
Effects of Supervised Strength Training on Physical Fitness in Children and Adolescents: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Quality Assessment Data Extraction
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
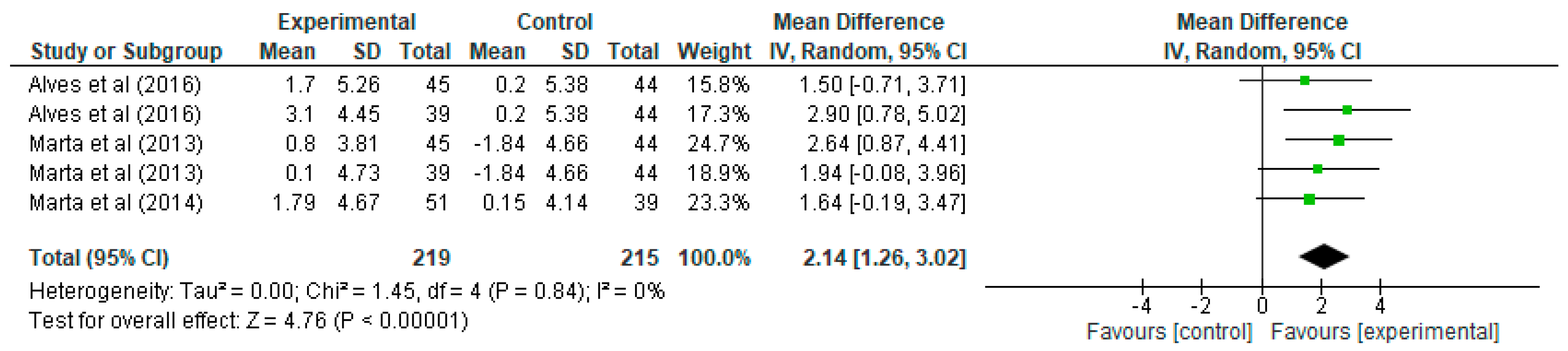
3.1. Results of Strength Training on Maximal Oxygen Volume
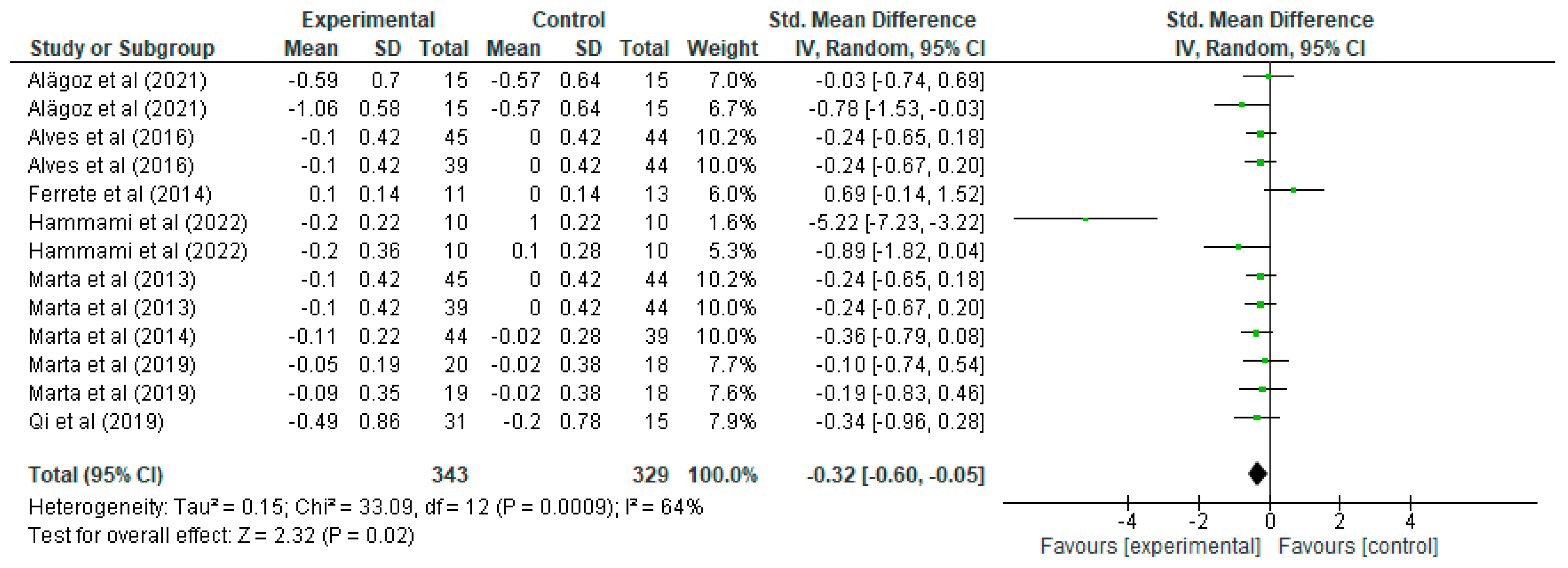
3.2. Results of Strength Training in Sprinting
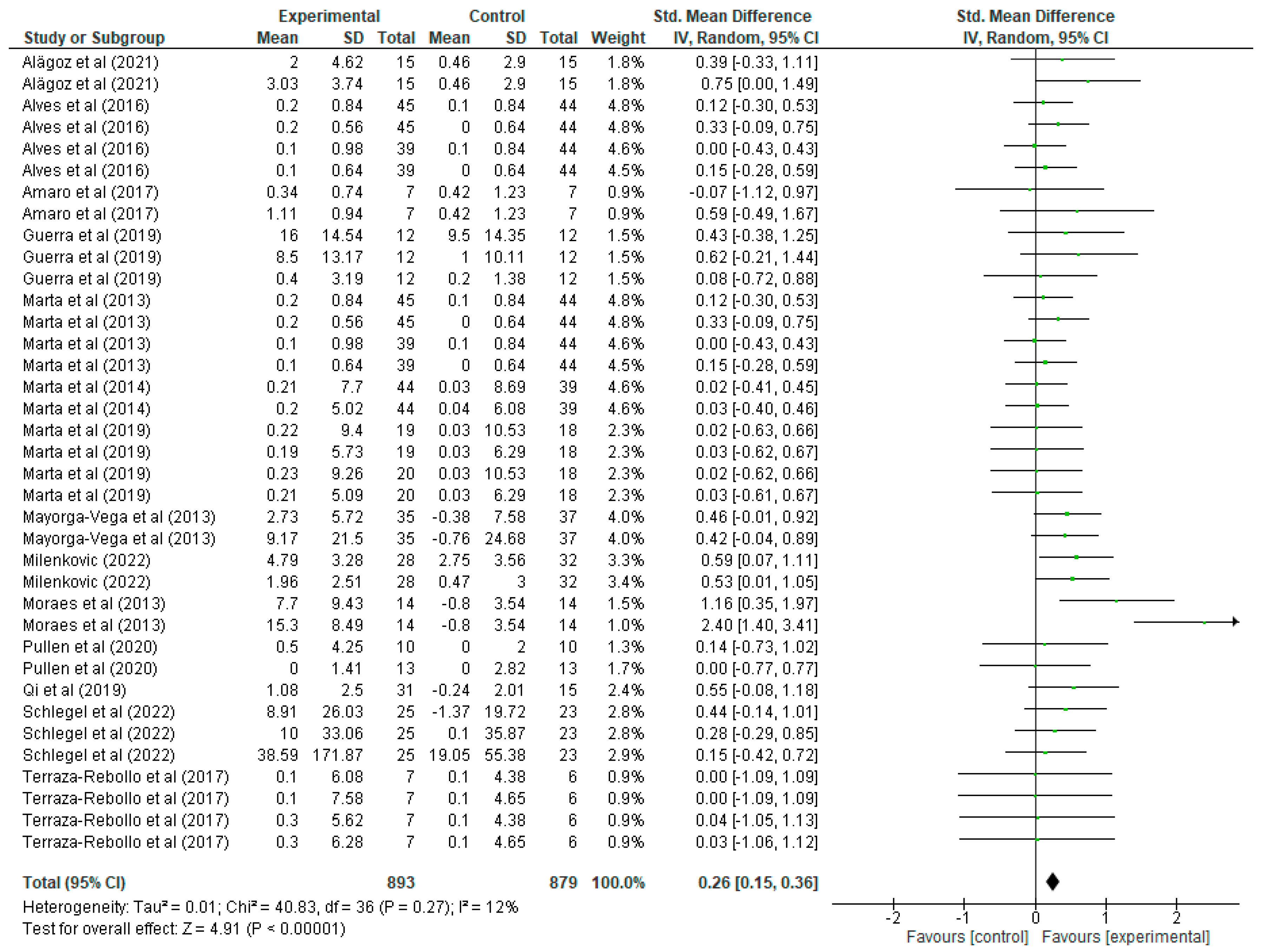
3.3. Results of Strength Training in Upper Limb Strength Improvement
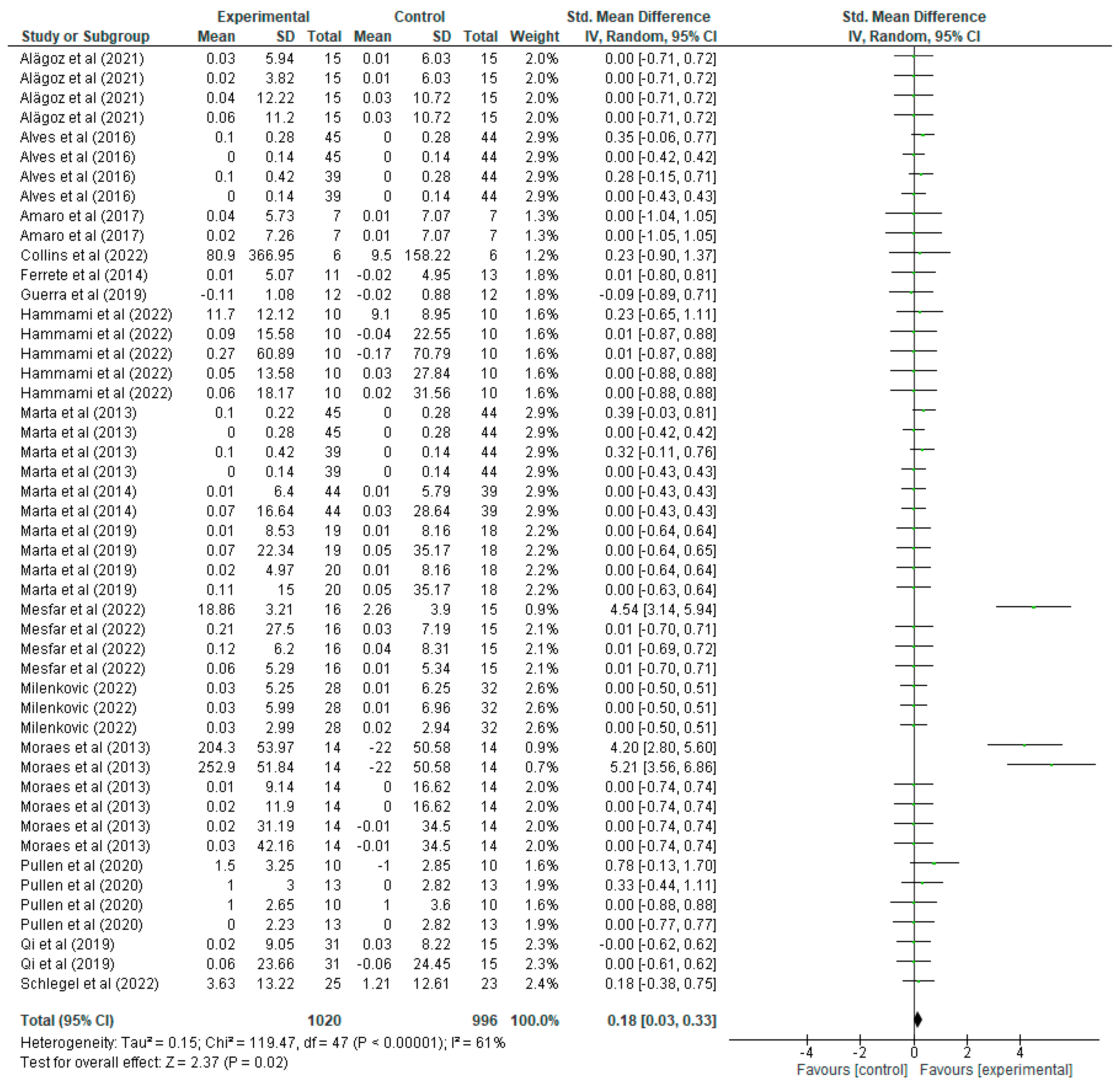
3.4. Results of Strength Training on Lower Limb Strength Improvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mastorci, F.; Lazzeri, M.; Vassalle, C.; Pingitore, A. The transition from childhood to adolescence: Between health and vulnerability. Children 2024, 11, 989. [Google Scholar] [CrossRef]
- Behm, D.G.; Faigenbaum, A.D.; Falk, B.; Klentrou, P. Canadian Society for Exercise Physiology position paper: Resistance training in children and adolescents. Appl. Physiol. Nutr. Metab. 2008, 33, 547–561. [Google Scholar] [CrossRef]
- Peinado, E.; Mora, C.A.; Hutchison, L.R. Entrenamiento de la fuerza en niños y adolescentes: Una revisión sistemática años 2018–2022. Sportis 2024, 10, 158–187. [Google Scholar] [CrossRef]
- Villa-González, E.; Barranco-Ruiz, Y.; García-Hermoso, A.; Faigenbaum, A.D. Efficacy of school-based interventions for improving muscular fitness outcomes in children: A systematic review and meta-analysis. Eur. J. Sport Sci. 2023, 23, 444–459. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Myer, G.D. Resistance training among young athletes: Safety, efficacy and injury prevention effects. Br. J. Sports Med. 2010, 44, 56–63. [Google Scholar] [CrossRef]
- Haff, G.G.; Triplett, N.T. (Eds.) Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Benson, A.C.; Torode, M.E.; Singh, F. The effect of high-intensity progressive resistance training on adiposity in children: A randomized controlled trial. Int. J. Obes. 2008, 32, 1016–1027. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Cronin, J.B.; Faigenbaum, A.D.; Haff, G.G.; Howard, R.; Kraemer, W.J.; Micheli, L.J.; Myer, G.D.; Oliver, J.L. National Strength and Conditioning Association position statement on long-term athletic development. J. Strength Conditining Res. 2016, 30, 1491–1509. [Google Scholar] [CrossRef]
- Valle, V.; Vanaclocha-Amat, P.; Villa-González, E. Efectos del entrenamiento de fuerza pediátrico sobre parámetros de salud en niños: Una revisión sistemática. Sportis 2022, 8, 283–308. [Google Scholar] [CrossRef]
- Vázquez, B.L.; González, J.A.R. Entrenamiento de fuerza con bandas elásticas en niños y adolescentes: Una revisión sistemática. Retos 2022, 44, 202–208. [Google Scholar] [CrossRef]
- Lobelo, F.; Muth, N.D.; Hanson, S.; Nemeth, B.A.; LaBella, C.R.; Brooks, M.A.; Canty, G.; Diamond, A.B.; Hennrikus, W.; Logan, K.; et al. Physical activity assessment and counseling in pediatric clinical settings. Pediatrics 2020, 145, 3. [Google Scholar] [CrossRef]
- Logan, N.; Ward-Ritacco, C. The developing brain: Considering the multifactorial effects of obesity, physical activity & mental wellbeing in childhood and adolescence. Children 2022, 9, 1802. [Google Scholar] [CrossRef]
- Leidy, H.; Gwin, J. Growing up strong: The importance of physical, mental, and emotional strength during childhood and adolescence with focus on dietary factors. Appl. Physiol. Nutr. Metab. 2020, 45, 1071–1080. [Google Scholar] [CrossRef]
