Abstract
Background/Objectives: To understand the clinical characteristics, risk factors, diagnosis, treatment, and outcomes of xanthogranulomatous prostatitis. Methods: A comprehensive search was conducted across PubMed, Embase, and Medline following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, including case reports and case series. Study quality and risk of bias were assessed using the Oxford Centre for Evidence-Based Medicine (CEBM) document. The systematic review process aimed to gather and synthesize all available research evidence on the topic. Results: We included 24 articles reporting on 33 patients, with a median age of 64 years. The most common presenting symptoms were lower urinary tract symptoms (81.8%), and only one patient was asymptomatic. The mean prostate-specific antigen (PSA) level upon presentation was 6.5 ng/mL. Notably, 51.5% of patients were suspected of harbouring clinically significant prostate carcinoma, and only one patient had concurrent prostate adenocarcinoma. All diagnoses were based on changes associated with xanthogranulomatous prostatitis demonstrated upon histopathological examination. A variety of pathogens were isolated, including Escherichia coli, Pseudomonas aeruginosa, Proteus species, and Enterobacter species. Transurethral resection of the prostate (60.6%) was the mainstay approach to management. In total, 27.3% of patients were successfully managed with non-surgical therapy. Conclusions: The majority of patients were suspected of prostate carcinoma prior to the histopathological diagnosis of xanthogranulomatous prostatitis. One patient underwent unnecessary radical prostatectomy as a result. The management of xanthogranulomatous prostatitis includes transurethral resection of the prostate and conservative management with the use of antibiotics. This outlines the importance of following well-established protocols upon suspicion of prostate carcinoma in order to avoid unnecessary radical prostatectomy.
1. Introduction
Xanthogranulomatous prostatitis (XGP) is an uncommon chronic inflammatory condition of the prostate, characterized by the accumulation of lipid-laden macrophages, plasma cells, and lymphocytes, which form granulomatous lesions within the prostate tissue [1]. XGP represents a rare histological entity, with only isolated case reports and small case series reported in the literature, and its exact prevalence is still largely unknown. The clinical presentation of XGP often mimics that of other prostatic diseases, including benign prostatic hyperplasia (BPH) and, more importantly, prostate carcinoma, leading to diagnostic uncertainty and potential overtreatment [2,3,4,5,6,7,8,9,10,11,12].
The aetiology and pathogenesis of XGP are not well understood but are thought to be multifactorial. Chronic infections, urinary tract obstruction, and immune-mediated processes are potential contributing factors [1]. Bacterial pathogens such as Escherichia coli, Pseudomonas aeruginosa, and Proteus species have been isolated in patients diagnosed with XGP, suggesting a possible link to chronic bacterial prostatitis [6,13,14,15]. The inflammatory process leads to the formation of xanthogranulomatous tissue, which can resemble a prostatic neoplasm in imaging studies, thus complicating the diagnostic process.
Clinically, patients with XGP typically present with lower urinary tract symptoms (LUTS), including urinary frequency, urgency, dysuria, and obstructive symptoms. These non-specific symptoms overlap significantly with those of other common prostatic conditions, which can contribute to diagnostic challenges. In some cases, elevated serum prostate-specific antigen (PSA) levels and imaging findings that mimic prostate carcinoma may lead to suspicion of malignancy, prompting further diagnostic interventions, such as prostate biopsies or even surgical treatment. In a few instances, misdiagnosis has led to radical prostatectomy, underscoring the need for caution in clinical decision-making when malignancy is suspected.
The diagnosis of XGP is confirmed through histopathological examination, which reveals characteristic xanthogranulomatous changes. These changes are marked by aggregates of foamy macrophages, multinucleated giant cells, and chronic inflammatory cells. The foamy macrophages stain positive for the histiocytic marker CD163 in immunohistochemistry analyses and aid in differentiating XGP from carcinoma. However, due to tissue destruction and inflammation, histopathological diagnosis can be challenging [16]. Given the overlap in clinical presentation with other prostatic diseases, the role of biopsy and careful histopathological analysis cannot be overemphasized. The lack of specific clinical or imaging features makes it difficult to distinguish XGP from malignancy or other benign inflammatory conditions preoperatively.
