
Factors Influencing Second and Third Dose Observance during Seasonal Malaria Chemoprevention (SMC): A Quantitative Study in Burkina Faso, Mali and Niger

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site and Population
2.2. Study Design
2.3. Data Collection
2.4. Ethical Considerations
2.5. Sample Size and Statistical Analysis
3. Results
3.1. Baseline Characteristic of the Respondents
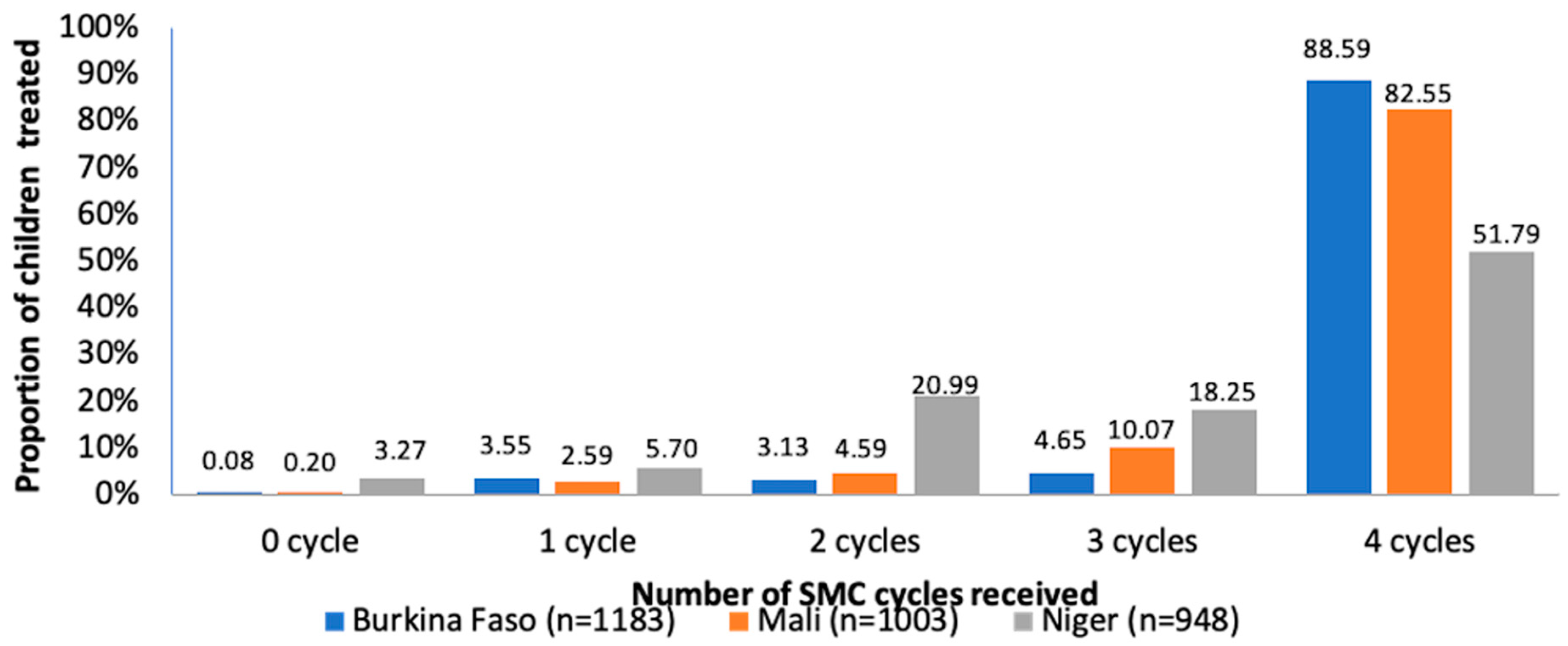
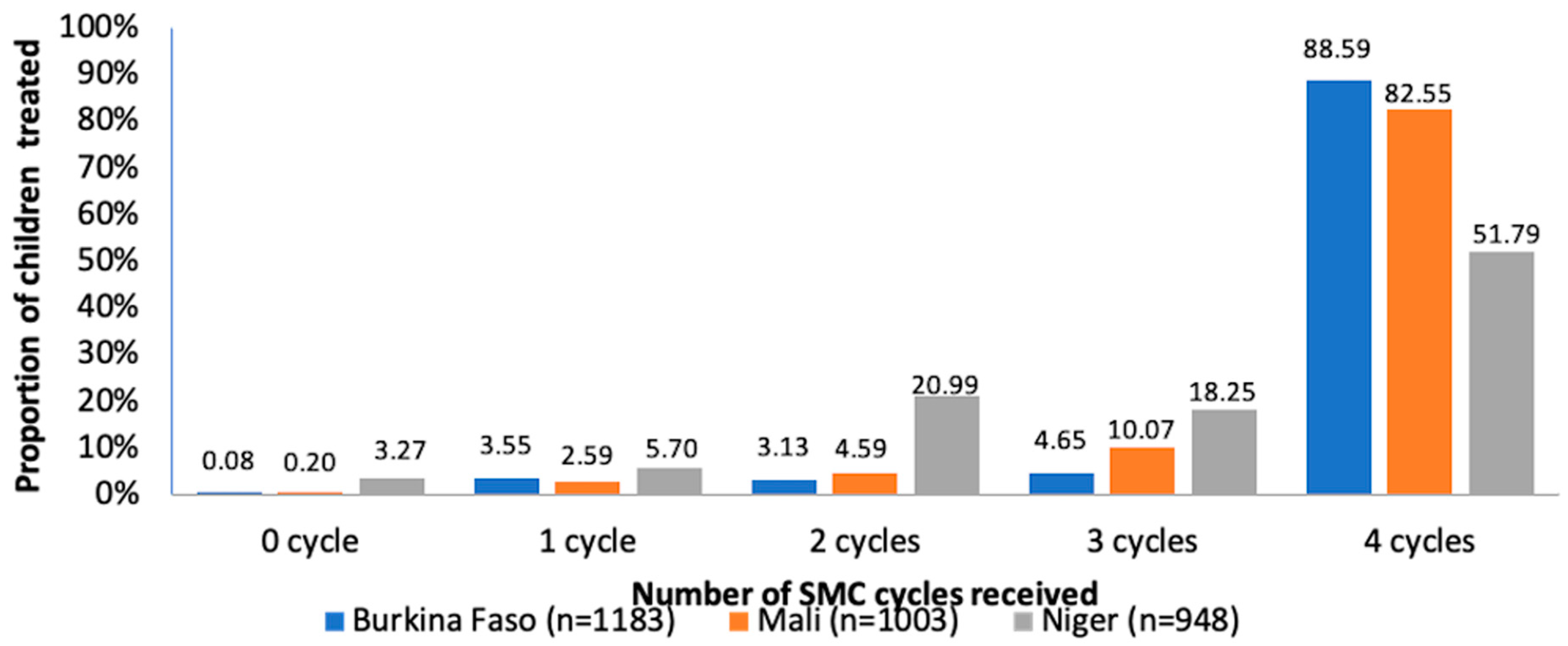
3.2. SMC Coverage and Cards Possession
3.3. Non-Adherence of Second and Third Doses of SMC
3.3.1. Causes of Non-Adherence of the Second Dose Potentially due to Children
3.3.2. Causes of Non-Adherence of the Second Dose due to Parents
3.3.3. Causes of Non-Adherence of the Second Dose due to Community Distributors
3.3.4. Sociodemographic Characteristics of Parents Who Did Not Administer the Second Dose
3.3.5. Causes of Non-Adherence of the Third Dose Potentially due to Children
3.3.6. Causes of Non-Adherence of the Third Dose Potentially due to Parents
3.3.7. Causes of Non-Adherence of the Third Dose Potentially due to Community Distributors
3.3.8. Sociodemographic Characteristics of Parents Who Did Not Administer the Third Dose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malara Report 2020: 20 Years of Global Progress and Challenges; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. WHO Policy Recommendation: Seasonal Malaria Chemoprevention (SMC) for Plasmodium falciparum Malaria Control in Highly Seasonal Transmission Areas of the Sahel Sub-Region in Africa; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Greenwood, B. Review: Intermittent preventive treatment—A new approach to the prevention of malaria in children in areas with seasonal malaria transmission. Trop. Med. Int. Health 2006, 11, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Cairns, M.; Roca-Feltrer, A.; Garske, T.; Wilson, A.L.; Diallo, D.; Milligan, P.J.; Ghani, A.C.; Greenwood, B.M. Estimating the potential public health impact of seasonal malaria chemoprevention in African children. Nat. Commun. 2012, 3, 881. [Google Scholar] [CrossRef] [PubMed]
- Cisse, B.; Sokhna, C.; Boulanger, D.; Milet, J.; Ba, E.H.; Richardson, K.; Hallett, R.; Sutherland, C.; Simondon, K.; Simondon, F.; et al. Seasonal intermittent preventive treatment with artesunate and sulfadoxine-pyrimethamine for prevention of malaria in Senegalese children: A randomised, placebo-controlled, double-blind trial. Lancet 2006, 367, 659–667. [Google Scholar] [CrossRef]
