

The Impact of a Multidimensional Physical Activity Intervention on Glycemic Control in Type 1 Diabetes: A Preliminary Study

 , ,
, ,  ,
, 
 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Description
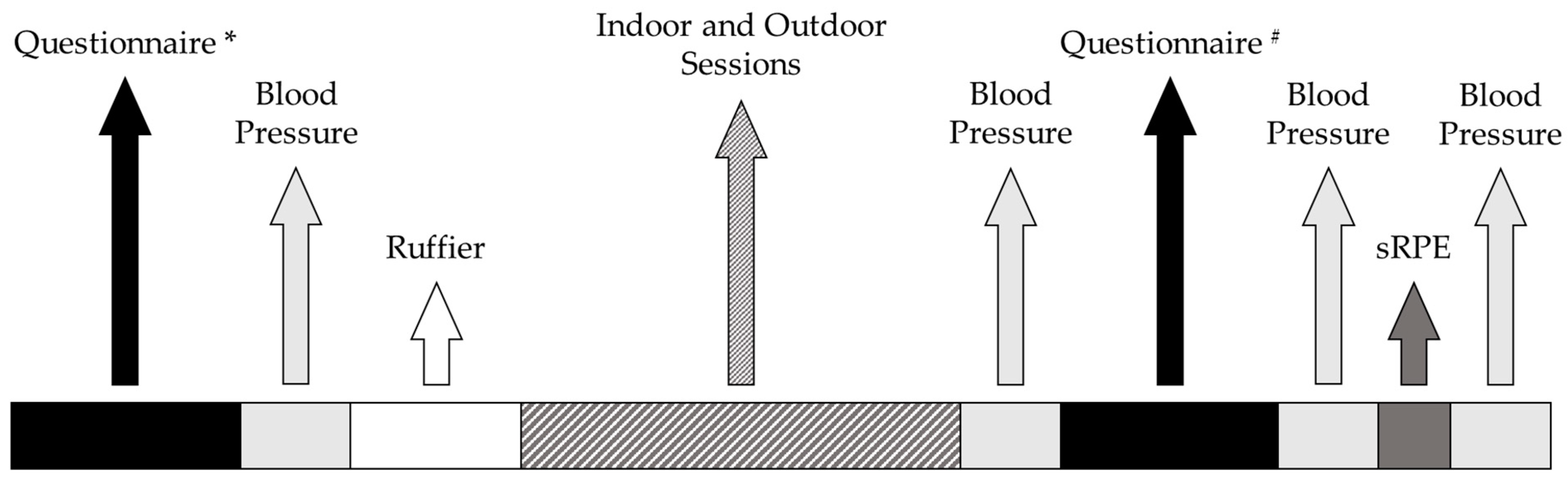
2.2. Procedures
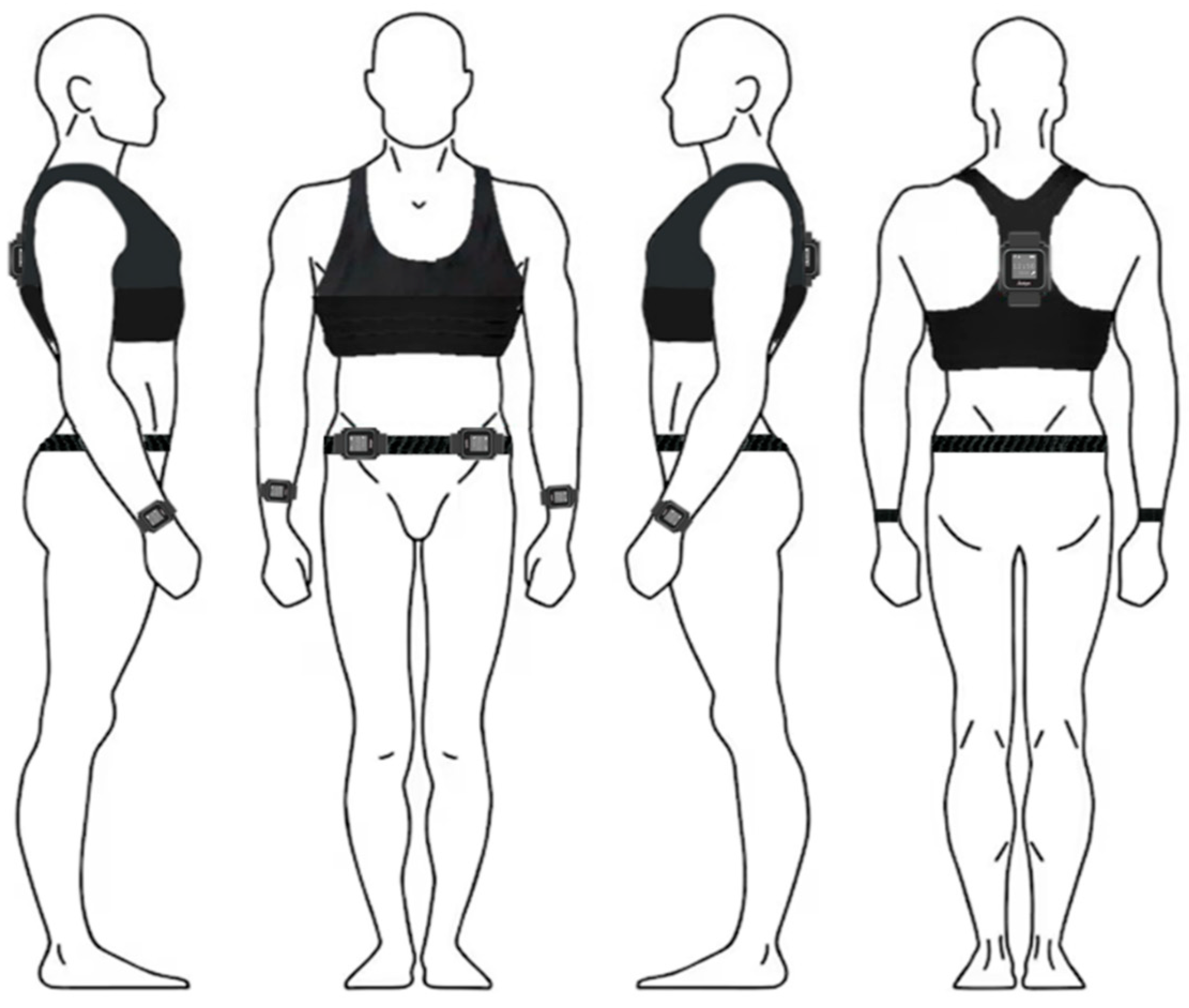
2.2.1. Measurements
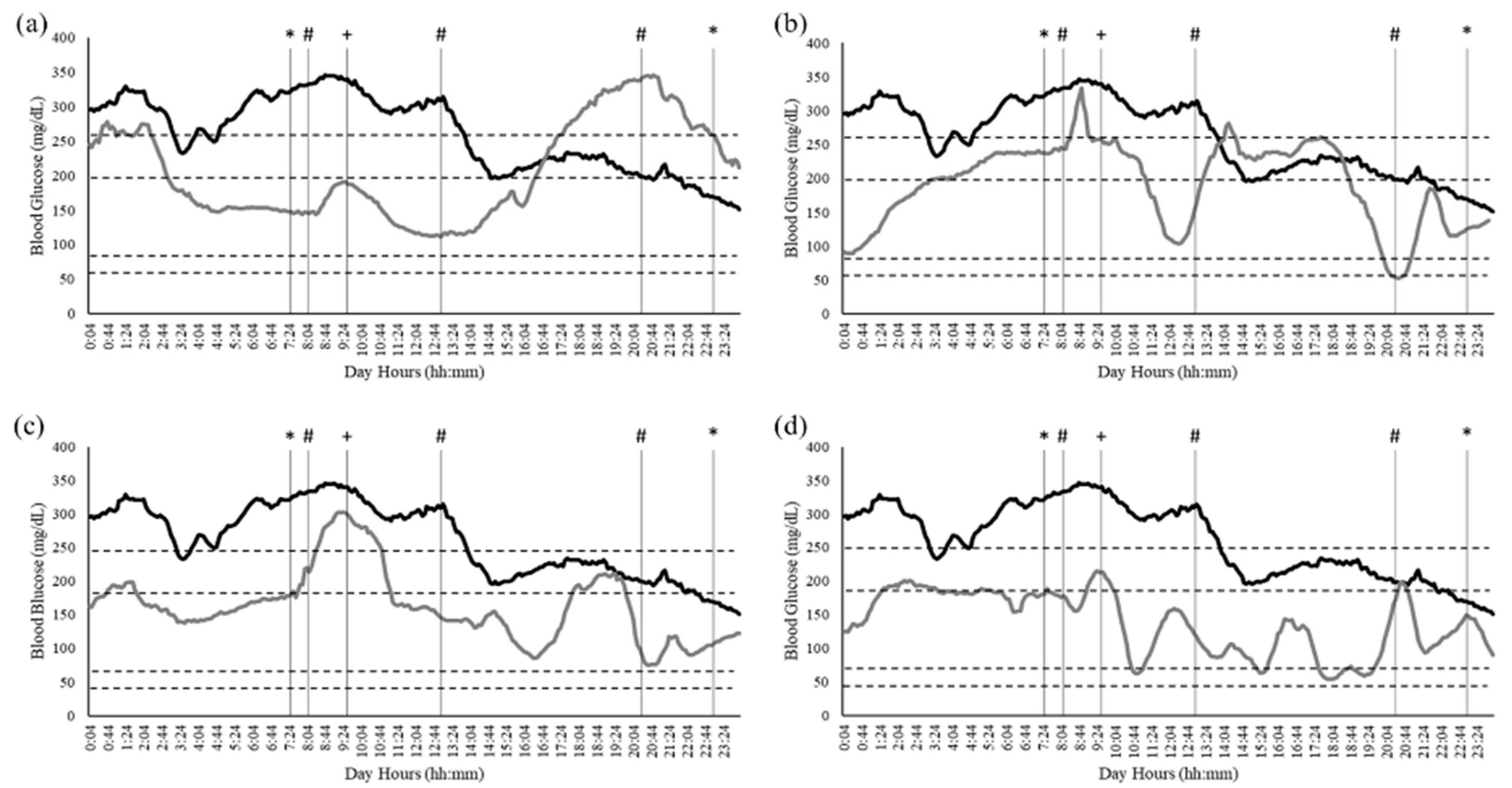
2.2.2. Data Extraction and Analysis
- >250 mg/dL: Very high;
- 181–250 mg/dL: High;
- 180–70 mg/dL: Normal or Target;
- 54–69 mg/dL: Low;
- <54 mg/dL: Very low.
