Abstract
Recreational dance offers significant psychological well-being potential. However, traditional instruction emphasizes technique while limiting attention to nervous system development and embodied meaning-making. Despite empirical support for polyvagal theory, motor learning science, somatic education, and phenomenology, their systematic integration into unified structures is not clearly established in recreational dance contexts. This protocol integrates nervous system regulation, motor learning, and creative expression within structured Imperial Society of Teachers of Dancing (ISTD) modern dance syllabus for recreational adults. It presents a 12-week integrated dance-mindfulness intervention addressing this gap through a three-phase structure grounded in neuroscience and embodied pedagogy. The intervention comprises eight standardized components delivered weekly. The randomized controlled trial evaluates intervention effects using the Satisfaction With Life Scale (SWLS), Depression Anxiety Stress Scales-21 (DASS-21), the Mindful Attention Awareness Scale (MAAS), the Subjective Happiness Scale (SHS), and the Leisure Involvement Scale (LIS). Qualitative assessment via semi-structured phenomenological interviews (Weeks 8 and 12) and weekly journaling captures somatic awareness, nervous system resilience, technical confidence, creative expression, relational and social belonging, and embodied meaning-making. Intervention participants are expected to show significantly greater improvements compared to controls. Results will establish evidence-based practice standards for recreational dance and demonstrate neuroscience integration’s efficacy for psychological wellbeing and embodied meaning-making.
1. Introduction
1.1. Background
Recreational dance is a leisure-based movement activity. It is pursued primarily for intrinsic rewards including enjoyment, self-expression, social connection, and personal well-being, as distinguished from professional performance contexts or clinical therapeutic interventions [1,2]. Research confirms that dance interventions significantly enhance emotional regulation, reduce stress, and promote social integration in recreational adult dancers and other populations [1,3,4], while also serving as a neuroprotective activity demanding complex cognitive engagement. For those navigating psychological distress, conscious movement facilitates non-verbal emotional expression and fosters psychological safety [5].
Traditional dance instruction emphasizes proprioceptive awareness to guide and coordinate complex movements [6,7]. However, dancers often receive limited support for developing psychological awareness and holistic well-being competencies that support mental health [7]. This represents a critical gap in dance education: while dance can be a powerful medium for psychological health and embodied resilience, current training rarely integrates mental skills development with technical instruction. Research has identified the absence of standardized, integrated protocols combining these elements as a significant limitation in the field [3].
Polyvagal Theory [8,9] positions the autonomic nervous system as the foundation for social engagement and learning capacity through neuroception. Neuroception is the subconscious physiological detection and interpretation of environmental cues signaling safety or threat, independent of conscious appraisal. Neuroception operates automatically, influencing whether the nervous system moves toward social engagement or defensive dysregulation. While Polyvagal Theory has generated important insights into nervous system regulation, recent neuroscientific debate has raised questions regarding specific anatomical claims [9]. This protocol draws on PVT’s overarching framework of nervous system hierarchy and safety-based learning while remaining open to evolving neuroscientific understanding.
In dance education, the presence of a safe, co-regulated environment allows the nervous system to maintain a parasympathetic tone (ventral vagal state) while remaining capable of engaging sympathetic activation for movement without triggering dysregulation into threat states, which is a critical condition for creative expression and learning [8,10]. Evidence indicates that deliberate cultivation of the Social Engagement System (ventral vagal activation) optimizes nervous system flexibility—the organism’s capacity to dynamically regulate physiological arousal to meet environmental and task demands [9,11]. This flexibility creates conditions where technical development can occur without physiological distress or threat-based dysregulation.
Motor learning science demonstrates that dance technique mastery is enhanced when new motor information builds upon, and is compatible with, existing motor schemas, generalized rules, and parameters that guide motor behavior, thereby accelerating skill integration and transfer [12,13,14]. Achieving a state of flow (full task engagement with optimal challenge) depends on the balance between an individual’s skills and the perceived task difficulty [15,16]. However, to maintain flow while progressively increasing difficulty, the gradual titration of challenge must also consider nervous system capacity. Within neuroscience frameworks, this means ensuring participants remain within their window of tolerance, the optimal arousal zone where learning occurs without triggering threat-based defensive states [10,17], thereby avoiding both anxiety (hyperarousal) and boredom (hypoarousal), which inhibit functional learning.
Functional breathing re-education provides specific techniques for physiological regulation during movement. Practices such as nasal breathing and diaphragmatic activation assist in maintaining sympathovagal balance and supporting autonomic regulation [18]. Research on acute responses to exercise protocols demonstrates that affective experience and perceived exertion vary across different training modalities [19].
Body movement influences emotion regulation through multiple complementary mechanisms. First, physiological: intense, rhythmic movement triggers neurochemical changes in neurotransmitter (serotonin, dopamine), hormone (cortisol), and endocannabinoid levels, thereby reducing anxiety and depression [18]. Second, kinesthetic/somatic: deliberate, mindful modifications of movement quality such as weight distribution, postural adjustments, and breath-informed pacing enhance emotional states through embodied feedback loops and interoceptive awareness [18]. Third, neuropsychological: dance and music activities create flow states (full task engagement with reduced self-referential thinking) mediated by dopaminergic reward systems [20], while also enhancing creative expression, self-confidence, and social connection [21,22].
The central point to this integrated approach is “embodied learning” or “bodyfulness,” where the body is treated as the site of lived experience rather than just an instrument. This approach encourages somatic awareness and regulation, transforming dance into a holistic practice of psychological flexibility [2,3,5]. The phenomenological approach recognizes dance as a process of embodied meaning-making [23,24]. Phenomenology operates as an analytical framework that documents how participants experience neurological and kinesthetic changes during the protocol [25]. This process extends beyond individual development; according to interpersonal neurobiology theory, consciousness emerges as an embodied and relational phenomenon arising through interaction [10].
