
Porous Zirconia Blocks for Bone Repair: An Integrative Review on Biological and Mechanical Outcomes

 ,
,  , ,
, , 


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
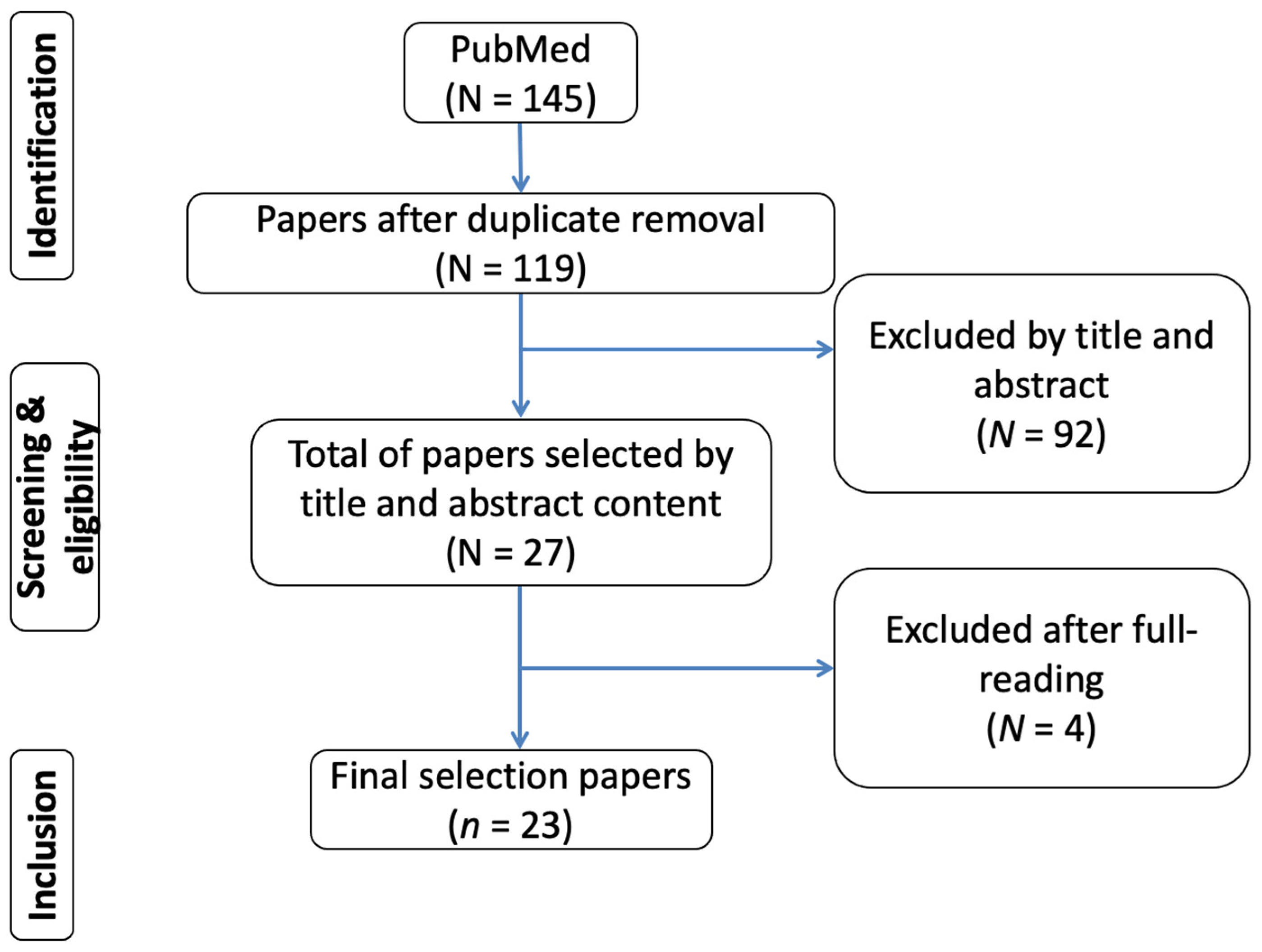
2.1. Information Sources and Search Strategy
2.2. Study Selection and Data Collection Process
3. Results
4. Discussion
4.1. Zirconia
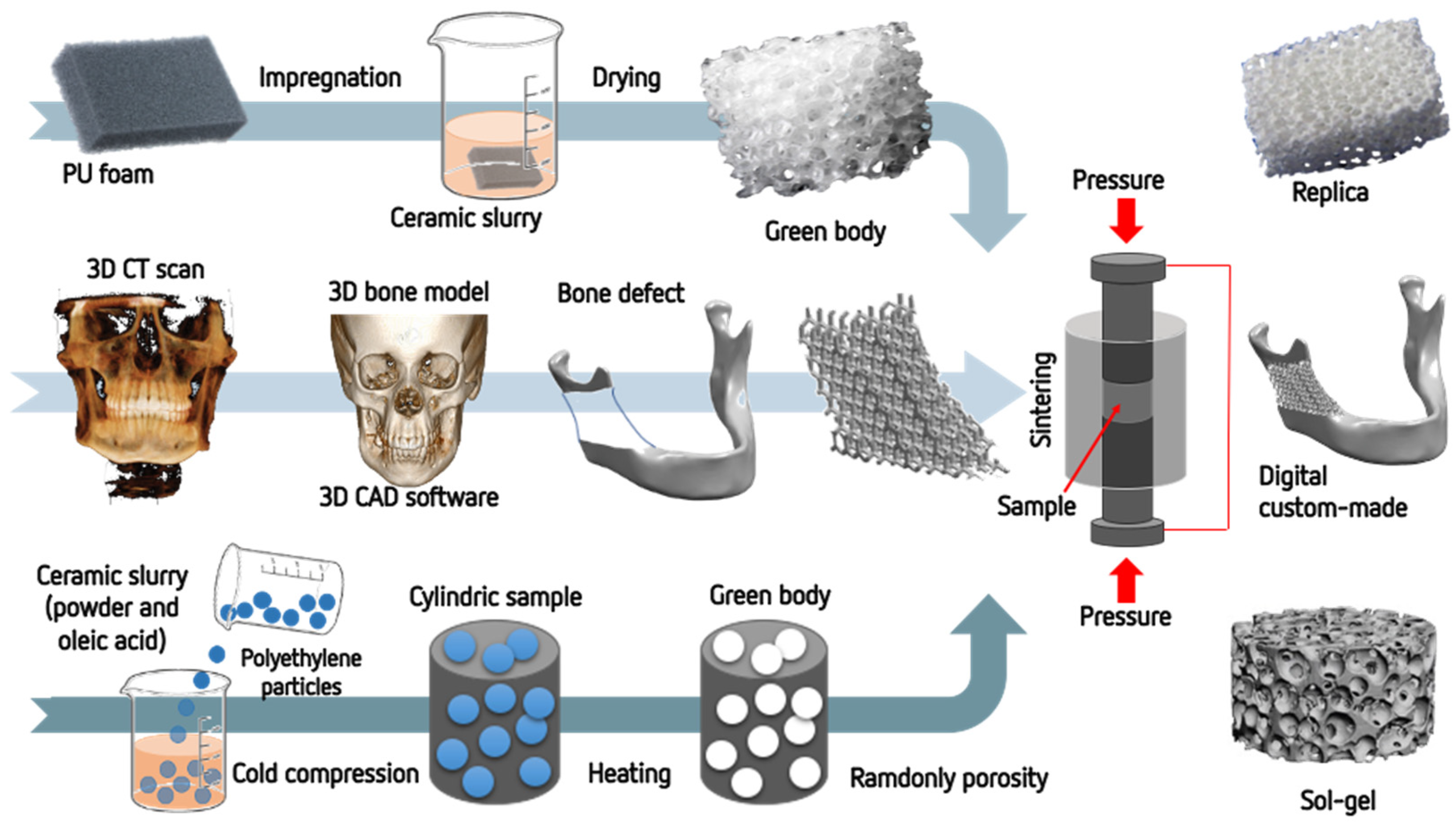
4.2. Manufacturing of Zirconia Porous Structures
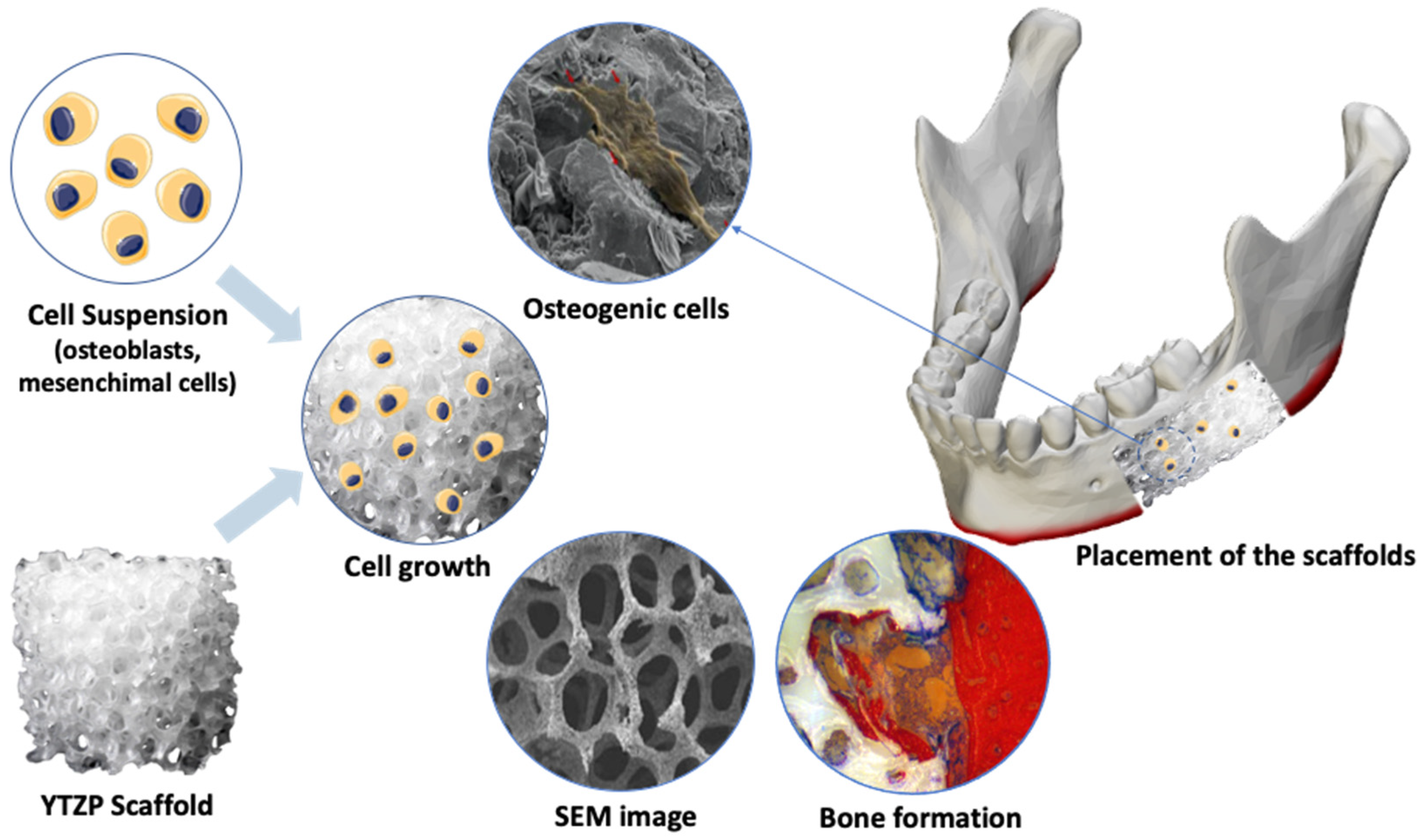
4.3. Biological Effects of Porous Zirconia Structures
5. Conclusions
- Most studies described the manufacturing of zirconia porous structures by using CAD-CAM, replica methods, and powder sintering. Control of the size and percentage of pores can be achieved by designing the models by CAD or polyurethane patterns;
- Considering the mechanical properties of zirconia, a high porosity of approximately 85% and large pores ranging from 100 up to 400 μm can be accomplished without compromising the application of zirconia porous structures in extensive surgical bone sites;
- Macro-scale pores ranging from 100 to 400 μm allow cell ingrowth and angiogenesis into the porous structures, while pores at micro-scale (1–50 μm) provide an increase in the wettability, protein adsorption, and cell adhesion;
- Most in vivo studies reported increased bone growth by contact and distance osteogenesis into the porous zirconia compared to highly dense zirconia. Porous zirconia showed significantly improved new bone formation into the interconnected channels after placement in rabbits for 4 and 12 weeks and after placement in humans for about 3 months;
- Further studies should be carried out to determine the optimum balance between porosity, pores’ size, and the strength of the porous zirconia structures. In addition, hybrid bioactive ceramic containing zirconia and modified surfaces could be explored as the surfaces of porous structures play a key role in the adsorption of proteins and osteogenic cells.
