Abstract
Myocarditis represents a potential complication of various infectious and noninfectious agents and a common diagnostic challenge for clinicians. Data regarding Campylobacter-associated myocarditis are limited. Here, a case of a 13-year-old female with Campylobacter jejuni gastroenteritis complicated by myocarditis is presented, followed by a literature review in order to retrieve information about Campylobacter-associated carditis in the pediatric population. A search on MEDLINE/PubMed yielded 7relevant cases in the last 20 years. Most of them (six/seven) were males and the mean age was 16.1 years. All patients presented with gastrointestinal symptoms followed in six/seven cases by chest pain within two to seven days. Campylobacter was isolated from stool cultures in six patients; abnormal electrocardiographic findings were detected in six; and abnormal echocardiographic findings in three of the cases. Five patients were treated with antibiotics. Full recovery was the clinical outcome in six patients, whereas one patient died. Concerning the nonspecific symptoms of patients with myocarditis, high clinical suspicion of this complication is necessary in cases where patients with a recent infection present with chest pain and elevated cardiac biomarkers.
1. Introduction
Myocarditis is defined as the inflammation of the heart muscle and represents a potential complication of various infectious and noninfectious agents. Recently, the development of sensitive diagnostic tests, such as polymerase chain reaction (PCR) assays, led to the isolation of responsible pathogens; viral causes continue to be the most prevalent among all causes [1]. Bacterial infections are a rare cause of myocarditis, with gastrointestinal pathogens including Salmonella spp. and Shigella spp. being commonly reported. A few cases of myocarditis as a complication of Campylobacter jejuni infection have been reported in adults thus far [2].
Here, we present a case of a healthy female adolescent who was diagnosed with C. jejuni-associated myocarditis. We also present the results of a literature review regarding Campylobacter-associated carditis in the pediatric population (<18 years old).
2. Case Report
A 13-year-old previously healthy and fully vaccinated female was admitted to the Emergency Department (ED) of “Aghia Sophia” Children’s Hospital of Athens in July. She complained of fever (Tmax = 38.5 °C), intermittent diffuse abdominal pain, and non-bloody diarrhea for the last two days. She also reported headaches and nuchal ache during active movement. A few days before the onset of diarrhea, she had eaten poultry in a local restaurant. There were no other family members with gastrointestinal symptoms. On examination, the patient was in good general condition, afebrile (T = 37.2 °C), with BP = 118/62 mmHg, HR = 123 bpm, RR = 18/min, and SpO2 = 98% on room air. There were no signs of nuchal rigidity, photophobia, and pupils were equal and reactive. Lungs were clear to auscultation, cardiac auscultation revealed normal S1, S2 with no murmurs, gallops, or pericardial friction rub, and distal pulses were symmetrical and equal. Abdominal examination revealed diffuse tenderness upon deep palpation with no signs of guarding. The review of the other systems was grossly normal. The patient was admitted to the General Pediatric Ward with the working differential diagnosis of infectious enteritis and acute appendicitis; patient’s neurological examination was normal, Kernig’s and Brudzinski’s signs were negative, and therefore meningitis was low in our differential diagnosis list. Surgical consultation was requested, which did not show any signs of acute abdomen, no evident signs of appendicitis, with McBurney’s sign being negative.
Initial laboratory investigations revealed normal complete blood count, electrolytes, renal, and liver function tests, whereas serum C-reactive protein value was elevated at 25 mg/dL (reference <0.5 mg/dL). Urinalysis was normal whereas blood, urine, and stool cultures were sent.
Upon admission, the patient received intravenous maintenance fluids and remained in good general condition. During the second day of hospitalization, she had three episodes of fever (Tmax = 38.2 °C) and started to complain about stabbing, intermittent pain at the anterior chest, without radiation. There were no alleviating or aggravating factors. Her physical examination was unremarkable. Laboratory investigation including cardiac biomarkers were sent and showed elevated total Creatine Kinase (CK) (307 IU/L; reference range <140), CK-MB (25.3 ng/mL; reference <3), and Τroponin-T (456.4 pg/mL; reference< 14) levels (Table 1). An electrocardiogram (ECG) was performed that showed sinus rhythm, normal ST-segments, and normal T waves (Figure 1). Due to persisting chest pain and due to the abnormal cardiac biomarkers, a cardiological consultation was requested. Cardiac echocardiography was performed that showed normal left ventricular (LV) function, with a >65% ejection fraction and no pericardial effusion (Figure 2).

Table 1.
Laboratory parameters and cardiological tests.