Within dance contexts, embodied self-awareness provides the foundation for developing reflective capacity. The body becomes the site where reflection originates, merged with empathic connection and fostering interpersonal presence [23]. Technical skill development does not occur in isolation but rather through sustained embodied reflection nested within collaborative movement, group improvisation, and reciprocal perspective-taking [25]. When participants engage in these relational movement experiences, where individuals retain their uniqueness while simultaneously participating in collective expression, learning is catalyzed by recognition of social interdependence and awareness that personal performance contributes to collective accomplishment [3,14]. Research on motor learning demonstrates that social-comparative feedback and collaborative contexts enhance both performance expectancies and learning outcomes [14]. Consequently, technical advancement, emotional resilience, and social integration develop synergistically within an integrated, embodied learning ecology through the coordinated engagement of individual expression, relational attunement and collective coherence [3,14].
Christensen et al. [1] identified six foundational components in recreational dance: rhythm and music, sociality, technique and fitness, connectedness, flow and mindfulness, and esthetic emotions. These components develop emotional regulation through complementary mechanisms like physiological (neurochemical shifts from rhythmic movement), kinesthetic-somatic (interoceptive awareness and embodied feedback), and neuropsychological (flow states and creative expression). Recreational dance, evaluated by how it “feels” rather than how it appears, naturally reduces stress and fosters authentic self-expression in supportive, non-competitive contexts [1]. Social synchrony through group movement engages mirror neuron systems and oxytocin-mediated bonding, while technique mastery demands complex cognitive integration. Critically, while these six components operate synergistically in lived recreational dance practice, current pedagogy rarely systematizes their intentional integration or monitors their psychological effects through rigorous empirical assessment [1].
Despite the potential of dance for well-being, the current literature reveals critical disconnects in pedagogical and neuroscientific application for recreational populations. Existing interventions lack cohesive theoretical frameworks that systematically operationalize neuroscience into dance pedagogy. As Zafeiroudi et al. [3] report, programs are often fragmented, lacking the ability to clearly bridge the gap between abstract somatic theory and concrete teaching methodology. Most concerning is the distinct lack of Randomized Controlled Trials (RCTs) targeting recreational dancers. Research predominantly focuses on clinical populations (therapy) or elite professionals (performance), leaving recreational dancers, who seek well-being and expression, without clear evidence-based guidelines [2,3]. Finally, the existing literature lacks phase-based pedagogical structures that respect the nervous system, progressing from safety establishment to optimal challenge while ensuring participants remain regulated throughout the learning process during dance class.
1.2. Aim and Objectives
The aim of this study is to develop and theoretically justify a comprehensive, 12-week integrated dance-mindfulness protocol grounded in polyvagal theory, motor learning science, and embodied phenomenology. The protocol systematically operationalizes the cultivation of nervous system resilience, technical dance competence, authentic creative expression, and social belonging within structured modern dance theater (Imperial Society of Teachers of Dancing-ISTD syllabus [26]) for community-based adult dancers. The study investigates whether this integrated protocol produces measurable psychological improvements compared to standard dance instruction, and whether participants report enhanced embodied meaning-making and somatic awareness through phenomenological accounts. The specific objectives are:
- (1)
- To develop and operationalize a comprehensive, 12-week integrated dance-mindfulness protocol grounded in neuroscience, motor learning, and embodied phenomenology that systematically integrates theory with practice.
- (2)
- To evaluate the protocol’s effectiveness using a mixed-methods RCT design comparing intervention and control groups on quantitative and qualitative outcomes.
- (3)
- To evaluate the intervention’s effectiveness on psychological well-being and embodied experience.
Based on the theoretical framework and structure of the 12-week intervention, it is hypothesized that participants in the dance mindfulness intervention group will demonstrate significantly greater improvements than those in the control group across primary quantitative outcomes (life satisfaction, subjective happiness, psychological distress, mindful attentional capacity, and leisure involvement) and secondary qualitative outcomes (enhanced somatic awareness, nervous system resilience, technical confidence, creative expression, relational belonging, social connection and embodied meaning-making).
The present protocol is designed for community-based, non-clinical recreational dance classes rather than as a therapeutic program for trauma or other clinical mental health conditions. It targets healthy adult recreational dancers and focuses on supporting everyday psychological wellbeing in the context of regular dance classes. The pedagogical approach aims to foster nervous-system regulation to facilitate learning and flow while maintaining clear professional boundaries: instructors provide structured movement and mindfulness-based cues but do not deliver psychotherapy or intentionally explore traumatic material. If a participant experiences significant emotional distress during a session, their participation in that session is paused and they are referred to external mental health professionals for appropriate clinical support.
2. Experimental Design
2.1. Trial Design
This study has been prospectively registered on ClinicalTrials.gov (NCT07262177; brief title: Dance-Mindfulness Intervention for Well-Being in Recreational Adults-DanceMind) and approved by the institutional Research Ethics Committee (IEC, DPESS, UTH 4-2/2.4.2025; Supplementary File S8 [27]). The protocol follows SPIRIT [28,29], TIDieR [30], and CONSORT standards [31].
This is a two-parallel group randomized controlled trial (RCT). The intervention group receives a 12-week integrated dance-mindfulness protocol grounded in polyvagal theory, motor learning science, and embodied phenomenology. The control group continues regular recreational dance activities without mindfulness or somatic-reflective components. Participants are randomly allocated 2:1 (intervention: control) using computer-generated randomization with allocation concealment.
