Correlation between Helicobacter pylori Infection and Gastric Atrophy Examined in the Sera of Mongolian People

 and
and
Abstract
1. Introduction
2. Results
2.1. Detection of Anti-H. pylori Antibodies in the Sera of Mongolian People by Two Different ELISA Kits
2.2. Detection of Anti-CagA Antibodies in the Sera of Mongolian People
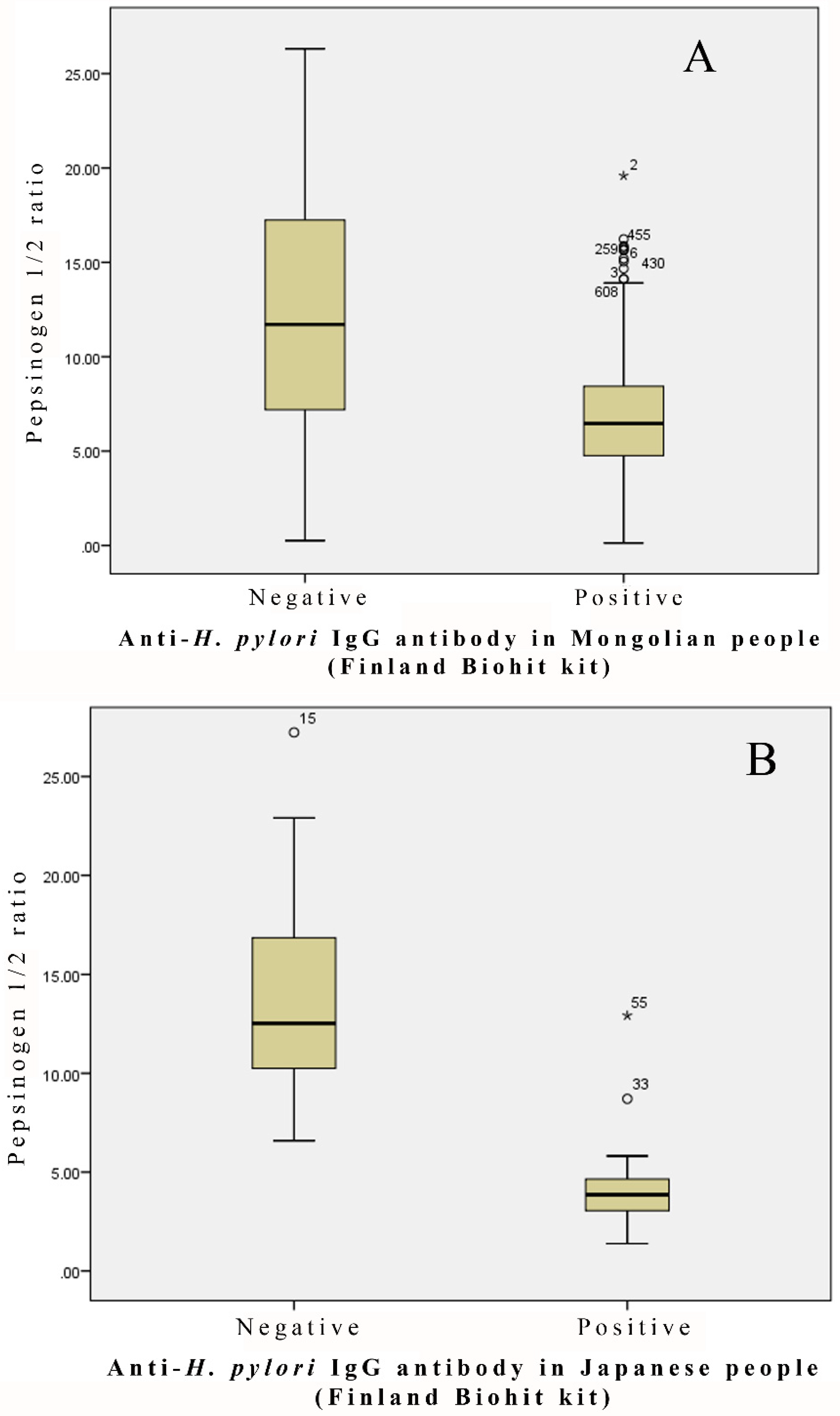
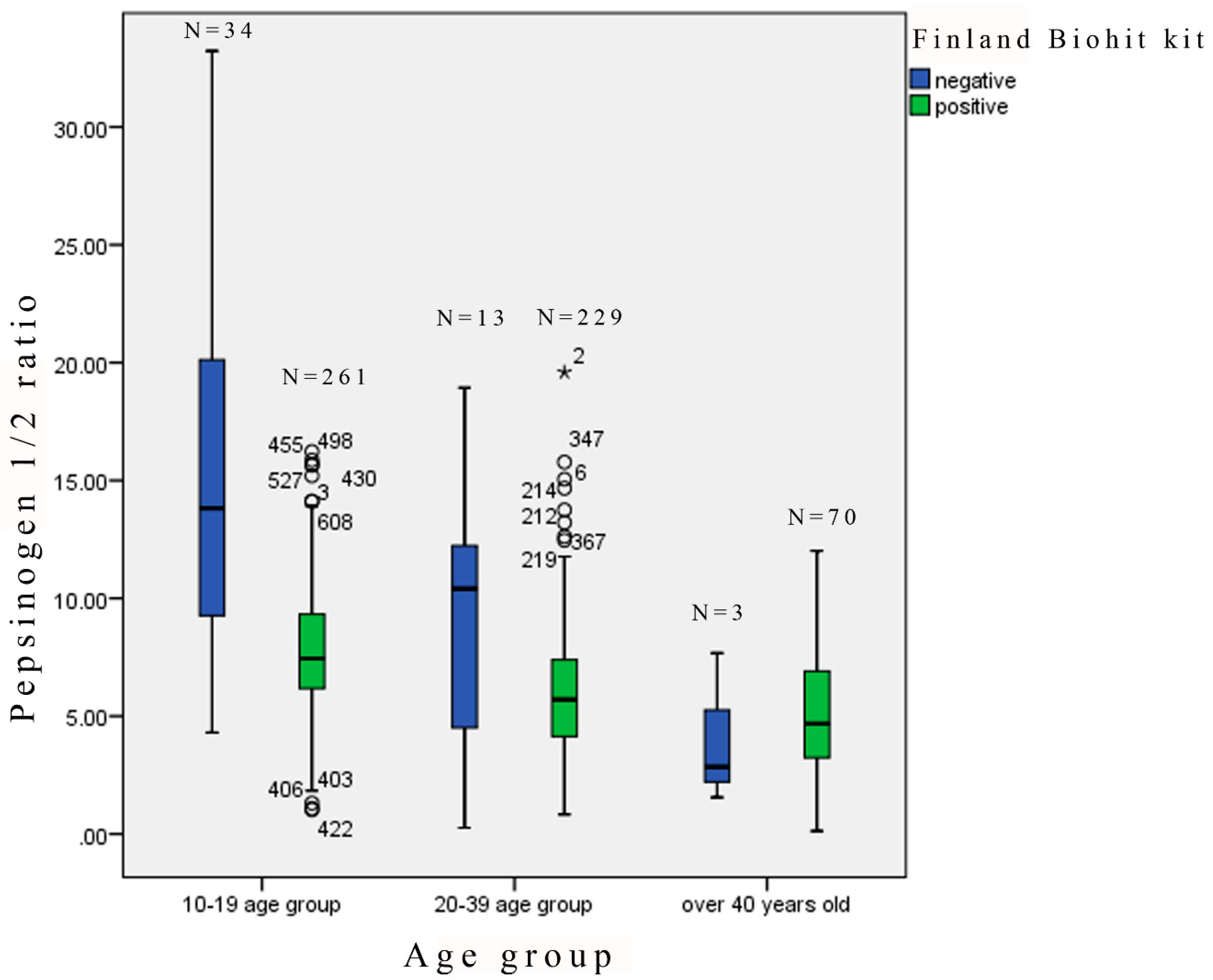
2.3. Relationship between the Ratio of Pepsinogen 1/2 and H. pylori Infection
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Detection of Antibodies against H. pylori, CagA, and Pepsinogens in Serum Specimens
4.3. Ethics
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- IARC. Schistosomes, Liver Flukes and Helicobacter Pylori; IARC: Lyon, France, 1994; Volume 61. [Google Scholar]
- Kuipers, E.J. Review article: Exploring the link between Helicobacter pylori and gastric cancer. Aliment. Pharmacol. Ther. 1999, 13, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Parsonnet, J.; Isaacson, P.G. Bacterial infection and MALT lymphoma. N. Engl. J. Med. 2004, 350, 213–215. [Google Scholar] [CrossRef]
- Ekstrom, A.M.; Held, M.; Hansson, L.E.; Engstrand, L.; Nyrén, O. Helicobacter pylori in gastric cancer established by CagA immunoblot as a marker of past infection. Gastroenterology 2001, 121, 784–791. [Google Scholar] [CrossRef]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori infection and the development of gastric cancer. N. Engl. J. Med. 2001, 345, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.R.; Won, Y.J.; Jung, K.W.; Kong, H.J.; Yim, S.H.; Lee, J.K.; Noh, H.I.; Lee, J.K.; Pisani, P.; Park, J.G.; et al. Nationwide cancer incidence in Korea, 1999~2001; first result using the national cancer incidence database. Cancer Res. Treat. 2005, 37, 325–331. [Google Scholar] [CrossRef]
- Nomura, K. (Ed.) Cancer Statistics in Japan 2005; Foundation for Promotion of Cancer Reseach (FPCR): Tokyo, Japan, 2005. [Google Scholar]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA-A Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- State Implementing Agency of Health, G.O.M. (Ed.) Health Indicators 2003; State Implementing Agency of Health, G.O.M.: Ulaanbaatar, Mongolia, 2003. [Google Scholar]
- State Implementing Agency of Health, G.O.M. (Ed.) Health Indicators 2011; State Implementing Agency of Health, G.O.M.: Ulaanbaatar, Mongolia, 2011. [Google Scholar]