- if VMU Counts per Minute were >2453
- if VMU Counts per Minute were ≤2453
3. Results
4. Discussion
Limitations and Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HIIT | High-Intensity Interval Training |
| WHR | Waist-to-Hip Ratio |
| RPE | Rate of Perceived Exertion |
| PREDIMED | PREvención con Dieta MEDiterránea |
| PSQI | Pittsburgh Sleep Quality Index |
| IPAQ | International Physical Activity Questionnaire |
| MeQ | Morningness–Eveningness Questionnaire |
| sRPE | Session Rate of Perceived Exertion |
| VO2 | Oxygen Uptake |
| CAI | Club Alpino Italiano |
| RER | Respiratory Exchange Ratio |
| VE | Minute Ventilation |
| MET | Metabolic Equivalent Task |
| PACES | Physical Activity Enjoyment Scale |
| HbA1c | Glycated hemoglobin |
References
- Georgoulis, M.; Kontogianni, M.; Yiannakouris, N. Mediterranean Diet and Diabetes: Prevention and Treatment. Nutrients 2014, 6, 1406–1423. [Google Scholar] [CrossRef] [PubMed]
- Petersmann, A.; Müller-Wieland, D.; Müller, U.A.; Landgraf, R.; Nauck, M.; Freckmann, G.; Heinemann, L.; Schleicher, E. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2019, 127, S1–S7. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; Dragomir, M.; Autier, P.; Boyle, P. Physical Activity and Change in Fasting Glucose and HbA1c: A Quantitative Meta-Analysis of Randomized Trials. Acta Diabetol. 2017, 54, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Ruderman, N.; Campaigne, B.N.; Devlin, J.T.; Schneider, S.H. Physical Activity/Exercise and Diabetes Mellitus. Diabetes Care 2003, 26, S73. [Google Scholar] [CrossRef]
- Marcovecchio, M.L. Complications of Acute and Chronic Hyperglycemia. US Endocrinol. 2017, 13, 17–21. [Google Scholar] [CrossRef]
- Ding, S.; Schumacher, M. Sensor Monitoring of Physical Activity to Improve Glucose Management in Diabetic Patients: A Review. Sensors 2016, 16, 589. [Google Scholar] [CrossRef]
- American Diabetes Association. Check Your Blood Glucose|Diabetes Testing & Monitoring. Available online: https://diabetes.org/living-with-diabetes/treatment-care/checking-your-blood-sugar (accessed on 27 January 2025).
- Byberg, S.; Hansen, A.L.S.; Christensen, D.L.; Vistisen, D.; Aadahl, M.; Linneberg, A.; Witte, D.R. Sleep Duration and Sleep Quality Are Associated Differently with Alterations of Glucose Homeostasis. Diabet. Med. 2012, 29, 354–360. [Google Scholar] [CrossRef]
- Vasto, S.; Amato, A.; Proia, P.; Baldassano, S. Is the Secret in the Gut? SuperJump Activity Improves Bone Remodeling and Glucose Homeostasis by GLP-1 and GIP Peptides in Eumenorrheic Women. Biology 2022, 11, 296. [Google Scholar] [CrossRef]
- Larcher, S.; Benhamou, P.-Y.; Pépin, J.-L.; Borel, A.-L. Sleep Habits and Diabetes. Diabetes Metab. 2015, 41, 263–271. [Google Scholar] [CrossRef]
- Tan, X.; Chapman, C.D.; Cedernaes, J.; Benedict, C. Association between Long Sleep Duration and Increased Risk of Obesity and Type 2 Diabetes: A Review of Possible Mechanisms. Sleep Med. Rev. 2018, 40, 127–134. [Google Scholar] [CrossRef]
- Rutters, F.; Nefs, G. Sleep and Circadian Rhythm Disturbances in Diabetes: A Narrative Review. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 3627–3637. [Google Scholar] [CrossRef] [PubMed]
- Purwono, J.; Fitri, N.L.; Hasanah, U.; Ayubbana, S. Effects of Sleep Quality Towards Blood Glucose Levels As At Type Ii Diabetes Mellitus Patients. Syst. Rev. Pharm. 2020, 11, 223. [Google Scholar]