Quantitative assessments occur at baseline (T0) and post-intervention (T2 Week 12). Qualitative data collection occurs at mid-intervention (T1 Week 8) and post-intervention (T2 Week 12). This mixed-methods design permits concurrent testing of quantitative psychological outcomes (life satisfaction, subjective happiness, psychological distress, mindful attention, leisure involvement) and qualitative embodied experiences (somatic awareness, nervous system resilience, technical confidence, creative expression, relational belonging, meaning-making).
All procedures follow ethical principles outlined in the Declaration of Helsinki. Written informed consent is obtained prior to enrollment. Participants have the right to withdraw at any time without consequence. Personal data are stored securely in encrypted databases. Each participant receives a unique study code; identifying information is separated from research data. All facilitators hold CPR/First Aid certification and mindfulness training. Session checklists document adverse events. If a participant reports intense psychological distress, the study is suspended for that individual with clinical referral provided. Facilitators are trained to recognize signs of emotional dysregulation and provide immediate basic containment (quiet space, grounding breath), without attempting psychological exploration. Control group participants receive delayed access to the intervention after post-intervention assessment (Supplementary Files S1–S8 [27]).
2.2. Study Setting
The study will be conducted across private dance schools in Thessaly, Greece. All baseline (T0) and post-intervention (T2) quantitative assessments will be held in quiet, standardized studio environments at each participating dance school to ensure ecological validity and participant accessibility. All qualitative interviews (T1 Week 8, T2 Week 12) will be conducted in private, quiet locations at the respective dance schools. The 12-week dance-mindfulness intervention will be delivered at the designated dance studios in Thessaly region in Greece. Each studio meets the standardized environmental specifications to ensure consistent and safe delivery across sites (Supplementary File S2 [27]).
2.3. Eligibility Criteria
Participants for this study will be recreational adult dancers aged ≥ 18 years with a minimum of 6 months prior recreational dance experience at community dance schools. Eligible participants must demonstrate capacity for sustained moderate-intensity movement (60 min sessions) and good health with no severe musculoskeletal injuries within the past 2 weeks or intense medical conditions preventing coordinated group movement. Participants must commit to attending at least 70% of sessions (minimum 8 of 12 weeks) and baseline and post-intervention assessments, and be fluent in Greek language (written/verbal).
Exclusion criteria include: (1) active engagement in concurrent mindfulness-based or somatic-movement practices (yoga, Pilates, tai-chi, MBSR programs, etc.), which share theoretical overlap with the intervention’s mindfulness and embodied awareness components and could confound results; (2) severe psychiatric symptomatology requiring clinical psychiatric intervention (hospitalization, crisis stabilization, active suicidality). However, individuals with stable, treated psychiatric conditions are eligible, provided they have been stable on their current medication for a minimum of 6 months and have medical clearance from their treating clinician confirming appropriateness for moderate-intensity physical activity; (3) active substance abuse or dependence (current or within the past 12 months); (4) significant uncorrected hearing or vision impairment affecting the ability to participate in group dance and receive verbal or visual instructions; (5) current pregnancy; (6) acute physical contraindication to movement, including intense musculoskeletal injury occurring within 2 weeks prior to enrollment, severe infection, or uncontrolled cardiovascular event.
Individuals with injuries, mild to moderate, well-controlled chronic medical conditions (e.g., diabetes, hypertension, asthma, arthritis) or stable chronic psychological conditions are not exclusionary if participants provide written medical clearance from their treating physician/clinician confirming capacity for sustained moderate-intensity movement (90–100 min sessions) and documenting any activity modifications required. Severe or poorly controlled chronic conditions are exclusionary and require individual assessment by the principal investigator in consultation with the participant’s clinician.
During preliminary telephone or in-person screening, trained site coordinators conduct structured interviews assessing adherence to inclusion and exclusion criteria. Prospective participants receive a comprehensive eligibility information sheet listing all criteria in accessible language and are invited to self-identify any exclusions or concerns. Those meeting preliminary eligibility criteria (age ≥ 18, minimum 6 months recreational dance experience, availability to attend ≥70% of sessions, Greek language fluency) proceed to formal baseline assessment. Site coordinators maintain a screening log documenting all preliminary screenings, including numbers screened, numbers excluded at each stage, and reasons for exclusion, to enable identification of potential selection bias.
2.4. Sample Size and Recruitment
To determine the appropriate sample size for this study, a power analysis was conducted using GPower 3.1 software [32]. The analysis was based on a repeated-measures design with two groups (experimental and control), with measurements taken at baseline and post-intervention. The following parameters were used: Effect Size (Cohen’s d) = 0.50 (medium effect); Alpha Level (α) = 0.05 (5% significance threshold); Power (1 − β) = 0.80 (80% probability of detecting a true effect); two measurement time points (pre- and post-intervention); and two groups (experimental and control). According to the power analysis, the minimum sample size required to achieve sufficient statistical power is 114 participants, with 38 participants in the control group and 76 in the experimental group.
Participants will be informed about the study through targeted outreach at private recreational dance schools in four cities (Larissa, Trikala, Karditsa, Kalampaka) within the Thessaly region, Greece, with an estimated 1–2 participating schools across these cities. Recruitment methods include flyers, posters, verbal announcements during dance classes, and direct recruitment by dance school directors. Recruitment occurs over an anticipated 1–2 month period, with baseline assessments completed by the end of Month 2. During initial contact, prospective participants receive a participant information sheet detailing study aims, procedures, risks, benefits, confidentiality protections, and withdrawal rights. The information sheet describes the study as “a 12-week integrated modern dance program” without mentioning mindfulness components, to minimize selection bias toward mindfulness-seeking participants. Individuals expressing interest undergo preliminary telephone or in-person screening with a trained site coordinator to assess adherence to inclusion and exclusion criteria (Section 2.3). Those meeting preliminary eligibility criteria are informed of the next steps. Individuals with intense mental health distress or active engagement in concurrent mindfulness-based interventions are offered future participation following symptom resolution or completion of conflicting interventions, rather than immediate exclusion.
