Abstract
Spontaneous pneumothorax in the setting of coronavirus disease 19 (COVID-19) has been first described as an unlikely complication, mainly occurring in critically ill patients or as a consequence of mechanical ventilation. We report a case with COVID-19 pneumonia followed by a spontaneous pneumothorax in a young non-smoker without any predisposing pathology.
1. Introduction
The first cases of Coronavirus disease 2019 (COVID-19) were described in Wuhan, China, and quickly spread around the world to become a threat to public health, the economy, and other areas [1]. According to JHU CSSE COVID-19 data, since the outbreak of COVID-19, more than 136 million cases have been confirmed, with nearly 3 million fatal outcomes. The WHO declared the disease as a pandemic.
It seems that COVID-19 does not spare a system: Even though the disease mainly affects the respiratory tract, manifesting as viral pneumonia with common symptoms of dyspnea or respiratory failure. Additionally, the nervous, cardiovascular, gastrointestinal, and/or renal systems can be involved [2,3].
Most of the patients present with a mild course of the disease—the mortality ranges from less than 1% to 8% depending on the country [4,5]. Additionally, new variants have been reported showing differences in infection rate, severity, and mortality [5,6].
Most cases present with a relatively mild symptoms, yet severe complications have been observed, with even fatal outcomes—cytokine release syndrome, responsible for acute respiratory distress syndrome; acute kidney failure; or severe myocardial damage, as well as secondary infections with septic shock [7,8]. According to some literature data, approximately 20% of patients progressed to acute respiratory distress syndrome requiring mechanical ventilation [9,10]. Decreased pulmonary compliance and alveolar inflammation demand higher levels of airway pressure and fraction of inspired oxygen in order to achieve adequate ventilation and gas exchange. Higher levels of airway pressure are among the most probable causes for a number of pulmonary complications, including secondary spontaneous pneumothorax.
Pneumothorax or pneumomediastinum development during the course of COVID-19 disease was first described as a rather unlikely complication (1% of cases), usually affecting critically ill patients or those with mechanical ventilation [11,12,13,14]. However, recent data suggest that pneumothorax could also occur in patients without ventilation support [15,16,17].
We report on a case with COVID-19 pneumonia followed by a spontaneous pneumothorax in a young non-smoker, no alcohol abuse, and HIV-negative, without any predisposing pathology.
2. Case Report
A 35-year-old male patient presented with suspected COVID-19 pneumonia. He complained about fever (up to 38.5 °C), headache, cough, shortness of breath, and chest tightness for the last 2 days. No comorbidities were known, except for ulcerative colitis in remission. The patient denied smoking, as well as alcohol abuse; there were no data about other drug abuses(e.g., steroids, 5-ASA, etc.). No family history of respiratory tract diseases was available or other specific lung anomalies.
His vitals on admission were as follows: heart rate of 98/min, respiratory rate of 24/min, and peripheral oxygen saturation of 90%.
The laboratory results (Table 1) showed an elevation of the c-reactive protein (CRP: 106 mg/L; normal range: <5 mg/L) with a normal procalcitonin level (PCT: 0.08 ng/mL; normal range: <0.5 ng/mL). Creatinine was normal (Crea: 0.8 mg/dL; normal range 0.7–1.2 mg/dL), while lactate dehydrogenase was elevated (LDH: 367 U/L; normal range: <250 U/L). D-dimer was also elevated (d-dimer: 310 ng/mL; normal range: <250 ng/mL).

Table 1.
Laboratory findings on admission.
Chest X-ray showed bilateral interstitial infiltrates (Figure 1). Positive reverse transcriptase polymerase chain reaction (RT-PCR) test with nasal swab (Genexpect system) confirmed COVID-19 infection. The patient was admitted to the isolation ward and received supportive treatment. Oxygen supplementation was also necessary—poly mask was applied (his pO2 increased to 98%), with no mechanical ventilation. The patient was discharged in a stable condition at day +5 after admission. A chest CT was performed, revealing no bulla present at the time of discharge.