- Frenck, R.W., Jr.; Clemens, J. Helicobacter in the developing world. Microb. Infect. 2003, 5, 705–713. [Google Scholar] [CrossRef]
- Rothenbacher, D.; Brenner, H. Burden of Helicobacter pylori and H. pylori-related diseases in developed countries: Recent developments and future implications. Microb. Infect. 2003, 5, 693–703. [Google Scholar] [CrossRef]
- van Doorn, L.J.; Figueiredo, C.; Sanna, R.; Plaisier, A.; Schneeberger, P.; de Boer, W.; Quint, W. Clinical relevance of the cagA, vacA, and iceA status of Helicobacter pylori. Gastroenterology 1998, 115, 58–66. [Google Scholar] [CrossRef]
- Ashour, A.A.; Magalhães, P.P.; Mendes, E.N.; Collares, G.B.; De Gusmão, V.R.; Queiroz, D.M.; Nogueira, A.M.M.; Rocha, G.A.; De Oliveira, C.A. Distribution of vacA genotypes in Helicobacter pylori strains isolated from Brazilian adult patients with gastritis, duodenal ulcer or gastric carcinoma. FEMS Immunol. Med. Microbiol. 2002, 33, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Woo, C.W.; Lee, Y.M.; Son, B.R.; Kim, J.W.; Chae, H.B.; Youn, S.J.; Park, S.M. Genotyping CagA, VacA subtype, IceA1, and BabA of Helicobacter pylori isolates from Korean patients, and their association with gastroduodenal diseases. J. Korean Med. Sci. 2001, 16, 579–584. [Google Scholar] [CrossRef]
- Asrat, D.; Nilsson, I.; Mengistu, Y.; Kassa, E.; Ashenafi, S.; Ayenew, K.; Wadström, T.; Abu-Al-Soud, W. Prevalence of Helicobacter pylori vacA and cagA genotypes in Ethiopian dyspeptic patients. J. Clin. Microbiol. 2004, 42, 2682–2684. [Google Scholar] [CrossRef]
- Azuma, T.; Yamakawa, A.; Yamazaki, S.; Fukuta, K.; Ohtani, M.; Ito, Y.; Dojo, M.; Yamazaki, Y.; Kuriyama, M. Correlation between variation of the 3′ region of the cagA gene in Helicobacter pylori and disease outcome in Japan. J. Infect. Dis. 2002, 186, 1621–1630. [Google Scholar] [CrossRef]
- Oishi, Y.; Kiyohara, Y.; Kubo, M.; Tanaka, K.; Tanizaki, Y.; Ninomiya, T.; Doi, Y.; Shikata, K.; Yonemoto, K.; Shirota, T.; et al. The serum pepsinogen test as a predictor of gastric cancer—The Hisayama study. Am. J. Epidemiol. 2006, 163, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Dinis-Ribeiro, M.; da Costa-Pereira, A.; Lopes, C.; Barbosa, J.; Guilherme, M.; Moreira-Dias, L.; Lomba-Viana, H.; Silva, R.; Abreu, N.; Lomba-Viana, R. Validity of serum pepsinogen I/II ratio for the diagnosis of gastric epithelial dysplasia and intestinal metaplasia during the follow-up of patients at risk for intestinal-type gastric adenocarcinoma. Neoplasia 2004, 6, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Bornschein, J.; Selgrad, M.; Wex, T.; Kuester, D.; Malfertheiner, P. Serological assessment of gastric mucosal atrophy in gastric cancer. BMC Gastroenterol. 