Embolization of Bio-Alcamid Gluteal Injections in a Female Patient with Patent Foramen Ovale Leading to ARDS and Embolic Stroke



{kind=link}
{kind=link}
Abstract
1. Introduction
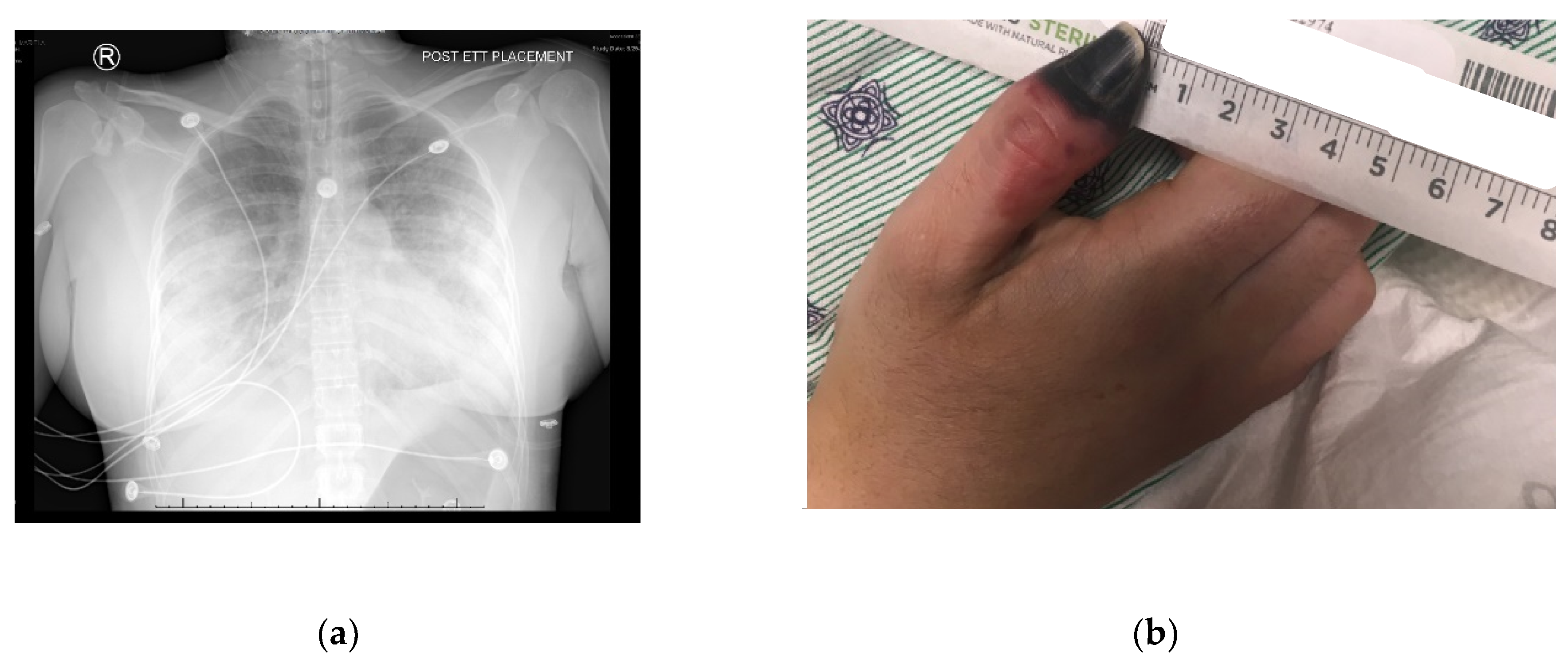
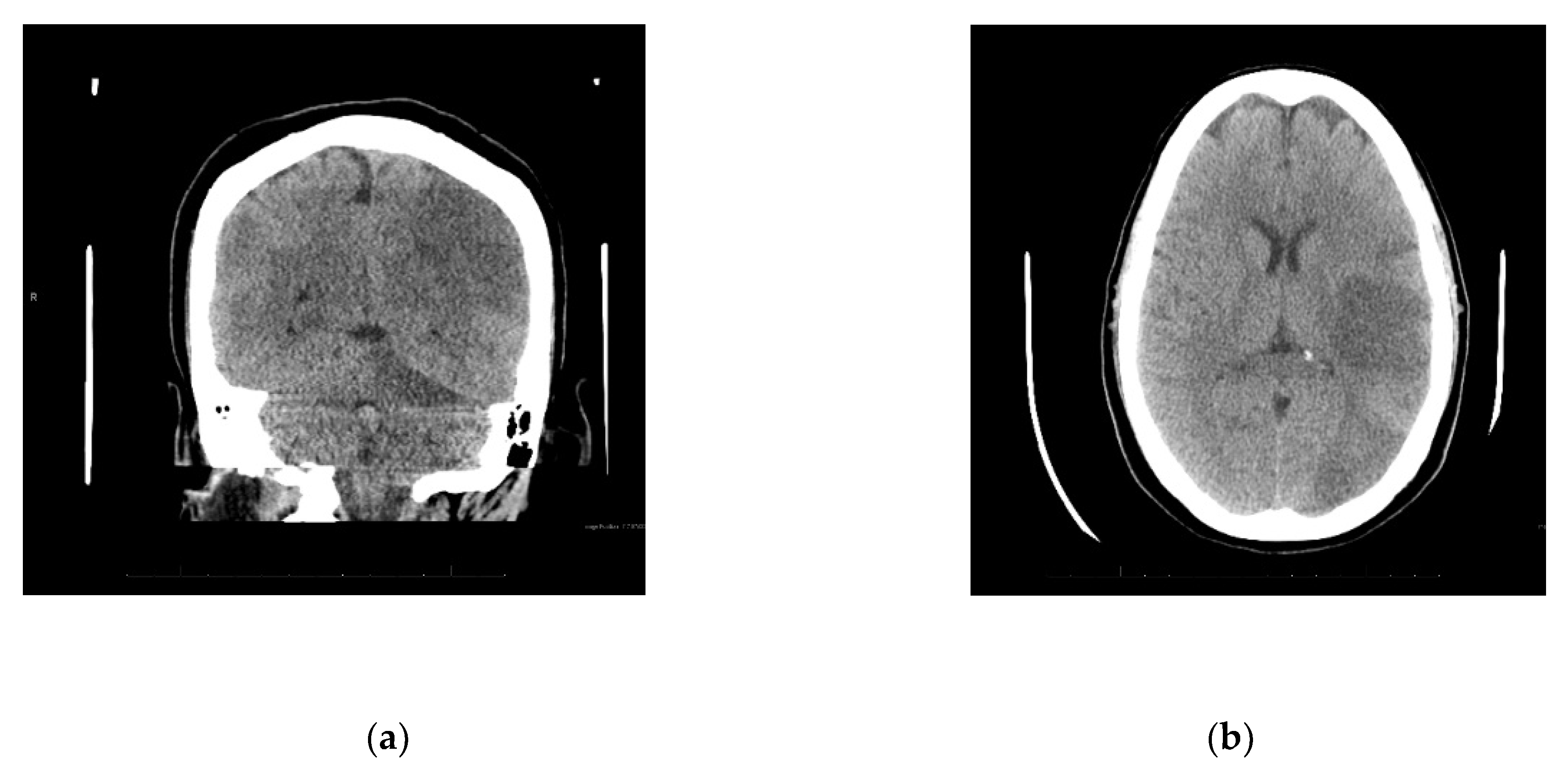
2. Case Presentation Section
3. Discussion
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Serra, M.S.; Gonçalves, L.Z. Permanent Fillers. In Botulinum Toxins, Fillers and Related Substances, 1st ed.; Issa, M.C.A., Tamura, B., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–8. [Google Scholar]
- US Food and Drug Administration. Available online: www.fda.gov/MedicalDevices/ucm2007470.htm#hcp (accessed on 29 August 2018).
- Akrish, S.; Dayan, D.; Taicher, S.; Adam, I.; Nagler, R.M. Foreign body granulomas after injection of Bio-alcamid for lip augmentation. Am. J. Otolaryngol. 2009, 30, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Campana, M.; Lazzeri, D.; Rosato, L.; Perello, R.; Vaccaro, M.; Ciappi, S.; Campa, A.; Brafa, A.; Nisi, G.; Brandi, C.; et al. Late-onset gluteal Escherichia coli abscess formation 7 years after soft tissue augmentation with Bio-Alcamid in a HIV-positive patient. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 709–7110. [Google Scholar] [CrossRef] [PubMed]
- Hönig, J. Cheek augmentation with Bio-Alcamid in facial lipoatrophy in HIV seropositive patients. J. Craniofac. Surg. 2008, 19, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- DeLorenzi, C. Complications of injectable fillers, part 2: Vascular complications. Aesthet. Surg. J. 2014, 34, 584–600. [Google Scholar] [CrossRef] [PubMed]
- Rostom, M.; Brendling, L.; Stewart, K. Bio-Alcamid complications: A 10 year review. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 848–862. [Google Scholar] [CrossRef] [PubMed]
- Schelke, L.W.; van den Elzen, H.J.; Canninga, M.; Neumann, M.H. Complications after treatment with polyalkylimide. Dermatol. Surg. 2009, 35, 1625–1628. [Google Scholar] [CrossRef] [PubMed]