Participants proceed to formal baseline assessment (T0), which includes informed consent and administration of quantitative outcome measures (SWLS, DASS-21, MAAS, SHS, LIS; approximately 20–30 min). After completion of baseline assessment (T0), eligible participants are randomly allocated 2:1 (intervention: control) using computer-generated randomization with allocation concealment (administered by an independent data manager not involved in recruitment or assessment). Randomization is conducted via a secure, password-protected electronic system accessible only to the data manager, ensuring that recruitment staff and outcome assessors remain blind to allocation. Following randomization, intervention group participants receive full disclosure of the 12-week dance-mindfulness protocol and provide additional written informed consent confirming understanding of the intervention and commitment to attending the sessions.
Control group participants receive written guidelines regarding their usual recreational dance activities during the 12–week study period, including instructions to exclude concurrent mind–body practices (yoga, Pilates, tai-chi, MBSR programs, etc.). Control group participants are informed that they will have access to the full 12-week dance-mindfulness program at no cost after post-intervention assessment (T2, Week 12), providing equitable delayed intervention access.
Site coordinators maintain a screening log documenting all preliminary screening contacts, including date of screening, recruitment source, preliminary eligibility status (age, dance experience, attendance availability, language fluency), exclusion criteria met (if applicable, specifying which criterion 1–6), clearance documentation status, and disposition (enrolled in baseline assessment, not meeting criteria, awaiting clearance). This log enables complete CONSORT [31] flowchart documentation and allows identification of potential selection bias or recruitment barriers. In the event that randomized participants withdraw or fail to meet attendance criteria (≤70% of sessions), they are retained in all analyses using intention-to-treat methodology. Missing outcome data will be addressed through multiple imputation or last-observation-carried-forward approaches, as appropriate based on data missingness patterns. Replacement participants are not recruited mid-trial, as this would create methodological complications (unbalanced final sample size, potential confounding from replacement timing differences). Final sample size analyzed may differ from target sample size and will be fully documented in the CONSORT compliant participant flowchart, which will be generated upon study completion detailing actual enrollment, randomization, and attrition data by group and reason for withdrawal.
All participants provide written informed consent prior to baseline enrollment. Personal data are handled in strict compliance with the General Data Protection Regulation. All participant identifiers are replaced with unique numeric codes; codebooks linking codes to identifying information are encrypted and stored separately from all research data, accessible only to the principal investigator. Paper materials are stored in locked filing cabinets in restricted-access laboratory space; digital data are stored on secure, password-protected institutional servers with automated daily backups. Data are retained for five years following study completion; paper documents are shredded, and digital data securely deleted thereafter, in accordance with institutional policies and GDPR regulations.
2.5. Measurement Instruments
All quantitative outcome measures are validated for Greek adult populations and administered at baseline (T0) and post-intervention (T2). Qualitative data collection occurs at mid-intervention (T1, Week 8) and post-intervention (T2, Week 12).
The quantitative measurement instruments are presented in the following Table 1.

Table 1.
Quantitative Outcome Measures.
The qualitative data collection instruments will be the following (Supplementary File S3 [27]):
Phenomenological Interview Guide. A semi-structured interview protocol guides qualitative data collection at mid-intervention (T1, Week 8, n~30) and post-intervention (T2, Week 12, n~30). The interview guide contains open-ended questions focused on: (1) embodied experience and somatic awareness (e.g., “Can you describe moments when you felt particularly aware of your body during the sessions?” and “How did your relationship with your breath or bodily sensations evolve across the weeks?”); (2) emotional awareness and regulation (e.g., “What emotional experiences stood out for you during the program?”); (3) movement identity and creative expression (e.g., “How has your relationship with dance or your own movement changed?”); (4) meaning-making and personal insights (e.g., “What meaning did you make from your experiences in the program?” and “Were there moments that connected with your personal life, values, or self-understanding?”); (5) perceived changes like psychological, physical, and social (e.g., “Since the beginning of the program, what changes, if any, have you noticed in yourself?” and “Do you feel different in daily life because of this experience?”); and (6) program structure and safety (e.g., “How did you experience the environment and safety of the sessions?”). Interviews are digitally recorded (after participant consent) and transcribed verbatim for qualitative analysis.
Weekly Journaling Prompts. Participants provide weekly written reflections using standardized prompts distributed at the end of each session (5–10 min per entry). Prompts guide attention to: (1) breath and embodiment (e.g., “Which movements or exercises helped you feel embodied or aware of your internal sensations?”); (2) emotional states and internal reactions (e.g., “Did you notice any shifts in mood, tension, or energy throughout the session?”); (3) awareness of movement and creative exploration (e.g., “Were there moments where movement felt effortless, challenging, playful, or meaningful?”); (4) meaning-making (e.g., “How did today’s experience connect with your life outside the studio?”); and (5) change across sessions (e.g., “Compared to earlier weeks, do you notice any changes in your awareness, emotions, or movement?”). Journals are completed on standardized paper forms, collected weekly, and analyzed for thematic patterns regarding embodied experience, affective change, and perceived transformation.