- Kweku, M.; Liu, D.; Adjuik, M.; Binka, F.; Seidu, M.; Greenwood, B.; Chandramohan, D. Seasonal intermittent preventive treatment for the prevention of anaemia and malaria in Ghanaian children: A randomized, placebo controlled trial. PLoS ONE 2008, 3, e4000. [Google Scholar] [CrossRef]
- Dicko, A.; Diallo, A.I.; Tembine, I.; Dicko, Y.; Dara, N.; Sidibe, Y.; Santara, G.; Diawara, H.; Conare, T.; Djimde, A.; et al. Intermittent preventive treatment of malaria provides substantial protection against malaria in children already protected by an insecticide-treated bednet in Mali: A randomised, double-blind, placebo-controlled trial. PLoS Med. 2011, 8, e1000407. [Google Scholar] [CrossRef] [PubMed]
- Konate, A.T.; Yaro, J.B.; Ouedraogo, A.Z.; Diarra, A.; Gansane, A.; Soulama, I.; Kangoye, D.T.; Kabore, Y.; Ouedraogo, E.; Ouedraogo, A.; et al. Intermittent preventive treatment of malaria provides substantial protection against malaria in children already protected by an insecticide-treated bednet in Burkina Faso: A randomised, double-blind, placebo-controlled trial. PLoS Med. 2011, 8, e1000408. [Google Scholar] [CrossRef] [PubMed]
- Bojang, K.A.; Akor, F.; Conteh, L.; Webb, E.; Bittaye, O.; Conway, D.J.; Jasseh, M.; Wiseman, V.; Milligan, P.J.; Greenwood, B. Two strategies for the delivery of IPTc in an area of seasonal malaria transmission in the Gambia: A randomised controlled trial. PLoS Med. 2011, 8, e1000409. [Google Scholar] [CrossRef] [PubMed]
- ACCESS-SMC Partnership. Effectiveness of seasonal malaria chemoprevention at scale in west and central Africa: An observational study. Lancet 2020, 396, 1829–1840. [CrossRef]
- Kirakoya-Samadoulougou, F.; De Brouwere, V.; Fokam, A.F.; Ouédraogo, M.; Yé, Y. Assessing the effect of seasonal malaria chemoprevention on malaria burden among children under 5 years in Burkina Faso. Malar. J. 2022, 21, 143. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.; Issiaka, D.; Traore, T.; Mahamar, A.; Diarra, B.; Sagara, I.; Kone, D.; Doumbo, O.K.; Duffy, P.; Fried, M.; et al. Optimal mode for delivery of seasonal malaria chemoprevention in Ouelessebougou, Mali: A cluster randomized trial. PLoS ONE 2018, 13, e0193296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. High Burden to High Impact: A Target Malaria Response; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Cairns, M.; Ceesay, S.J.; Sagara, I.; Zongo, I.; Kessely, H.; Gamougam, K.; Diallo, A.; Ogboi, J.S.; Moroso, D.; Van Hulle, S.; et al. Effectiveness of seasonal malaria chemoprevention (SMC) treatments when SMC is implemented at scale: Case-control studies in 5 countries. PLoS Med. 2021, 18, e1003727. [Google Scholar] [CrossRef] [PubMed]
