An 84-year-old fit and well male farmer presented to the emergency department with acute urinary clot retention. A 3-way indwelling catheter for continuous bladder irrigation was inserted. Vital signs and blood tests were unremarkable. Digital-rectal examination revealed a grossly enlarged benign prostate. Prostate specific antigen (PSA) was elevated at 25.6 ng/mL, but PSA density was normal at 0.038 ng/mL2. CT demonstrated prostatomegaly, with the prostate measuring 117 mm × 92 mm × 127 mm, extending superiorly beyond the true pelvis (Figure 1). There was no associated hydroureteronephrosis. Gland volume was calculated at 665 mL.

Figure 1.
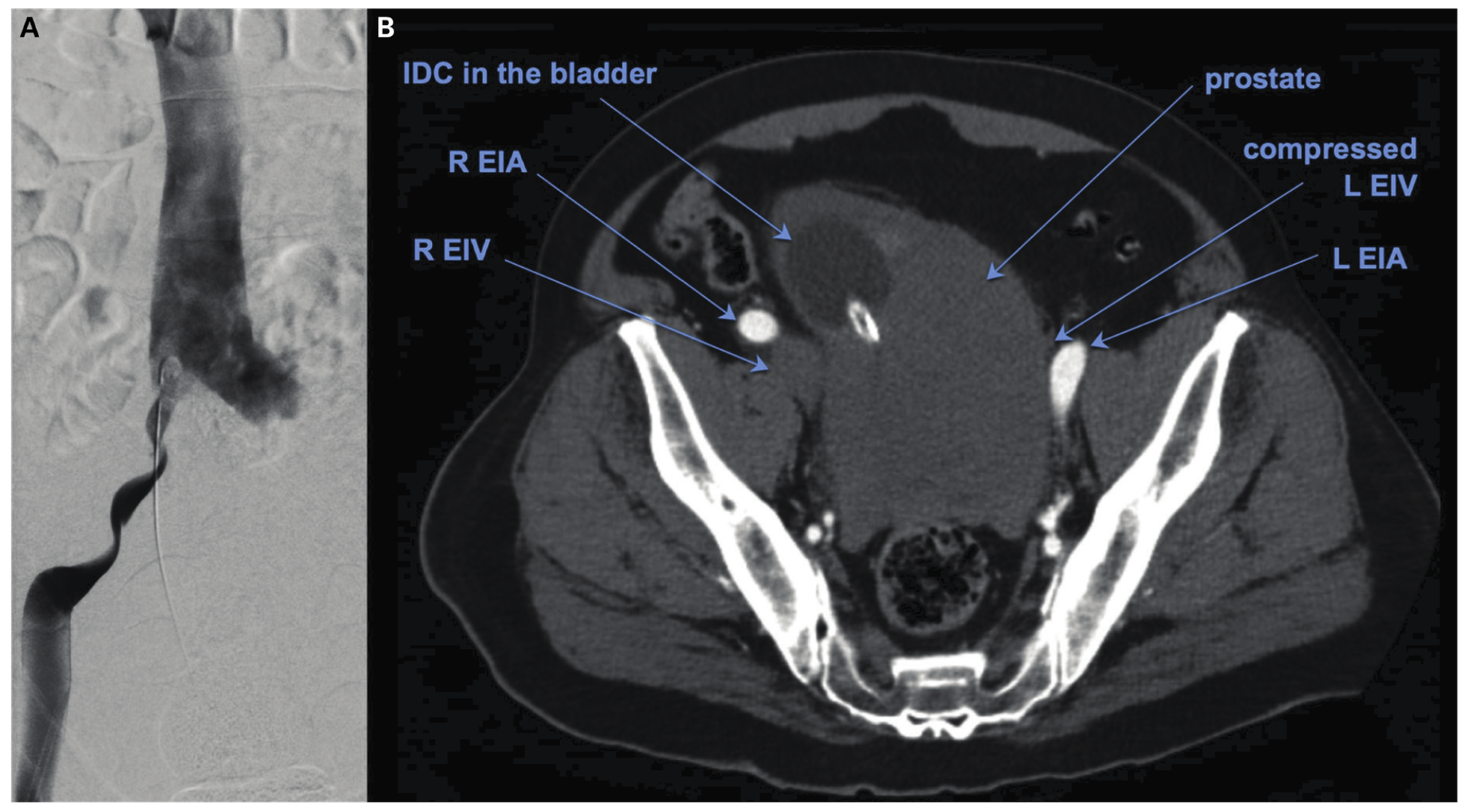
(A) Venogram via the right femoral sheath showing extrinsic compression and narrowing of the left iliac veins. The inferior impression is from the external iliac artery and the superior impression is from the internal iliac artery. Figure 1. (A) CT angiogram of the pelvis in the axial plane with bilateral labelled structures for comparison. The left iliac vein is compressed by the iliac arteries and pelvis sidewall, as seen on the venogram.
Forty-eight hours into his admission, the patient experienced a syncopal episode associated with rapid atrial fibrillation, tachypnoea, and a troponin leak. CT pulmonary angiogram (CTPA) revealed extensive bilateral, non-occlusive PE extending distally from the main pulmonary arteries. Lower limb Doppler ultrasonography confirmed left below knee deep vein thrombosis (DVT).
The patient subsequently underwent catheter-directed thrombolysis. Significant extrinsic compression of the left iliac veins was noted between the megaprostate and the external and internal iliac arteries. Alteplase was infused at 1 mg/hour via each infusion catheter (total 2 mg/hour) for 24 hours, resulting in complete resolution of the bilateral PE down to the segmental level. However, this resulted in transfusion-dependent haematuria.