- Márquez, S. Beneficios psicológicos de la actividad física. Rev. Fed. Españ. Asoc. Psicol. 1995, 48, 185–206. [Google Scholar]
- Chacón-Cuberos, R.; Zurita-Ortega, F.; Ramírez-Granizo, I.; Castro-Sánchez, M. Actividad física y rendimiento académico en la infancia y la preadolescencia: Una revisión sistemática. Apunt. Educ. Fís. Deportes 2020, 36, 1–9. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L. The youth physical development model: A new approach to long-term athletic development. Strength Cond. J. 2012, 34, 61–72. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef]
- Gorce, P.; Jacquier-Bret, J. Work-Related Musculoskeletal Disorder Prevalence by Body Area Among Nurses in Europe: Systematic Review and Meta-Analysis. J. Funct. Morphol. Kinesiol. 2025, 10, 66. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Alagöz, İ.; Can, S.; Demirkan, E.; Özkadı, T.; Demir, E. Effect of different training models on motoric and swimming performance in prepubescent swimmers. Pedagog. Phys. Cult. Sports 2021, 25, 286–295. [Google Scholar] [CrossRef]
- Alves, A.R.; Marta, C.C.; Neiva, H.P.; Izquierdo, M.; Marques, M.C. Does intrasession concurrent strength and aerobic training order influence training-induced explosive strength and VO2max in prepubescent children? J. Strength Cond. Res. 2016, 30, 3267–3277. [Google Scholar] [CrossRef] [PubMed]
- Amaro, N.M.; Marinho, D.A.; Marques, M.C.; Batalha, N.P.; Morouço, P.G. Effects of dry-land strength and conditioning programs in age group swimmers. J. Strength Cond. Res. 2017, 31, 2447–2454. [Google Scholar] [CrossRef]
- Assunção, A.R.; Bottaro, M.; Ferreira-Junior, J.B.; Izquierdo, M.; Cadore, E.L.; Gentil, P. The chronic effects of low-and high-intensity resistance training on muscular fitness in adolescents. PLoS ONE 2016, 11, e0160650. [Google Scholar] [CrossRef]
- Ben Othman, A.; Behm, D.G.; Chaouachi, A. Evidence of homologous and heterologous effects after unilateral leg training in youth. Appl. Physiol. Nutr. Metab. 2018, 43, 282–291. [Google Scholar] [CrossRef]
- Collins, H.M.; Fawkner, S.; Booth, J.N.; Duncan, A. The impact of resistance training on strength and correlates of physical activity in youth. J. Sports Sci. 2022, 40, 40–49. [Google Scholar] [CrossRef]
- Dobbs, I.J.; Oliver, J.L.; Wong, M.A.; Moore, I.S.; Myer, G.D.; Lloyd, R.S. Effects of a 4-week neuromuscular training program on movement competency during the back-squat assessment in pre–and post–peak height velocity male athletes. J. Strength Cond. Res. 2021, 35, 2698–2705. [Google Scholar] [CrossRef]
- Ferrete, C.; Requena, B.; Suarez-Arrones, L.; de Villarreal, E.S. Effect of strength and high-intensity training on jumping, sprinting, and intermittent endurance performance in prepubertal soccer players. J. Strength Cond. Res. 2014, 28, 413–422. [Google Scholar] [CrossRef]
- Guerra, L.A.; Dos Santos, L.R.A.; Pereira, P.E.; Lauria, V.T.; De Lima, C.; Evangelista, A.L.; Rica, R.L.; Bocalini, D.; Bastos-Messias, C.; Teixeira, C.V.L.S. A low-cost and time-efficient calisthenics strength training program improves fitness performance of children. J. Phys. Educ. Sport 2019, 19, 58–62. [Google Scholar]
- Hammami, R.; Duncan, M.J.; Nebigh, A.; Werfelli, H.; Rebai, H. The effects of 6 weeks eccentric training on speed, dynamic balance, muscle strength, power, and lower limb asymmetry in prepubescent weightlifters. J. Strength Cond. Res. 2022, 36, 955–962. [Google Scholar] [CrossRef]