2.6. Intervention and Control Conditions
The intervention group will consist of participants who attend 12 weekly sessions (90–100 min each) structured across three phases: (1) Foundations (Weeks 1–4), (2) Embodied Exploration (Weeks 5–8), and (3) Expressive Integration (Weeks 9–12). Each session integrates eight standardized components (warm-up/breath grounding, technical dance work, conditioning, mindful break, rhythm/improvisation, choreographed sequences, cool-down/reflective integration, phenomenological journaling). Detailed component descriptions, facilitator language, and session structure are specified in Supplementary File S1 [27].
The control group will consist of participants who continue usual recreational dance activities (preferred modern dance and/or contemporary classes) for 12 weeks, excluding mind–body practices (e.g., yoga, Pilates, tai-chi) that share overlap with the intervention. Control participants do not receive mindfulness training, somatic cuing, or reflective journaling prompts. After post-intervention assessment (T2, Week 12), control participants are offered access to the full 12–week Dance-Mindfulness program at no cost (delayed intervention, ethical equity control).
2.7. Data Collection and Analysis
Self-report questionnaires (SWLS, DASS-21, MAAS, SHS, LIS) are administered on paper at baseline (T0) and post-intervention (T2) by trained site coordinators in quiet studio environments (~20–30 min per assessment). Questionnaires are entered into a secure electronic database with double-entry verification.
Demographic and baseline characteristics are summarized using descriptive statistics (means, standard deviations, medians, frequencies, percentages). Shapiro–Wilk tests and visual inspection (Q-Q plots, histograms) assess normality for all primary outcome variables. Between-group demographic comparisons use independent-samples t-tests (continuous) and chi-square tests (categorical). Internal consistency is assessed using Cronbach’s alpha (α ≥ 0.70); test–retest reliability via intraclass correlation coefficients (ICC ≥ 0.70) in the control group.
If normality is met (Shapiro–Wilk p > 0.05), a 2 (Group) × 2 (Time) mixed-model repeated-measures ANOVA is conducted on each primary outcome, with Bonferroni-corrected α = 0.01 to control Type I error. Alternative testing via MANOVA (Wilks’ Lambda, α = 0.05) proceeds to univariate ANOVAs if significant. ANCOVA with T0 baseline covariates is conducted with Levene’s test assessing homogeneity of variance; if violated (p < 0.05). Effect sizes and 95% confidence intervals are reported.
If normality is violated (Shapiro–Wilk p < 0.05), non-parametric tests will be used: Friedman’s test (within-group time effects), Mann–Whitney U (between-group comparisons), Wilcoxon signed-rank test (within-group pre–post). Post hoc pairwise comparisons use Bonferroni-corrected alpha. Pearson correlations (Bonferroni-corrected) for normally distributed variables; Spearman’s rank-order correlations for non-normal variables. Correlations ≥ |0.30| are highlighted. Quantitative analyses use IBM SPSS v. 28; results are reported per CONSORT guidelines [31] with summary statistics, 95% confidence intervals, and effect sizes. Significance level: α = 0.05 (two-tailed) unless otherwise specified (Bonferroni-corrected α = 0.01).
In qualitative analysis, semi-structured interviews (n~30, T1 Week 8 and T2 Week 12; maximum variation sampling) and weekly journal entries are collected from intervention participants. Interview data are analyzed using Interpretative Phenomenological Analysis (IPA; six-step procedure per [23,40,41] with inter-rater reliability assessed via Cohen’s kappa (κ ≥ 0.70). Weekly journals are analyzed using Reflexive Thematic Analysis [42,43] with phase-specific coding (Weeks 1–4, 5–8, 9–12). Two independent coders conduct all qualitative analysis; discrepancies are resolved through consensus. Analysis examines themes related to embodied awareness, emotional regulation, nervous system resilience, relational presence, and personal transformation (detailed methodology in Supplementary File S3 [27]).
Quantitative measures (both groups, T0–T2) test intervention efficacy; qualitative data (intervention group only) explores embodied mechanisms of change, providing mechanistic understanding complementary to quantitative hypothesis testing.
3. Procedure
The study procedure intervention delivery, and data collection processes across the 12-week trial. All detailed facilitator guidelines, environmental specifications, and data management protocols are documented in Supplementary Files S2 [27]. This section provides a procedural overview; complete procedural specifications appear in Supplementary Materials (Figure 1). Data collection will begin in early January 2026 and conclude in early April 2026. Participant recruitment will be completed by 10 January 2026.
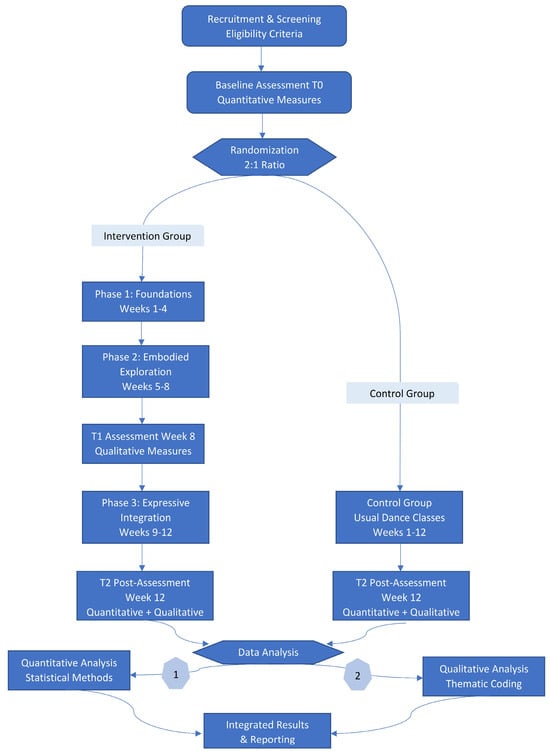
Figure 1.
Study workflow: participant enrollment, randomization, intervention delivery, data collection timeline, and follow-up across the 12–week trial.
