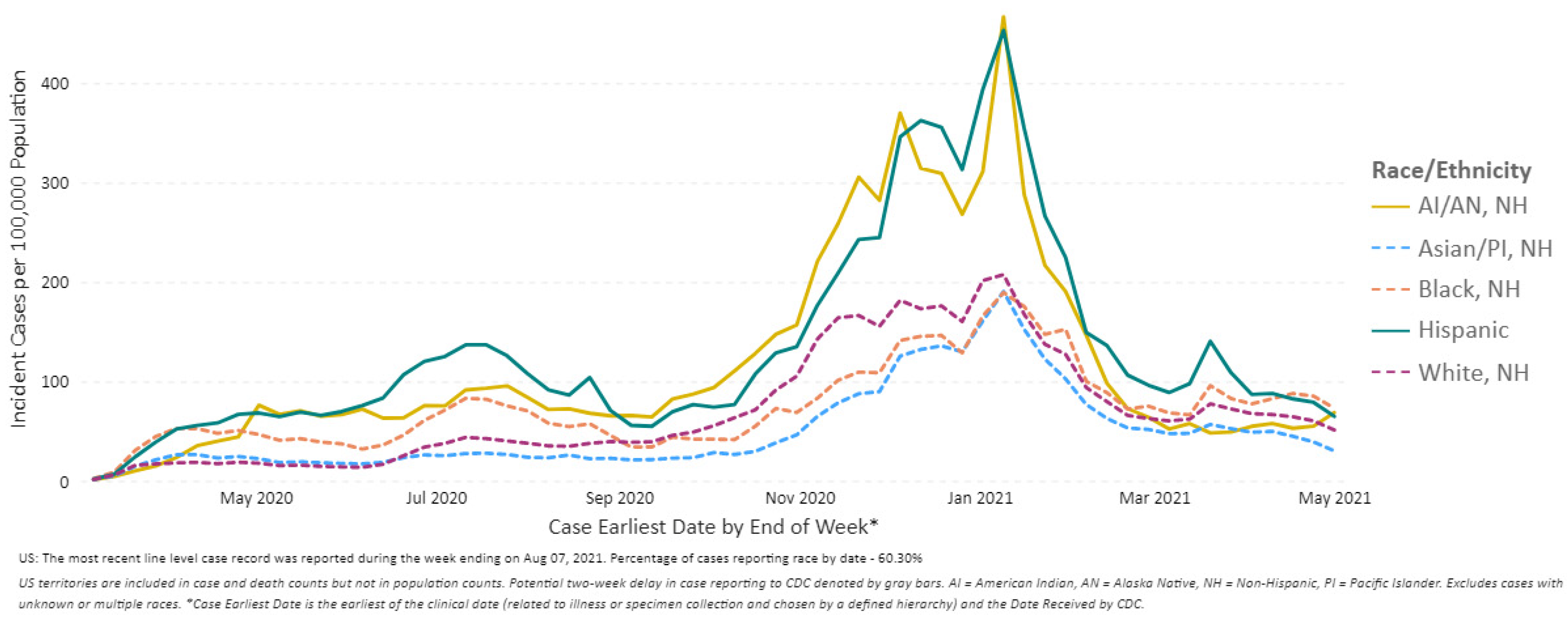
2.4. Racial Disparities
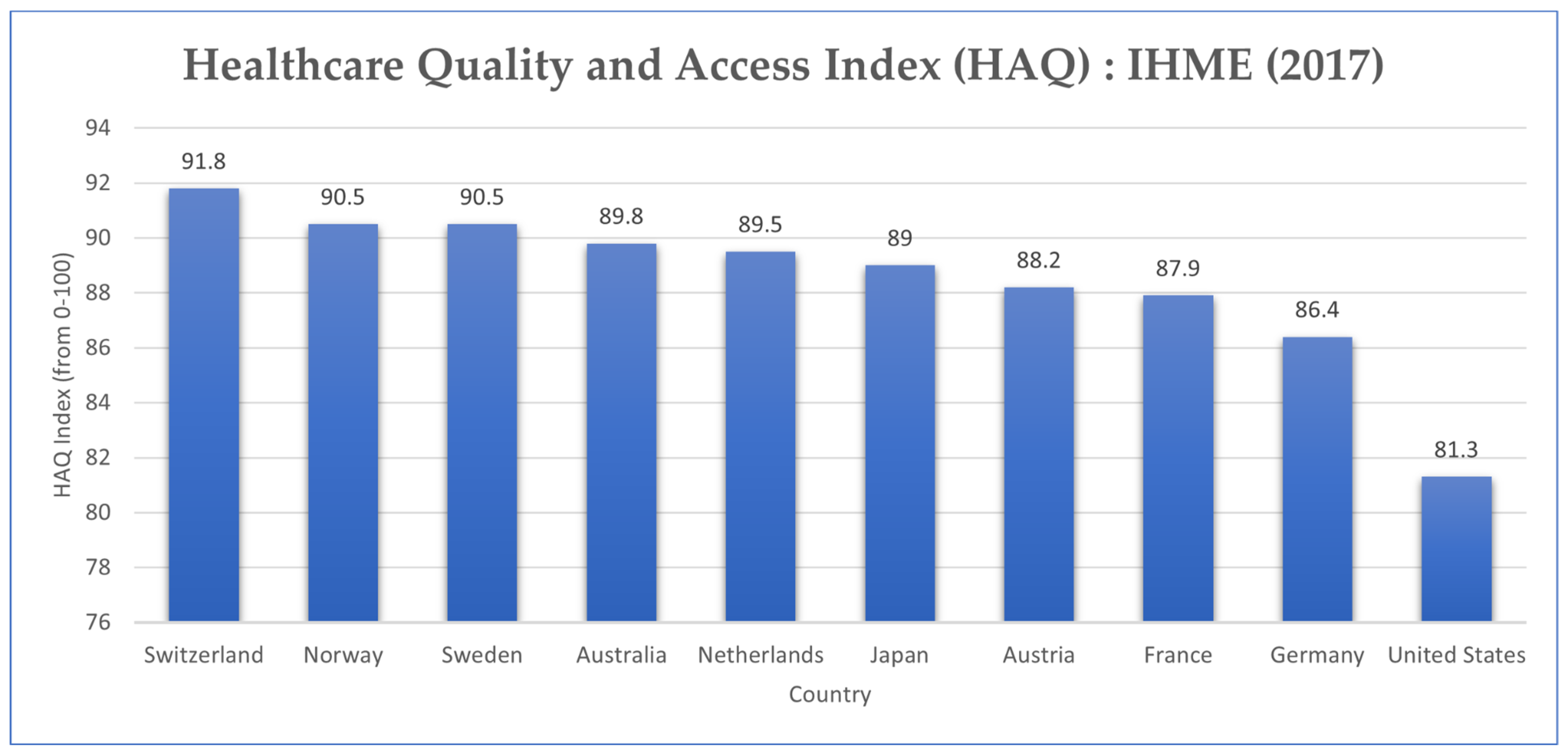
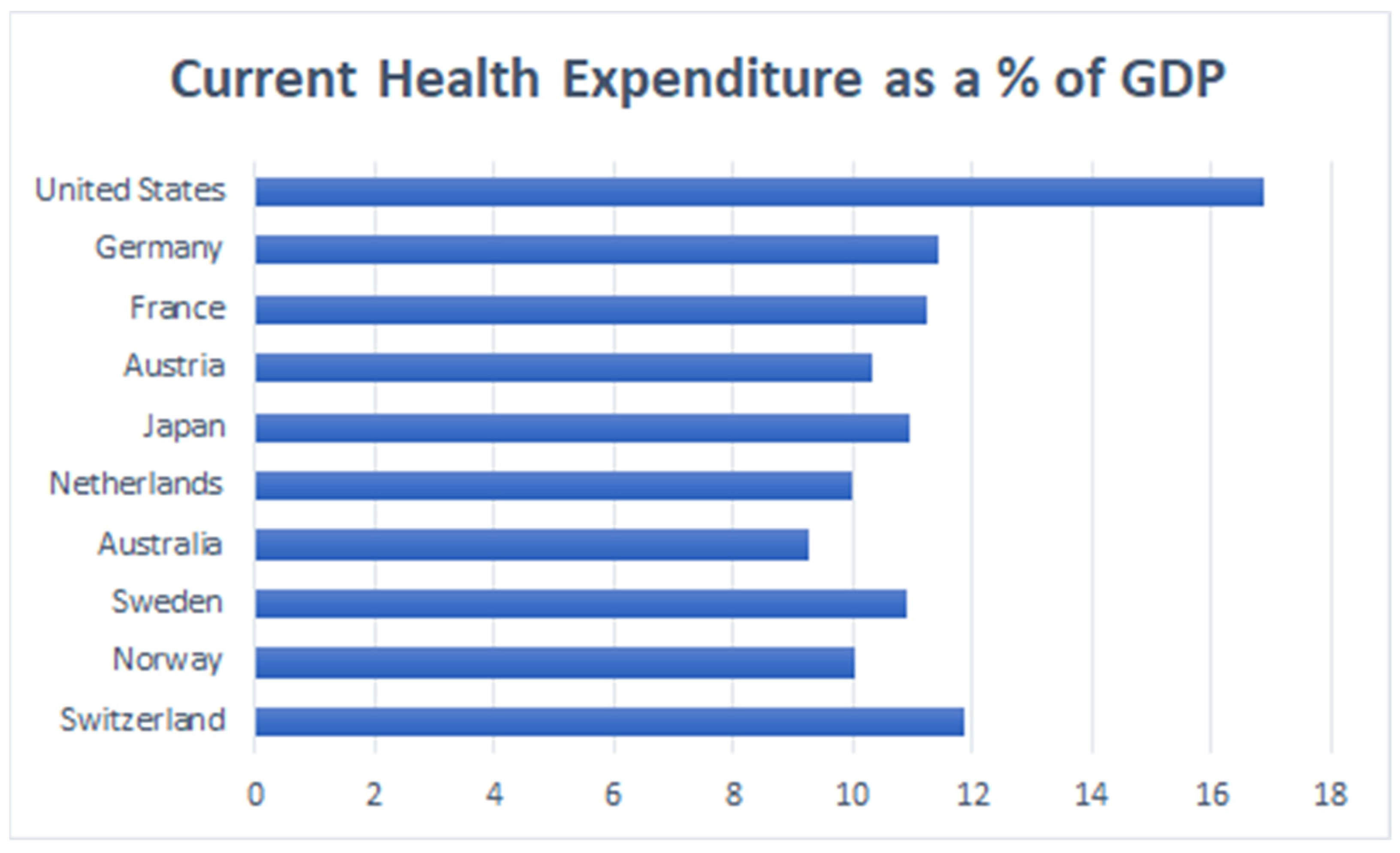
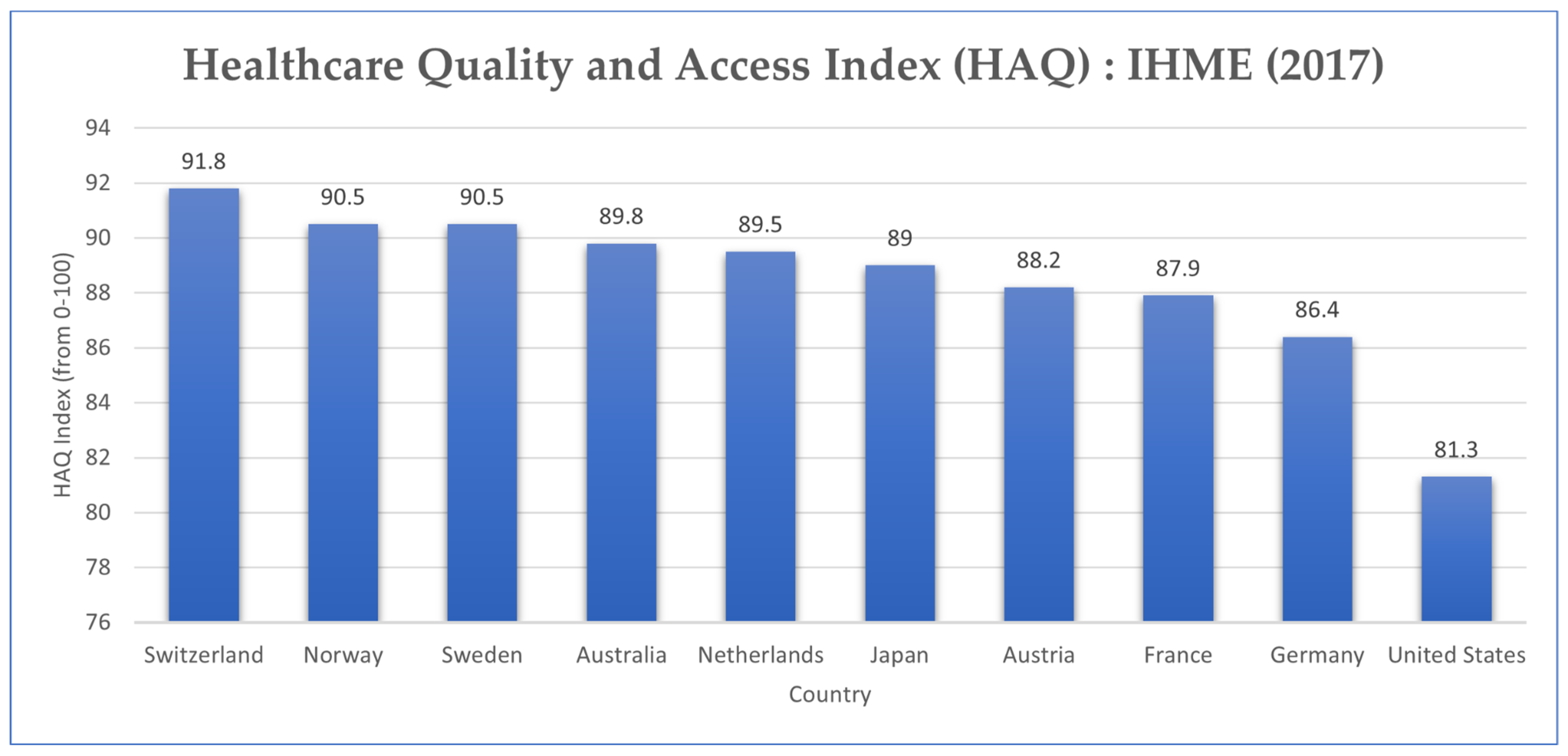
2.5. United States’ Healthcare System
3. Management and Outcome
3.1. Political Management of the COVID-19 Outbreak
3.2. Challenges to COVID-19 Vaccine Acceptance
3.3. Non-Pharmaceutical Intervention Measures Undertaken by Health Authorities
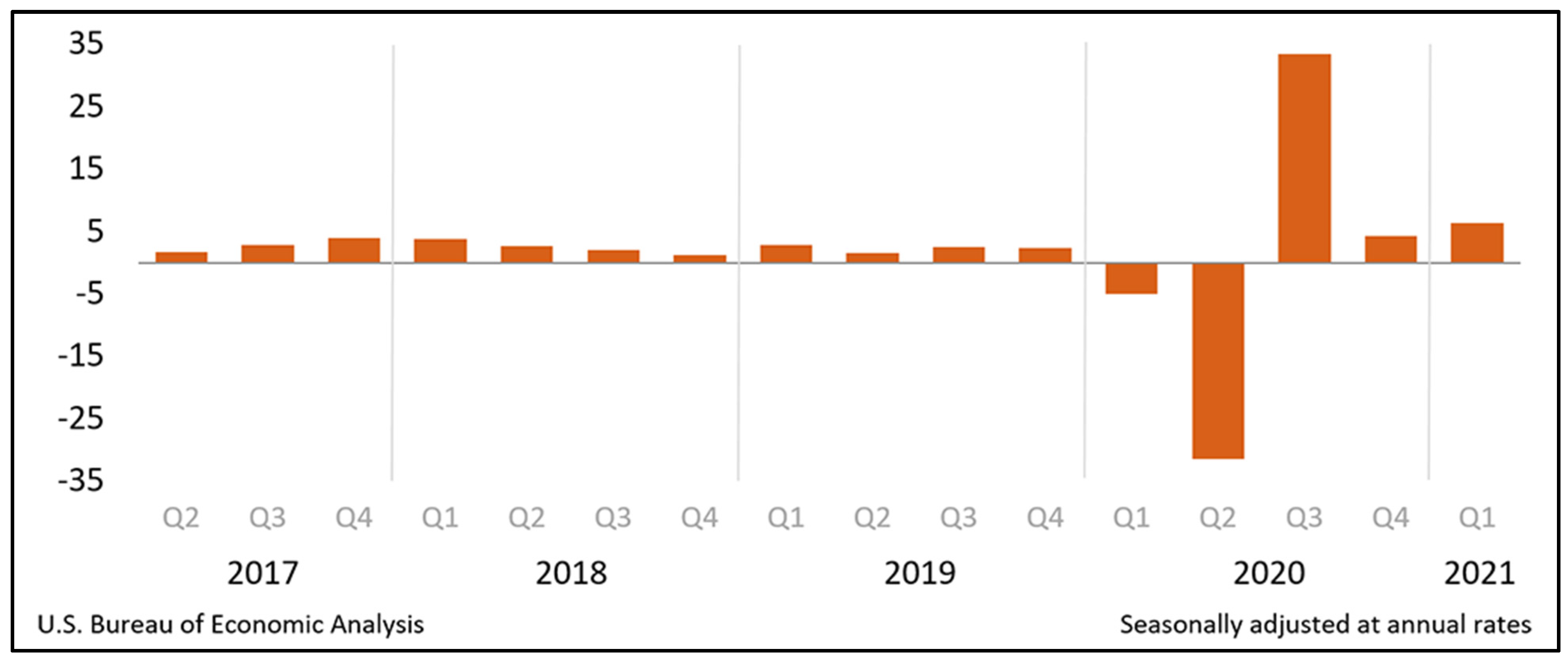
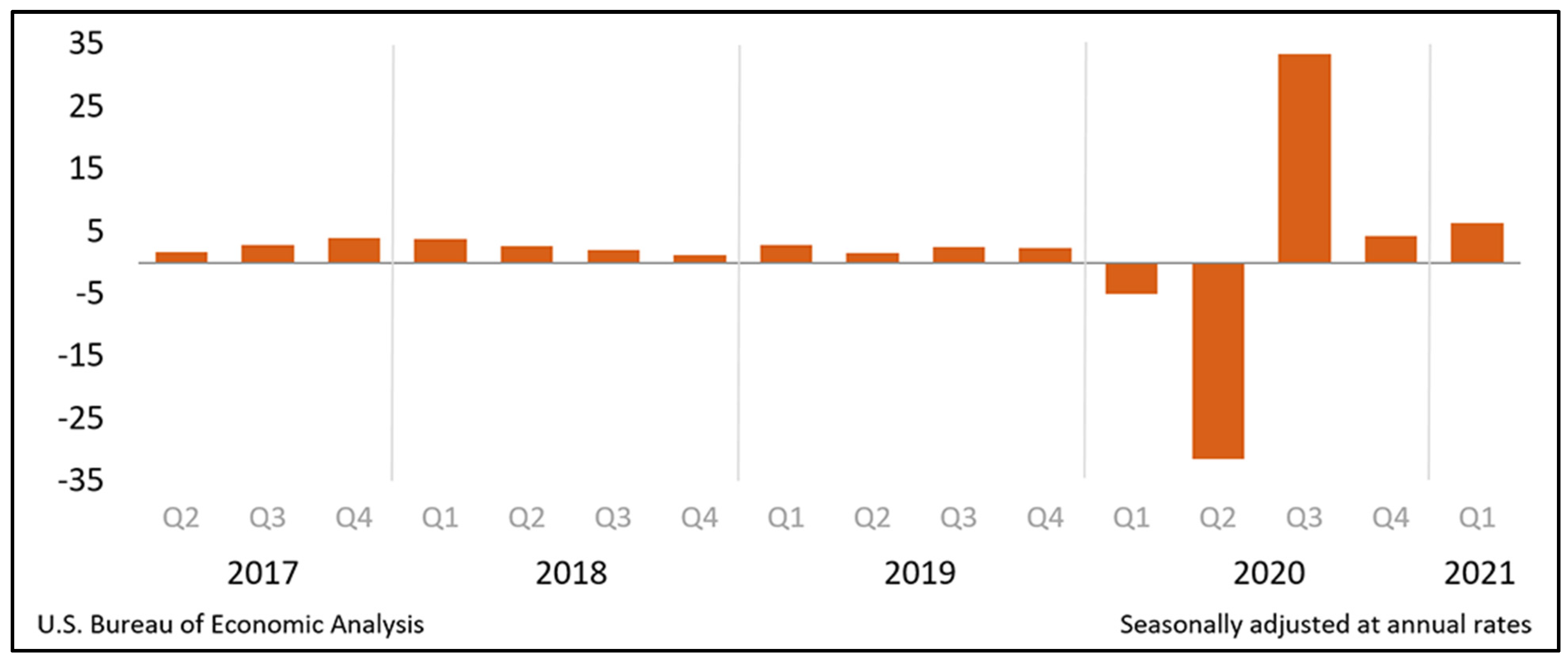
3.4. Economic Effects of COVID-19
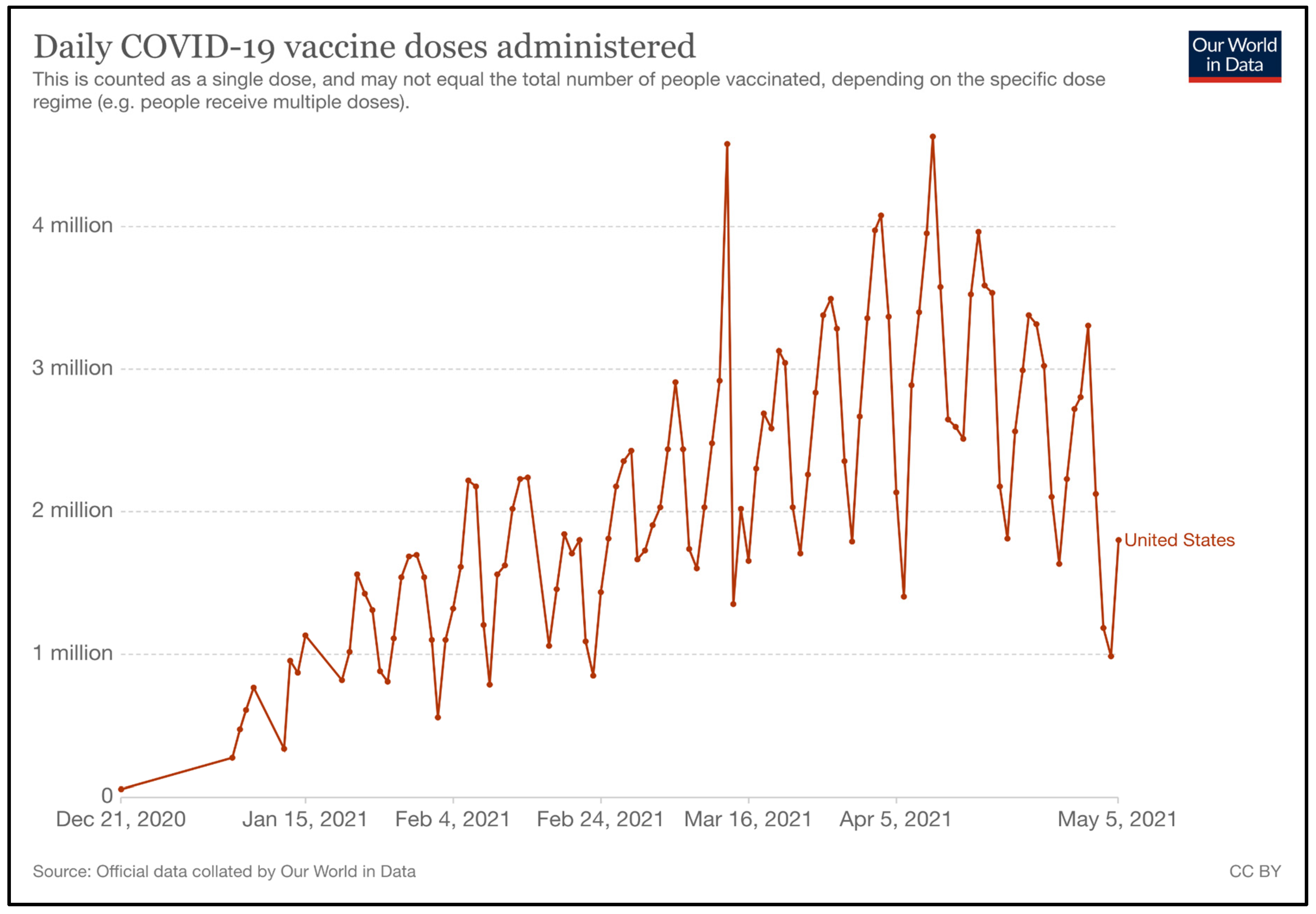
4. Vaccination Strategy
4.1. Vaccine Characteristics and Registration Procedure
- The CBRN agent to which the EUA applies can endanger life, or cause different conditions or diseases [87].
- Reasonable evidence to believe that the medical product “may be effective” in preventing, diagnosing, or treating the disease or condition [87].