- Kalmbach, D.A.; Schneider, L.D.; Cheung, J.; Bertrand, S.J.; Kariharan, T.; Pack, A.I.; Gehrman, P.R. Genetic Basis of Chronotype in Humans: Insights from Three Landmark Gwas. Sleep 2017, 40, zsw048. [Google Scholar] [CrossRef]
- Carvalho-Mendes, R.P.; Menna-Barreto, L. Why Should Chronobiology Be Included in Teachers’ Training? Pro-Posições 2022, 33, e20210030. [Google Scholar] [CrossRef]
- Reutrakul, S.; Hood, M.M.; Crowley, S.J.; Morgan, M.K.; Teodori, M.; Knutson, K.L.; Van Cauter, E. Chronotype Is Independently Associated with Glycemic Control in Type 2 Diabetes. Diabetes Care 2013, 36, 2523–2529. [Google Scholar] [CrossRef]
- Russell, W.R.; Baka, A.; Björck, I.; Delzenne, N.; Gao, D.; Griffiths, H.R.; Hadjilucas, E.; Juvonen, K.; Lahtinen, S.; Lansink, M.; et al. Impact of Diet Composition on Blood Glucose Regulation. Crit. Rev. Food Sci. Nutr. 2016, 56, 541–590. [Google Scholar] [CrossRef] [PubMed]
- Lamonte, M.J.; Blair, S.N.; Church, T.S. Physical Activity and Diabetes Prevention. J. Appl. Physiol. 2005, 99, 1205–1213. [Google Scholar] [CrossRef]
- American Diabetes Association. Physical Activity/Exercise and Diabetes. Diabetes Care 2004, 27, s58–s62. [Google Scholar] [CrossRef]
- Sigal, R.J.; Armstrong, M.J.; Bacon, S.L.; Boulé, N.G.; Dasgupta, K.; Kenny, G.P.; Riddell, M.C. Physical Activity and Diabetes. Can. J. Diabetes 2018, 42, S54–S63. [Google Scholar] [CrossRef]
- Papale, O.; Festino, E.; Condello, G.; Di Rocco, F.; De Maio, M.; Cortis, C.; Fusco, A. Psychophysiological Data Harmonization for the Sustainability of Outdoor Activities. Sustainability 2023, 15, 15838. [Google Scholar] [CrossRef]
- Adams, P. The Impact of Brief High-Intensity Exercise on Blood Glucose Levels. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 113–122. [Google Scholar] [CrossRef]
- Smutok, M.; Reece, C.; Kokkinos, P.; Farmer, C.; Dawson, P.; De Vane, J.; Patterson, J.; Goldberg, A.; Hurley, B. Effects of Exercise Training Modality on Glucose Tolerance in Men with Abnormal Glucose Regulation. Int. J. Sports Med. 1994, 15, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, G.S.; Skeva, I.I.; Zourbaki, A.S.; Mountokalakis, T.D. Self-Monitoring of Blood Pressure at Home: How Many Measurements Are Needed? J. Hypertens. 1998, 16, 725–731. [Google Scholar] [CrossRef] [PubMed]
- de Camarda, S.R.A.; Tebexreni, A.S.; Páfaro, C.N.; Sasai, F.B.; Tambeiro, V.L.; Juliano, Y.; de Barros Neto, T.L. Comparison of Maximal Heart Rate Using the Prediction Equations Proposed by Karvonen and Tanaka. Arq. Bras. Cardiol. 2008, 91, 311–314. [Google Scholar] [CrossRef]
- Sampath Kumar, A.; Arun Maiya, G.; Shastry, B.A.; Vaishali, K.; Maiya, S.; Umakanth, S. Correlation between Basal Metabolic Rate, Visceral Fat and Insulin Resistance among Type 2 Diabetes Mellitus with Peripheral Neuropathy. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Foster, C.; Anholm, J.D.; Bok, D.; Boullosa, D.; Condello, G.; Cortis, C.; Fusco, A.; Jaime, S.J.; de Koning, J.J.; Lucia, A.; et al. Generalized Approach to Translating Exercise Tests and Prescribing Exercise. J. Funct. Morphol. Kinesiol. 2020, 5, 63. [Google Scholar] [CrossRef]