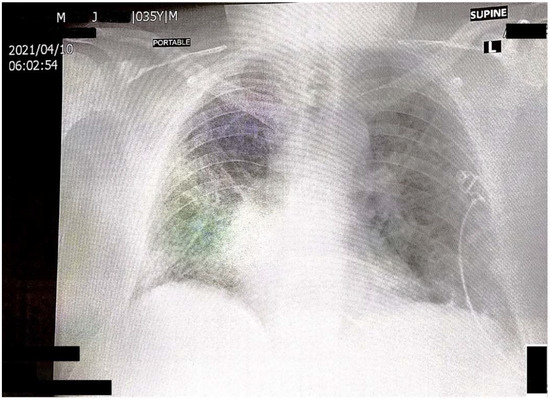
Figure 1.
Chest X-ray on admission—showing bilateral interstitial infiltrates without blebs.
Twenty days after discharge, the patient presented again in the emergency department with severe chest pain and shortness of breath. CT chest revealed a significant pneumothorax on the right side (Figure 2). A chest tube was inserted with subsequent drainage, leading to a re-expansion of the right lung.
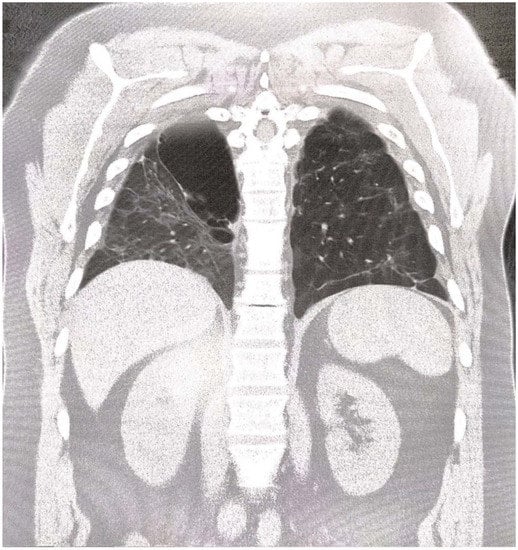
Figure 2.
CT chest—showing pneumothorax on the right side.
The patient was followed-up once again a month later. He could walk a kilometer distance without getting breathless. Clinically, there was a normal expansion of the both lungs with normal percussion margins. There was no need for new X-rays as the patient was clinically stable, asymptomatic, and was feeling fine.
3. Discussion
Approximately 1% of patients with COVID-19 pneumonia develop pneumothorax, presumably due to the barotrauma caused by positive pressure ventilation [12,18].
In the case presented, no such trauma could be suspected. Other possible “culprits” (emphysema, cystic fibrosis, necrotizing pneumonia, severe asthma, lung inflammation/malignancy, as well as Marfan syndrome and alpha 1-antitrypsin deficiency) also cannot be taken in consideration [19,20]. The patient is a non-smoker and in good physical condition (could walk for 5 km prior to the COVID-19 infection); he was tested for alpha 1-antitripsin deficiency (negative). The control CT scan before the discharge did not show any bulla or emphysema. The patient denies having significant cough—thus, the so-called Maclin effect (occurs due to extensive cough in an area that the alveolar walls are weakened) should also be excluded.
There are a few possibilities to explain the complication described:
- Small (micro) sub pleural bleb formation in the course of the disease that broke later into the pleural space [20];
- Given the hypercoagulable state observed in COVID-19 patients, a microembolus leading to infection with subsequent alveolar wall damage and leakage in the pleural compartment could be suspected [21,22];
- Diffuse alveolar damage leading to alveolar rupture and air leak [17].
4. Conclusions
It is obvious that there is only a thin burden between the mild course of the disease and full-blown respiratory failure (with life-threatening consequences), as well as between the “really recovered” patient after the discharge and the patient with unsuspected risk for ulterior complications.
Increasing evidence of spontaneous pneumothorax in non-ventilated patients after COVID-19 should make clinicians aware of the “rare” possibility for a spontaneous pneumothorax to cause acute worsening dyspnea or acute clinical deterioration in patients with a recent COVID-19 history.