- The product’s identified and prospective benefits exceed its identified and prospective risks [87].
- There are no other suitable alternatives available or approved for the prevention, diagnosis, or treatment of the disease or condition [87].
4.1.1. Pfizer-BioNTech
4.1.2. Moderna
4.1.3. Janssen Biotech, Inc.
4.2. Production and Purchase Schedule for Vaccines and Related Medical Products
4.3. Prioritization of Target Groups
4.3.1. Phase 1a
4.3.2. Phase 1b
4.3.3. Phase 1c
4.3.4. Phase 2
4.4. Vaccine Supply Chain and Dynamics
4.5. Clinical Management of Vaccination
4.6. Investigational Therapeutics for COVID-19
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gretchen, B.; Shubham, S.; Meredith, L.; John, S. Challenges Emerge for the US Healthcare System as COVID-19 Cases Rise; Mckinsey Co.: Chicago, IL, USA, 2020; Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/challenges-emerge-for-the-us-healthcare-system-as-covid-19-cases-rise (accessed on 5 May 2021).
- COVID in the U.S.: Latest Map and Case Count–The New York Times. Available online: https://www.nytimes.com/interactive/2021/us/covid-cases.html (accessed on 5 May 2021).
- CDC. COVID Data Tracker. 2021. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 5 May 2021).
- United States Census Bureau. Population Clock. Available online: https://www.census.gov/popclock/ (accessed on 5 May 2021).
- United States|History, Map, Flag, & Population|Britannica. Available online: https://www.britannica.com/place/United-States (accessed on 16 August 2021).
- UNData App. Available online: http://data.un.org/en/iso/us.html (accessed on 5 May 2021).
- World Population Prospects-Population Division-United Nations. Available online: https://population.un.org/wpp/ (accessed on 5 May 2021).