- Marinho, D.A.; Neiva, H.P.; Marques, L.; Lopes, V.P.; Morais, J.E. The influence of a specific high-intensity circuit training during physical education classes in children’s physical activity and body composition markers. Montenegrin J. Sports Sci. Med. 2022, 2, 29–36. [Google Scholar] [CrossRef]
- Marta, C.; Alves, A.R.; Esteves, P.T.; Casanova, N.; Marinho, D.; Neiva, H.P.; Marques, M.C. Effects of suspension versus traditional resistance training on explosive strength in elementary school-aged boys. Pediatr. Exerc. Sci. 2019, 31, 473–479. [Google Scholar] [CrossRef]
- Marta, C.; Marinho, D.A.; Barbosa, T.M.; Izquierdo, M.; Marques, M.C. Effects of concurrent training on explosive strength and VO2max in prepubescent children. Int. J. Sports Med. 2013, 34, 888–896. [Google Scholar] [CrossRef]
- Marta, C.C.; Marinho, D.A.; Izquierdo, M.; Marques, M.C. Differentiating maturational influence on training-induced strength and endurance adaptations in prepubescent children. Am. J. Hum. Biol. 2014, 26, 469–475. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Viciana, J.; Cocca, A. Effects of a circuit training program on muscular and cardiovascular endurance and their maintenance in schoolchildren. J. Hum. Kinet. 2013, 37, 153–160. [Google Scholar] [CrossRef]
- Mesfar, A.; Hammami, R.; Selmi, W.; Gaied-Chortane, S.; Duncan, M.; Bowman, T.G.; Nobari, H.; van den Tillaar, R. Effects of 8-week in-season contrast strength training program on measures of athletic performance and lower-limb asymmetry in male youth volleyball players. Int. J. Environ. Res. Public Health 2022, 19, 6547. [Google Scholar] [CrossRef]
- Milenković, D. Effect of 8-week circuit training on the development of different forms of muscle strength in physical education. J. Effic. Responsib. Educ. Sci. 2022, 15, 221–227. [Google Scholar] [CrossRef]
- Moraes, E.; Fleck, S.J.; Dias, M.R.; Simão, R. Effects on strength, power, and flexibility in adolescents of nonperiodized vs. daily nonlinear periodized weight training. J. Strength Conditioining Res. 2013, 27, 3310–3321. [Google Scholar] [CrossRef]
- Pullen, B.J.; Oliver, J.L.; Lloyd, R.S.; Knight, C.J. The effects of strength and conditioning in physical education on athletic motor skill competencies and psychological attributes of secondary school children: A pilot study. Sports 2020, 8, 138. [Google Scholar] [CrossRef]
- Qi, F.; Kong, Z.; Xiao, T.; Leong, K.; Zschorlich, V.R.; Zou, L. Effects of combined training on physical fitness and anthropometric measures among boys aged 8 to 12 years in the physical education setting. Sustainability 2019, 11, 1219. [Google Scholar] [CrossRef]
- Schlegel, P.; Sedláková, L.; Křehký, A. Street workout is the new gymnastics-strength development in a very short school-based program. J. Phys. Educ. Sport 2022, 22, 489–494. [Google Scholar]
- Terraza-Rebollo, M.; Baiget, E.; Corbi, F.; Anzano, A.P. Efectos del entrenamiento de fuerza en la velocidad de golpeo en tenistas jóvenes. J. Med. Sci. Phys. Act. Sport 2017, 17, 349–366. [Google Scholar]
- Neyeloff, J.L.; Fuchs, S.C.; Moreira, L.B. Meta-analyses and forest plots using a Microsoft Excel spreadsheet: Step-by-step guide focusing on descriptive data analysis. BMC Res. Notes 2012, 5, 52. [Google Scholar] [CrossRef]
- Malina, R.M. Weight training in youth-growth, maturation, and safety: An evidence-based review. Clin. J. Sport Med. 2006, 16, 478–487. [Google Scholar] [CrossRef]