The management of XGP is not standardized due to the rarity of the condition, but treatment options include both surgical and conservative approaches. Patients with a systematic response to XGP, such as the presence of fever, are treated primarily with antibiotics. This approach has shown success in patients with milder forms of the disease or when a bacterial aetiology is suspected [2,4,7]. Transurethral resection of the prostate (TURP) has commonly been employed to relieve obstructive symptoms and obtain diagnostic tissue [12].
This systematic review aims to summarize the current knowledge regarding the clinical characteristics, diagnostic modalities, treatment options, and outcomes of XGP. By synthesizing data from existing case reports and case series, we seek to provide a comprehensive understanding of this rare condition and highlight the challenges in differentiating it from prostatic malignancy. Improved awareness of XGP among clinicians may help reduce the incidence of unnecessary surgical procedures and guide more appropriate management strategies for affected patients.
2. Materials and Methods
A comprehensive search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines using the following databases: PubMed, Embase, and Medline. We searched these databases from inception until October 2024. The reference lists of included studies and relevant reviews were manually checked to identify additional potential studies.
The search strategy combined key terms related to xanthogranulomatous prostatitis with terms chosen with the assistance of our local health district librarian. The terms used were “xanthogranulomatous” AND “granulomatous” and “prostatitis”. An English language restriction was imposed.
2.1. Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria:
- Original articles reporting on patients diagnosed with xanthogranulomatous prostatitis upon histopathological examination.
- Studies providing data on at least one of the following outcomes: patient demographics, clinical presentation, mode of diagnosis, treatment modalities, and patient outcomes.
- Case reports, case series, observational studies (cohort and case–control), and clinical trials were included.
Articles were excluded if they met the following criteria:
- Reviews, commentaries, editorials, letters, conference abstracts, or expert opinions.
- Studies not providing specific data on outcomes for patients.
- Studies on paediatric or neonatal patients (aged < 18 years).
2.2. Data Extraction and Quality Assessment
Data were extracted using a pre-specified data extraction form. The following information was obtained from each study: first author’s name, year of publication, study design, patients’ baseline characteristics, clinical findings, diagnostic methods, treatment methods, and outcomes.
The methodological quality of the included studies was assessed by two independent authors (K.C. and G.M.). Any disagreements between reviewers were resolved through discussion or consultation with a third reviewer if necessary.
2.3. Data Synthesis and Analysis
Given the nature of the included studies being primarily case reports and case series, a meta-analysis was not feasible. Instead, data were synthesized qualitatively. Patient characteristics, such as age, gender, and presenting symptoms, were described. In addition, details about diagnostic procedures, pathologic findings, treatments, and outcomes were collated. Descriptive statistics were used to summarize the data.
2.4. Risk of Bias Across Studies
The risk of bias in case reports and case series was evaluated using the Oxford Centre for Evidence-Based Medicine: Levels of Evidence (CEBM) document. All articles were of level 4 evidence.
Given that case reports and case series are inherently high in bias and low in evidence level, the overall evidence generated by this review should be interpreted with caution.
2.5. Ethics Approval and Consent to Participate
As this study was a systematic review, it did not involve direct contact with patients or alteration to patient care, and thus did not require ethics committee approval.
2.6. Availability of Data and Material
All data generated or analysed during this study are included in this published article or are available from the corresponding author on request.