- The U.S. Refugee Resettlement Program Explained. Available online: https://www.unrefugees.org/news/the-u-s-refugee-resettlement-program-explained/ (accessed on 5 May 2021).
- Climate and Temperature Development in the United States. WorlddataInfo. Available online: https://www.worlddata.info/america/usa/climate.php (accessed on 5 May 2021).
- Our Government. White House. Available online: https://www.whitehouse.gov/about-the-white-house/our-government/ (accessed on 5 May 2021).
- State and Local Government. White House. Available online: https://www.whitehouse.gov/about-the-white-house/our-government/state-local-government/ (accessed on 5 May 2021).
- Berman, E. The Roles of the State and Federal Governments in a Pandemic. 2020. Available online: https://jnslp.com/2020/10/19/the-roles-of-the-state-and-federal-governments-in-a-pandemic/ (accessed on 5 May 2021).
- Bearman, G.; Pryor, R.; Vokes, R.; Cooper, K.; Doll, M.; Godbout, E.J.; Stevens, M.P. Reflections on the COVID-19 pandemic in the USA: Will we be better prepared next time? Int. J. Infect. Dis. 2020, 96, 610–613. [Google Scholar] [CrossRef]
- Economy & Trade|United States Trade Representative. Available online: https://ustr.gov/issue-areas/economy-trade (accessed on 7 May 2021).
- GDP Growth (Annual %)-United States|Data. Available online: https://data.worldbank.org/indicator/NY.GDP.MKTP.KD.ZG?locations=US (accessed on 7 May 2021).
- Gross Domestic Product, First Quarter 2021 (Advance Estimate)|U.S. Bureau of Economic Analysis (BEA). Available online: https://www.bea.gov/news/2021/gross-domestic-product-first-quarter-2021-advance-estimate (accessed on 7 May 2021).
- Budget of the U.S. Government|USAGov. Available online: https://www.usa.gov/budget (accessed on 7 May 2021).
- U.S. Centers for Medicare & Medicaid Services. National Health Expenditures 2019 Highlights. 2019. Available online: https://www.cms.gov/files/document/highlights.pdf (accessed on 6 May 2021).
- WHO|Pneumonia of Unknown Cause–China. WHO. Available online: http://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/ (accessed on 5 May 2021).
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Early Look at Implications COVID-19 Pandemic for Health Coverage|Commonwealth Fund. Available online: https://www.commonwealthfund.org/publications/issue-briefs/2020/jun/implications-covid-19-pandemic-health-insurance-survey (accessed on 5 May 2021).
- Mann, D.M.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. J. Am. Med. Inform. Assoc. JAMIA 2020, 27, 1132–1135. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Updates-March 31. Available online: https://myemail.constantcontact.com/COVID-19-Updates---March-31.html?soid=1107826135286&aid=_CBriJNgEs0 (accessed on 6 May 2021).
- The COVID Tracking Project by the Atlantic Monthly Group, 2021, Regional Cases. Available online: https://covidtracking.com/data/charts/regional-cases (accessed on 5 May 2021).
- United States: The Latest Coronavirus Counts, Charts and Maps. Available online: https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/united-states/ (accessed on 5 May 2021).
- CDC. COVID Data Tracker Weekly Review. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html (accessed on 5 May 2021).
- COVID-19 Updates-30 April 2021. Johns Hopkins Cent Health Secur. Available online: https://myemail.constantcontact.com/COVID-19-Updates---April-30--2021.html?soid=1107826135286&aid=PpRKoQy88Ds (accessed on 5 May 2021).
- Loweree, J.; Reichlin-Melnick, A.; Ewing, W. The Impact of COVID-19 on Noncitizens and Across the U.S. Immigration System. 2020. Available online: https://www.americanimmigrationcouncil.org/research/impact-covid-19-us-immigration-system (accessed on 5 May 2021).
- Pierce MC Sarah Pierce Muzaffar Chishti and Sarah. Crisis within a Crisis: Immigration in the United States in a Time of COVID-19. MigrationpolicyOrg. 2020. Available online: https://www.migrationpolicy.org/article/crisis-within-crisis-immigration-time-covid-19 (accessed on 5 May 2021).
- CBP Announces March 2021 Operational Update. US Cust Bord Prot. Available online: https://www.cbp.gov/newsroom/national-media-release/cbp-announces-march-2021-operational-update (accessed on 5 May 2021).
- Child migrants: What Is happening at the US border? BBC News. 2021. Available online: https://www.bbc.com/news/world-us-canada-56405009 (accessed on 10 May 2021).
- Southwest Land Border Encounters|U.S. Customs and Border Protection. Available online: https://www.cbp.gov/newsroom/stats/southwest-land-border-encounters (accessed on 6 May 2021).
- Romano, S.D.; Blackstock, A.J.; Taylor, E.V.; El Burai Felix, S.; Adjei, S.; Singleton, C.-M. Trends in Racial and Ethnic Disparities in COVID-19 Hospitalizations, by Region-United States, March-December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 56, 560–565. [Google Scholar] [CrossRef]
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. COVID-19—Implications for the Health Care System|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/nejmsb2021088 (accessed on 5 May 2021).
- Millett, G.A.; Jones, A.T.; Benkeser, D.; Baral, S.; Mercer, L.; Beyrer, C. Assessing differential impacts of COVID-19 on black communities. Ann. Epidemiol. 2020, 47, 37–44. [Google Scholar] [CrossRef]
- Kirschner, K.L.; Iezzoni, L.I.; Shah, T. The Invisible COVID Workforce: Direct Care Workers for Those with Disabilities. Retrieved Sept. 2020, 1, 2020. [Google Scholar] [CrossRef]
- Ray, R. Why Are Blacks Dying at Higher Rates from COVID-19? Brookings. 2020. Available online: https://www.brookings.edu/blog/fixgov/2020/04/09/why-are-blacks-dying-at-higher-rates-from-covid-19/ (accessed on 16 August 2021).
- Selden, T.M.; Berdahl, T.A. COVID-19 and Racial/Ethnic Disparities in Health Risk, Employment, and Household Composition. Health Aff. 2020, 39, 1624–1632. [Google Scholar] [CrossRef] [PubMed]
- Anthony Fauci Compares Race Disparities of Coronavirus to AIDS Epidemic. Available online: https://nypost.com/2020/04/07/anthony-fauci-compares-race-disparities-of-coronavirus-to-aids-epidemic/ (accessed on 16 August 2021).
- Ralph, L.; Kevin, Z.; Daniel, Z.; Erich, H. A longitudinal study of convergence between Black and White COVID-19 Mortality: A County Fixed Effects Approach, The Lancet Regional Health-Americas. 2021. Available online: https://www.sciencedirect.com/science/article/pii/S2667193X2100003X (accessed on 16 August 2021).
- Gross Domestic Product by State, 4th Quarter 2020 and Annual 2020 (Preliminary)|U.S. Bureau of Economic Analysis (BEA). Available online: https://www.bea.gov/news/2021/gross-domestic-product-state-4th-quarter-2020-and-annual-2020-preliminary (accessed on 5 May 2021).
- Elhauge, E. The Fragmentation of U.S. Health Care: Causes and Solutions; Oxford University Press: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Our World In Data: Dataset—Current Health expenditure (% of GDP), Date Source: World Health Organization Global Health Expenditure database. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS (accessed on 6 May 2021).
- United States Census Bureau. Health Insurance Coverage in the United States: 2019. US Census Bur. Available online: https://www.census.gov/library/publications/2020/demo/p60-271.html (accessed on 5 May 2021).
- Healthcare Access and Quality Index, 2015, Our World in Data. Available online: https://ourworldindata.org/grapher/healthcare-access-and-quality-index?tab=chart&country=USA~SWE~CHE~NOR~NLD~AUS~JPN~AUT~DEU~FRA (accessed on 6 May 2021).
- Dorsett, M. Point of no Return: COVID-19 and the U.S. Healthcare System: An Emergency Physician’s Perspective|Science Advances. Available online: https://advances.sciencemag.org/content/6/26/eabc5354 (accessed on 5 May 2021).
- Himmelstein, D.U.; Woolhandler, S. The, U.S. Health Care System on the Eve of the COVID-19 Epidemic: A Summary of Recent Evidence on Its Impaired Performance. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7331107/ (accessed on 5 May 2021).
- Paavola, A. 266 Hospitals Furloughing Workers in Response to COVID-19. Available online: https://www.beckershospitalreview.com/finance/49-hospitals-furloughing-workers-in-response-to-covid-19.html (accessed on 5 May 2021).
- Baccini, L.; Brodeur, A.; Weymouth, S. The COVID-19 pandemic and the 2020 US presidential election. J. Popul. Econ. 2021, 34, 739–767. [Google Scholar] [CrossRef] [PubMed]
- Brooks, D.J.; Saad, L. The COVID-19 Responses of Men vs. Women. GallupCom. 2020. Available online: https://news.gallup.com/opinion/gallup/321698/covid-responses-men-women.aspx (accessed on 5 May 2021).
