Case Report
Intravesical Bacillus Calmette-Guerin (BCG) remains the gold standard adjuvant therapy for intermediate and high-risk non-muscle invasive bladder cancer (NMIBC). While effective, BCG can cause complications, from mild local effects to rare systemic events, including mycotic aneurysms [1].
A 55-year-old man with high- and low-grade NMIBC received induction and maintenance BCG, which was ceased after two months due to thrombocytopenia and cystitis. He was transitioned to intravesical chemotherapy with no recurrence ofbladder cancer. He later presented with six months of nonspecific but concerning symptoms, including fatigue, anorexia, 14 kg weight loss, lower abdominal pain, and night sweats. Despite minimal urinary symptoms or recurrence on surveillance cystoscopy, these systemic signs prompted further investigation.
Computed tomography (CT) initially identified a non-specific lesion, which, upon review with fluorodeoxyglucose positron emission tomography (FDG-PET), was found to be a pre-aortic soft tissue mass with peripheral hypermetabolism and central hypometabolism, consistent with an inflammatory or infectious process (Figure 1). Arterial phase CT confirmed a 9 mm saccular false aneurysm from the anterior wall of the infrarenal aorta (Figure 2), with additional foci in the bilateral iliac arteries, consistent with mycotic aneurysms. Urine cultures later confirmed Mycobacterium bovis infection. The patient underwent successful endovascular stenting and anti-mycobacterial therapy, with excellent clinical improvement.
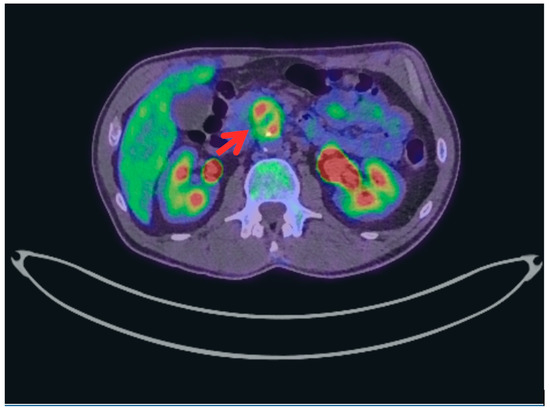
Figure 1.
Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) Scan axial slice demonstrating a lesion within the infrarenal abdominal aorta with central fluorodeoxyglucose (FDG) avidity and peripheral hypometabolism, suggestive of a mycotic aneurysm.
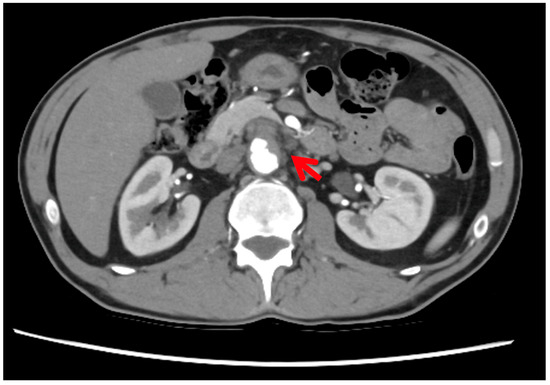
Figure 2.
Arterial phase axial computed tomography (CT) image showing a saccular false aneurysm from the anterior wall of the infrarenal aorta. A 12 mm non-thrombosed component is surrounded by a 24 × 22 mm thrombosed sac with peripheral enhancement and no calcification, consistent with a partially thrombosed mycotic aneurysm.
This case underscores the importance of investigating persistent systemic symptoms, even in the absence of urological findings, and illustrates a rare complication of BCG: vascular dissemination forming mycotic aneurysms. While serious, this should not deter the use of intravesical BCG, a highly effective therapy [2,3]. Clinicians should remain vigilant but reassure patients that such complications are exceedingly uncommon [3]. For those unable to continue BCG, alternative intravesical agents (e.g., gemcitabine/docetaxel [4]) are available.
Author Contributions
Writing—original draft preparation, S.B.; writing—review and editing, S.B., K.Y.Z., B.I. and A.J.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This work is exempt from formal ethics committee review on the basis that it constitutes (a) negligible risk research and (b) use of existing clinical information that is fully de-identified. The manuscript is classified as ‘negligible/minimal risk’ as there is no foreseeable risk of harm or discomfort, and any potential risk is limited to minor inconvenience.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy and ethical reasons.
Acknowledgments
During the preparation of this manuscript, the authors used Grammarly AI/Word Copilot (version 19.2509.34011.0) for the purposes of assistance with reviewing spelling and grammar. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviation is used in this manuscript:
| BCG | Intravesical Bacillus Calmette-Guerin |
| NMIBC | Non-muscle invasive bladder cancer |
| CT | Computed tomography |
| FDG-PET | Fluorodeoxyglucose positron emission tomography |
| FDG | Fluorodeoxyglucose |
References
- European Association of Urology. EAU Guidelines on Non-Muscle-Invasive Bladder Cancer (TaT1 and CIS); EAU Guidelines Office: Arnhem, The Netherlands, 2025; p. 8. Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Non-muscle-invasive-Bladder-Cancer-2025.pdf (accessed on 23 June 2025).
- Witjens, A.C.; Witjes, J.A. Clinical case discussion: Mycotic aortic aneurysm and psoas abscess as a complication of Bacillus Calmette-Guérin instillations. Eur. Urol. Focus 2016, 2, 353–354. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Selph, S.; Buckley, D.I.; Fu, R.; Griffin, J.C.; Grusing, S.; Gore, J.L. Intravesical therapy for the treatment of nonmuscle invasive bladder cancer: A systematic review and meta-analysis. J. Urol. 2017, 197, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Arulraj, K.; Ghorai, R.P.; Nayak, B. Alternative therapy to intravesical Bacillus Calmette–Guérin in nonmuscle invasive bladder cancer. UroCancer Clin. India 2024, 2, 79–84. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Société Internationale d’Urologie. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).