3. Results
3.1. Study Selection and Characteristics
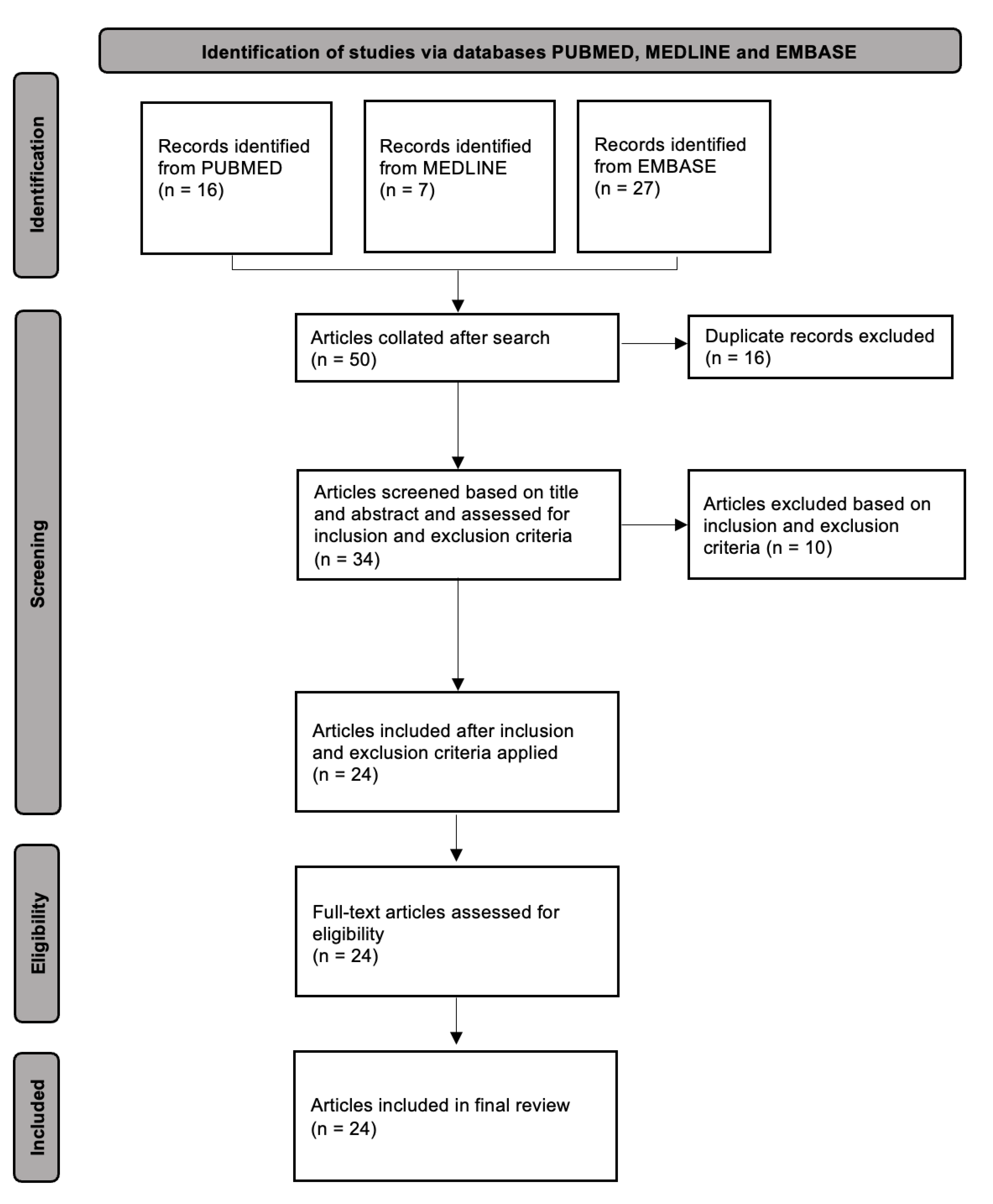
The initial search yielded a total of 50 studies, which were screened for eligibility. Of these, 26 were excluded due to various reasons, such as irrelevant topics, not reporting specific data on patients, or not being original articles. A total of 24 articles, all case reports and case series, met our inclusion criteria and were included in the final qualitative synthesis [2,3,4,5,6,7,8,9,10,11,12,13,14,15,17,18,19,20,21,22,23,24,25,26]. The PRISMA flow diagram of the study selection process is shown in Figure 1.