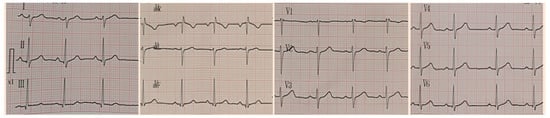
Figure 1.
ECG on Day 2.
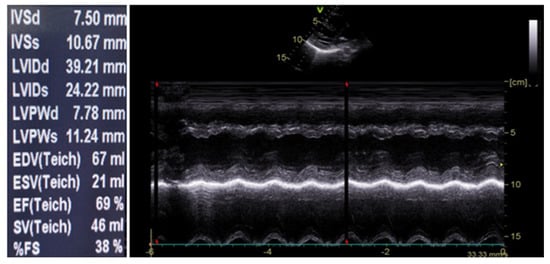
Figure 2.
Cardiac echocardiography on Day 2.
An extensive laboratory and microbiological evaluation on a working diagnosis of acute myocarditis were performed. A rapid multiplex PCR stool analysis using the BioFire® FilmArray® Gastrointestinal (GI) panel was sent identifying Campylobacter spp. Subsequently, further laboratory evaluation for common cardiotropic infectious causes was negative (Table 2). Therefore, with the diagnosis of suspected/potential acute myocarditis associated with Campylobacter spp. enterocolitis the patient was treated with a five-day antibiotic course of azithromycin (initial dose of 10 mg/kg followed by 5 mg/kg once daily for 4 days), and antiarrhythmic medication of carvedilol (0.05 mg/kg BD) and captopril (6.25 mg BD). Immunomodulatory or immunosuppressive therapies, including corticosteroids, intravenous immunoglobulin (IVIG), azathioprine, and cyclosporine reported in the literature [1] were not part of our therapeutic approach for our patient. Later on during hospitalization, fecal cultures were negative for common bacterial and viral agents, whereas Campylobacter jejuni was isolated which was resistant to fluoroquinolones and sensitive to macrolides and tetracyclines. Blood cultures were negative.
Table 2.
Microbiological tests.
During hospitalization, the patient remained in good general condition and was hemodynamically stable. In order to closely monitor her cardiovascular status, repeated electrocardiographic and echocardiographic evaluations, as well as a continuous 24 h cardiac rhythm Holter monitoring, were performed (all of which were normal). She remained afebrile and diarrhea stopped during the third day of hospitalization. Chest pain resolved by the fourth in-hospital day. Regarding her laboratory tests, CK value peaked at 643 IU/L, CK-MB to 51.6 ng/mL, Troponin-T to 872.2 ng/mL, N-terminal-proBNP to 715 pg/mL, AST to 64 IU/L and C-reactive protein to 48 mg/L. The patient was discharged in a good clinical condition after eight days of hospitalization with a follow-up appointment in order to have cardiac magnetic resonance imaging (CMR) and cardiologic evaluation.
On the follow-up appointment, one month after discharge, patient’s electrocardiographic and echocardiographic evaluations as well as serum cardiac biomarkers were normal. Additionally, the CMR findings did not demonstrate any markers of myocardial inflammation and necrosis (Figure 3). The Luise Lake Criteria for acute myocarditis were not fulfilled by that time as no high signal intensity on T2-weighted imaging, increased T2 and T1 times, myocardial thickening, or rapid uptake (early gadolinium enhancement) of contrast were revealed [3]. Subsequently, antiarrythmic medication was discontinued.
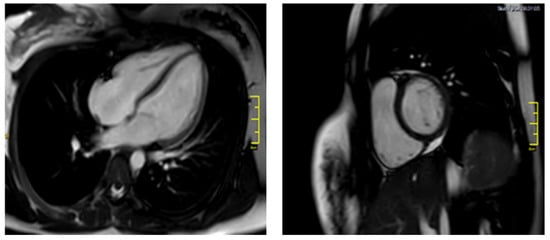
Figure 3.
Follow-up CMR.
3. Discussion and Literature Review
In this case report, we present a previously healthy young female patient, who was admitted with gastroenteritis symptoms and within 24 h from admission developed chest pain. Based on the clinical symptoms, elevated cardiac biomarkers, the isolation of Campylobacter jejuni from both stool culture and PCR array, as well as the lack of potential alternative diagnosis, she was diagnosed with suspected/potential Campylobacter jejuni–associated myocarditis in accordance with AHA statement [1]. Our patient represents the third case of C. jejuni-associated myocarditis and the second female case reported in the literature. Importantly, both electrocardiographic and echocardiographic findings of our patient were normal, the patient remained in good clinical condition and full recovery was the clinical outcome. The cardiological follow-up evaluation one month later was also normal.
