
Microleakage Study of a Bulk Fill over an Uncured Adhesive System

 ,
,  , , ,
, , ,  ,
,  ,
,  and
and 
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection
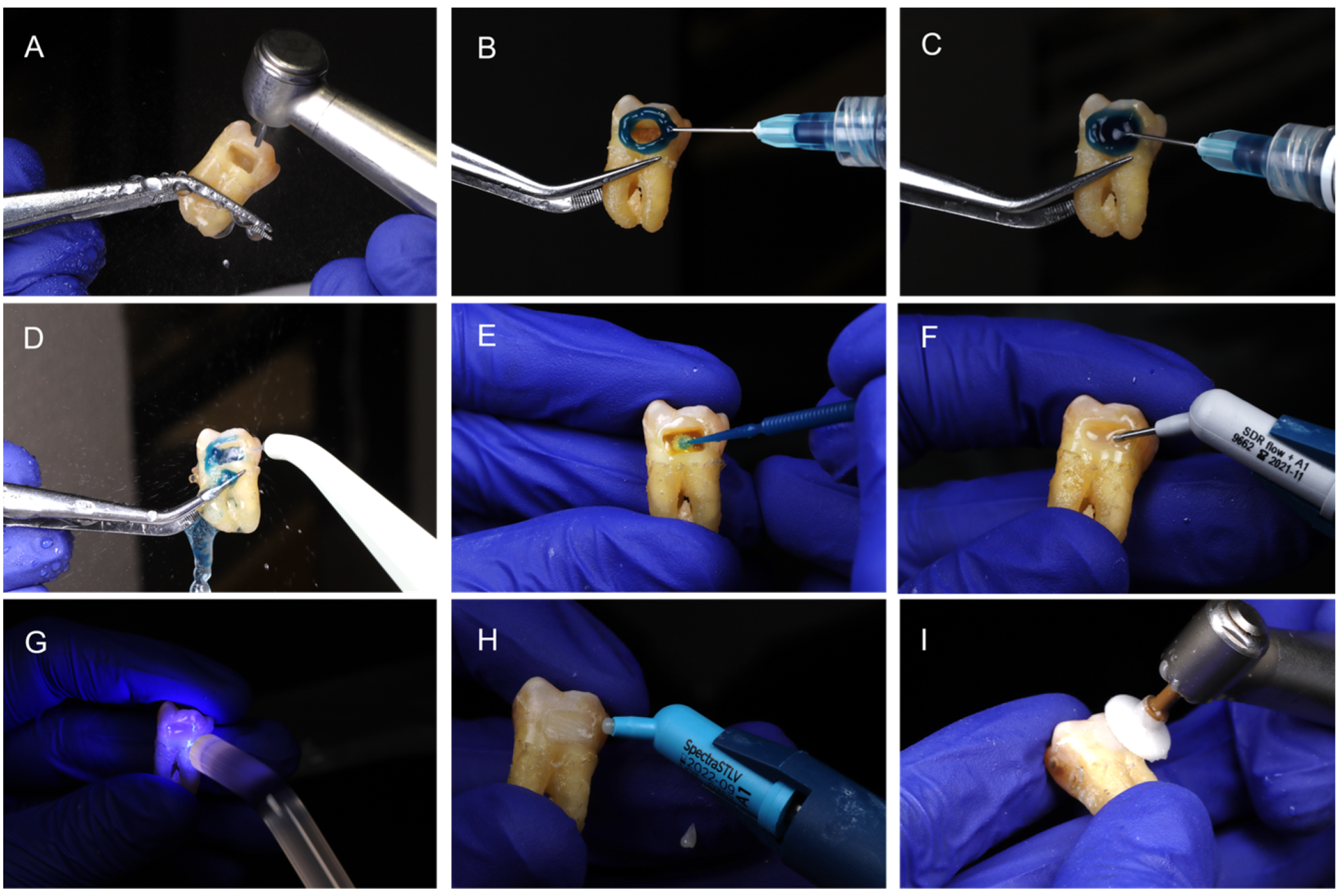
2.2. Sample Preparation
2.3. Study Groups
2.4. Nuclear Medicine Technique for Microleakage Assessment
2.5. Statistical Analysis
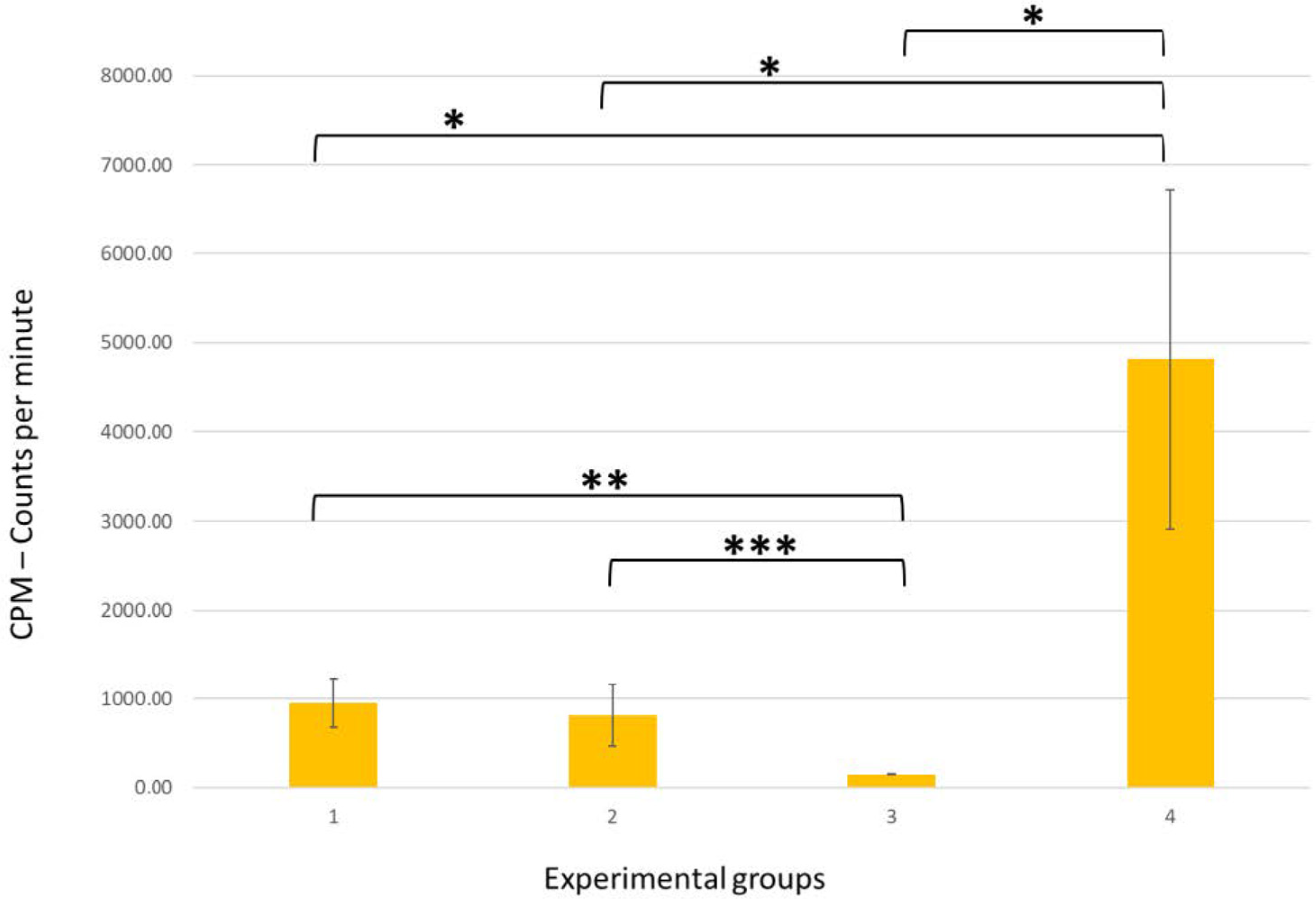
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breschi, L.; Maravic, T.; Cunha, S.R.; Comba, A.; Cadenaro, M.; Tjaderhane, L.; Pashley, D.H.; Tay, F.R.; Mazzoni, A. Dentin bonding systems: From dentin collagen structure to bond preservation and clinical applications. Dent. Mater. 2018, 34, 78–96. [Google Scholar] [CrossRef] [PubMed]
- Tjaderhane, L. Dentin bonding: Can we make it last? Oper. Dent. 2015, 40, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Nakabayashi, N.; Nakamura, M.; Yasuda, N. Hybrid layer as a dentin-bonding mechanism. J. Esthet. Dent. 1991, 3, 133–138. [Google Scholar] [CrossRef]
- Nakabayashi, N.; Kojima, K.; Masuhara, E. The promotion of adhesion by the infiltration of monomers into tooth substrates. J Biomed. Mater. Res. 1982, 16, 265–273. [Google Scholar] [CrossRef]
- Al-Nabulsi, M.; Daud, A.; Yiu, C.; Omar, H.; Sauro, S.; Fawzy, A.; Daood, U. Co-Blend Application Mode of Bulk Fill Composite Resin. Materials 2019, 12, 2504. [Google Scholar] [CrossRef]
- Tay, F.R.; Pashley, D.H. Have dentin adhesives become too hydrophilic? J. Can. Dent. Assoc. 2003, 69, 726–731. [Google Scholar] [PubMed]
- Sano, H.; Shono, T.; Takatsu, T.; Hosoda, H. Microporous dentin zone beneath resin-impregnated layer. Oper. Dent. 1994, 19, 59–64. [Google Scholar] [PubMed]
- Pashley, D.H.; Tay, F.R.; Yiu, C.; Hashimoto, M.; Breschi, L.; Carvalho, R.M.; Ito, S. Collagen degradation by host-derived enzymes during aging. J. Dent. Res. 2004, 83, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Pashley, D.H.; Tay, F.R.; Breschi, L.; Tjaderhane, L.; Carvalho, R.M.; Carrilho, M.; Tezvergil-Mutluay, A. State of the art etch-and-rinse adhesives. Dent. Mater. 2011, 27, 1–16. [Google Scholar] [CrossRef]