- Granacher, U.; Lesinski, M.; Büsch, D.; Muehlbauer, T.; Prieske, O.; Puta, C.; Zieschang, T.; Behm, D.G. Effects of resistance training in youth athletes on muscular fitness and athletic performance: A conceptual model for long-term athlete development. Front. Physiol. 2016, 7, 164. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Faigenbaum, A.D.; Stone, M.H.; Oliver, J.L.; Jeffreys, I.; Moody, J.A.; Brewer, C.; Pierce, K.C.; McCambridge, T.M.; Howard, R.; et al. Position statement on youth resistance training: The 2014 International Consensus. Br. J. Sports Med. 2014, 48, 498–505. [Google Scholar] [CrossRef]
- Martin, D. Allgemeine Methodik der Kinder- und Jugendtrainings; [General Methodology of Children’s and Youth Training]; Karl Hofmann: Schorndorf, Germany, 2001. [Google Scholar]
- Bompa, T.O.; Buzzichelli, C. Training and Conditioning Young Athletes; Human Kinetics: Champaign, IL, USA, 2021. [Google Scholar]
- Dahab, K.S.; McCambridge, T. Strength Training in Children and Adolescents. Sports Health 2009, 1, 223–226. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | YES | No | %YES | Risk of Biais |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [20] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [21] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [22] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [23] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [24] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | NO | NO | YES | 14 | 5 | 74% | MEDIUM |
| [25] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [26] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [27] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [28] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [29] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [30] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [31] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [32] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [33] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [34] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [35] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [36] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [37] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [38] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [39] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [40] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| [41] | YES | YES | NO | YES | YES | YES | NO | YES | YES | YES | YES | YES | NO | NA | YES | YES | YES | YES | NO | YES | 15 | 4 | 79% | MEDIUM |
| Author | Design, Sample, Age | Inclusion Criteria | Intervention | Time, Freq, Duration, Rep, Sets | Variables | Instruments |
|---|---|---|---|---|---|---|
| [20] | Design: Quasi-experimental Sample: EG = 30; CG = 15 Age: EG = 9.0 ± 0.6; CG = 9.1 ± 0.7 | Children who regularly practice swimming, aged between 9 and 11 years, with 2 years of experience. | E = Swimming training program and body strength program using bodyweight exercises, medicine ball, and resistance bands. C = Regular swimming training. | T = 12 weeks F = 3/weeks D = 90 (Strength + swimming) R = 8–12 S = 3 | Biceps, chest, waist, hip, and thigh circumference. Vertical jump, flexed arm strength, speed, upper body strength, horizontal jump, flexibility, aerobic endurance, balance, and 50 m freestyle swimming were also measured. | Anthropometric tests with their respective equipment. UBS test for ball throw. FAS test for static arm strength. Sit and reach test for spinal flexibility. Cooper test. |