2012, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Waterboer, T.; Dondog, B.; Michael, K.M.; Michel, A.; Schmitt, M.; Vaccarella, S.; Franceschi, S.; Clifford, G.; Pawlita, M. Dried blood spot samples for seroepidemiology of infections with human papillomaviruses, Helicobacter pylori, Hepatitis C Virus, and JC Virus. Cancer Epidemiol. Biomark. Prev. 2012, 21, 287–293. [Google Scholar] [CrossRef]
- Khasag, O.; Boldbaatar, G.; Tegshee, T.; Duger, D.; Dashdorj, A.; Uchida, T.; Matsuhisa, T.; Yamaoka, Y. The prevalence of Helicobacter pylori infection and other risk factors among Mongolian dyspeptic patients who have a high incidence and mortality rate of gastric cancer. Gut Pathog. 2018, 10, 14. [Google Scholar]
- Dunn, B.E.; Cohen, H.; Blaser, M.J. Helicobacter pylori. Clin. Microbiol. Rev. 1997, 10, 720–741. [Google Scholar] [CrossRef]
- Obata, Y.; Kikuchi, S.; Miwa, H.; Yagyu, K.; Lin, Y.; Ogihara, A. Diagnostic accuracy of serological kits for Helicobacter pylori infection with the same assay system but different antigens in a Japanese patient population. J. Med. Microbiol. 2003, 52, 889–892. [Google Scholar] [CrossRef] [PubMed]
- Marchildon, P.A.; Sugiyama, T.; Fukada, Y.; Peacock, J.S.; Asaka, M.; Shimoyama, T.; Graham, D.Y. Evaluation of the effects of strain-specific antigen variation on the accuracy of serologic diagnosis of Helicobacter pylori infection. J. Clin. Microbiol. 2003, 41, 1480–1485. [Google Scholar] [CrossRef]
- Megraud, F.; Lehours, P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin. Microbiol. Rev. 2007, 20, 280–322. [Google Scholar] [CrossRef]
- Okuda, M.; Miyashiro, E.; Koike, M.; Tanaka, T.; Bouoka, M.; Okuda, S.; Yoshikawa, N. Serodiagnosis of Helicobacter pylori infection is not accurate for children aged below 10. Pediatr. Int. 2002, 44, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Nasrollahzadeh, D.; Aghcheli, K.; Sotoudeh, M.; Shakeri, R.; Persson, E.C.; Islami, F.; Kamangar, F.; Abnet, C.C.; Boffetta, P.; Engstrand, L.; et al. Accuracy and cut-off values of pepsinogens I, II and gastrin 17 for diagnosis of gastric fundic atrophy: Influence of gastritis. PLoS ONE 2011, 6, e26957. [Google Scholar] [CrossRef]