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Malmstrom, J.; Adolfsson, E.; Emanuelsson, L.; Thomsen, P. Bone ingrowth in zirconia and hydroxyapatite scaffolds with identical macroporosity. J. Mater. Sci. Mater. Med. 2008, 19, 2983–2992. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-W.; Shin, S.-Y.; Kim, H.-E.; Lee, Y.-M.; Chung, C.-P.; Lee, H.-H.; Rhyu, I.-C. Bone formation on the apatite-coated zirconia porous scaffolds within a rabbit calvarial defect. J. Biomater. Appl. 2008, 22, 485–504. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, I.S.; Magrin, G.L.; Magini, R.S.; Fredel, M.C.; Benfatti, C.A.M.; Souza, J.C.M. On the synthesis and characterization of β-tricalcium phosphate scaffolds coated with collagen or poly (D, L-lactic acid) for alveolar bone augmentation. Eur. J. Dent. 2017, 11, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Bhowmick, A.; Pramanik, N.; Jana, P.; Mitra, T.; Gnanamani, A.; Das, M.; Kundu, P.P. Development of bone-like zirconium oxide nanoceramic modified chitosan based porous nanocomposites for biomedical application. Int. J. Biol. Macromol. 2017, 95, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Mesquita-Guimarães, J.; Detsch, R.; Souza, A.C.; Henriques, B.; Silva, F.S.; Boccaccini, A.R.; Carvalho, O. Cell adhesion evaluation of laser-sintered HAp and 45S5 bioactive glass coatings on micro-textured zirconia surfaces using MC3T3-E1 osteoblast-like cells. Mater. Sci. Eng. C 2020, 109, 110492. [Google Scholar] [CrossRef]
- Peñarrieta-Juanito, G.; Cruz, M.; Costa, M.; Miranda, G.; Marques, J.; Magini, R.; Mata, A.; Souza, J.C.M.; Caramês, J.; Silva, F.S. A novel gradated zirconia implant material embedding bioactive ceramics: Osteoblast behavior and physicochemical assessment. Materialia 2018, 1, 3–14. [Google Scholar] [CrossRef]
- Gouveia, P.F.; Mesquita-Guimarães, J.; Galárraga-Vinueza, M.E.; Souza, J.C.M.; Silva, F.S.; Fredel, M.C.; Boccaccini, A.R.; Detsch, R.; Henriques, B. In-vitro mechanical and biological evaluation of novel zirconia reinforced bioglass scaffolds for bone repair. J. Mech. Behav. Biomed. Mater. 2021, 114, 104164. [Google Scholar] [CrossRef]
- Grandfield, K.; Palmquist, A.; Ericson, F.; Malmstrom, J.; Emanuelsson, L.; Slotte, C.; Adolfsson, E.; Botton, G.A.; Thomsen, P.; Engqvist, H. Bone response to free-form fabricated hydroxyapatite and zirconia scaffolds: A transmission electron microscopy study in the human maxilla. Clin. Implant Dent. Relat. Res. 2012, 14, 461–469. [Google Scholar] [CrossRef]
- Hadjicharalambous, C.; Buyakov, A.; Buyakova, S.; Kulkov, S.; Chatzinikolaidou, M. Porous alumina, zirconia and alumina/zirconia for bone repair: Fabrication, mechanical and in vitro biological response. Biomed. Mater. 2015, 10, 25012. [Google Scholar] [CrossRef]
- Hadjicharalambous, C.; Mygdali, E.; Prymak, O.; Buyakov, A.; Kulkov, S.; Chatzinikolaidou, M. Proliferation and osteogenic response of MC3T3-E1 pre-osteoblastic cells on porous zirconia ceramics stabilized with magnesia or yttria. J. Biomed. Mater. Res. A 2015, 103, 3612–3624. [Google Scholar] [CrossRef]
- Shao, R.-X.; Quan, R.-F.; Wang, T.; Du, W.-B.; Jia, G.-Y.; Wang, D.; Lv, L.-B.; Xu, C.-Y.; Wei, X.-C.; Wang, J.-F.; et al. Effects of a bone graft substitute consisting of porous gradient HA/ZrO2 and gelatin/chitosan slow-release hydrogel containing BMP-2 and BMSCs on lumbar vertebral defect repair in rhesus monkey. J. Tissue Eng. Regen. Med. 2018, 12, e1813–e1825. [Google Scholar] [CrossRef] [PubMed]
- Aboushelib, M.N.; Shawky, R. Osteogenesis ability of CAD/CAM porous zirconia scaffolds enriched with nano-hydroxyapatite particles. Int. J. Implant Dent. 2017, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- Fabris, D.; Mesquita-Guimarães, J.; Pinto, P.; Souza, J.C.M.; Fredel, M.C.; Silva, F.S.; Henriques, B. Mechanical properties of zirconia periodic open cellular structures. Ceram. Int. 2019, 45, 15799–15806. [Google Scholar] [CrossRef]