| [21] | Design: RCT Sample: EG = 84; CG = 44 Age: EG = 10.5 ± 0.8; CG = 10.6 ± 0.9 | Aged 10 to 12 years without chronic paediatric disease or orthopaedic limitations and without regular extracurricular physical activity (i.e., participation in a sport at an academy). | E = Strength and aerobic training before or after strength training. C = Physical education classes only. | T = 8 weeks F = 2/week D = 45–90 min S = 2–4 R = 4–8 | Strength, VO2max, and anthropometric variables. | Anthropometric instruments, Eurofit test battery, contact mat, and photocells. |
| [22] | Design: Controlled trial Sample: EG = 14; CG = 7 Age: EG = 12.7 ± 0.8; CG = 12.7 ± 0.8 | Two years of experience in swimming. | E = Strength training and swimming. C = Strength training only. | T = 10 weeks. F = 2/week D = 30 min Before swimming S = 3 R = as many as possible in 40 s | Strength, mechanical impulse, vertical jump, and ball throw. | Contact mat, medicine ball, stopwatch. |
| [23] | Design: RCT Sample: EG-LRM = 17; EG-HRM = 16; CG = 12 Age: EG = 13.7 ± 0.8; CG = 13.7 ± 0.8 | The potential participants had to be between 13 and 15 years old, have never participated in a resistance training program, and have no health issues. | E = Leg press, knee extension, barbell bench press, dumbbell fly, lat pulldown, seated row, crunches, and leg raises. C = Without training. | T = 9 weeks F = 2/week. D = 1 h S = 2 R = 4–6 y 12–15. | Upper and lower body muscle strength. | Machinery for the exercises described. |
| [24] | Design: Controlled trial Sample: EG = 16; CG = 16 Age: EG = 11.5 ± 0.6; CG = 11.9 ± 1.2 | Healthy children without diagnosed diseases. | E = Strength program for upper and lower body. C = Without training. | T = 8 weeks F = 3/week D = NR S = 4–8 y 1–2 R = 5 y 20 (First, a high-load and low-repetition group, followed by a high-repetition group) | Unilateral, ipsilateral, and contralateral strength of the lower limbs, power, and endurance (one-repetition maximum (1RM) leg press, knee extensors (KE) and flexors (KF) maximum voluntary isometric contractions (MVIC), countermovement jump (CMJ), muscle endurance test (leg press repetitions at 60% of 1RM)), and unilateral upper body elbow MVIC. | Horizontal press measuring 1RM. Isometric quadriceps and hamstring extension. Dynamometer. Ergojump for CMJ. Hand dynamometer for arm strength. |
| [25] | Design: Quasi-experimental Sample: EG = 6; CG = 6 Age: EG = 8.9 ± 1.0; CG = 8.9 ± 1.0 | Students aged 8 to 10 years, with no current participation in resistance training, no pathology or disability affecting movement, behaviour, or neuropsychological function, and no physical injury. | E = Strength training with deadlift, squat, row, lunge, pull-ups, and hollow hold, along with a warm-up and cool-down. C = Normal physical activity, without resistance training. | T = 10 week F = 2/week D = 45 min S = 2 R = 6–8 | Perceived strength, physical self-assessment, global self-esteem, sports competence, physical condition, FMS, height, body mass, BMI, skinfolds, hip, waist, and arm circumference, maximum strength, and relative strength. | Anthropometric instruments, feedback session, and questionnaires (CY-PSPP), Actigraph GT3X+ accelerometer, FMS (Canadian assessment of agility and movement skills), extension machine for performing an isometric mid-thigh pull to measure strength. |
| [26] | Design: RCT Sample: EG = 11; CG = 11 Age: EG = 15.4 ± 0.9; CG = 14.5 ± 0.8 | Healthy subjects without injuries or pathologies. | E = Full-body strength training. C = Normal life. | T = 4 week F = 2/week D = 60 min S = 3–4 R = 10–15 | Strength through the execution of the back squat. Peak squat velocity. | Necessary equipment for squat execution and anthropometric materials for muscle mass and height measurement, as well as an accelerometer for peak velocity. |