Author Contributions
Conceptualization, V.G. and H.N.; methodology, M.G., E.G. and H.N.; software, M.G. and E.G.; validation, M.G. and E.G.; formal analysis, M.G., E.G. and H.N.; investigation, V.G. and M.G.; resources, V.G., M.G., E.G. and H.N.; data curation, E.G.; writing—original draft preparation, M.G., E.G. and H.N.; writing—review and editing, V.G.; visualization, M.G., E.G. and H.N.; supervision, V.G. and H.N.; project administration, E.G.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. Novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult in patients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, J.C.; Félix, V.B.; Leão, S.A.B.F.; Trindade-Filho, E.M.; Scorza, F.A. New Brazilian variant of the SARS-CoV-2 (P1/Gamma) of COVID-19 in Alagoas state. Braz. J. Infect. Dis. 2021, 25, 101588. [Google Scholar] [CrossRef]
- Da Silva, S.J.R.; Pena, L. Collapse of the public health system and the emergence of new variants during the second wave of the COVID-19 pandemic in Brazil. One Health 2021, 13, 100287. [Google Scholar] [CrossRef]
- Young, B.E.; Ong, S.W.X.; Kalimuddin, S.; Low, J.G.; Tan, S.Y.; Loh, J.; Ng, O.T.; Marimuthu, K.; Ang, L.W.; Mak, T.M.; et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. JAMA 2020, 323, 1488–1494. [Google Scholar] [CrossRef] [Green Version]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host-Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Ziehr, D.; Alladina, J.; Petri, C.A.; Maley, J.H.; Moskowitz, A.; Medoff, B.D.; Hibbert, K.A.; Thompson, B.T.; Hardin, C.C. Pathophysiology of mechanically ventilated patients with COVID 19 a Cohort study. Am. J. Respir. Crit. Care Med. 2020, 201, 1560–1564. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Quincho-Lopez, A.; Quincho-Lopez, D.L.; Hurtado-Medina, F.D. Case Report: Pneumothorax and Pneumomediastinum as Uncommon Complications of COVID-19 Pneumonia-Literature Review. Am. J. Trop. Med. Hyg. 2020, 103, 1170–1176. [Google Scholar] [CrossRef]
- Martinelli, A.W.; Ingle, T.; Newman, J.; Nadeem, I.; Jackson, K.; Lane, N.D.; Melhorn, J.; Davies, H.E.; Rostron, A.J.; Adeni, A.; et al. COVID-19 and pneumothorax: A multicentre retrospective case series. Eur. Respir. J. 2020, 56, 2002697. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Belletti, A.; Palumbo, D.; Zangrillo, A.; Fominskiy, E.V.; Franchini, S.; Dell’Acqua, A.; Marinosci, A.; Monti, G.; Vitali, G.; Colombo, S.; et al. Predictors of Pneumothorax/Pneumomediastinum in Mechanically Ventilated COVID-19 Patients. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3642–3651. [Google Scholar] [CrossRef] [PubMed]
- Schiller, M.; Wunsch, A.; Fisahn, J.; Gschwendtner, A.; Huebner, U.; Kick, W. Pneumothorax with bullous lesions as a late complication of COVID-19 pneumonia—A report on two clinical cases. J. Emerg. Med. 2021, 61, 581–586. [Google Scholar] [CrossRef]
- Sun, R.; Liu, H.; Sang, X. Mediastinal emphysema, giant bulla and pneumothorax developed during the course of COVID-19 pneumonia. Korean J. Radiol. 2020, 21, 541–544. [Google Scholar] [CrossRef] [Green Version]
- Tucker, L.; Patel, S.; Vatsis, C.; Poma, A.; Ammar, A.; Nasser, W.; Mukkera, S.; Vo, M.; Khan, R.; Carlan, S. Pneumothorax and Pneumomediastinum Secondary to COVID-19 Disease Unrelated to Mechanical Ventilation. Case Rep. Crit. Care 2020, 2020, 6655428. [Google Scholar] [CrossRef] [PubMed]
- Elhakim, T.S.; Abdul, H.S.; Pelaez Romero, C.; Rodriguez-Fuentes, Y. Spontaneous pneumomediastinum, pneumothorax and subcutaneous emphysema in COVID-19 pneumonia: A rare case and literature review. BMJ Case Rep. 2020, 13, e239489. [Google Scholar] [CrossRef]
- Noppen, M. Spontaneos pneumothorax. Epiemiology, pathophysiology and cause. Eur. Respir. Rev. 2010, 19, 217–219. [Google Scholar] [CrossRef] [Green Version]
- Schramel, F.; Meyer, C.J.; Postmus, P.E. Inflammation as a cause of spontaneous pneumothorax and empyema like changes. Results of bronchoalveolar lavage. Eur. Respir. Rev. 1995, 8, 397s. [Google Scholar]
- Connors, J.M.; Levy, J.H. Covid 19 and its implication for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier-Decrucq, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary Embolism in Patients with COVID-19: Awareness of an Increased Prevalence. Circulation 2020, 142, 184–186. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).