A search on MEDLINE/PubMed using multiple combinations of MESH-terms “Campylobacter”, “Campylobacter jejuni”. “myocarditis”, “myopericarditis”, and “pericarditis” yielded seven relevant cases during the last 20 years in the pediatric population (<18 years old). Specifically, four cases of myopericarditis [4,5,6], two cases of myocarditis [7,8], and one case of pericarditis [9] associated with Campylobacter spp. infection have been described. Patients’ clinical characteristics are provided in Table 3.
Table 3.
Summary of the cases reported in the literature.
Regarding the characteristics of the patients included in this review, most of them were males (six/seven patients) and the mean age was 16.1 years. Past medical history of the patients was as follows; one patient had β-thalassemia [9], one patient had a previous episode of myopericarditis three years before the current episode [4], one patient suffered from bronchial asthma [8], whereas no comorbidities were reported for the rest of the patients.
All patients presented with early onset gastrointestinal tract symptoms followed by clinical symptoms of carditis within two to seven days. Chest pain was the main complaint of carditis in the patients described, whereas only one [9] did not have any cardiac symptoms. Laboratory tests demonstrated the release of cardio-specific enzymes (CK, CK-MB, Troponin T/I) in all patients (n = 6) tested for cardiac biomarkers [4,5,6,7,8].
Electrocardiographic and echocardiographic evaluation were performed in six out of seven patients as long as cardiac symptoms were present [4,5,6,8,9]. Abnormal ECG findings were detected in 6 [4,5,6,8,9]. Specifically, isolated ST-segment elevations [4,5,8,9] or combined with T waves inversions [6] were commonly reported. Abnormal echocardiographic findings were present in three patients, including impaired left ventricular function (reduced ejection fraction) in two of them [4,5], and large pericardial effusion in the third one [9]. One patient [6] had normal transthoracic echocardiography. In two cases [5,6] myocardial damage was detected in a CMR conducted early after the onset of cardiac symptoms, confirming the diagnosis. Despite the fact that endomyocardial biopsy (EMB) is the gold standard to prove the diagnosis of myocarditis [1], it was used only in one case report [7] as part of the autopsy. Low sensitivity due to sampling error, variability in pathologic interpretation, and potential complications such as myocardial perforation and tamponade are reasons for its reduced use [3].
The diagnosis of Campylobacter infection was based on the isolation of the microbe from stool cultures in all patients, except for one where Campylobacter was isolated from the pericardial fluid [9]. In six of the cases stool isolate was Campylobacter jejuni, whereas Campylobacter fetus was detected in one case [9].
Antibiotics were part of the therapeutic approach in five out of the seven patients in this review [4,5,6,9]. Concerning clinical outcomes, six patients fully recovered [4,5,6,8,9], whereas one death was recorded [7].
Acute myocarditis represents a potentially life-threatening diagnosis and a common diagnostic challenge for clinicians due to the non-specific nature of presenting symptoms such as chest pain and fever. Recently, the American Heart Association published a scientific statement concerning the diagnosis, etiological factors, and management of myocarditis in children. Among commonly isolated pathogens, viral infections appear the most prevalent, including Enteroviruses (Coxsackie A and B, Echoviruses), Epstein–Barr virus (EBV), Cytomegalovirus (CMV), Human Herpes Virus 6 (HHV6), Adenoviruses, Influenza A and B, Parvovirus B19, and Hepatitis B and C. Additionally, bacterial and fungal agents, as well as immunοlogical and pharmaceutical agents are also reported as less common factors to cause myocarditis [1]. Of note, in this statement Campylobacter is not described as a potential etiological factor.
Campylobacter infections represent a common cause of gastroenteritis in children worldwide, and Campylobacter jejuni is the most commonly isolated Campylobacter spp. Typically, symptoms are relatively mild and Campylobacter gastroenteritis is usually self-limited. However, multiple acute and late complications including cholecystitis, reactive arthritis, Guillain-Barre syndrome (GBS), and rarely myocarditis and pericarditis have been reported in the literature [10,11,12,13,14]. The exact pathogenetic mechanism responsible for cardiac inflammation remains uncertain; potential mechanisms include—but are not limited to—direct bacterial invasion of cardiac tissue, the release of bacterial toxins, circulating immune complexes, and cytotoxic T-cells [15].
The results of this literature review highlight that Campylobacter-related cardiac complications predominately affect male adolescents, which is in line with the current reported literature regarding acute myo(peri)carditis in the pediatric population [16]. Importantly, most of the cases responded well to antibiotic and supportive treatment, following a benign course. Regarding initial clinical presentation, all patients presented with early gastrointestinal symptoms, followed by clinical symptoms of carditis within the next few days. Cardio-specific biomarkers were typically elevated, while electrocardiographic and echocardiographic changes were present in the majority of cases. These findings are more specific and contribute in clinical practice to the diagnosis. Of note, in two casesCMR was performed confirming the diagnosis of acute myocarditis [5,6].