Figure 1 presents the complete study workflow across the 12-week trial. It illustrates participant flow from recruitment and baseline assessment (T0) through randomization (2:1 intervention:control), the three-phase intervention structure, mid-point qualitative assessment (T1, Week 8), post-intervention assessments (T2, Week 12), and final mixed-methods analysis combining quantitative and qualitative outcomes.
3.1. Intervention Delivery and Safety Monitoring
Intervention sessions are delivered weekly by trained facilitators holding CPR/First Aid certification and formal mindfulness training (qualifications detailed in Supplementary File S2 [27]). Facilitators maintain standardized session structure per Section 2.6 and detailed protocols in Supplementary File S1 (Intervention Manual) [27]. Attendance and adverse events are documented on standardized checklists completed immediately post-session.
If a participant reports severe psychological distress or adverse effects during a session, the facilitator pauses the activity, provides immediate support in a private setting, and offers clinical referral if indicated. Participation may be suspended pending further evaluation. All safety incidents are documented on incident forms and reported to the principal investigator within 24 h. If a participant reports acute psychiatric symptoms requiring hospitalization, crisis stabilization, or active suicidality, the study is suspended for that individual with clinical referral provided to a local mental health resource.
Intervention fidelity is monitored through: (1) Standardized session checklists documenting component completion, duration, deviations, and engagement level (completed immediately post-session by facilitator); (2) facilitator reflection journals documenting session flow, group atmosphere, facilitator reflections, adaptations, and concerns (reviewed weekly by Principle Investigator-PI); (3) audio recording of approximately 5–10% of sessions (stratified across phases and facilitators) for independent fidelity assessment using structured fidelity observation sheets (detailed in Supplementary File S4 [27]); and (4) monthly facilitator supervision meetings (2 h per month minimum) reviewing fidelity data, addressing participant safety, discussing facilitator well-being, and documenting protocol adaptations. Fidelity assessment occurs at three time points per site (Week 2, Week 6, Week 10) to capture early, mid-course, and late-stage implementation quality.
3.2. Data Collection
Quantitative outcome measures (described in Section 2.5) are administered on paper at baseline (T0) and post-intervention (T2, Week 12). Post-intervention assessments are conducted by trained coordinators/assessors blinded to group allocation; blinding is maintained by: (1) providing assessors only the participant study code (no group information); (2) restricting assessor access to baseline data or randomization records; and (3) ensuring assessors have no knowledge of intervention attendance or session fidelity ratings. Completed questionnaires are entered into a secure electronic with double-entry verification. Missing data patterns are examined; Section 2.7 specifies handling strategies.
Weekly Journaling (Intervention Group Only): Intervention group participants complete standardized written reflections (5–10 min) at the end of each session using prompts addressing: breath/embodiment, emotional states, movement awareness, meaning-making, and perceived changes across weeks (prompts detailed in Supplementary File S3 [27]). Journal forms are collected weekly by facilitators and maintained in secure storage. A purposive sample of journal entries (selected from Weeks 1, 4, 8, and 12, plus entries with maximum phenomenological variation) is analyzed for thematic patterns regarding embodied experience, affective change, and perceived transformation using Reflexive Thematic Analysis with phase-specific coding (Weeks 1–4, 5–8, 9–12; detailed methodology in Supplementary File S3 [27]). Two independent coders will analyze qualitative data using structured coding protocols; differences are resolved through consensus discussion. Control group participants do not complete journaling; they complete quantitative assessments only (T0 and T2).
Semi-Structured Interviews (Intervention Group Subsample): Approximately 30 intervention group participants are selected via maximum variation sampling (Section 2.7). Semi-structured interviews are conducted by trained research staff not involved in intervention delivery at mid-intervention (T1, Week 8) and post-intervention (T2, Week 12) in private, quiet locations at the respective dance schools. Each interview is approximately 20–30 min in duration and is audio recorded after participant consent. The interview guide (Supplementary File S3 [27]) addresses: embodied experience and somatic awareness, emotional awareness and regulation, movement identity and creative expression, meaning-making, perceived changes (psychological, physical, social), and program structure and safety.
Interview data will be analyzed using Interpretative Phenomenological Analysis (IPA) following the six-step procedure [40]: (1) reading and re-reading transcripts; (2) initial line-by-line coding; (3) developing emergent themes within each case; (4) searching for connections across themes within cases; (5) repeating steps 1–4 for each interview independently; and (6) cross-case analysis to identify superordinate themes and patterns (Supplementary File S3 [27]).
3.3. Study’s Intervention Protocol
The 12–week dance mindfulness intervention was structured as a phased, component-based protocol delivered through weekly 90–100 min sessions, organized across three developmental phases (Phase 1: Foundational Weeks 1–4; Phase 2: Embodied Exploration Weeks 5–8; Phase 3: Expressive Integration Weeks 9–12) and comprising eight standardized components designed to integrate nervous system regulation, motor skill development, and embodied meaning-making within ISTD modern dance syllabi [26]. Each session follows the standardized eight-component protocol detailed in Supplementary Files S1 [27]:
- Warm-up and breath grounding (9–10 min);
- Technical dance work (14–15 min);
- Conditioning and strength work with nervous system awareness (9–10 min);
- Break/transition and nervous system settling (4–5 min);
- Rhythm and improvisation (8–9 min);
- Choreographed dance sequences (15–17 min);
- Cool-down and reflective integration (8–9 min);
- Phenomenological journaling (10–20 min, flexible duration).
Component 1: Warm-Up and Breath Grounding (9–10 min).