- Weck, M.N.; Gao, L.; Brenner, H. Helicobacter pylori infection and chronic atrophic gastritis: Associations according to severity of disease. Epidemiology 2009, 20, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Varis, K.; Sipponen, P.; Laxen, F.; Samloff, I.M.; Huttunen, J.K.; Taylor, P.R.; Heinonen, O.P.; Albanes, D.; Sande, N.; Virtamo, J.; et al. Implications of serum pepsinogen I in early endoscopic diagnosis of gastric cancer and dysplasia. Helsinki Gastritis Study Group. Scand. J. Gastroenterol. 2000, 35, 950–956. [Google Scholar]
- Vannella, L.; Lahner, E.; Annibale, B. Risk for gastric neoplasias in patients with chronic atrophic gastritis: A critical reappraisal. World J. Gastroenterol. 2012, 18, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Broutet, N.; Plebani, M.; Sakarovitch, C.; Sipponen, P.; Megraud, F. Pepsinogen A, pepsinogen C, and gastrin as markers of atrophic chronic gastritis in European dyspeptics. Br. J. Cancer 2003, 88, 1239–1247. [Google Scholar] [CrossRef]
- Vaananen, H.; Vauhkonen, M.; Helske, T.; Kääriäinen, I.; Rasmussen, M.; Tunturi-Hihnala, H.; Koskenpato, J.; Sotka, M.; Turunen, M.; Sandström, R.; et al. Non-endoscopic diagnosis of atrophic gastritis with a blood test. Correlation between gastric histology and serum levels of gastrin-17 and pepsinogen I: A multicentre study. Eur. J. Gastroenterol. Hepatol. 2003, 15, 885–891. [Google Scholar] [CrossRef]
- Dinis-Ribeiro, M.; Yamaki, G.; Miki, K.; Costa-Pereira, A.; Matsukawa, M.; Kurihara, M. Meta-analysis on the validity of pepsinogen test for gastric carcinoma, dysplasia or chronic atrophic gastritis screening. J. Med. Screen 2004, 11, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Telaranta-Keerie, A.; Kara, R.; Paloheimo, L.; Härkönen, M.; Sipponen, P. Prevalence of undiagnosed advanced atrophic corpus gastritis in Finland: An observational study among 4,256 volunteers without specific complaints. Scand. J. Gastroenterol. 2010, 45, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Gantuya, B.; Oyuntsetseg, K.; Bolor, D.; Erdene-Ochir, Y.; Sanduijav, R.; Davaadorj, D.; Tserentogtokh, T.; Uchida, T.; Yamaoka, Y. Evaluation of serum markers for gastric cancer and its precursor diseases among high incidence and mortality rate of gastric cancer area. J. Castric. Cancer 2019, 22, 104–112. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age Group | Gender | Total | ||
|---|---|---|---|---|
| Female | Male | |||
| 10–15 | 10–19 | 137 | 102 | 239 |