- Cairns, M.E.; Sagara, I.; Zongo, I.; Kuepfer, I.; Thera, I.; Nikiema, F.; Diarra, M.; Yerbanga, S.R.; Barry, A.; Tapily, A.; et al. Evaluation of seasonal malaria chemoprevention in two areas of intense seasonal malaria transmission: Secondary analysis of a household-randomised, placebo-controlled trial in Houndé District, Burkina Faso and Bougouni District, Mali. PLoS Med. 2020, 17, e1003214. [Google Scholar] [CrossRef] [PubMed]
- Coldiron, M.E.; Assao, B.; Guindo, O.; Sayinzoga-Makombe, N.; Koscalova, A.; Sterk, E.; Quere, M.; Ciglenecki, I.; Mumina, A.; Atti, S.; et al. Prevalence of malaria in an area receiving seasonal malaria chemoprevention in Niger. Malar. J. 2021, 20, 419. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.O.; Ceesay, F.K.; Obed, S.A.; Adjei, A.A.; Gyasi, R.K.; Rodney, P.; Ndjakani, Y.; Anderson, W.A.; Lucchi, N.W.; Stiles, J.K. Intermittent preventive treatment with sulfadoxine-pyrimethamine against malaria and anemia in pregnant women. Am. J. Trop. Med. Hyg. 2011, 85, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.L. A systematic review and meta-analysis of the efficacy and safety of intermittent preventive treatment of malaria in children (IPTc). PLoS ONE 2011, 6, e16976. [Google Scholar] [CrossRef] [PubMed]
- Maiga, H.; Barger, B.; Sagara, I.; Guindo, A.; Traore, O.B.; Tekete, M.; Dara, A.; Traore, Z.I.; Diarra, M.; Coumare, S.; et al. Impact of Three-Year Intermittent Preventive Treatment Using Artemisinin-Based Combination Therapies on Malaria Morbidity in Malian Schoolchildren. Trop. Med. Infect. Dis. 2020, 5, 148. [Google Scholar] [CrossRef] [PubMed]
- Maiga, H.; Gaudart, J.; Sagara, I.; Diarra, M.; Bamadio, A.; Djimde, M.; Coumare, S.; Sangare, B.; Dicko, Y.; Tembely, A.; et al. Two-Year Scale-Up of Seasonal Malaria Chemoprevention Reduced Malaria Morbidity among Children in the Health District of Koutiala, Mali. Int. J. Environ. Res. Public Health 2020, 17, 6639. [Google Scholar] [CrossRef] [PubMed]
- Diawara, F.; Steinhardt, L.C.; Mahamar, A.; Traore, T.; Kone, D.T.; Diawara, H.; Kamate, B.; Kone, D.; Diallo, M.; Sadou, A.; et al. Measuring the impact of seasonal malaria chemoprevention as part of routine malaria control in Kita, Mali. Malar. J. 2017, 16, 325. [Google Scholar] [CrossRef] [PubMed]