- Pashley, D.H.; Ciucchi, B.; Sano, H.; Horner, J.A. Permeability of dentin to adhesive agents. Quintessence Int. 1993, 24, 618–631. [Google Scholar]
- Tay, F.R.; Hashimoto, M.; Pashley, D.H.; Peters, M.C.; Lai, S.C.; Yiu, C.K.; Cheong, C. Aging affects two modes of nanoleakage expression in bonded dentin. J. Dent. Res. 2003, 82, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Cadenaro, M.; Antoniolli, F.; Sauro, S.; Tay, F.R.; Di Lenarda, R.; Prati, C.; Biasotto, M.; Contardo, L.; Breschi, L. Degree of conversion and permeability of dental adhesives. Eur. J. Oral Sci. 2005, 113, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Spencer, P.; Wang, Y. Adhesive phase separation at the dentin interface under wet bonding conditions. J. Biomed. Mater. Res. 2002, 62, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Frassetto, A.; Breschi, L.; Turco, G.; Marchesi, G.; Di Lenarda, R.; Tay, F.R.; Pashley, D.H.; Cadenaro, M. Mechanisms of degradation of the hybrid layer in adhesive dentistry and therapeutic agents to improve bond durability—A literature review. Dent. Mater. 2016, 32, e41–e53. [Google Scholar] [CrossRef]
- Hashimoto, M. A review—Micromorphological evidence of degradation in resin-dentin bonds and potential preventional solutions. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 92, 268–280. [Google Scholar] [CrossRef]
- Boruziniat, A.; Alizadeh, S.; Gifani, M.; Cehreli, Z.C.; Khazaei, Y. The effect of ethanol wet bonding technique on postoperative hypersensitivity of Class II composite restorations: A randomized trial. Dent. Res. J. 2021, 18, 97. [Google Scholar]
- Taschner, M.; Kummerling, M.; Lohbauer, U.; Breschi, L.; Petschelt, A.; Frankenberger, R. Effect of double-layer application on dentin bond durability of one-step self-etch adhesives. Oper. Dent. 2014, 39, 416–426. [Google Scholar] [CrossRef]