Component 1 is a 9–10 min warm-up establishing embodied presence and nervous system readiness through progressively complex breath-movement integration across three four-week phases. Phase 1 (Weeks 1–4) establishes parasympathetic baseline through synchronized nasal breathing (4-count pattern) with gentle arm movements, light rhythmic activation, and joint mobility sequences. Nasal breathing activates nitric oxide production in paranasal sinuses, enhancing oxygen utilization and reducing chemosensitivity to CO2, key mechanisms for parasympathetic engagement [18]. Joint mobility and sensory-kinetic awareness develop interoceptive capacity, allowing participants to access sources of evaluation based on felt sensation rather than external perfectionistic criteria [44]
Phase 2 (Weeks 5–8) develops sympathetic–parasympathetic balance by adding coordinated leg extensions, multi-directional stepping (invisible cross patterns), and elevated-heart-rate activities while maintaining nasal breathing. This trains the nervous system to sustain sympathetic mobilization while maintaining parasympathetic baseline, a critical resilience capacity [8,18]. Learning strategies embedded in facilitator cuing support autonomy and reduce perfectionistic cognitions [44].
Phase 3 (Weeks 9–12) achieves embodied automaticity by weaving all movements into one continuous 7–8 min sequence. Participants execute complex motor patterns automatically while maintaining nervous system coherence, demonstrated by steady heart rate, relaxed presence, and uninterrupted nasal breathing. Dance and movement are recognized as neural exercises that shift affective states within a safe context, optimizing mental and physical health [45].
The three-phase progression mirrors motor learning stages [14]: cognitive (Phase 1, conscious effort), associative (Phase 2, coordinated integration), and automatic (Phase 3, effortless execution) (Table 2). Facilitator language continuously signals safety via warm presence and explicit nervous system cuing, activating the social engagement system and supporting parasympathetic dominance throughout [8]. This approach operationalizes vagal efficiency, the dynamic effectiveness of the vagal brake in regulating heart rate and metabolic output to match environmental and situational demands [8,45].
Table 2.
Component 1: Warm-Up and Breath Grounding.
Component 2: Technical Dance Work (14–15 min)
Phase 1 (Grade 2) establishes body literacy (the ability to identify and reference internal sensation) creating an interoceptive foundation for technical development [46]. Dancers learn basic patterns while optimizing motor synergies and reducing unnecessary muscle tension [47]. Phase 2 (Grade 3) deepens proprioceptive awareness through enhanced complexity, operationalizing how explicit and implicit motor sequence learning occur simultaneously [12,13]. Participants consciously recall movements while implicit systems optimize motor efficiency. Facilitator cuing emphasizes interoceptive feedback rather than external form correction [46]. Phase 3 (Grade 4) integrates embodied self-awareness into authentic expression [23]. Complex sequences become vehicles for the dancer’s voice. Transfer learning principles enable Grade 3 to Grade 4 compatibility through shared movement transitions [13], demonstrating that technical mastery emerges from interoceptive awareness, not perfectionistic replication [23] (Table 3).
Table 3.
Component 2: Technical Dance Work.
Component 3: Conditioning and Strength Work (9–10 min).
Phase 1 (Weeks 1–4) develops foundational embodied awareness during light exertion, teaching the nervous system that effort and parasympathetic presence coexist. Participants learn to breathe through work rather than against it, establishing an interoceptive baseline where sensation-awareness precedes physical adaptation [48]. Phase 2 (Weeks 5–8) deepens nervous system flexibility through rhythmic endurance and oscillation between effort and recovery, demonstrating how the body can sustain challenge while maintaining regulatory access [9]. Participants consciously regulate intensity via breath-monitoring while implicit motor systems optimize efficiency. Facilitator cuing shifts from “work harder” to “what is your breath telling you?” Phase 3 (Weeks 9–12) integrates vagal efficiency (the capacity to meet complex demands while maintaining parasympathetic access) through sustained whole-body effort under controlled intensity [9]. Technical strength becomes clear, serving embodied resilience and nervous system coherence [49]. Participants experience, directly, that they can sustain intensity while staying regulated; this shift in neuroception (the nervous system’s implicit detection of safety) is the core mechanism of trauma recovery [9,48] but, here, it enables optimal flow states in recreational movement practice (Table 4).
Table 4.
Component 3: Conditioning and Strength Work.
Component 4: Nervous System Settling and Break (4–5 min).
Phase 1 (Weeks 1–4) establishes parasympathetic reactivation following moderate exertion, teaching the body that intensity naturally resolves into calm. Participants practice sustained parasympathetic engagement through gentle grounding, developing interoceptive confidence in the nervous system’s capacity to self-regulate downward [17]. Phase 2 (Weeks 5–8) deepens parasympathetic recovery through rhythm and vagal tone restoration, demonstrating the nervous system’s oscillatory capacity and the transition from sympathetic arousal to parasympathetic dominance [11]. Heart rate variability (HRV) returns toward baseline as recovery progresses; facilitator cues emphasize interoceptive confirmation of this shift (“Feel your heartbeat slowing… feel your breath deepening…”). Phase 3 (Weeks 9–12) integrates embodied belonging and collective nervous system coherence through co-regulated presence, where participants experience their individual nervous system settling within the group’s shared regulation [10]. This “feeling felt” by the group reinforces the ventral vagal pathway and establishes relational nervous system healing. Recovery is complete when participants’ interoceptive baseline has reset and parasympathetic dominance is confirmed via visible calm and stable breath [19,50] (Table 5).
Table 5.
Component 4: Break/Transition and Nervous System Settling.
Component 5: Rhythm and Improvisation (8–9 min).