- Druetz, T.; Corneau-Tremblay, N.; Millogo, T.; Kouanda, S.; Ly, A.; Bicaba, A.; Haddad, S. Impact Evaluation of Seasonal Malaria Chemoprevention under Routine Program Implementation: A Quasi-Experimental Study in Burkina Faso. Am. J. Trop. Med. Hyg. 2018, 98, 524–533. [Google Scholar] [CrossRef]
- Issa, S.; Lamine, M.M.; Yerima, B.; Ibrahim, A.; Djakou, H.; Maman, L.I. Perception de la chimioprévention du paludisme saisonnier au Niger. Int. J. Biol. Chem. Sci. 2016, 10, 2710–2715. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Burkina Faso | Mali | Niger | |
|---|---|---|---|
| Proportion of total sample size% (n/N) | 38 (1183/3132) | 32 (1003/3132) | 30 (946/3132) |
| Age (years) | |||
| Mean (SD) | 31.10 (9.44) | 30/30.45 (8.54) | 30/31.68 (10.35) |
| Minimum-Maximum | 15–75 | 15–75 | 15–70 |
| Sex | |||
| Male n (%) | 191 (16.15) | 56 (5.58) | 63 (6.60) |
| Female n (%) | 992 (83.85) | 947 (94.42) | 883 (93.40) |
| Marital status | |||
| Married n (%) | 1164 (98.39) | 1000 (99.7) | 933 (98.5) |
| Single n (%) | 19 (1.61) | 3 (0.3) | 14 (1.5) |
| Education level | |||
| Illiterate n (%) | 924 (65.64) | 551 (54.94) | 362 (38.27) |
| Middle school n (%) | 31 (2.62) | 40 (3.99) | 148 (15.64) |
| Primary school n (%) | 109 (9.21) | 203 (20.24) | 181 (19.13) |
| Koranic school n (%) | 75 (6.34) | 84 (8.37) | 212 (22.41) |
| High school n (%) | 21 (1.78) | 40 (4) | 16 (1.69) |
| Literate n (%) | 112 (9.47) | 42 (4.19) | 12 (1.27) |
| University n (%) | 1 (0.08) | 18 (1.79) | 10 (1.06) |
| Others (pre-school, etc) | 6 (0.5) | 14 (1.40) | 5(0.53) |
| Relation of the respondent with the child | |||
| Father/mother n (%) | 1117 (94.42) | 971 (96.81) | 857 (90.59) |
| Grandparents n (%) | 40 (3.38) | 20 (2) | 71 (7.5) |
| Others (aunt, brother, sister, uncle) n (%) | 26 (2.20) | 12 (1.9) | 17 (1.80) |
| Knowledge of SMC | |||
| Yes n (%) | 1145 (96.79) | 968 (96.5) | 747 (78.96) |
| No n (%) | 38 (3.21) | 35 (3.5) | 199 (21.04) |
| Knowledge of SMC utility | |||
| Yes n (%) | 1096 (92.65) | 876 (87.34) | 811 (85.73) |
| No n (%) | 82 (6.93) | 113 (11.27) | 68 (7.20) |
| Do not know n (%) | 5 (0.42) | 14 (1.4) | 67 (7.08) |
| Use of bednets n (%) | |||
| Yes n (%) | 1076 (90.96) | 957 (95.41) | 907 (95.88) |
| No n (%) | 107 (9.04) | 46 (4.59) | 39 (4.12) |
| Knowledge of adverse events of SMC | |||
| Yes n (%) | 82 (6.93) | 116 (11.57) | 197 (20.82) |
| No n (%) | 1101 (93.07) | 887 (88.43) | 749 (79.17) |
| Do not know n (%) | 0 | 0 | 16 (1.59) |