- Foster, C.; Walraven, L.; Bok, D.; Barroso, R.; Boullosa, D.; Casado, A.; Cortis, C.; de Koning, J.J.; Festino, E.; Fusco, A.; et al. Physiological Drift during Steady-State Exercise Based on the Incremental Talk Test. Hum. Mov. 2025, 26, 71–80. [Google Scholar] [CrossRef]
- Wetten, A.A.; Batterham, M.; Tan, S.Y.; Tapsell, L. Relative Validity of 3 Accelerometer Models for Estimating Energy Expenditure During Light Activity. J. Phys. Act. Health 2014, 11, 638–647. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. Accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Reutrakul, S.; Thakkinstian, A.; Anothaisintawee, T.; Chontong, S.; Borel, A.-L.; Perfect, M.M.; Janovsky, C.C.P.S.; Kessler, R.; Schultes, B.; Harsch, I.A.; et al. Sleep Characteristics in Type 1 Diabetes and Associations with Glycemic Control: Systematic Review and Meta-Analysis. Sleep Med. 2016, 23, 26–45. [Google Scholar] [CrossRef]
- Di Credico, A.; Perpetuini, D.; Chiacchiaretta, P.; Cardone, D.; Filippini, C.; Gaggi, G.; Merla, A.; Ghinassi, B.; Di Baldassarre, A.; Izzicupo, P. The Prediction of Running Velocity during the 30–15 Intermittent Fitness Test Using Accelerometry-Derived Metrics and Physiological Parameters: A Machine Learning Approach. Int. J. Environ. Res. Public Health 2021, 18, 10854. [Google Scholar] [CrossRef]
- Halliwill, J.R. Mechanisms and Clinical Implications of Post-Exercise Hypotension in Humans. Exerc. Sport Sci. Rev. 2001, 29, 65–70. [Google Scholar] [CrossRef]
- Ayán Pérez, C.; Reigosa Galáns, F.; Cancela Carral, J.M.; Rodríguez Barreiro, H.; Martínez-Lemos, I. Test-Retest Reliability and Convergent Validity of the Ruffier Index in Children under 12 Years Old. Sci. Sports 2018, 33, 353–360. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.M.; Lentjes, M.A.H.; Luben, R.N.; Khaw, K.T.; Wareham, N.J.; Forouhi, N.G. Dietary Dairy Product Intake and Incident Type 2 Diabetes: A Prospective Study Using Dietary Data from a 7-Day Food Diary. Diabetologia 2014, 57, 909–917. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D. The Pittsburgh Sleep Quality Index (PSQI): A New Instrument for Psychiatric Research and Practice. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Horne, J.A.; Ostberg, O. A Self-Assessment Questionnaire to Determine Morningness-Eveningness in Human Circadian Rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Mannocci, A.; Di Thiene, D.; Del Cimmuto, A.; Masala, D.; Boccia, A.; De Vito, E.; La Torre, G. International Physical Activity Questionnaire: Validation and Assessment in an Italian Sample. Ital. J. Public Health 2010, 7, 369–376. [Google Scholar] [CrossRef]
- Festino, E.; Papale, O.; Di Rocco, F.; De Maio, M.; Cortis, C.; Fusco, A. Effect of Physical Activity Behaviors, Team Sports, and Sitting Time on Body Image and Exercise Dependence. Sports 2024, 12, 260. [Google Scholar] [CrossRef]
- Chen, C.; Weyland, S.; Fritsch, J.; Woll, A.; Niessner, C.; Burchartz, A.; Schmidt, S.C.E.; Jekauc, D. A Short Version of the Physical Activity Enjoyment Scale: Development and Psychometric Properties. Int. J. Environ. Res. Public Health 2021, 18, 11035. [Google Scholar] [CrossRef]
- Rodríguez De Vera-Gómez, P.; Piñar-Gutiérrez, A.; Guerrero-Vázquez, R.; Bellido, V.; Morales-Portillo, C.; Sancho-Márquez, M.P.; Espejo-García, P.; Gros-Herguido, N.; López-Gallardo, G.; Martínez-Brocca, M.A.; et al. Flash Glucose Monitoring and Diabetes Mellitus Induced by Immune Checkpoint Inhibitors: An Approach to Clinical Practice. J. Diabetes Res. 2022, 2022, 4508633. [Google Scholar] [CrossRef] [PubMed]