- Melillo, G. What We’re Reading: Additional Doses of Pfizer Vaccine Purchased; Walmart Sued Over Opioid Crisis; 2020 May Be Deadliest Year in US History. Available online: https://www.ajmc.com/view/what-we-re-reading-us-buys-more-pfizer-vaccine-walmart-sued-over-opioid-crisis-2020-s-deadly-toll (accessed on 16 August 2021).
- Kim, J.H.; Hotez, P.; Batista, C.; Ergonul, O.; Figueroa, J.P.; Gilbert, S. Operation Warp Speed: Implications for global vaccine security. Lancet Glob. Health 2021, 10, 140. [Google Scholar] [CrossRef]
- Baker, S.; Koons, C. Inside Operation Warp Speed’s $18 Billion Sprint for a Vaccine. BloombergCom. 2020. Available online: https://www.bloomberg.com/news/features/2020-10-29/inside-operation-warp-speed-s-18-billion-sprint-for-a-vaccine (accessed on 16 August 2021).
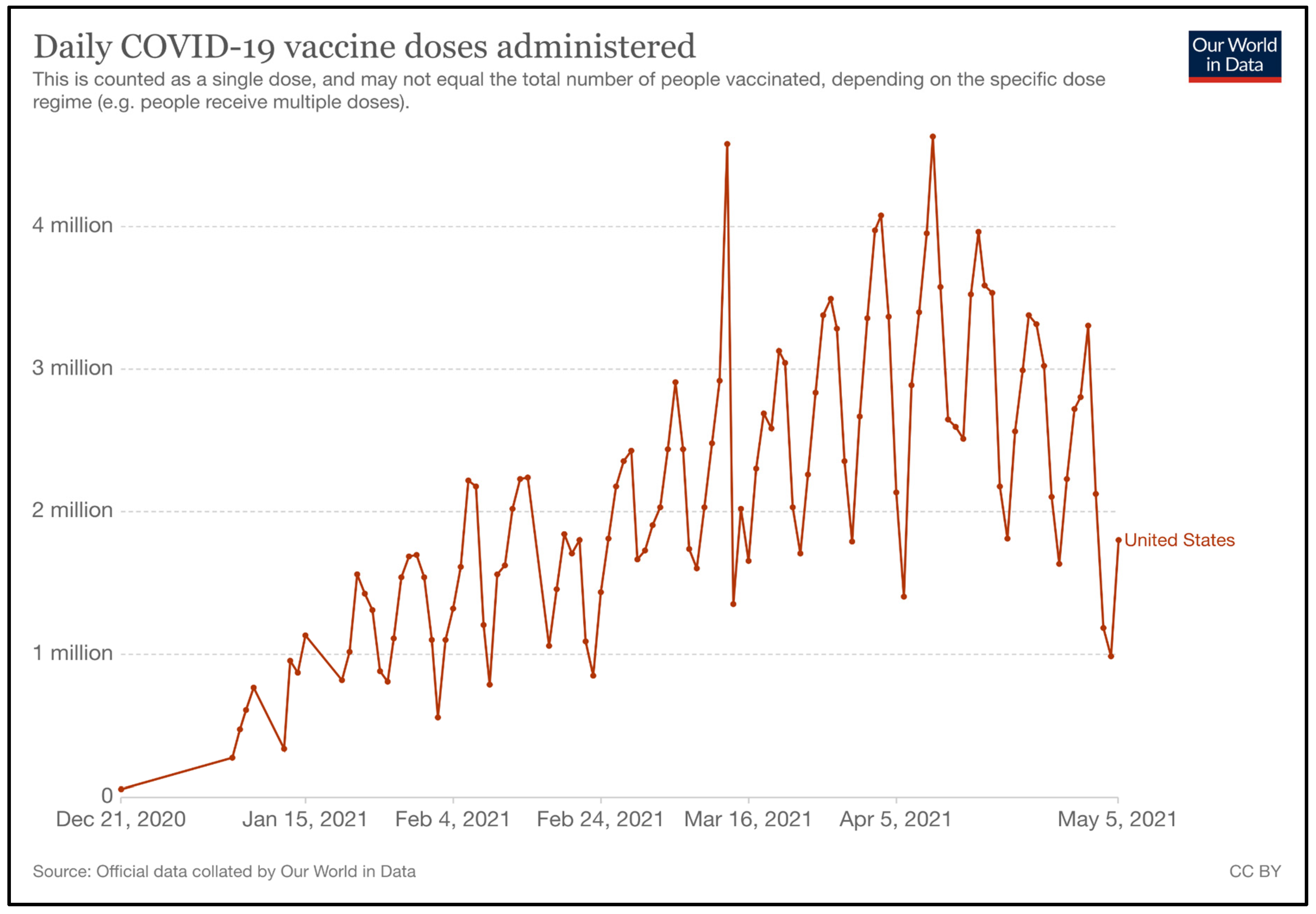
- US: Daily COVID-19 Vaccine Doses Administered. Our World Data n.d. Available online: https://ourworldindata.org/grapher/us-daily-covid-vaccine-doses-administered (accessed on 2 September 2021).
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Board on Health Sciences Policy; Committee on Equitable Allocation of Vaccine for the Novel Coronavirus. Kahn, B., Brown, L., Foege, W., Gayle, H., Eds.; Achieving Acceptance of COVID-19 Vaccine. In Framework for Equitable Allocation of COVID-19 Vaccine; National Academies Press (US): Washington, DC, USA, 2 October 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK564098/ (accessed on 6 May 2021).
- Zimet, G.D.; Silverman, R.D.; Fortenberry, J.D. Coronavirus Disease 2019 and Vaccination of Children and Adolescents: Prospects and Challenges. J. Pediatr. 2021, 231, 254–258. [Google Scholar] [CrossRef]
- Gayle, H.; Foege, W.; Brown, L.; Kahn, B. (Eds.) Medicine Framework for Equitable Allocation of COVID-19 Vaccine; The National Academies Press: Washington, DC, USA, 2020; 272p. [Google Scholar]
- Vaccinate with Confidence: COVID-19 Vaccines Strategy|CDC 2021. Available online: https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence/strategy.html (accessed on 5 May 2021).
- FACT SHEET: Biden Administration Announces Historic $10 Billion Investment to Expand Access to COVID-19 Vaccines and Build Vaccine Confidence in Hardest-Hit and Highest-Risk Communities. White House. 2021. Available online: https://www.whitehouse.gov/briefing-room/statements-releases/2021/03/25/fact-sheet-biden-administration-announces-historic-10-billion-investment-to-expand-access-to-covid-19-vaccines-and-build-vaccine-confidence-in-hardest-hit-and-highest-risk-communities/ (accessed on 5 May 2021).
- Watson, C.; Cicero, A.; Blumenstock, J.; Fraser, M. Johns Hopkins School of Public Health Center for Health Security and Association of State and Territorial Health Officials. In A National Plan to Enable Comprehensive COVID-19 Case Finding and Contact Tracing in the US; Johns Hopkins University: Baltimore, MD, USA, 2020. [Google Scholar]
- European Observatory on Health Systems and Policies; Rajan, S.; Cylus, J.; McKee, M. Successful find-test-trace-isolate-support systems: How to win at snakes and ladders. Eurohealth 2020, 26, 34–39. Available online: https://apps.who.int/iris/handle/10665/336292 (accessed on 6 May 2021).
- Grantz, K.; Lee, E.; D’Agostino, L. Maximizing and Evaluating the Impact of Test-Trace-Isolate Programs: A Modeling Study. Available online: https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1003585 (accessed on 25 June 2021).
- CDC. Health Departments. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tracing-training.html (accessed on 16 August 2021).
- Parmet, W.E.; Sinha, M.S. COVID-19—The Law and Limits of Quarantine. N. Engl. J. Med. 2020, 56, 4211. [Google Scholar] [CrossRef]
- Lewis, D. Why many countries failed at COVID contact-tracing—but some got it right. Nature 2020, 588, 384–387. [Google Scholar] [CrossRef]
- Fazio, M. How Mask Guidelines Have Evolved. New York Times, 27 April 2021. [Google Scholar]
- Stolberg, S.G.; Rabin, R.C.C.D.C. Eases Outdoor Mask Guidance for Vaccinated Americans. New York Times, 27 April 2021. [Google Scholar]
- New York Times. See How Vaccinations Are Going in Your County and State. New York Times. 2021. Available online: https://www.nytimes.com/interactive/2020/us/covid-19-vaccine-doses.html (accessed on 18 August 2021).
- California S of about COVID-19 Restrictions. Available online: https://covid19.ca.gov/stay-home-except-for-essential-needs/ (accessed on 5 May 2021).
- Michigan Medicine. MI COVID Response Data and Modeling Update. 2021. Available online: https://www.michigan.gov/documents/coronavirus/20210406_Data_and_modeling_update_vmediaT_002_721704_7.pdf (accessed on 6 May 2021).
- Infographic: The U.S. States Hit Hardest by COVID-19. Stat Infographics. Available online: https://www.statista.com/chart/24248/covid-19-death-rate-in-us-states/ (accessed on 6 May 2021).
- New York Times. New York City Coronavirus Map and Case Count. New York Times. 2021. Available online: https://www.nytimes.com/interactive/2021/us/new-york-covid-cases.html (accessed on 18 August 2021).