| [27] | Design: Controlled trial Sample: EG = 11; CG = 13 Age: EG = 9.32 ± 0.25; CG = 8.26 ± 0.33 | Subjects with potential medical problems or a history of ankle, knee, or back pathology within 3 months prior to the start of the study. | E = strength training with ¼ squat, weighted vertical jump, deep squat, push-ups, hurdle jumps, and sprints. C = normal soccer training. | T = 26 week. F = 2/week D = 30 min S = 2–4 R = 4–8 | Strength, speed, endurance and flexibility. | Anthropometric instruments, CMJ with ergojump contact platform, photocells for sprint speed, YO-YO test and sit-and-reach test. |
| [28] | Design: Controlled trial Sample: EG = 12; CG = 12 Age: EG = 15.0 ± 0.84; CG = 15.0 ± 0.84 | Students without sports practice. | E = 6-station strength circuit, including squats, push-ups, triceps dips, horizontal jump, plank and “the rower” curl up. C = physical education classes without strength training, they did stretch. | T = 8 weeks F = 2/week. D = 50 min S = 3 R = 30 s of execution of each of the exercises, as many repetitions as possible. | Strength and power in upper and lower body. | Meter and stopwatch. |
| [29] | Design: RCT Sample: EG = 10; CG = 10 Age: EG = 11.1 ± 0.8; CG = 11.1 ± 0.8 | Weightlifting children. | E = eccentric training program focusing on hamstrings with glute and hamstring raises, glute push-ups, good mornings, one-leg Romanian deadlifts, and manual glute raises. C = normal weightlifting training. | T = 6 weeks F = 2/week D = 60–90 min S = 3–5 R = 10–12 | Sprint, balance, muscle strength, power and asymmetry between lower limbs. | Sprint with photocells. Horizontal jump power meter. Squat bar for measuring 1RM to measure muscle strength. Asymmetry meter using a single leg jump. Y-balance test, apparatus. |
| [30] | Design: RCT Sample: EG = 42; CG = 63 Age: EG = 11.63 ± 0.97; CG = 11.64 ± 0.87 | Apparently healthy children. | E = high intensity strength program. C = normal physical education class. | T = 8 weeks F = 2/week D = 60 min S = 2 R = It was carried out by execution time, week 1 and 2 (30 s), week 3 and 5 (40 s) and week 6 and 8 (45 s). | Cardiorespiratory variables and certain aspects related to muscle strength were measured. Fat mass. | Fat mass and body mass with bioimpedance. Physical fitness with fitnessgram test. Walking and return tests with cones to assess cardiorespiratory fitness. SLJ tests to assess the power of the lower limbs. And curl up, push up, standing long jump, and vertical jump to assess strength. |
| [31] | Design: RCT Sample: ER = 19; ES = 20; CG = 18 Age: ER = 10.6 ± 0.5; ES = 10.7 ± 0.5; CG = 10.6 ± 0.5 | Children between 10 and 11 years old, physically active, in optimal health and who regularly attend training sessions. | E = strength training with conventional and TRX exercises. C = conventional physical education classes. | T = 8 weeks F = 2/week D = 45 min S = 2–4 R = 8–15 | The strength of the lower and upper limbs, as well as motor coordination, was observed. | Contact platform, manual dynamometer, and photocells. |