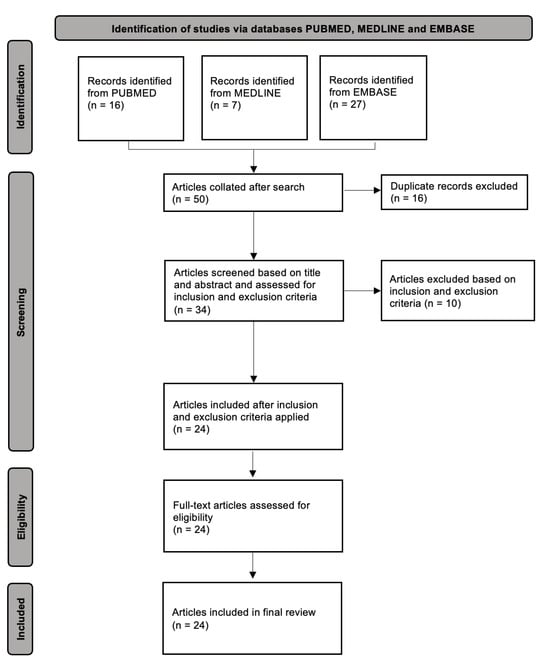
Figure 1.
PRISMA flow diagram for systematic review of xanthogranulomatous prostatitis.
3.2. Patient Characteristics and Clinical Presentation
The 24 articles included a total of 33 patients (Table 1) with a diagnosis of xanthogranulomatous prostatitis, with ages ranging from 47 to 82 (median age: 64). The most common presenting symptom was lower urinary tract symptoms (LUTS) (n = 27, 81.8%), followed by fevers (n = 10, 30.3%) and haematuria (n = 9, 27.3%). The median PSA was 6.5 (range = 0.54 to 172.5). The initial diagnoses were prostate carcinoma (n = 17, 51.5%), benign prostatic enlargement (BPE) (n = 10, 30.3%), and prostatitis (n = 5, 15.2%) (Table S1).

Table 1.
List of all articles and patients included in the review in chronological order [2,3,4,5,6,7,8,9,10,11,12,13,14,15,17,18,19,20,21,22,23,24,25,26].
3.3. Diagnostic Procedures and Pathologic Findings
All patients received a diagnosis of xanthogranulomatous prostatitis confirmed by histopathological analysis. Imaging modalities varied, including computed tomography, ultrasonography, and magnetic resonance imaging (MRI). MRI of the prostate was performed in 10 patients, with a Prostate Imaging Reporting and Data System (PI-RADS) 5 lesion identified in 5 patients.
3.4. Treatment and Outcomes
While there was variation in the approach to management across case reports, transurethral resection of the prostate (TURP) was a mainstay of therapy (n = 20, 60.6%), followed by non-surgical management with or without antibiotic therapy (n = 9, 27.3%).
Importantly, one patient underwent unnecessary radical prostatectomy due to a missed diagnosis of xanthogranulomatous prostatitis. This patient proceeded to radical surgery based on clinical and imaging findings and a histopathological finding of prostate carcinoma, which was later revised to xanthogranulomatous prostatitis.
All patients responded well to their respective management, with no deaths and the resolution of symptoms.
3.5. Quality of Included Studies
As per the Oxford Centre for Evidence-Based Medicine (CEBM) Critical Appraisal Tools, the quality of the included studies varied. Many case reports and series lacked details about patient demographics, specific interventions, or precise clinical outcomes, contributing to the risk of bias. It is important to interpret the results keeping this limitation in mind (Table S2).
4. Discussion
This systematic review highlights the clinical characteristics, risk factors, diagnosis, treatment, and outcomes of xanthogranulomatous prostatitis (XGP), a rare inflammatory condition of the prostate. Our findings provide insights into the diagnostic challenges and management approaches of XGP, based on the analysis of 24 articles involving 33 patients. XGP predominantly presents with lower urinary tract symptoms (LUTS) in older patients, with a median age of 64 years, and can often mimic other prostatic diseases, especially prostate carcinoma.