| Knowledge of malaria causes | |||
| Yes (mosquitoes) n (%) | 1135 (95.94) | 896 (89.33) | 876 (92.6) |
| Inadequate (any other responses) n (%) | 43 (3.63) | 92 (9.17) | 54 (5.71) |
| Do not know n (%) | 3 (0.25) | 11 (1.1) | 4 (0.4) |
| Knowledge of death as consequences | |||
| Yes n (%) | 1161 (98.14) | 964 (96.11) | 930 (98.31) |
| No n (%) | 16 (1.35) | 29 (2.89) | 6 (0.6) |
| Do not know n (%) | 6 (0.51) | 10 (1) | 10 (1.06) |
| Country | Administration of Dose 2 | Administration of Dose 3 | Total | |
|---|---|---|---|---|
| Yes | No | |||
| Burkina Faso | Yes | 1131 | 2 | 1133 |
| No | 4 | 45 | 49 | |
| Mali | Yes | 945 | 0 | 945 |
| No | 0 | 56 | 56 | |
| Niger | Yes | 782 | 13 | 795 |
| No | 3 | 119 | 122 | |
| Total | 2865 | 235 | 3100 | |
| Burkina Faso | Mali | Niger | ||||
|---|---|---|---|---|---|---|
| Potentially Related to Children | 2nd Dose (N = 49) | 3rd Dose (N = 47) | 2nd Dose (N = 56) | 3rd Dose (N = 56) | 2nd Dose (N = 122) | 3rd Dose (N = 132) |
| Disease other than malaria n (%) | 14 (28.5) | 14 (29.78) | 3 (5.35) | 3 (5.35) | 2 (1.6) | 1 (0.75) |
| Vomiting n (%) | 6 (12.24) | 5 (10.63) | 0 | 0 | 3 (2.45) | 5 (3.78) |
| Refusal n (%) | 3 (6.12) | 2 (4.25) | 19 (33.9) | 9 (15.25) | 1(0.8) | 2 (1.51) |
| Potentially related to parents | ||||||
| Absence of parents n (%) | 14 (28.5) | 13 (27.65) | 9 (16.07) | 9 (16.07) | 9 (7.37) | 8 (6.06) |
| Travel n (%) | 6 (12.24) | 6 (12.76) | 11 ((19.64) | 11 (19.64) | 1 (0.81) | 1 (0.75) |
| Forgetting n (%) | 1 (2.04) | 2 (4.25) | 1 (1.78) | 1 (1.78) | 3(2.45) | 4 (3.03) |
| Child treated with antimalarial n (%) | 1 (2.04) | 0 | 0 | 0 | 0 | 1(0.75) |
| No trust in SMC drugs n (%) | 0 | 0 | 0 | 8 (14.28) | 1 (0.81) | 0 |
| Waiting for next disease episode n (%) | 0 | 0 | 1 (1.78) | 1 (1.78) | 0 | 0 |
| Problem with previous cycle n (%) | 0 | 1 | 0 | 0 | 1 (0.81) | 1 (0.75) |
| SMC card (lost, not received…) etc.) n (%) | 0 | 0 | 8 (14.28) | 0 | 0 | 1 (0.75) |
| Potentially related community distributors | ||||||
| Missing doses n (%) | 2 (4.08) | 2 (4.25) | 13 (23.21) | 13 (23.21) | 94 (77.04) | 101 (76.51) |
| Drugs out of stock n (%) | 2 (4.08) | 2 (4.25) | 0 | 0 | 0 | 0 |
| Not informed n (%) | 0 | 0 | 1 (1.78) | 1 (1.78) | 0 | 0 |
| Drug administration not explained n (%) | 0 | 0 | 0 | 0 | 1 (0.81) | 1 (0.75) |
| No Answer or no reason n (%) | 0 | 0 | 0 | 0 | 5 (4.10) | 1 (0.75) |
| Missing data n (%) | 0 | 0 | 0 | 0 | 1 (0.81) | 5 (3.78) |