- Texas Coronavirus Map and Case Count-The New York Times. Available online: https://www.nytimes.com/interactive/2021/us/texas-covid-cases.html (accessed on 6 May 2021).
- Svitek, P. Texas Coronavirus Cases Haven’t Surged Since Gov. Greg Abbott Lifted the Mask Order. Experts Warn It’s too Soon to Celebrate. 2021. Available online: https://www.texastribune.org/2021/04/14/texas-coronavirus-mask-order-abbott/ (accessed on 6 May 2021).
- Hasell, J. Which Countries Have Protected Both Health and the Economy in the Pandemic? Our World Data. Available online: https://ourworldindata.org/covid-health-economy (accessed on 6 May 2021).
- United States Census Bureau. Initial Impact of COVID-19 on U.S. Economy More Widespread Than on Mortality. U S Census Bur. Available online: https://www.census.gov/library/stories/2021/03/initial-impact-covid-19-on-united-states-economy-more-widespread-than-on-mortality.html (accessed on 6 May 2021).
- Katz, J.; Lu, D.; Sanger-Katz, M. 574,000 More U.S. Deaths Than Normal Since COVID-19 Struck. New York Times, 24 March 2021. [Google Scholar]
- Polyakova, M.; Kocks, G.; Udalova, V.; Finkelstein, A. Initial economic damage from the COVID-19 pandemic in the United States is more widespread across ages and geographies than initial mortality impacts. Proc. Natl. Acad. Sci. USA 2020, 117, 27934–27939. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.K.; Weiss, M.A.; Schwarzenberg, A.B.; Nelson, R.M.; Sutter, K.M.; Sutherland, M.D. Global Economic Effects of COVID-19. Congr. Res. Serv. 2020, 10, 151. [Google Scholar]
- Weinstock, L.R. COVID-19 and the U.S. Economy. Congressional Research Service. 2021. Available online: https://crsreports.congress.gov/product/pdf/R/R46606 (accessed on 6 May 2021).
- Bergquist, S.; Otten, T.; Sarich, N. COVID-19 pandemic in the United States. Health Policy Technol. 2020, 9, 623–638. [Google Scholar] [CrossRef]
- Labonte, M. The Federal Reserve’s Response to COVID-19; Congressional Research Service: Washington, DC, USA, 2021. Available online: https://crsreports.congress.gov/product/pdf/R/R46411 (accessed on 6 May 2021).
- First Things First|McKinsey & Company. Available online: https://www.mckinsey.com/featured-insights/coronavirus-leading-through-the-crisis/charting-the-path-to-the-next-normal/first-things-first (accessed on 6 May 2021).
- CDC. Different COVID-19 Vaccines. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines.html (accessed on 6 May 2021).
- Sekar, K.; Bodie, A. Vaccine Safety in the United States: Overview and Considerations for COVID-19 Vaccines. Vaccines Oper. Warp Speed Regul. Saf. 2020, 14, 155–219. [Google Scholar]
- U.S. FDA. Emergency Use Authorization for Vaccines Explained; FDA: Silver Spring, MD, USA, 2020. Available online: https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained (accessed on 6 May 2021).
- U.S. FDA. COVID-19 Vaccines; FDA: Silver Spring, MD, USA, 2021.
- Pfizer-BioNTech COVID-19 Vaccine EUA Letter of Authorization Reissued 02-25-2021. Available online: https://www.fda.gov/media/144412/download (accessed on 6 May 2021).
- Pfizer Inc. Pfizer and Biontech Confirm High Efficacy and No Serious Safety Concerns Through up to Six Months Following Second Dose in Updated Topline Analysis of Landmark COVID-19 Vaccine Study; Pfizer Inc. & BioNTech: Mainz, Germany; New York, NY, USA, 2021. [Google Scholar]
- Interim Clinical Considerations for Use of COVID-19 Vaccines|CDC 2021. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/clinical-considerations.html (accessed on 6 May 2021).
- Pfizer and BioNTech Initiate Rolling Submission of Biologics License Application for U.S. FDA Approval of Their COVID 19 Vaccine|Pfpfizeruscom. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-initiate-rolling-submission-biologics (accessed on 9 May 2021).
- Pfizer-BioNTech Announce Positive Topline Results of Pivotal COVID-19 Vaccine Study in Adolescents|Pfpfizeruscom. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-biontech-announce-positive-topline-results-pivotal (accessed on 9 May 2021).
- U.S. FDA. Emergency Use Authorization for Pfizer-BioNTech COVID-19 Vaccine Review Memorandum; FDA: Silver Spring, MD, USA, 2020. Available online: https://www.fda.gov/media/144416/download (accessed on 6 May 2021).
- U.S. FDA. Moderna COVID-19 Vaccine; FDA: Silver Spring, MD, USA, 2021. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/moderna-covid-19-vaccine (accessed on 6 May 2021).
- ModernaTX, Inc. Moderna COVID-19 Vaccine EUA FDA Review Memorandum 2020; FDA: Silver Spring, MD, USA, 2021. Available online: https://www.fda.gov/media/144673/download (accessed on 6 May 2021).
- Moderna Reports First Quarter Fiscal Year 2021 Financial Results and Provides Business Updates|Moderna, Inc. Available online: https://investors.modernatx.com/news-releases/news-release-details/moderna-reports-first-quarter-fiscal-year-2021-financial-results/ (accessed on 9 May 2021).
- Janssen Biotech, Inc. Janssen COVID-19 Vaccine EUA Letter of Authorization. 2021. Available online: https://www.fda.gov/media/146303/download (accessed on 6 May 2021).
- U.S. FDA. Janssen COVID-19 Vaccine EUA FDA Review Memorandum 2021; FDA: Silver Spring, MD, USA, 2021. Available online: https://www.fda.gov/media/146338/download (accessed on 6 May 2021).
- Johnson & Johnson Single-Shot COVID-19 Vaccinations to Resume in the U.S. for All Adults Aged 18 and Older Following CDC and FDA Decision|Johnson & Johnson. Content Lab US. Available online: https://www.jnj.com/johnson-johnson-single-shot-covid-19-vaccinations-to-resume-in-the-u-s-for-all-adults-aged-18-and-older-following-cdc-and-fda-decision (accessed on 9 May 2021).
- Johnson & Johnson Expands Phase 2a Clinical Trial of COVID-19 Vaccine Candidate to Include Adolescents|Johnson & Johnson. Content Lab US. Available online: https://www.jnj.com/johnson-johnson-expands-phase-2a-clinical-trial-of-covid-19-vaccine-candidate-to-include-adolescents (accessed on 9 May 2021).
- Pfizer and BioNTech Announce an Agreement with U.S. Government for up to 600 Million Doses of mRNA-Based Vaccine Candidate Against SARS-CoV-2|pfpfizeruscom. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-agreement-us-government-600 (accessed on 6 May 2021).
- Pfizer and BioNTech to Supply the U.S. with 100 Million Additional Doses of COVID-19 Vaccine|pfpfizeruscom. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-supply-us-100-million-additional-doses (accessed on 6 May 2021).
- CDC. Key Things to Know about COVID-19 Vaccines. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html (accessed on 6 May 2021).
- Moderna Provides Clinical and Supply Updates on COVID-19 Vaccine Program Ahead of 2nd Annual Vaccines Day|Moderna, Inc. Available online: https://investors.modernatx.com/news-releases/news-release-details/moderna-provides-clinical-and-supply-updates-covid-19-vaccine/ (accessed on 6 May 2021).
- Moderna Announces Shipment of 100 Millionth Dose of its COVID-19 Vaccine to the U.S. Government|Moderna, Inc. Available online: https://investors.modernatx.com/news-releases/news-release-details/moderna-announces-shipment-100-millionth-dose-its-covid-19/ (accessed on 6 May 2021).
- Siddalingaiah, S.V. Operation Warp Speed Contracts for COVID 19 Vaccines and Ancillary Vaccination Materials; Congressional Research Service: Washington, DC, USA, 2021. Available online: https://crsreports.congress.gov/product/pdf/IN/IN11560 (accessed on 6 May 2021).
- Johnson & Johnson. Johnson & Johnson Announces U.S. CDC Advisory Committee Recommends First Single-Shot COVID-19 Vaccine for Adults 18 and Older in U.S.; Johnson & Johnson: New Brunswick, NJ, USA, 2021. [Google Scholar]
- BARDA’S Rapidly-Expanding COVID-19 Medical Countermeasure Portfolio. Available online: https://www.medicalcountermeasures.gov/app/barda/coronavirus/COVID19.aspx (accessed on 6 May 2021).
- Coronavirus: Operation Warp Speed. Available online: https://www.defense.gov/Explore/Spotlight/Coronavirus/Operation-Warp-Speed/ (accessed on 6 May 2021).
- WHO Team on Emergencies Preparedness, Strategic Advisory Group of Experts on Immunization. WHO SAGE Framework Allocation and Prioritization 2020, WHO Headquarters (HQ). 2020. Available online: https://www.who.int/publications/i/item/who-sage-values-framework-for-the-allocation-and-prioritization-of-covid-19-vaccination (accessed on 18 August 2021).