One of the key findings of this review is that over half of the patients were initially suspected of harbouring clinically significant prostate carcinoma, which highlights the diagnostic uncertainty surrounding XGP. Five patients had a prostate MRI demonstrating a PI-RADS 5 lesion. This similarity in clinical presentation often leads to an initial misdiagnosis, emphasizing the importance of accurate differential diagnosis to avoid unnecessary invasive interventions. In our review, one patient underwent unnecessary radical prostatectomy, highlighting the need to follow well-established international protocols in the diagnosis of prostate carcinoma and the importance of a clear understanding of the distinct morphological features of XGP [3].
Histopathological examination remains the gold standard for the diagnosis of XGP. Characteristic findings of xanthogranulomatous inflammation were consistently reported in all patients, confirming that a definitive diagnosis cannot be reliably made based on imaging or clinical symptoms alone. The isolation of various pathogens, including Escherichia coli, Pseudomonas aeruginosa, Proteus species, and Enterobacter species, suggests that XGP may be associated with an infectious aetiology, though the exact pathogenesis remains unclear [6,13,14,15]. This raises important questions about the role of chronic bacterial infections in the development of this condition, which warrants further investigation.
Management approaches for XGP varied among the cases reviewed. The majority of patients (60.6%) were treated with transurethral resection of the prostate (TURP), which proved effective in alleviating symptoms and debulking the inflamed tissue. However, a significant proportion of patients (27.3%) were successfully managed with conservative therapies, such as antibiotics, highlighting that surgical intervention may not always be necessary. These findings suggest that the choice of treatment should be individualized based on the severity of symptoms and patient comorbidities. Our recommendation is to commence antibiotic and alpha-blocker therapy for up to 4–6 weeks until symptoms resolve, unless there is presence of prostatic abscess, which requires more urgent surgical intervention in the form of transurethral deroofing or percutaneous drainage. If symptoms persist, re-imaging and uroflowmetry should be performed, and if there is suggestion of bladder outlet obstruction or persistence of symptoms, a TURP should be performed. Once treatment is complete, re-imaging and PSA testing can be considered to assess response to therapy. We also recommend the use of a multi-disciplinary team in the management of this rare entity.
This review underscores the importance of adhering to well-established protocols for the evaluation of suspected prostate carcinoma, including the use of prostate-specific antigen (PSA) levels, imaging, and biopsy, to minimize the risk of overtreatment. Given the rarity of XGP, its clinical presentation is easily mistaken for malignancy, which can lead to aggressive treatment approaches that may not be warranted. Therefore, clinicians should maintain a high index of suspicion for XGP in patients presenting with LUTS and a history of recurrent urinary tract infections or other risk factors, particularly when imaging findings are atypical for carcinoma.
The limitations of this systematic review include the reliance on case reports and case series, which are inherently prone to bias and may not represent the broader population. The small sample size and the variability in reported clinical details also limit the generalizability of our findings. Another important limitation is that there is a confounder in the review that only patients that undergo surgical intervention or have a biopsy have tissue confirmation of XGP, which may mean that a percentage of patients with a clinical diagnosis of BPE or prostatitis treated conservatively are under-represented. Nevertheless, this review provides a comprehensive synthesis of the available literature on XGP and serves to raise awareness of this rare condition among clinicians.
5. Conclusions
XGP is a rare but important differential diagnosis in patients presenting with LUTS, or with clinical examination and PSA levels suggestive of prostate carcinoma. Accurate diagnosis via histopathological examination is crucial to avoid unnecessary radical procedures. Both surgical and conservative management options are available, with TURP being the most common approach. Conservative approaches in the absence of prostate abscess should be considered as a first-line treatment, followed by TURP if patients fail to improve. Future research should aim to elucidate the pathogenesis of XGP and establish standardized diagnostic and management protocols to improve patient outcomes.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/siuj6020026/s1, Table S1: Detailed review of all included articles relating to xanthogranulomatous prostatitis; Table S2: CEBM Analysis of all articles included in systematic review.