| [32] | Design: Controlled trial Sample: ER = 41; ECoN = 45; CG = 39 Age: ER = 10; ECoN = 10; CG = 10 | Boys and girls aged 10 to 11.5 years without chronic paediatric disease or orthopaedic limitation and without regular extracurricular PA. | E = strength training and the RYF group was also subjected to a 20 m round trip race after strength training. C = normal physical education. | T = 8 weeks F = 2/week D = 45–60 min S = 2–5 R = 4–8 | Body anthropometric measurements were made, explosive strength of the lower and upper body, running speed and VO2max were calculated. | CD and audio for the 20 m dash. Contact pad for CJM, cones for the 20 m dash distance, and medicine balls for strength training. |
| [33] | Design: Controlled trial Sample: ER = 41; ECoN = 45; CG = 39 Age: ER = 10.7 ± 0.4; ECoN = 10.7 ± 0.5; CG = 10.8 ± 0.5 | Children aged between 10 and 11.5 years (5th and 6th grade), without chronic paediatric disease or orthopaedic limitation and without regular extracurricular physical activity (e.g., practicing a sport in a club) | ER and CON = After the warm-up period, both GR and GCON groups were subjected to a strength training program consisting of 1 and 3 kg medicine ball throws; box jumps from 0.3 m to 0.5 m; plyometric jumps over a 0.3–0.5 m high hurdle and 30–40 m sprint runs. After finishing strength training for the GR and GCON groups, the GCON group was additionally subjected to a 20 m shuttle run exercise. C = Physical education class. | T = 8 weeks F = 2/week D = 45–60 min S = 2–5 R = 3–8 | Strength and VO2max measurements were carried out. | Contact platform. Eurofit battery. Photocells for sprinting and viewing the acquired speed. Course navette and formula to calculate Vo2max. Anthropometric tools. |
| [34] | Design: Controlled trial Sample: EG = 35; CG = 37 Age: EG = 11.10 ± 0.38; CG = 11.10 ± 0.38 | Healthy children with no apparent illness. | E = Strength/endurance and cardiovascular circuit program. C = Physical education class. | T = 8 weeks F = 2/week D = 50 min S = 2 R = for time of 15 a 30 s. | Abdominal muscle endurance, upper body endurance, and cardiovascular endurance were measured. | Medicine balls, pull-up bar/wall bars for hanging, and speaker for course navette. |
| [35] | Design: RCT Sample: EG = 16; CG = 15 Age: EG = 14.4 ± 0.6; CG = 14.5 ± 0.5 | Playing volleyball regularly, 3–4 times x week (i.e., ~90 min per session), with one match played during the weekend, for more than 3 years. | E = Resistance training with bench press, pull over, half squat, and forward lunge C = Normal training. | T = 8 weeks F = 2/week D = 50 min S = 3–4 R = 2–4 | Dynamic balance was measured. 1RM back squat. CMJ was measured. Lower limb asymmetry. | Y test. Barbell and plates for back squat. Contact platform for CMJ. |
| [36] | Design: RCT Sample: EG = 28; CG = 32 Age: EG = 13; CG = 13 | There were no chronic illnesses or major injuries in the students’ health records. | E = special program for strength development using circuit training within the main part of the class C = regular physical education class. | T = 8 weeks F = 2/week D = 50 min S = 2 R = 30 s | The jump squat and CMJ were measured. Normal squat. Push-ups and sit-ups. | CMJ and sato squat with photocells. |
| [37] | Design: RCT Sample: EG = 14; CG = 10 Age: EG = 15.4 ± 0.9; CG = 15.4 ± 0.9 | Physically active, but had not performed RT; had no functional limitation in performing the prescribed RT program; had no injuries. | E = strength training with bench press on machine, leg press at 45°, front lat pull-down, leg extension, military press, seated leg curl, triceps extension on pulley, sit-ups and arm curl. C = normal life, without ST. | T = 12 weeks F = 3/week D = 60 min S = 3 R = 3–20 | 1RM strength, power, and flexibility. | Leg press and bench press. Contact platform. Flexibility box. |