- Choi, L.; Liu, Z.; Mattews, C.E.; Buchowski, M.S. Validation of Accelerometer Wear and Nonwear Time Classification Algorithm. Med. Sci. Sport. Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and Comparison of ActiGraph Activity Monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer Health: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef]
- Yardley, J.E.; Kenny, G.P.; Perkins, B.A.; Riddell, M.C.; Balaa, N.; Malcolm, J.; Boulay, P.; Khandwala, F.; Sigal, R.J. Resistance Versus Aerobic Exercise. Diabetes Care 2013, 36, 537–542. [Google Scholar] [CrossRef]
- Riddell, M.; Perkins, B.A. Exercise and Glucose Metabolism in Persons with Diabetes Mellitus: Perspectives on the Role for Continuous Glucose Monitoring. J. Diabetes Sci. Technol. 2009, 3, 914–923. [Google Scholar] [CrossRef]
- Malakou, E.; Linardakis, M.; Armstrong, M.E.G.; Zannidi, D.; Foster, C.; Johnson, L.; Papadaki, A. The Combined Effect of Promoting the Mediterranean Diet and Physical Activity on Metabolic Risk Factors in Adults: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2018, 10, 1577. [Google Scholar] [CrossRef]
- von Schnurbein, J.; Boettcher, C.; Brandt, S.; Karges, B.; Dunstheimer, D.; Galler, A.; Denzer, C.; Denzer, F.; Vollbach, H.; Wabitsch, M.; et al. Sleep and Glycemic Control in Adolescents with Type 1 Diabetes. Pediatr. Diabetes 2018, 19, 143–149. [Google Scholar] [CrossRef]
- González-Devesa, D.; Sanchez-Lastra, M.A.; Pérez-Fernández, P.; Diz-Gómez, J.C.; Ayán-Pérez, C. The Effect of Physical Activity on Sleep Quality in People with Diabetes: Systematic Review and Meta-Analysis. Sleep Breath 2024, 29, 23. [Google Scholar] [CrossRef]
- Henson, J.; Rowlands, A.V.; Baldry, E.; Brady, E.M.; Davies, M.J.; Edwardson, C.L.; Yates, T.; Hall, A.P. Physical Behaviors and Chronotype in People with Type 2 Diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001375. [Google Scholar] [CrossRef]
- Sleiman, D.; Al-Badri, M.R.; Azar, S.T. Effect of Mediterranean Diet in Diabetes Control and Cardiovascular Risk Modification: A Systematic Review. Front. Public Health 2015, 3, 69. [Google Scholar] [CrossRef] [PubMed]
- Focht, B.C. Brief Walks in Outdoor and Laboratory Environments. Res. Q. Exerc. Sport 2009, 80, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Fraser, M.; Polson, R.; Munoz, S.A.; Macrury, S. Psychological Effects of Outdoor Activity in Type 2 Diabetes: A Review. Health Promot. Int. 2020, 35, 841–851. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Daily Dietary Intake | Indoor Session 1 | Indoor Session 2 | Outdoor Session 1 | Outdoor Session 2 | |
| CHO (g) | 110 | 196 | 155 | 160 | |
| PRO (g) | 62 | 72 | 98 | 69 | |
| FAT (g) | 37 | 24 | 30 | 25 | |
| Daily Caloric Intake (kcal) | 1025 | 1288 | 1229 | 1127 | |
| Questionnaire | Enrolment | Indoor Session 1 | Indoor Session 2 | Outdoor Session 1 | Outdoor Session 2 |
| Mediterranean Diet (AU) | 7 | 8 | 7 | 7 | 7 |
| Sleep Score (AU) | 4 | 3 | 2 | 3 | 4 |
| Chronotype (AU) | 63 | 62 | 58 | 58 | 57 |
| Enjoyment (AU) | N/A | 28 | 20 | 28 | 29 |
| IPAQ Parameters | |||||
| MET × week (MET) | 320 | 1920 | 3840 | 800 | 1200 |