| Total n (%) | 49 (100) | 47(100) | 56 (100) | 56 (100) | 122 (100) | 132 (100) |
| Burkina Faso | Mali | Niger | ||||
|---|---|---|---|---|---|---|
| Sex of Respondents | 2nd Dose (N = 49) | 3rd Dose (N = 47) | 2nd Dose (N = 56) | 3rd Dose (N = 56) | 2nd Dose (N = 122) | 3rd Dose (N = 132) |
| Female n (%) | 44 (89.8) | 41 (87.23) | 53 (94.65) | 53 (94.64) | 117 (95.90) | 123 (93.18) |
| Male n (%) | 5 (10.20) | 6 (12.77) | 3 (5.35) | 3 (5.36) | 5 (4.10) | 9 (6.82) |
| Marital status of respondents | ||||||
| Married n (%) | 47 (95.92) | 45 (95.74) | 56 (100) | 56 (100) | 119 (97.54) | 129 (97.73) |
| Single n (%) | 2 (4.08) | 2 (4.26) | 0 | 0 | 3 (2.46) | 3 (2.27) |
| Education level of respondents | ||||||
| Illiterate n (%) | 27 (55.10) | 33 (70.20) | 30 (53.57) | 30 (53.57) | 53 (43.44) | 59 (44.70) |
| Middle school n (%) | 1 (2.04) | 1 (2.13) | 0 | 1 (1.78) | 24 (19.67) | 27 (20.45) |
| Primary school n (%) | 3 (6.12) | 3 (6.38) | 18 (32.14) | 18 (32.14) | 24 (19.67) | 25 (18.94) |
| Koranic school n (%) | 1 (2.04) | 2 (4.26) | 4 (7.14) | 3 (5.36) | 17 (13.93) | 15 (11.36) |
| High school n (%) | 1 (2.04) | 1 (2.13) | 1 (1.78) | 1 (1.78) | 3 (2.46) | 4 (3.03) |
| Literate n (%) | 5 (10.20) | 6 (12.77) | 1 (1.78) | 1 (1.78) | 0 | 0 |
| University n (%) | 0 | 1 (2.13) | 2 (3.57) | 2 (3.57) | 1 (0.82) | 2 (1.51) |
| Relationship of respondents with the child | ||||||
| Father/mother n (%) | 45 (91.83) | 43 (91.49) | 55 (98.21) | 55 (98.22) | 117 (95.90) | 127 (96.21) |
| Grand-parents n (%) | 1 (2.04) | 1 (2.13) | 0 | 0 | 4 (3.28) | 4 (3.03) |
| Other (aunts, brothers …) n (%) | 3 (6.12) | 3 (6.38) | 1 (1.78) | 1 (1.78) | 1 (0.82) | 1 (0.76) |
| Aware of SMC program | ||||||
| Yes n (%) | 44 (89.8) | 41 (87.23) | 53 (94.65) | 53 (94.64) | 80 (65.58) | 87 (65.91) |
| No n (%) | 5 (10.20) | 5 (12.77) | 3 (5.35) | 3 (5.36) | 42 (34.42) | 45 (34.09) |
| knowledge of SMC utility | ||||||
| Protect against malaria n (%) | 41 (83.67) | 39 (82.98) | 46 (82.14) | 46 (82.14) | 93 (76.23) | 99 (75) |
| Do not know SMC utility n (%) | 8 (16.33) | 8 (17.02) | 10 (17.86) | 6 (10.72) | 16 (13.11) | 17 (12.88) |
| No response n (%) | 0 | 0 | 0 | 4 (7.14) | 13 (10.66) | 16 (12.12) |
| bed-nets use | ||||||
| Yes n (%) | 40 (81.63) | 38 (80.85) | 48 (85.71) | 48 (85.71) | 119 (97.54) | 129 (97.73) |
| No n (%) | 9 (18.37) | 9 (19.15) | 8 (14.29) | 8 (14.29) | 3 (2.46) | 3 (2.27) |
| Presence of adverse events after SMC | ||||||
| Yes n (%) | 10 (20.41) | 11 (22.44) | 0 | 5 (8.93) | 18 (14.75) | 22 (16.67) |