In summary, this case highlights a patient with Campylobacter jejuni gastroenteritis that was subsequently complicated by clinical and laboratory manifestations of myocarditis. Therefore, high clinical suspicion of myocarditis is necessary in patients with a recent infection that present with chest pain and elevated cardiac biomarkers.
Author Contributions
Conceptualization: A.-P.C., S.K., C.K.-G. and E.B.; methodology: A.-P.C., S.K. and P.P.; data acquisition: A.-P.C., S.K., P.P., E.G., T.C., K.S. and G.P.; writing—original draft preparation: A.-P.C., S.K.; writing—review and editing, all authors; supervision: C.K.-G., E.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Law, Y.M.; Lal, A.K.; Chen, S.; Čiháková, D.; Cooper, L.T.; Deshpande, S.; Godown, J.; Grosse-Wortmann, L.; Robinson, J.D.; Towbin, J.A.; et al. Diagnosis and Management of Myocarditis in Children: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e123–e135. [Google Scholar] [CrossRef] [PubMed]
- Hessulf, F.; Ljungberg, J.; Johansson, P.-A.; Lindgren, M.; Engdahl, J. Campylobacter jejuni-associated perimyocarditis: Two case reports and review of the literature. BMC Infect. Dis. 2016, 16, 289. [Google Scholar] [CrossRef] [PubMed]
- Putschoegl, A.; Auerbach, S. Diagnosis, Evaluation, and Treatment of Myocarditis in Children. Pediatric Clin. N. Am. 2020, 67, 855–874. [Google Scholar] [CrossRef] [PubMed]
- Dind, A.; Whalley, D. Recurrence of myopericarditis triggered by Campylobacter jejuni. Intern. Med. J. 2019, 49, 409–411. [Google Scholar] [CrossRef] [PubMed]
- Heinzl, B.; Köstenberger, M.; Nagel, B.; Sorantin, E.; Beitzke, A.; Gamillscheg, A. Campylobacter jejuni infection associated with myopericarditis in adolescents: Report of two cases. Eur. J. Pediatr. 2010, 169, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Fica, A.; Seelmann, D.; Porte, L.; Eugenin, D.; Gallardo, R. A case of myopericarditis associated to Campylobacter jejuni infection in the southern hemisphere. Braz. J. Infect. Dis. 2012, 16, 294–296. [Google Scholar] [CrossRef][Green Version]
- Pena, L.A.; Fishbein, M.C. Fatal myocarditis related to Campylobacter jejuni infection: A case report. Cardiovasc. Pathol. 2007, 16, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Yaita, S.; Tago, M.; Hisata, Y.; Fujiwara, M.; Yamashita, S. Relapse of acute myocarditis associated with Campylobacter jejuni enterocolitis. Clin. Case Rep. 2020, 8, 2605–2609. [Google Scholar] [CrossRef] [PubMed]
- Kanj, S.S.; Araj, G.F.; Taher, A.; Reller, L.B. Campylobacter fetus pericarditis in a patient with β-thalassemia: Case report and review of the literature. Clin. Microbiol. Infect. 2001, 7, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, C. Campylobacter. Clin. Lab. Med. 2015, 35, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Same, R.G.; Tamma, P.D. Campylobacter Infections in Children. Pediatrics Rev. 2018, 39, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Vaughan-Shaw, P.G.; Rees, J.R.; White, D.; Burgess, P. Campylobacter jejuni cholecystitis: A rare but significant clinical entity. Case Rep. 2010, 2010, bcr1020092365. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.E.; Krizova, A.; Garg, A.X.; Thiessen-Philbrook, H.; Ouimet, J.M. Campylobacter Reactive Arthritis: A Systematic Review. Semin. Arthritis Rheum. 2007, 37, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Nachamkin, I.; Allos, B.M.; Ho, T. Campylobacter Species and Guillain-Barré Syndrome. Clin. Microbiol. Rev. 1998, 11, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Veerasamy, M.; Alguire, C.T. Food finds its way to a woman’s heart: Campylobacter jejuni-associated myopericarditis. Glob. Cardiol. Sci. Pract. 2017, 2017, e201708. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sharma, J.; Fernandes, N.; Alvarez, D.; Khanna, S. Acute Myopericarditis in an Adolescent Mimicking Acute Myocardial Infarction. Pediatric Emerg. Care 2015, 31, 427–430. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).