Author Contributions
K.K.Y.C.—Conceptualization, Methodology, Writing—Original Draft, Writing—Review and Editing; G.C.H.M.—Conceptualization, Methodology, Data Curation; E.L.H.W.—Supervision, Writing—Review and Editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data supporting the findings of this study are available within the article and/or its Supplementary Material.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bryan, R.L.; Newman, J.; Campbell, A.; Fitzgerald, G.; Kadow, C.; O’Brien, J.M. Granulomatous prostatitis: A clinicopathological study. Histopathology 1991, 19, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.M.C. Xanthogranulomatous Prostatitis: Novel Presentation of a Rare Condition. Am. J. Case Rep. 2021, 22, e932869. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Sureka, S.K.; Ruidas, S.; Lal, H. Xanthogranulomatous prostatitis mimicking prostatic adenocarcinoma: A diagnostic dilemma. BMJ Case Rep. 2019, 12, e231945. [Google Scholar] [CrossRef]
- Lee, H.Y.; Kuo, Y.T.; Tsai, S.Y.; Li, C.C.; Wu, W.J.; Huang, C.H.; Juan, Y.-S. Xanthogranulomatous prostatitis: A rare entity resembling prostate adenocarcinoma with magnetic resonance image picture. Clin. Imaging 2012, 36, 858–860. [Google Scholar] [CrossRef]
- Mukendi, A.M.; Doherty, S.; Mohanlal, R. Xanthogranulomatous prostatitis: A rare mimicker of prostate adenocarcinoma. Clin. Case Rep. 2020, 8, 203–205. [Google Scholar] [CrossRef]
- Mehta, S.; Kampantais, S.; Wolfe, K.; Liyanage, S.H. Xanthogranulomatous prostatitis: Impressive MRI appearance of a rare entity. Asian J. Urol. 2020, 7, 384–386. [Google Scholar] [CrossRef]
- Tang, Y.; Yang, J.; Zhou, C.; Li, J.; Hu, S. False-positive mpMRI and true-negative 68Ga-PSMA PET/CT xanthogranulomatous prostatitis: A case report. Transl. Androl. Urol. 2022, 11, 561–566. [Google Scholar] [CrossRef]
- Xing, L.; Liu, Z.; Deng, G.; Wang, H.; Zhu, Y.; Shi, P.; Huo, B.; Li, Y. Xanthogranulomatous prostatitis with prostato-rectal fistula: A case report and review of the literature. Res. Rep. Urol. 2016, 8, 165–168. [Google Scholar] [CrossRef]
- Rafique, M.; Yaqoob, N. Xanthogranulomatous prostatitis: A mimic of carcinoma of prostate. World J. Surg. Oncol. 2006, 4, 30. [Google Scholar] [CrossRef]
- Demeter, J.; Deshmukh, A.; Salari, B.; Sindhwani, P.; Khan, O. An improbable trifecta: Occurrence of xanthogranulomatous prostatitis, prostate cancer, and prostatic abscess in a single patient. Urol. Case Rep. 2020, 35, 101526. [Google Scholar] [CrossRef]
- De Silva, S.; De Silva, L.; Sooriyaarchchi, S.; Wijesighe, H.; Ranaweera, G.; De Silva, S.; De Silva, C. Different clinical presentations of xanthogranulomatous prostatitis: A case series and review of the literature. J. Clin. Urol. 2021, 14, 293–299. [Google Scholar]
- Pastore, A.L.; Palleschi, G.; Fuschi, A.; Porta, N.; Cerbelli, B.; Di Cristofano, C.; Petrozza, V.; Carbone, A. Hematospermia and xanthogranulomatous prostatitis: An unusual onset of a rare diagnosis. Can. Urol. Assoc. J. 2013, 7, E820–E822. [Google Scholar]