- ACIP General Information|CDC. 2020. Available online: https://www.cdc.gov/vaccines/acip/committee/index.html (accessed on 6 May 2021).
- Dooling, K. Phased Allocation of COVID-19 Vaccines. 2020. Available online: https://stacks.cdc.gov/view/cdc/105184 (accessed on 6 May 2021).
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, 3097. [Google Scholar] [CrossRef] [PubMed]
- Erdem, H.; Lucey, D.R. Healthcare worker infections and deaths due to COVID-19: A survey from 37 nations and a call for WHO to post national data on their website. Int. J. Infect. Dis. 2021, 102, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Evidence Table for COVID-19 Vaccines Allocation in Phase 1a of the Vaccination Program|CDC. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19/evidence-table.html (accessed on 6 May 2021).
- New York Times. Nearly One-Third of U.S. Coronavirus Deaths Are Linked to Nursing Homes. New York Time. 2020. Available online: https://www.nytimes.com/interactive/2020/us/coronavirus-nursing-homes.html (accessed on 18 August 2021).
- Dooling, K. The Advisory Committee on Immunization Practices’ Updated Interim Recommendation for Allocation of COVID-19 Vaccine—United States, December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 69, 695152e2. [Google Scholar] [CrossRef]
- Categories of Essential Workers: COVID-19 Vaccination|CDC. 2021. Available online: https://www.cdc.gov/vaccines/covid-19/categories-essential-workers.html (accessed on 6 May 2021).
- Evidence Table for COVID-19 Vaccines Allocation in Phases 1b and 1c of the Vaccination Program|CDC. 2021. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19/evidence-table-phase-1b-1c.html (accessed on 6 May 2021).
- Biden Aims for 70% of U.S. Adults to Get One Vaccine Dose by July 4|Reuters. Available online: https://www.reuters.com/world/us/biden-set-outline-plans-make-vaccine-doses-more-accessible-2021-05-04/ (accessed on 25 June 2021).
- Affairs (ASPA) AS for P. COVID-19 Vaccine Distribution: The Process. HHSGov. 2020. Available online: https://www.hhs.gov/coronavirus/covid-19-vaccines/distribution/index.html (accessed on 6 May 2021).
- CDC. COVID-19 Vaccination: How COVID-19 Vaccines Get to You. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/distributing.html (accessed on 6 May 2021).
- VTrckS: Vaccine Tracking System|CDC. 2021. Available online: https://www.cdc.gov/vaccines/programs/vtrcks/index.html (accessed on 6 May 2021).
- COVID-19 Vaccine U.S. Distribution Fact Sheet|Pfpfizeruscom. Available online: https://www.pfizer.com/news/hot-topics/covid_19_vaccine_u_s_distribution_fact_sheet (accessed on 6 May 2021).
- Coronavirus Vaccine Support for COVID-19|McKesson. Available online: https://www.mckesson.com/About-McKesson/COVID-19/Vaccine-Support/ (accessed on 6 May 2021).
- Vaccines Storage and Handling Toolkit|CDC 2021. Available online: https://www.cdc.gov/vaccines/hcp/admin/storage/toolkit/index.html (accessed on 6 May 2021).
- From the Factory to the Frontlines: The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine. Rural Spotlight. 2020. Available online: https://ruralhealthinfocenter.health.mo.gov/from-the-factory-to-the-frontlines-the-operation-warp-speed-strategy-for-distributing-a-covid-19-vaccine/ (accessed on 6 September 2021).
- Coronavirus (COVID-19) Vaccinations-Statistics and Research. Our World Data. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 7 May 2021).
- Interim Public Health Recommendations for Fully Vaccinated People|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated-guidance.html (accessed on 6 May 2021).
- CDC. COVID-19 and Your Health. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/travelers/travel-during-covid19.html (accessed on 6 May 2021).
- WHO Lists Additional COVID-19 Vaccine for Emergency Use and Issues Interim Policy Recommendations. Available online: https://www.who.int/news/item/07-05-2021-who-lists-additional-covid-19-vaccine-for-emergency-use-and-issues-interim-policy-recommendations (accessed on 25 June 2021).
- Sonani, B.; Aslam, F.; Goyal, A.; Patel, J.; Bansal, P. COVID-19 vaccination in immunocompromised patients. Clin. Rheumatol. 2021, 7, 1–2. [Google Scholar] [CrossRef]
- Clinical Immunization Safety Assessment (CISA) Project|CISA|Monitoring|Ensuring Safety|Vaccine Safety|CDC. 2020. Available online: https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/cisa/index.html (accessed on 6 May 2021).
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L. Preliminary Findings of mRNA COVID-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 4, 4983. [Google Scholar] [CrossRef]
- CDC. V-safe After Vaccination Health Checker. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/vsafe.html (accessed on 6 May 2021).
- Vaccine Safety Monitoring|Vaccine Safety|CDC. 2020. Available online: https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/index.html (accessed on 6 May 2021).
- VAERS-Data. Available online: https://vaers.hhs.gov/data.html (accessed on 6 May 2021).
- CDC. Healthcare Workers. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/therapeutic-options.html (accessed on 24 June 2021).
- Therapeutic Management. COVID-19 Treat Guidel. Available online: https://www.covid19treatmentguidelines.nih.gov/management/therapeutic-management/ (accessed on 24 June 2021).
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet Lond. Engl. 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Spinner, C.D.; Gottlieb, R.L.; Criner, G.J.; Arribas López, J.R.; Cattelan, A.M.; Soriano Viladomiu, A. Effect of Remdesivir vs. Standard Care on Clinical Status at 11 Days in Patients with Moderate COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1048–1057. [Google Scholar] [CrossRef]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C. Remdesivir for the Treatment of COVID-19-Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients with Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef]
- Jeronimo, C.M.P.; Farias, M.E.L.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C. Methylprednisolone as Adjunctive Therapy for Patients Hospitalized with Coronavirus Disease 2019 (COVID-19; Metcovid): A Randomized, Double-blind, Phase IIb, Placebo-controlled Trial. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, e373–e381. [Google Scholar] [CrossRef]
- Angus, D.C.; Derde, L.; Al-Beidh, F.; Annane, D.; Arabi, Y.; Beane, A. Effect of Hydrocortisone on Mortality and Organ Support in Patients with Severe COVID-19: The REMAP-CAP COVID-19 Corticosteroid Domain Randomized Clinical Trial. JAMA 2020, 324, 1317–1329. [Google Scholar] [CrossRef]
- Tocilizumab in Patients Admitted to Hospital with COVID-19 (RECOVERY): Preliminary Results of a Randomised, Controlled, Open-Label, Platform Trial|Medrxiv. Available online: https://www.medrxiv.org/content/10.1101/2021.02.11.21249258v1 (accessed on 24 June 2021).
- REMAP-CAP Investigators; Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, L.B.; Kristen, E.; Broady, W.; Edelberg, J. Ten Facts about COVID-19 and the U.S. Economy. Brookings. 2020. Available online: https://www.brookings.edu/research/ten-facts-about-covid-19-and-the-u-s-economy/ (accessed on 6 May 2021).
- Rader, B.; Astley, C.M.; Sy, K.T.L.; Sewalk, K.; Hswen, Y.; Brownstein, J.S. Geographic access to United States SARS-CoV-2 testing sites highlights healthcare disparities and may bias transmission estimates. J. Travel. Med. 2020, 27, taaa076. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Yue, H.; Wang, C.; She, B.; Ye, X.; Liu, R. Racial Segregation, Testing Site Access, and COVID-19 Incidence Rate in Massachusetts, USA. Int. J. Environ. Res. Public Health 2020, 17, 9528. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.H.; Bonds, J.M.; Parnell, A.M.; Bright, C.M. Coronavirus Vaccine Distribution: Moving to a Race Conscious Approach for a Racially Disparate Problem. J. Racial. Ethn. Health Disparities 2021, 8, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Bureau, U.C. American Community Survey 5-Year Data (2009–2019). US Census Bur. Available online: https://www.census.gov/data/developers/data-sets/acs-5year.html (accessed on 30 August 2021).
- A Three-Tiered Approach to Address Barriers to COVID-19 Vaccine Delivery in the Black Community-The Lancet Global Health. Available online: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(21)00099-1/fulltext (accessed on 30 August 2021).
- Yu, S.W.Y.; Hill, C.; Ricks, M.L.; Bennet, J.; Oriol, N.E. The scope and impact of mobile health clinics in the United States: A literature review. Int. J. Equity Health 2017, 16, 178. [Google Scholar] [CrossRef]
- CDC. COVID Data Tracker: Variant Proportions. Available online: https://covid.cdc.gov/covid-data-tracker/#variant-proportions (accessed on 16 August 2021).
- CDC. Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html (accessed on 16 August 2021).
- Coronavirus (COVID-19) Cases-Statistics and Research. Our World Data. Available online: https://ourworldindata.org/covid-cases (accessed on 6 May 2021).
- Office USGA. Operation Warp Speed: Accelerated COVID-19 Vaccine Development Status and Efforts to Address Manufacturing Challenges. Available online: https://www.gao.gov/products/gao-21-319 (accessed on 6 May 2021).