Multidisciplinary consensus supported prostate artery embolisation (PAE) for the management of intractable haematuria in the context of therapeutic anticoagulation and to alleviate iliac venous compression through organ atrophy in the longer term. Transarterial particle embolisation of the prostate using the PErFecTED technique was performed via left conventional radial access (Figure 2). Macrohaematuria resolved within 24 hours of embolisation with a successful trial-of-void 14 days post procedure.
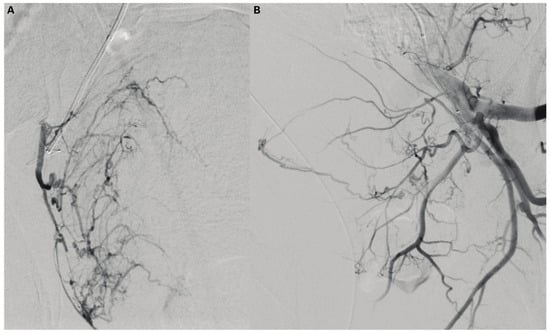
Figure 2.
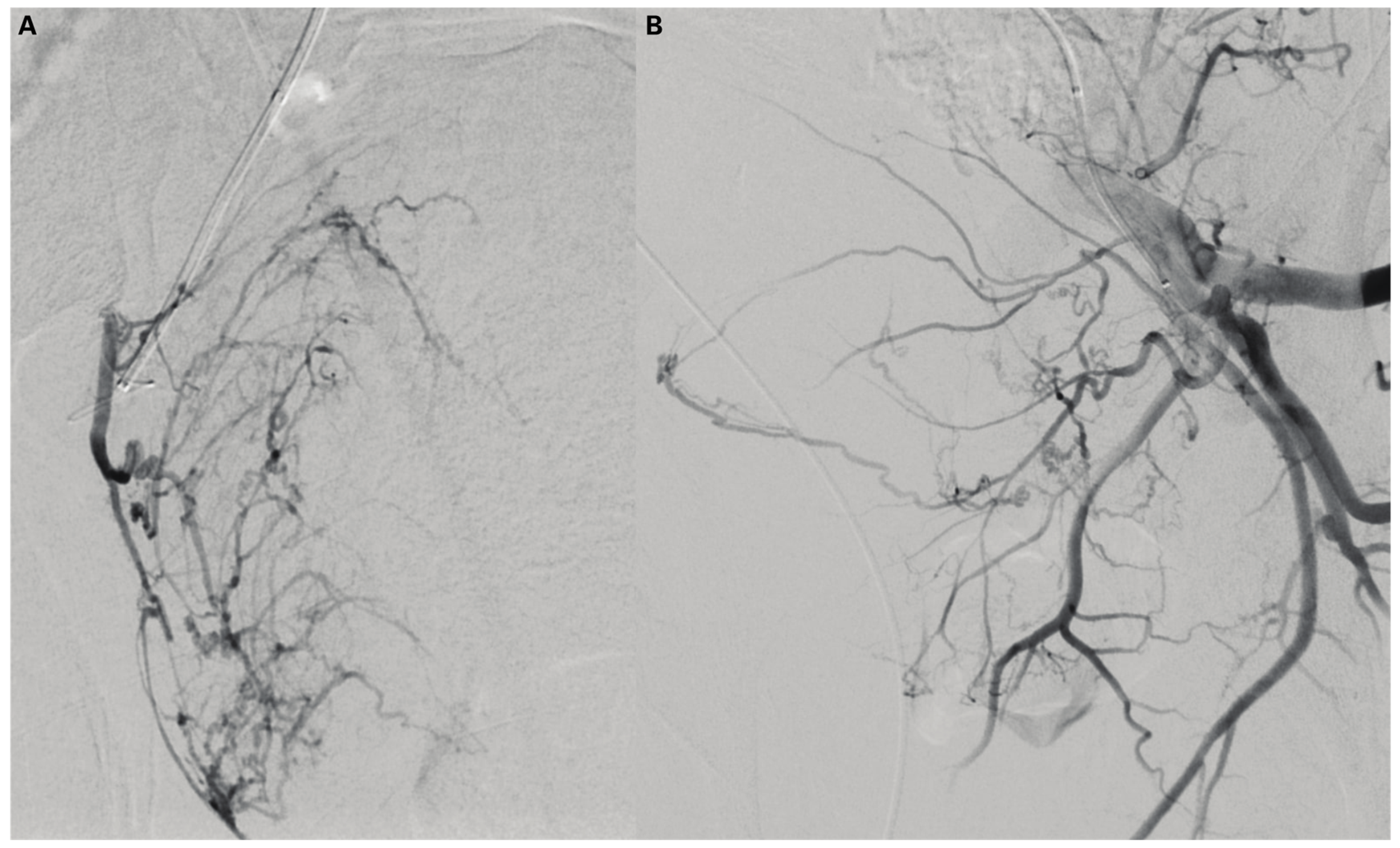
(A) Angiogram via the microcatheter in the right prostate artery. The base catheter is positioned in the right obturator artery which arises conventionally off the anterior division of the internal iliac artery. (B) The left prostate artery arises from the left obturator artery, which is replaced arising from the left external iliac artery.
Conflicts of Interest
None declared. Patient Consent: Obtained.
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2023 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.