| [38] | Design: RCT Sample: EM = 10; EF = 13; CM = 10; CF = 13 Age: EM = 12.07 ± 0.3; EF = 12.56 ± 0.97; CM = 11.67 ± 0.35; CF = 11.90 ± 0.76 | Children from 11 to 14 years old, minimum attendance at 5 sessions. | E = activities based on strength and physical conditioning. C = regular physical education class. | T = 6 weeks F = 3 sessions every 2 weeks. D = 60 min S = 1 R = 5–60 y 30 s according to exercise | Strength, autonomy, global self-esteem and physical self-efficacy. | Measuring meter. Test. |
| [39] | Design: Controlled trial Sample: EG = 31; CG = 15 Age: EG = 8–12; CG = 8–12 | Healthy children. | E = strength-resistance training and plyometrics. Squats, biceps curls, lunges, jumps, sit-ups and running. C = normal physical education classes. | T = 12 weeks F = 2/week D = 60 min S = 2–4 R = 8–30 | Anthropometric variables were measured, strength profiles with biceps curl, vertical jump and long jump with one foot and power and speed with a 30 m sprint. | Anthropometric utensils. Metro. Photocells. Chronometer. |
| [40] | Design: RCT Sample: EG = 25; CG = 23 Age: EG = 10–11; CG = 10–11 | Without inclusion criteria, regular school without specialization in strength and/or resistance. | E = Strength training with body weight resistance consisting of push up, hang hold, sit and reach, squat and plank hold. C = Regular physical education classes. | T = 6 weeks F = 2/week D = 45 min S = 1–3 min R = <15 | Strength was measured through tests that they had trained for, to see changes from the beginning to the present moment. The tests included push ups, squats, suspended hold, plank, and sit-and-reach. | Pull-up bar, parallel bars, stopwatch, and meter. |
| [41] | Design: Controlled trial Sample: EG = 14; CG = 6 Age: EG = 14.9 ± 0.7; CG = 15.5 ± 0.9 | More than 4 years’ prior experience in tennis training, not practice any other sport, not have participated in any strength training and have not suffered any injuries during the last 6 months. | E = strength training with overload and elastic bands. C = technical-tactical training | T = 8 weeks F = 3/week D = 3 h S = 3 R = 6 | It was measured through the improvement in strength as well as how the tennis throwing speed was improved. | radar (Stalker Pro, Newark, CA, USA) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Torres, J.M.; García-Roca, J.A.; Abellan-Aynes, O.; Diaz-Aroca, A. Effects of Supervised Strength Training on Physical Fitness in Children and Adolescents: A Systematic Review and Meta-Analysis. J. Funct. Morphol. Kinesiol. 2025, 10, 162. https://doi.org/10.3390/jfmk10020162
Moreno-Torres JM, García-Roca JA, Abellan-Aynes O, Diaz-Aroca A. Effects of Supervised Strength Training on Physical Fitness in Children and Adolescents: A Systematic Review and Meta-Analysis. Journal of Functional Morphology and Kinesiology. 2025; 10(2):162. https://doi.org/10.3390/jfmk10020162
Chicago/Turabian StyleMoreno-Torres, José M., Juan Alfonso García-Roca, Oriol Abellan-Aynes, and Alvaro Diaz-Aroca. 2025. "Effects of Supervised Strength Training on Physical Fitness in Children and Adolescents: A Systematic Review and Meta-Analysis" Journal of Functional Morphology and Kinesiology 10, no. 2: 162. https://doi.org/10.3390/jfmk10020162
APA StyleMoreno-Torres, J. M., García-Roca, J. A., Abellan-Aynes, O., & Diaz-Aroca, A. (2025). Effects of Supervised Strength Training on Physical Fitness in Children and Adolescents: A Systematic Review and Meta-Analysis. Journal of Functional Morphology and Kinesiology, 10(2), 162. https://doi.org/10.3390/jfmk10020162