- Karzoun, M.Z.; Al-Naimi, A.; Abdelfattah, O.; Ibrahim, T. Granulomatous and xanthogranulomatous prostatitis: A case report. Urol. Case Rep. 2022, 40, 101887. [Google Scholar]
- Belga, S.; Chen, W.; Low, G.; Cervera, C. Xanthogranulomatous prostatitis presenting as Pseudomonas aeruginosa prostatic abscesses: An uncommon complication after kidney transplantation. IDCases 2019, 17, e00559. [Google Scholar] [PubMed]
- Miekoś, E.; Włodarczyk, W.; Szram, S. Xanthogranulomatous prostatitis. Int. Urol. Nephrol. 1986, 18, 433–437. [Google Scholar]
- Bostwick, D.G.; Cheng, L. Urologic Surgical Pathology; Elsevier Health Sciences: Gurugram, India, 2008; 1037p. [Google Scholar]
- Cheng, Y.; Zhang, X.; Ji, Q.; Shen, W. Xanthogranulomatous prostatitis: Multiparametric MRI appearances. Clin. Imaging 2014, 38, 755–757. [Google Scholar]
- Grewal, N.; Tuli, A.; Sridhar, F.K.; Mammen, K.J. Xanthogranulomatous Prostatitis with Benign Prostatic Hyperplasia: A Rare Combination. CHRISMED J. Health Res. 2017, 4, 214. [Google Scholar]
- Jabbour, Y.; Lamchahab, H.; Harrison, S.; El Ouazzani, H.; Karmouni, T.; El Khader, K.; Koutani, A.; Andaloussi, A.I.A. Prostatic Abscess on Xanthogranulomatous Prostatitis: Uncommon Complication of an Uncommon Disease. Case Rep. Urol. 2018, 2018, 5417903. [Google Scholar]
- Min, K.S.; Oh, S.Y.; Chun, J.Y.; Um, J.D.; Choi, S.H.; Jung, S.J. A Case of Xanthogranulomatous Prostatitis Concurrent with a Prostatic Abscess. Korean J. Androl. 2011, 29, 174–176. [Google Scholar]
- Noyola, A.; Gil, J.F.; Lujano, H.; Piñon, O.; Muñoz, G.; Michel, J.M.; Garcia, J.; Valdez, J.; Morales, O. Xanthogranulomatous Prostatitis, a Rare Prostatic Entity. Urol. Case Rep. 2016, 10, 4–5. [Google Scholar]
- Patil, N.; Kundargi, V.S.; Patil, S.B.; Biradar, A.K.; Desai, A.S. Xanthogranulomatous Prostatitis: A Rare Case Report. Med. Surg. Urol. 2014, 3, 1. Available online: https://www.omicsonline.org/open-access/xanthogranulomatous-prostatitis-a-rare-case-report-2168-9857.1000131.php?aid=25027 (accessed on 30 September 2024).
- Shukla, P.; Gulwani, H.V.; Kaur, S. Granulomatous prostatitis: Clinical and histomorphologic survey of the disease in a tertiary care hospital. Prostate Int. 2017, 5, 29–34. [Google Scholar] [PubMed]
- Valsangkar, R.S.; Singh, D.P.; Gaur, D.D. Xanthogranulomatous prostatitis: Rare presentation of rare disease. Indian J. Urol. 2012, 28, 204–205. [Google Scholar] [PubMed]
- Wollin, D.A.; Brucker, B.M. Dramatic Enlargement of the Prostate due to Xanthogranulomatous Inflammation. Low. Urin. Tract Symptoms 2015, 7, 166–168. [Google Scholar]
- Zaber, K.; Al-Bareeq, R. Xanthogranulomatous prostatitis causing entero-vesical fistula. Bahrain Med. Bull. 2004, 26, 165–166. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Société Internationale d’Urologie. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).