| No n (%) | 39 (79.59) | 36 (3.04) | 56 (100) | 51 (91.07) | 104 (85.25) | 110 (83.33) |
| Knowledge of malaria cause | ||||||
| Yes (mosquitoes) n (%) | 43 (87.75) | 41 (87.23) | 48 (85.71) | 47 (83.92) | 110 (90.16) | 120 (90.90) |
| Any response other than mosquitoes n (%) | 6 (12.25) | 6 (12.77) | 6 (10.72) | 7 (12.50) | 11 (9.02) | 11 (18.34) |
| Do not know n (%) | 0 | 0 | 2 (3.57) | 2 (3.58) | 1 (0.82) | 1 (0.76) |
| Knowledge of malaria consequences | ||||||
| Yes n (%) | 47 (95.92) | 45 (95.74) | 55 (98.21) | 55 (98.22) | 121 (99.18) | 129 (97.73) |
| No n (%) | 2 (4.08) | 2(4.26) | 1 (1.79) | 1 (1.78) | 1 (0.82) | 1 (0.76) |
| Do not know n (%) | 0 | 0 | 0 | 0 | 0 | 2 (1.51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somé, A.F.; Zongo, I.; Sagara, I.; Ibrahim, A.; Ahanhanzo, C.D.; Agbanouvi-agassi, E.E.; Sayi, D.A.; Toe, L.P.; Kabré, Z.; Nikiéma, F.; et al. Factors Influencing Second and Third Dose Observance during Seasonal Malaria Chemoprevention (SMC): A Quantitative Study in Burkina Faso, Mali and Niger. Trop. Med. Infect. Dis. 2022, 7, 214. https://doi.org/10.3390/tropicalmed7090214
Somé AF, Zongo I, Sagara I, Ibrahim A, Ahanhanzo CD, Agbanouvi-agassi EE, Sayi DA, Toe LP, Kabré Z, Nikiéma F, et al. Factors Influencing Second and Third Dose Observance during Seasonal Malaria Chemoprevention (SMC): A Quantitative Study in Burkina Faso, Mali and Niger. Tropical Medicine and Infectious Disease. 2022; 7(9):214. https://doi.org/10.3390/tropicalmed7090214
Chicago/Turabian StyleSomé, Anyirékun Fabrice, Issaka Zongo, Issaka Sagara, Alkassoum Ibrahim, Césaire Damien Ahanhanzo, Edoh Eddie Agbanouvi-agassi, Dona Alain Sayi, Lea Pare Toe, Zachari Kabré, Frédéric Nikiéma, and et al. 2022. "Factors Influencing Second and Third Dose Observance during Seasonal Malaria Chemoprevention (SMC): A Quantitative Study in Burkina Faso, Mali and Niger" Tropical Medicine and Infectious Disease 7, no. 9: 214. https://doi.org/10.3390/tropicalmed7090214
APA StyleSomé, A. F., Zongo, I., Sagara, I., Ibrahim, A., Ahanhanzo, C. D., Agbanouvi-agassi, E. E., Sayi, D. A., Toe, L. P., Kabré, Z., Nikiéma, F., Bazié, T., Ouédraogo, S., Sombié, I., Dicko, A., Adehossi, E., Ouédraogo, J.-B., & Dabiré, K. R. (2022). Factors Influencing Second and Third Dose Observance during Seasonal Malaria Chemoprevention (SMC): A Quantitative Study in Burkina Faso, Mali and Niger. Tropical Medicine and Infectious Disease, 7(9), 214. https://doi.org/10.3390/tropicalmed7090214