- Alizadeh, A.; Moztarzadeh, F.; Ostad, S.N.; Azami, M.; Geramizadeh, B.; Hatam, G.; Bizari, D.; Tavangar, S.M.; Vasei, M.; Ai, J. Synthesis of calcium phosphate-zirconia scaffold and human endometrial adult stem cells for bone tissue engineering. Artif. Cells Nanomed. Biotechnol. 2016, 44, 66–73. [Google Scholar] [CrossRef] [PubMed]
- An, S.-H.; Matsumoto, T.; Miyajima, H.; Nakahira, A.; Kim, K.-H.; Imazato, S. Porous zirconia/hydroxyapatite scaffolds for bone reconstruction. Dent. Mater. 2012, 28, 1221–1231. [Google Scholar] [CrossRef] [PubMed]
- Pessanha-Andrade, M.; Sordi, M.B.; Henriques, B.; Silva, F.S.; Teughels, W.; Souza, J.C.M. Custom-made root-analogue zirconia implants: A scoping review on mechanical and biological benefits. J. Biomed. Mater. Res.-Part B Appl. Biomater. 2018, 106, 2888–2900. [Google Scholar] [CrossRef] [PubMed]
- Henriques, B.; Fabris, D.; Souza, J.C.M.; Silva, F.S.; Mesquita-Guimarães, J.; Zhang, Y.; Fredel, M. Influence of interlayer design on residual thermal stresses in trilayered and graded all-ceramic restorations. Mater. Sci. Eng. C 2016, 71, 1037–1045. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Silva, J.B.; Aladim, A.; Carvalho, O.; Nascimento, R.M.; Silva, F.S.; Martinelli, A.E.; Henriques, B. Effect of Zirconia and Alumina Fillers on the Microstructure and Mechanical Strength of Dental Glass Ionomer Cements. Open Dent. J. 2016, 10, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Dantas, T.A.; Roedel, S.; Flores, P.; Mesquita-Guimarães, J.; Souza, J.C.M.; Fredel, M.C.; Silva, F.S.; Henriques, B. Wear behaviour of tetragonal zirconia polycrystal with a porous surface. Int. J. Refract. Met. Hard Mater. 2018, 75, 85–93. [Google Scholar] [CrossRef]
- Roedel, S.; Mesquita-Guimarães, J.; Souza, J.C.M.; Silva, F.S.; Fredel, M.C.; Henriques, B. Production and characterization of zirconia structures with a porous surface. Mater. Sci. Eng. C 2019, 101, 264–273. [Google Scholar] [CrossRef]
- Cunha, W.; Carvalho, O.; Henriques, B.; Silva, F.S.; Özcan, M.; Souza, J.C.M. Surface modification of zirconia dental implants by laser texturing. Lasers Med. Sci. 2022, 37, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Henriques, B.; Fabris, D.; Souza, J.C.M.; Silva, F.S.; Carvalho, Ó.; Fredel, M.C.; Mesquita-Guimarães, J. Bond strength enhancement of zirconia-porcelain interfaces via Nd:YAG laser surface structuring. J. Mech. Behav. Biomed. Mater. 2018, 81, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-W.; Moussi, J.; Drury, J.L.; Wataha, J.C. Zirconia in biomedical applications. Expert Rev. Med. Devices 2016, 13, 945–963. [Google Scholar] [CrossRef] [PubMed]
- Gremillard, L.; Martin, L.; Zych, L.; Crosnier, E.; Chevalier, J.; Charbouillot, A.; Sainsot, P.; Espinouse, J.; Aurelle, J.-L. Combining ageing and wear to assess the durability of zirconia-based ceramic heads for total hip arthroplasty. Acta Biomater. 2013, 9, 7545–7555. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Kim, J.-S. Tribological and material analyses of retrieved alumina and zirconia ceramic heads correlated with polyethylene wear after total hip replacement. J. Bone Jt. Surg. Br. 2008, 90, 731–737. [Google Scholar] [CrossRef]
- Rodrigues, D.S.; Buciumeanu, M.; Martinelli, A.E.; Nascimento, R.M.; Henriques, B.; Silva, F.S.; Souza, J.C.M. Mechanical Strength and Wear of Dental Glass-Ionomer and Resin Composites Affected by Porosity and Chemical Composition. J. Bio- Tribo-Corros. 2015, 1, 24. [Google Scholar] [CrossRef]