- García-Pacheco, S.A.; Blanco-Rivas, R.; Campos-García, S. Polyalkylimide filler in human immunodeficiency virus-associated facial lipodystrophy: Ophthalmic complications. Arch. Soc. Esp. Oftalmol. 2014, 89, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Schütz, P.; Ibrahim, H.H.; Hussain, S.S.; Ali, T.S.; El-Bassuoni, K.; Thomas, J. Infected facial tissue fillers: Case series and review of the literature. J. Oral Maxillofac. Surg. 2012, 70, 2403–2412. [Google Scholar] [CrossRef] [PubMed]
- Goldan, O.; Georgiou, I.; Grabov-Nardini, G.; Regev, E.; Tessone, A.; Liran, A.; Haik, J.; Mendes, D.; Orenstein, A.; Winkler, E. Early and late complications after a nonabsorbable hydrogel polymer injection: A series of 14 patients and novel management. Dermatol. Surg. 2007, 33, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.D.; Brites, C.; Sprinz, E. HIV-associated lipodystrophy: A review from a Brazilian perspective. Ther. Clin. Risk Manag. 2014, 10, 559–566. [Google Scholar]
- Serrano, C.; Serrano, S. Delayed infection after Bio-alcamid implantation. Actas Dermosifiliogr. 2006, 97, 460–462. [Google Scholar] [CrossRef]
- Gómez-de la Fuente, E.; Alvarez-Fernández, J.G.; Pinedo, F.; Naz, E.; Gamo, R.; Vicente-Martín, F.J.; López-Estebaranz, J.L. Cutaneous adverse reaction to Bio-Alcamid implant. Actas Dermosifiliogr. 2007, 98, 271–275. [Google Scholar] [CrossRef]
- Chrastil-LaTowsky, B.; Wesley, N.O.; MacGregor, J.L.; Kaminer, M.S.; Arndt, K.A. Delayed Inflammatory Reaction to Bio-Alcamid Polyacrylamide Gel Used for Soft-Tissue Augmentation. Arch. Dermatol. 2009, 145, 1309–1312. [Google Scholar] [CrossRef] [PubMed]
- Karim, R.B.; Hage, J.J.; van Rozelaar, L.; Lange, C.A.; Raaijmakers, J. Complications of polyalkylimide 4% injections (Bio-Alcamid): A report of 18 cases. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 1409–1414. [Google Scholar] [CrossRef] [PubMed]