- King, N.M.; Tay, F.R.; Pashley, D.H.; Hashimoto, M.; Ito, S.; Brackett, W.W.; Garcia-Godoy, F.; Sunico, M. Conversion of one-step to two-step self-etch adhesives for improved efficacy and extended application. Am. J. Dent. 2005, 18, 126–134. [Google Scholar]
- Mena-Serrano, A.; Costa, T.R.; Patzlaff, R.T.; Loguercio, A.D.; Reis, A. Effect of sonic application mode on the resin-dentin bond strength and dentin permeability of self-etching systems. J. Adhes. Dent. 2014, 16, 435–440. [Google Scholar]
- Chapman, J.L.; Burgess, J.O.; Holst, S.; Sadan, A.; Blatz, M.B. Precuring of self-etching bonding agents and its effect on bond strength of resin composite to dentin and enamel. Quintessence Int. 2007, 38, 637–641. [Google Scholar]
- Camps, J.; Pashley, D. Reliability of the dye penetration studies. J. Endod. 2003, 29, 592–604. [Google Scholar] [CrossRef]
- Jafari, F.; Jafari, S. Importance and methodologies of endodontic microleakage studies: A systematic review. J. Clin. Exp. Dent. 2017, 9, e812–e819. [Google Scholar] [CrossRef]
- Jafari, F.; Rahimi, S.; Shahi, S.; Jafari, S. Endodontic microleakage studies: Correlation among different methods, clinical relevance, and potential laboratory errors. Minerva Stomatol. 2017, 66, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Pereira, I.R.; Carvalho, C.; Paulo, S.; Martinho, J.P.; Coelho, A.S.; Paula, A.B.; Marto, C.M.; Carrilho, E.; Botelho, M.F.; Abrantes, A.M.; et al. Apical Sealing Ability of Two Calcium Silicate-Based Sealers Using a Radioactive Isotope Method: An In Vitro Apexification Model. Materials 2021, 14, 6456. [Google Scholar] [CrossRef] [PubMed]
- Chesterman, J.; Jowett, A.; Gallacher, A.; Nixon, P. Bulk-fill resin-based composite restorative materials: A review. Br. Dent. J. 2017, 222, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Arola, D.D.; Gu, L.; Kim, Y.K.; Mai, S.; Liu, Y.; Pashley, D.H.; Tay, F.R. Functional biomimetic analogs help remineralize apatite-depleted demineralized resin-infiltrated dentin via a bottom-up approach. Acta. Biomater. 2010, 6, 2740–2750. [Google Scholar] [CrossRef]