- Fabris, D.; Souza, J.C.M.; Silva, F.S.; Fredel, M.; Mesquita-Guimarães, J.; Zhang, Y.; Henriques, B. Thermal residual stresses in bilayered, trilayered and graded dental ceramics. Ceram. Int. 2017, 43, 3670–3678. [Google Scholar] [CrossRef]
- Denry, I.; Kelly, J.R. Emerging ceramic-based materials for dentistry. J. Dent. Res. 2014, 93, 1235–1242. [Google Scholar] [CrossRef]
- Fabris, D.; Souza, J.C.M.; Silva, F.S.; Fredel, M.; Gasik, M.; Henriques, B. Influence of specimens’ geometry and materials on the thermal stresses in dental restorative materials during thermal cycling. J. Dent. 2018, 69, 41–48. [Google Scholar] [CrossRef]
- Sailer, I.; Makarov, N.A.; Thoma, D.S.; Zwahlen, M.; Pjetursson, B.E. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: Single crowns (SCs). Dent. Mater. 2015, 31, 603–623. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Bentes, A.C.; Reis, K.; Gavinha, S.; Buciumeanu, M.; Henriques, B.; Silva, F.S.; Gomes, J.R. Abrasive and sliding wear of resin composites for dental restorations. Tribol. Int. 2016, 102, 154–160. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhu, R.; Ma, J.; Weng, Z.; Wang, Y.; Shi, X.; Li, Y.; Yan, X.; Dong, Z.; Xu, J.; et al. In vitro cell proliferation evaluation of porous nano-zirconia scaffolds with different porosity for bone tissue engineering. Biomed. Mater. 2015, 10, 55009. [Google Scholar] [CrossRef] [PubMed]
- GARVIE, R.C.; HANNINK, R.H.; PASCOE, R.T. Ceramic steel? Nature 1975, 258, 703–704. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B.R. Novel Zirconia Materials in Dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Schünemann, F.H.; Galárraga-Vinueza, M.E.; Magini, R.; Fredel, M.; Silva, F.; Souza, J.C.M.; Zhang, Y.; Henriques, B. Zirconia surface modifications for implant dentistry. Mater. Sci. Eng. C 2019, 98, 1294–1305. [Google Scholar] [CrossRef] [PubMed]
- Roedel, S.; Souza, J.C.M.; Silva, F.S.; Mesquita-Guimarães, J.; Fredel, M.C.; Henriques, B. Optimized route for the production of zirconia structures with controlled surface porosity for biomedical applications. Ceram. Int. 2018, 44, 12496–12503. [Google Scholar] [CrossRef]
- Fabris, D.; Souza, J.C.M.; Silva, F.S.; Fredel, M.; Mesquita-Guimarães, J.; Zhang, Y.; Henriques, B. The bending stress distribution in bilayered and graded zirconia-based dental ceramics. Ceram. Int. 2016, 42, 11025–11031. [Google Scholar] [CrossRef] [PubMed]
- Galarraga-Vinueza, M.E.; Mesquita-Guimarães, J.; Magini, R.S.; Souza, J.C.M.; Fredel, M.C.; Boccaccini, A.R. Anti-biofilm properties of bioactive glasses embedding organic active compounds. J. Biomed. Mater. Res. Part A 2016, 105, 672–679. [Google Scholar] [CrossRef]
- Galarraga-Vinueza, M.E.M.E.; Mesquita-Guimarães, J.; Magini, R.S.; Souza, J.C.M.J.C.M.; Fredel, M.C.M.C.; Boccaccini, A.R.A.R.; Magini, R.; Souza, J.C.M.J.C.M.; Fredel, M.C.M.C.; Boccaccini, A.R.A.R. Mesoporous bioactive glass embedding propolis and cranberry antibiofilm compounds. J. Biomed. Mater. Res. Part A 2018, 106, 1614–1625. [Google Scholar] [CrossRef]
- Shao, R.-X.; Quan, R.-F.; Huang, X.-L.; Wang, T.; Xie, S.-J.; Gao, H.-H.; Wei, X.-C.; Yang, D.-S. Evaluation of porous gradient hydroxyapatite/zirconia composites for repair of lumbar vertebra defect in dogs. J. Biomater. Appl. 2016, 30, 1312–1321. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-W.; Kim, H.-E.; Salih, V.; Knowles, J.C. Dissolution control and cellular responses of calcium phosphate coatings on zirconia porous scaffold. J. Biomed. Mater. Res. A 2004, 68, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Peñarrieta-Juanito, G.M.; Costa, M.; Cruz, M.; Miranda, G.; Henriques, B.; Marques, J.; Magini, R.; Mata, A.; Caramês, J.; Silva, F.; et al. Bioactivity of novel functionally structured titanium-ceramic composites in contact with human osteoblasts. J. Biomed. Mater. Res. Part A 2018, 106, 1923–1931. [Google Scholar] [CrossRef] [PubMed]