| 16–19 | 29 | 27 | 56 | |
| 20–29 | 20–39 | 100 | 55 | 155 |
| 30–39 | 54 | 33 | 87 | |
| 40–49 | Over 40 | 38 | 24 | 62 |
| 50–59 | 4 | 2 | 6 | |
| Over 60 | 2 | 3 | 5 | |
| Total | 364 | 246 | 610 | |
| Mean age | 22.9 | |||
| Age Group | Anti-H. pylori IgG Biohit | Anti-H. pylori IgG E-plate | ||||
|---|---|---|---|---|---|---|
| Negative | Positive | Percent | Negative | Positive | Percent | |
| 10–19 | 34 | 261 | 88.47% | 107 | 188 | 63.72% |
| 20–39 | 13 | 229 | 94.63% | 80 | 162 | 66.94% |
| Over 40 | 3 | 70 | 95.89% | 35 | 38 | 52.05% |
| Total | 50 | 560 | 91.8% | 222 | 388 | 63.6% |
| Japanese | Anti-CagA Antibody | Mongolians | Anti-CagA Antibody | ||||
|---|---|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | ||||
| Biohit | Positive | 28 | 1 | Biohit | Positive | 500 | 60 |
| Negative | 0 | 41 | Negative | 6 | 44 | ||
| E-plate | Positive | 27 | 0 | E-plate | Positive | 367 | 21 |
| Negative | 1 | 42 | Negative | 139 | 83 | ||
| H. pylori | Pepsinogen Ratio | Age Group | Total | Total Positive Cases | ||
|---|---|---|---|---|---|---|
| 10–19 | 20–39 | Over 40 | ||||
| Positive | <3 | 8 | 26 | 13 | 47 | 560 |
| <5 | 28 | 91 | 38 | 157 | ||
| Negative | <3 | 0 | 2 | 2 | 4 | |
| <5 | 1 | 4 | 2 | 7 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amgalanbaatar, A.; Shimomura, H.; Sugano, K.; Bira, T.-O.; Okamoto, H.; Hirai, Y. Correlation between Helicobacter pylori Infection and Gastric Atrophy Examined in the Sera of Mongolian People. Gastrointest. Disord. 2019, 1, 241-252. https://doi.org/10.3390/gidisord1020019
Amgalanbaatar A, Shimomura H, Sugano K, Bira T-O, Okamoto H, Hirai Y. Correlation between Helicobacter pylori Infection and Gastric Atrophy Examined in the Sera of Mongolian People. Gastrointestinal Disorders. 2019; 1(2):241-252. https://doi.org/10.3390/gidisord1020019
Chicago/Turabian StyleAmgalanbaatar, Avarzed, Hirofumi Shimomura, Kentaro Sugano, Tsatsralt-Od Bira, Hiroaki Okamoto, and Yoshikazu Hirai. 2019. "Correlation between Helicobacter pylori Infection and Gastric Atrophy Examined in the Sera of Mongolian People" Gastrointestinal Disorders 1, no. 2: 241-252. https://doi.org/10.3390/gidisord1020019
APA StyleAmgalanbaatar, A., Shimomura, H., Sugano, K., Bira, T.-O., Okamoto, H., & Hirai, Y. (2019). Correlation between Helicobacter pylori Infection and Gastric Atrophy Examined in the Sera of Mongolian People. Gastrointestinal Disorders, 1(2), 241-252. https://doi.org/10.3390/gidisord1020019