- De Munck, J.; Van Landuyt, K.; Peumans, M.; Poitevin, A.; Lambrechts, P.; Braem, M.; Van Meerbeek, B. A critical review of the durability of adhesion to tooth tissue: Methods and results. J. Dent. Res. 2005, 84, 118–132. [Google Scholar] [CrossRef]
- McMurphy, A.; Xu, X.; Fournier, S.; Cehreli, Z.C.; Sherman, K.; Tremmel, C.; Qingzhao, Y.; Townsend, J. Effect of Cured Versus Uncured Adhesive Inclusion on the Microtensile Bond Strength of Sealants. J. Dent. Child. 2017, 84, 58–64. [Google Scholar]
- Mazzi, U. Technetium-99m Pharmaceuticals: Preparation and Quality Control in Nuclear Medicine, 1st ed.; Zolle, I., Ed.; Springer: Berlin, Germany, 2007; p. 95. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, M.V.; Pires, S.; Marto, C.M.; Amaro, I.; Coelho, A.; Sousa, J.; Ferreira, M.M.; Botelho, M.F.; Carrilho, E.; Abrantes, A.M.; et al. Microleakage Study of a Bulk Fill over an Uncured Adhesive System. J. Compos. Sci. 2023, 7, 40. https://doi.org/10.3390/jcs7010040
Pinto MV, Pires S, Marto CM, Amaro I, Coelho A, Sousa J, Ferreira MM, Botelho MF, Carrilho E, Abrantes AM, et al. Microleakage Study of a Bulk Fill over an Uncured Adhesive System. Journal of Composites Science. 2023; 7(1):40. https://doi.org/10.3390/jcs7010040
Chicago/Turabian StylePinto, Mariana Vaz, Salomé Pires, Carlos Miguel Marto, Inês Amaro, Ana Coelho, José Sousa, Manuel Marques Ferreira, Maria Filomena Botelho, Eunice Carrilho, Ana Margarida Abrantes, and et al. 2023. "Microleakage Study of a Bulk Fill over an Uncured Adhesive System" Journal of Composites Science 7, no. 1: 40. https://doi.org/10.3390/jcs7010040
APA StylePinto, M. V., Pires, S., Marto, C. M., Amaro, I., Coelho, A., Sousa, J., Ferreira, M. M., Botelho, M. F., Carrilho, E., Abrantes, A. M., & Paula, A. B. (2023). Microleakage Study of a Bulk Fill over an Uncured Adhesive System. Journal of Composites Science, 7(1), 40. https://doi.org/10.3390/jcs7010040