- da Cruz, M.; Marques, J.; Peñarrieta-Juanito, G.; Costa, M.; Souza, J.; Magini, R.; Miranda, G.; Silva, F.; Duarte Sola Pereira da Mata, A.; Mendez Caramês, J. Hard and Soft Tissue Cell Behavior on Polyetheretherketone, Zirconia, and Titanium Implant Materials. Int. J. Oral Maxillofac. Implants 2019, 34, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Bornstein, M.M.; Carrel, J.-P.; Buser, D.; Bernard, J.-P. Maxillary sinus grafting with a synthetic, nanocrystalline hydroxyapatite-silica gel in humans: Histologic and histomorphometric results. Int. J. Periodontics Restor. Dent. 2014, 34, 259–267. [Google Scholar] [CrossRef]
- Jensen, S.S.; Bornstein, M.M.; Dard, M.; Bosshardt, D.D.; Buser, D. Comparative study of biphasic calcium phosphates with different HA/TCP ratios in mandibular bone defects. A long-term histomorphometric study in minipigs. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 90, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontology 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Sordi, M.B.; Kanazawa, M.; Ravindran, S.; Henriques, B.; Silva, F.S.; Aparicio, C.; Cooper, L.F. Nano-scale modification of titanium implant surfaces to enhance osseointegration. Acta Biomater. 2019, 94, 112–131. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Rocha, L.; Ribeiro-Gonçalves, L.; Henriques, B.; Özcan, M.; Tiritan, M.E.; Souza, J.C.M. An integrative review on the toxicity of Bisphenol A (BPA) released from resin composites used in dentistry. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 1942–1952. [Google Scholar] [CrossRef] [PubMed]
- Tafur-Zelada, C.M.; Carvalho, O.; Silva, F.S.; Henriques, B.; Özcan, M.; Souza, J.C.M. The influence of zirconia veneer thickness on the degree of conversion of resin-matrix cements: An integrative review. Clin. Oral Investig. 2021, 25, 3395–3408. [Google Scholar] [CrossRef] [PubMed]
- Messous, R.; Henriques, B.; Bousbaa, H.; Silva, F.S.; Teughels, W.; Souza, J.C.M. Cytotoxic effects of submicron- and nano-scale titanium debris released from dental implants: An integrative review. Clin. Oral Investig. 2021, 25, 1627–1640. [Google Scholar] [CrossRef] [PubMed]
- Faria, M.; Guedes, A.; Rompante, P.; Carvalho, O.; Silva, F.; Henriques, B.; Özcan, M.; Souza, J.C.M. Wear Pathways of Tooth Occlusal Fissure Sealants: An Integrative Review. Biotribology 2021, 27, 100190. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Fernandes, V.; Correia, A.; Miller, P.; Carvalho, O.; Silva, F.; Özcan, M.; Henriques, B. Surface modification of glass fiber-reinforced composite posts to enhance their bond strength to resin-matrix cements: An integrative review. Clin. Oral Investig. 2022, 26, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.C.M.; Pinho, S.S.; Braz, M.P.; Silva, F.S.; Henriques, B. Carbon fiber-reinforced PEEK in implant dentistry: A scoping review on the finite element method. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1355–1367. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, I.C.; Faria, M.; Torres, O.; Rompante, P.; Henriques, B.; Silva, F.; Özcan, M.; Souza, J.C.M. Damage of Dental Amalgam and Resin-Matrix Composite Surfaces After Exposure to Bleaching Agents: An Integrative Review. J. Bio- Tribo-Corros. 2021, 7, 118. [Google Scholar] [CrossRef]