| Kcal × week (kcal) | 1072 | 4067 | 8134 | 2275 | 2861 |
| Sitting Time (minutes × day) | 425 | 120 | 150 | 80 | 150 |
| Physical Activity Level | Right Wrist | Left Wrist | Back | Right Waist | Left Waist |
|---|---|---|---|---|---|
| METs | 6.59 | 6.57 | 5.92 | 3.05 | 3.32 |
| Energy Expenditure (Kcal) | 394 | 383 | 375 | 394 | 383 |
| Activity counts (counts min−1) | 3936 | 3937 | 3929 | 4384 | 3937 |
| Psycho-Physiological Parameters | Indoor Session 1 | Indoor Session 2 | Outdoor Session 1 | Outdoor Session 2 |
|---|---|---|---|---|
| Energy Expenditure (kcal) | 197 | 558 | 553 | 296 |
| Recovery Index (AU) | 1.6 | 4 | 3.2 | 2.8 |
| Mean Heart Rate (beats·min−1) | 113 | 126 | 119 | 110 |
| Maximum Heart Rate (beats·min−1) | 196 | 183 | 159 | 170 |
| sRPE (AU) | 4 | 5 | 4 | 4 |
| Blood Pressure Measurements | PRE | POST | POST-15 | POST-30 | |
|---|---|---|---|---|---|
| Indoor 1 | Systolic (mmHg) | 131 | 130 | 129 | 130 |
| Diastolic (mmHg) | 88 | 80 | 91 | 86 | |
| Heart Rate (beats·min−1) | 65 | 78 | 75 | 78 | |
| Post-Exercise Hypotension (mmHg) | 1 | ||||
| Rate pressure product (sBP × HR) | 8515 | ||||
| Indoor 2 | Systolic (mmHg) | 130 | 129 | 123 | 127 |
| Diastolic (mmHg) | 91 | 92 | 88 | 87 | |
| Heart Rate (beats·min−1) | 65 | 87 | 78 | 82 | |
| Post-Exercise Hypotension (mmHg) | 3 | ||||
| Rate pressure product (sBP × HR) | 8547 | ||||
| Outdoor 1 | Systolic (mmHg) | 131 | 129 | 131 | 128 |
| Diastolic (mmHg) | 79 | 83 | 79 | 77 | |
| Heart Rate (beats·min−1) | 60 | 80 | 68 | 68 | |
| Post-Exercise Hypotension (mmHg) | 3 | ||||
| Rate pressure product (sBP × HR) | 7890 | ||||
| Outdoor 2 | Systolic (mmHg) | 130 | 128 | 121 | 116 |
| Diastolic (mmHg) | 82 | 90 | 84 | 75 | |
| Heart Rate (beats·min−1) | 75 | 91 | 84 | 86 | |
| Post-Exercise Hypotension (mmHg) | 13 | ||||
| Rate pressure product (sBP × HR) | 9750 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papale, O.; Festino, E.; Di Rocco, F.; Foster, C.; Prestanti, I.; Serafini, S.; Izzicupo, P.; Cortis, C.; Fusco, A. The Impact of a Multidimensional Physical Activity Intervention on Glycemic Control in Type 1 Diabetes: A Preliminary Study. J. Funct. Morphol. Kinesiol. 2025, 10, 163. https://doi.org/10.3390/jfmk10020163
Papale O, Festino E, Di Rocco F, Foster C, Prestanti I, Serafini S, Izzicupo P, Cortis C, Fusco A. The Impact of a Multidimensional Physical Activity Intervention on Glycemic Control in Type 1 Diabetes: A Preliminary Study. Journal of Functional Morphology and Kinesiology. 2025; 10(2):163. https://doi.org/10.3390/jfmk10020163
Chicago/Turabian StylePapale, Olga, Emanuel Festino, Francesca Di Rocco, Carl Foster, Iris Prestanti, Sofia Serafini, Pascal Izzicupo, Cristina Cortis, and Andrea Fusco. 2025. "The Impact of a Multidimensional Physical Activity Intervention on Glycemic Control in Type 1 Diabetes: A Preliminary Study" Journal of Functional Morphology and Kinesiology 10, no. 2: 163. https://doi.org/10.3390/jfmk10020163
APA StylePapale, O., Festino, E., Di Rocco, F., Foster, C., Prestanti, I., Serafini, S., Izzicupo, P., Cortis, C., & Fusco, A. (2025). The Impact of a Multidimensional Physical Activity Intervention on Glycemic Control in Type 1 Diabetes: A Preliminary Study. Journal of Functional Morphology and Kinesiology, 10(2), 163. https://doi.org/10.3390/jfmk10020163