- Nadarajah, J.T.; Collins, M.; Raboud, J.; Su, D.; Rao, K.; Loutfy, M.R.; Walmsley, S. Infectious complications of Bio-Alcamid filler used for HIV-related facial lipoatrophy. Clin. Infect. Dis. 2012, 55, 1568–1574. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, R.J.; Cohen, J.L.; Carruthers, J.D. Successful management of an unusual presentation of impending necrosis following a hyaluronic acid injection embolus and a proposed algorithm for management with hyaluronidase. Dermatol. Surg. 2007, 33, 357–360. [Google Scholar] [PubMed]
- Lim, J.H.; Lee, J.M.; Choi, S.H.; Nam, H.S.; Cho, J.H.; Ryu, J.S.; Kwak, S.M. Alveolar Hemorrhage after Polyacrylamide Injection for Breast Augmentation. Korean J. Med. 2015, 88, 438–441. [Google Scholar] [CrossRef]
- Peter, S.; Mennel, S. Retinal branch artery occlusion following injection of hyaluronic acid (Restylane). Clin. Exp. Ophthalmol. 2006, 34, 363–364. [Google Scholar] [CrossRef] [PubMed]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolduc, J.; Abdalla, B.; Choudhry, M.; Danial, M.; Rizvi, S.A.A. Embolization of Bio-Alcamid Gluteal Injections in a Female Patient with Patent Foramen Ovale Leading to ARDS and Embolic Stroke. Reports 2019, 2, 23. https://doi.org/10.3390/reports2040023
Bolduc J, Abdalla B, Choudhry M, Danial M, Rizvi SAA. Embolization of Bio-Alcamid Gluteal Injections in a Female Patient with Patent Foramen Ovale Leading to ARDS and Embolic Stroke. Reports. 2019; 2(4):23. https://doi.org/10.3390/reports2040023
Chicago/Turabian StyleBolduc, James, Beshoy Abdalla, Mansoor Choudhry, Muhammad Danial, and Syed A. A. Rizvi. 2019. "Embolization of Bio-Alcamid Gluteal Injections in a Female Patient with Patent Foramen Ovale Leading to ARDS and Embolic Stroke" Reports 2, no. 4: 23. https://doi.org/10.3390/reports2040023
APA StyleBolduc, J., Abdalla, B., Choudhry, M., Danial, M., & Rizvi, S. A. A. (2019). Embolization of Bio-Alcamid Gluteal Injections in a Female Patient with Patent Foramen Ovale Leading to ARDS and Embolic Stroke. Reports, 2(4), 23. https://doi.org/10.3390/reports2040023