- Sanon, C.; Chevalier, J.; Douillard, T.; Kohal, R.J.; Coelho, P.G.; Hjerppe, J.; Silva, N.R.F.A. Low temperature degradation and reliability of one-piece ceramic oral implants with a porous surface. Dent. Mater. 2013, 29, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.-G.; Cho, I.-H. Characteristics and osteogenic effect of zirconia porous scaffold coated with beta-TCP/HA. J. Adv. Prosthodont. 2014, 6, 285–294. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Malmstrom, J.; Slotte, C.; Adolfsson, E.; Norderyd, O.; Thomsen, P. Bone response to free form-fabricated hydroxyapatite and zirconia scaffolds: A histological study in the human maxilla. Clin. Oral Implants Res. 2009, 20, 379–385. [Google Scholar] [CrossRef]
- Teimouri, A.; Ebrahimi, R.; Emadi, R.; Beni, B.H.; Chermahini, A.N. Nano-composite of silk fibroin-chitosan/Nano ZrO2 for tissue engineering applications: Fabrication and morphology. Int. J. Biol. Macromol. 2015, 76, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Mesquita-Guimarães, J.; Detsch, R.; Ramos, L.; Grünewald, A.; Henriques, B.; Fredel, M.C.; Silva, F.S.; Boccaccini, A.R. Evaluation of in vitro properties of 3D micro-macro porous bioactive hybrid scaffolds for bone grafting by human osteoblast-like cell growth. J. Eur. Ceram. Soc. 2019, 39, 2545–2558. [Google Scholar] [CrossRef]
- Madeira, S.; Mesquita-Guimarães, J.; Ribeiro, P.; Fredel, M.; Souza, J.C.M.; Soares, D.; Silva, F.S.; Henriques, B. Y-TZP/porcelain graded dental restorations design for improved damping behavior—A study on damping capacity and dynamic Young’s modulus. J. Mech. Behav. Biomed. Mater. 2019, 96, 219–226. [Google Scholar] [CrossRef]
- Fabris, D.; Moura, J.P.A.; Fredel, M.C.; Souza, J.C.M.; Silva, F.S.; Henriques, B. Biomechanical analyses of one-piece dental implants composed of titanium, zirconia, PEEK, CFR-PEEK, or GFR-PEEK: Stresses, strains, and bone remodeling prediction by the finite element method. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Askari, E.; Cengiz, I.F.; Alves, J.L.; Henriques, B.; Flores, P.; Fredel, M.C.; Reis, R.L.; Oliveira, J.M.; Silva, F.S.; Mesquita-Guimarães, J. Micro-CT based finite element modelling and experimental characterization of the compressive mechanical properties of 3-D zirconia scaffolds for bone tissue engineering. J. Mech. Behav. Biomed. Mater. 2020, 102, 103516. [Google Scholar] [CrossRef] [PubMed]
- Balagangadharan, K.; Viji Chandran, S.; Arumugam, B.; Saravanan, S.; Devanand Venkatasubbu, G.; Selvamurugan, N. Chitosan/nano-hydroxyapatite/nano-zirconium dioxide scaffolds with miR-590-5p for bone regeneration. Int. J. Biol. Macromol. 2018, 111, 953–958. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Resende-Gonçalves, C.I.; Sampaio, N.; Moreira, J.; Carvalho, O.; Caramês, J.; Manzanares-Céspedes, M.C.; Silva, F.; Henriques, B.; Souza, J. Porous Zirconia Blocks for Bone Repair: An Integrative Review on Biological and Mechanical Outcomes. Ceramics 2022, 5, 161-172. https://doi.org/10.3390/ceramics5010014
Resende-Gonçalves CI, Sampaio N, Moreira J, Carvalho O, Caramês J, Manzanares-Céspedes MC, Silva F, Henriques B, Souza J. Porous Zirconia Blocks for Bone Repair: An Integrative Review on Biological and Mechanical Outcomes. Ceramics. 2022; 5(1):161-172. https://doi.org/10.3390/ceramics5010014
Chicago/Turabian StyleResende-Gonçalves, Cláudia Inês, Nuno Sampaio, Joaquim Moreira, Oscar Carvalho, João Caramês, Maria Cristina Manzanares-Céspedes, Filipe Silva, Bruno Henriques, and Júlio Souza. 2022. "Porous Zirconia Blocks for Bone Repair: An Integrative Review on Biological and Mechanical Outcomes" Ceramics 5, no. 1: 161-172. https://doi.org/10.3390/ceramics5010014
APA StyleResende-Gonçalves, C. I., Sampaio, N., Moreira, J., Carvalho, O., Caramês, J., Manzanares-Céspedes, M. C., Silva, F., Henriques, B., & Souza, J. (2022). Porous Zirconia Blocks for Bone Repair: An Integrative Review on Biological and Mechanical Outcomes. Ceramics, 5(1), 161-172. https://doi.org/10.3390/ceramics5010014