- A Global Pandemic Requires a World Effort to End It–None of Us Will Be Safe until Everyone Is Safe. Available online: https://www.who.int/news-room/commentaries/detail/a-global-pandemic-requires-a-world-effort-to-end-it-none-of-us-will-be-safe-until-everyone-is-safe (accessed on 6 May 2021).
- United States to Host Launch Event for Gavi COVAX AMC 2021 Investment Opportunity. Available online: https://www.gavi.org/news/media-room/united-states-host-launch-event-gavi-covax-amc-2021-investment-opportunity (accessed on 6 May 2021).
- Maxmen, A. In shock move, US backs waiving patents on COVID vaccines. Nature 2021, 38, 2243. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| California | Michigan | New York | Texas | |
|---|---|---|---|---|
| Population | 39.5 M | 9.9 M | 19.5 M | 29 M |
| Cases | ||||
| Total Reported | 3,748,832 | 948,029 | 2,057,701 | 2,904,178 |
| 7-Day Average * + (14-Day-Change) | 1766 (−25%) | 3594 (−48%) | 3148 (−46%) | 3097 (−4%) |
| Deaths | ||||
| Total Reported | 61,996 | 19,041 | 51,949 | 50,567 |
| 7-Day Average * + (14-Day-Change) | 70 (−14%) | 70 (+15%) | 52 (−17%) | 53 (−1%) |
| NPIs | Some businesses closed | Businesses mostly open | Businesses mostly open | Businesses open |
| Masks mandatory indoors | Masks mandatory indoors | Masks mandatory indoors | Masks not mandatory | |
| Stay-at-home advisory | ||||
| Doses Distributed to State | 39,630,080 | 9,500,250 | 19,018,995 | 25,514,685 |
| Doses Administered to State | 31,185,031 | 7, 281,555 | 15,980,527 | 19,205,116 |
| Percentage of Distributed Vaccines Administered | 78 | 76 | 84 | 75 |
| Percentage Fully Vaccinated | 32% | 33% | 36% | 28% |
| Vaccine | Dose | Dose Volume | Number of Doses/Series | Interval Between Doses | Active Ingredients | Inactive Ingredients |
|---|---|---|---|---|---|---|
| Pfizer-BioNTech | 30 µg | 0.3 mL | 2 | 21 days | Nucleoside-modified mRNA encoding the viral spike (S) glycoprotein of SARS-CoV-2 | 2[(polyethylene glycol (PEG))-2000]-N,N-ditetradecylacetamide 1,2-distearoyl-sn-glycero-3-phosphocholine Cholesterol (4-hydroxybutyl) azanediyl) bis(hexane-6,1-diyl) bis(2-hexyldecanoate) Sodium chloride Monobasic potassium phosphate Potassium chloride Dibasic sodium phosphate dihydrate Sucrose |
| Moderna | 100 µg | 0.5 mL | 2 | 28 days | Nucleoside-modified mRNA encoding the viral spike (S) glycoprotein of SARS-CoV-2 | PEG2000-DMG: 1,2-dimyristoyl-rac-glycerol, methoxypolyethylene glycol 1,2-distearoyl-sn-glycero-3-phosphocholine Cholesterol SM-102: heptadecan-9-yl 8-((2-hydroxyethyl) (6-oxo-6-(undecyloxy) hexyl) amino) octanoate Tromethamine Tromethamine hydrochloride Acetic acid Sodium acetate Sucrose |
| Johnson & Johnson | 5 × 1010 viral particles | 0.5 mL | 1 | N/A | Recombinant, replication- incompetent Ad26 vector, encoding a stabilized variant of the SARS-CoV-2 Spike (S) protein | Polysorbate-80 2-hydroxypropyl-β- cyclodextrin Citric acid monohydrate Trisodium citrate dihydrate Sodium chloride Ethanol |
| Study Number | Phases | Description | BNT162b2— Number of Participants | Placebo— Number of Participants |
|---|---|---|---|---|
| C4591001 | 1, 2, and 3 | Randomized, placebo-controlled, observer-blind. Evaluation: Efficacy, safety and immunogenicity. | Phase 1: 24 Phase 2/3: 21,823 | Phase 1: 6 Phase 2/3: 21,828 |
| BNT162-01 | 1 and 2 | Randomized, open-label. Evaluation: Safety, immunogenicity and dose escalation. | Phase 1/2: 12 | Phase 1/2: 0 |
| Study Number | Phases | Description | mRNA-1273— Number of Participants | Placebo— Number of Participants |
|---|---|---|---|---|
| P301 | 3 | Randomized, placebo-controlled, observer-blind, stratified. Evaluation: Efficacy and safety. | Phase 3: 15,181 | Phase 3: 15,170 |
| P201 | 2 | Randomized, placebo-controlled observer-blind, dose-confirmation. Evaluation: Immunogenicity and safety. | ||
| 20-0003 | 1 | Open-label, dose-ranging. Evaluation: Immunogenicity and safety. |
| Study Number | Phases | Description | Ad26.COV2.S— Number of Participants | Placebo— Number of Participants |
|---|---|---|---|---|
| 3001 | 3 | Randomized, double-blind, placebo-controlled. Evaluation: Efficacy and safety. | Phase 3: 21,895 | Phase 3: 21,888 |
| 3009 | 3 | Randomized, double-blind, placebo-controlled. Evaluation: Efficacy and safety. | ||
| 2001 | 2a | Randomized, double-blind, placebo-controlled. Evaluation: Immunogenicity and safety. | ||
| 1002 | 1 | Randomized, double-blind, placebo-controlled. Evaluation: Immunogenicity and safety. | ||
| 1001 | 1/2a | Randomized, double-blind, placebo-controlled. Evaluation: Immunogenicity and safety. |
| Company | Type | Contract Value | Specifications | Doses Per Person | Current Phase (Preliminary Effectiveness–U.S. Strain) | Storage |
|---|---|---|---|---|---|---|
| Pfizer- BioNTech | mRNA | $5.97B | 300 million doses | 2 | Phase II/III (95%) EUA Issued | Ultra Cold Storage (−70 °C) |
| Moderna | mRNA | $4.94B $954M | 300 million doses Development | 2 | Phase III (94.5%) EUA Issued | Cold Storage (6 mos, −20 °C) Refrigerator (30 days, −2 to −8 °C) |
| Janssen/Johnson & Johnson | Viral Vector | $1B $456M | 100 million doses Development | 1 | Phase III (72%) EUA Issued | Refrigerator (3 mos, −2 to −8 °C) |
| Company | Contract Value | Specifications |
|---|---|---|
| ApiJect Systems America | $138 million | 100 million prefilled syringes by the end of 2020 Expansion of manufacturing capacity to produce 500 million prefilled syringes in 2021. |
| Corning Pharmaceutical Technologies | $204 million | Expansion of manufacturing capacity to produce an additional 164 million Valor Glass vials per year if needed. |
| SiO2 Materials Science | $143 million | Expansion of manufacturing capacity to produce 120 million glass-coated plastic containers per year if needed. |
| Becton, Dickinson and Co. | $42.3 million | Expansion of manufacturing capacity to produce needles and syringes. |
| Smiths Medical, Inc. | $20.6 million | Expansion of manufacturing capacity to produce needles and syringes. |
| Goldbelt Security, LLC | $125 million | 530 million needles and syringes. |
| Retractable Technologies, Inc. | $53.6 million | Expansion of manufacturing capacity to produce safety needles and syringes. |
| Retractable Technologies, Inc. | $93.8 million | 320 million needles and syringes. |
| Marathon Medical Corp. | $27.5 million | |
| Duopross Meditech Corporation | $48 million | 134 million safety syringes by the end of 2020. |
| Cardinal Health Inc. | $15 million | 500 million safety syringes over a 12-month period (August 2020–August 2021). |
| Gold Coast Medical Supply, LP | $14 million | |
| HTL STREFA Inc. | $12 million | |
| Quality Impact, Inc. | $9 million | |
| Medline Industries, Inc. | $6 million |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amara, S.A.; Díaz, E.D.; Menon, L.K.; Singh, P.; Rozanova, L.; Flahault, A. COVID-19 Outbreak Management and Vaccination Strategy in The United States of America. Epidemiologia 2021, 2, 426-453. https://doi.org/10.3390/epidemiologia2030031
Amara SA, Díaz ED, Menon LK, Singh P, Rozanova L, Flahault A. COVID-19 Outbreak Management and Vaccination Strategy in The United States of America. Epidemiologia. 2021; 2(3):426-453. https://doi.org/10.3390/epidemiologia2030031
Chicago/Turabian StyleAmara, Sara Aicha, Estefany Daniella Díaz, Lakshmi Krishna Menon, Priyanka Singh, Liudmila Rozanova, and Antoine Flahault. 2021. "COVID-19 Outbreak Management and Vaccination Strategy in The United States of America" Epidemiologia 2, no. 3: 426-453. https://doi.org/10.3390/epidemiologia2030031
APA StyleAmara, S. A., Díaz, E. D., Menon, L. K., Singh, P., Rozanova, L., & Flahault, A. (2021). COVID-19 Outbreak Management and Vaccination Strategy in The United States of America. Epidemiologia, 2(3), 426-453. https://doi.org/10.3390/epidemiologia2030031