Phase 1 (Weeks 1–4) introduces foundational rhythm awareness through structured, minimally improvised movement, establishing intrinsic motivation through novelty and autonomy. Participants explore rhythm within contained parameters, developing felt sense of pulse and timing while maintaining a clear skill-challenge balance [51]. Phase 2 (Weeks 5–8) deepens flow state conditions through guided improvisation with increasing creative autonomy, where implicit learning systems optimize movement generation while attention focuses on embodied expression. Flow emerges when challenge and skill are balanced at moderate-to-high levels; participants experience loss of self-consciousness and merging of action-awareness [20]. Phase 3 (Weeks 9–12) integrates full improvisational engagement with optimally challenging creative tasks, where flow becomes dominant and participants experience absorption, full task engagement with low self-referential thinking [22,51]. Improvisation serves as both an anxiety-reduction tool and a pathway to embodied authenticity; through voluntary creative choices, participants access intrinsic motivation and experience the cascade of neurochemical states (dopamine, norepinephrine activation) that accompany sustained flow [20,21] (Table 6).
Table 6.
Component 5: Rhythm and Improvisation.
Component 6: Choreographed Dance Sequences (15–17 min).
Phase 1 (Weeks 1–4) introduces foundational choreographic learning through motor sequence acquisition, where declarative knowledge (step-by-step instructions) builds individual competence and somatic confidence. Participants develop beta oscillations in motor cortices associated with early learning; movement remains cognitively demanding but increasingly fluent [12]. Phase 2 (Weeks 5–8) deepens motor sequence consolidation through small-group collaborative movement, where implicit learning systems bind individual elements into skilled behavior while attention transitions from “how” to “why” and “with whom.” Ensemble presence emerges as participants experience synchronized nervous systems, inter-brain resonance where individual regulation supports collective coherence [9]. Phase 3 (Weeks 9–12) integrates full choreographic mastery with embodied authenticity, where automaticity permits genuine relational presence and ensemble artistry. Participants experience somatic knowledge acquired through 8 weeks of integrated practice; movement becomes “second nature”, a manifestation of the seven attitudinal factors of mindfulness (non-judging, patience, beginner’s mind, trust, non-striving, acceptance, letting go) embedded in choreography [52]. Ensemble becomes the vehicle for experiencing collective flow, where individual skill-challenge balance within group synchronization produces optimal task engagement and merging of action-awareness [12,15] (Table 7).
Table 7.
Component 6: Dance Sequences and Choreographed Material.
Component 7: Cool-Down and Reflective Integration (8–9 min).
Phase 1 (Weeks 1–4) establishes foundational cool-down through gentle movement and guided body scan, introducing participants to basic interoceptive awareness and parasympathetic settling. The body scan meditation, attending to sensations from feet to crown, activates the “sixth sense” (vertical integration via interoception) while facilitating memory consolidation of the session’s somatic learning through systematic attention to embodied sensation [52,53]. Phase 2 (Weeks 5–8) deepens cool-down through expanded stretching and reflective embodied awareness, where participants develop capacity to notice both sensations and emotions present in the body. Embodied reflection (attending to body phenomenologically through Merleau-Ponty’s lens) reveals how the body is the site where consciousness meets world, where hidden assumptions about our experience can surface through careful, embodied attending [54]. Phase 3 (Weeks 9–12) integrates full reflective embodied practice, where participants experience the seven attitudinal factors of mindfulness through cool-down: non-judging (observing sensations without evaluation), patience (allowing release to unfold), beginner’s mind (approaching body anew each session), trust (in natural settling), non-striving (releasing effort), acceptance (of what arises), and letting go (of tension and narratives) [52]. (Table 8) Neural and relational integration mutually support one another; as participants consolidate somatic memories through body scan and reflective practice, their individual nervous system integration simultaneously enables interpersonal regulation and collective well-being [10,53].
Table 8.
Component 7: Cool-Down and Reflective Integration.
Component 8: Phenomenological Journaling (10–20 min).
Phase 1 (Weeks 1–4) introduces foundational narrative-emotional meaning-making through guided journaling prompts focused on individual nervous system learning: “What did your body discover today?” Participants develop capacity to construct coherent narratives of their sensorimotor experience; writing consolidates learning through repeated re-representation of embodied events as language [55]. Phase 2 (Weeks 5–8) deepens journaling to include relational and emotional integration, where narrative-emotion process markers emerge: participants move from “Same Old Storytelling” (habitual narrative) through “Inchoate Storytelling” (tentative new narratives) toward “Discovery Storytelling” (transformed meaning-making) [56]. Phase 3 (Weeks 9–12) integrates full phenomenological reflection across four dimensions: individual transformation, relational attunement, spatial inhabitation, and social belonging. Participants practice embodied reflective practice, attending to how esthetic experience lived through movement translates into articulated meaning through written reflection [25,57]. Journaling serves as both memory consolidation mechanism (translating implicit motor learning into explicit declarative memory) and meaning-making vehicle where participants construct coherent narratives of their developing sense of self through repeated cycles of embodied experience and reflective articulation [55,58] (Table 9).
Table 9.
Component 8: Phenomenological Journaling.
3.4. Data Security and Management
All quantitative data will be entered into a secure, password-protected electronic database by trained data entry personnel, with range and consistency checks applied. Qualitative interviews are transcribed verbatim by trained transcriptionists, and transcripts are reviewed for accuracy against the audio recording. All participant identifiers are replaced with unique numeric codes; a codebook linking names to participant IDs is encrypted and stored separately from all data, accessible only to the principal investigator.
Paper questionnaires and journaling material are stored in restricted-access, locked filing cabinets at a research laboratory of Applied Leisure Sciences at the Department of Physical Education and Sport Science, University of Thessaly. Only the principal investigator and authorized research assistants have access. All data will be retained for five years following study completion; paper documents are shredded, and digital/audio data are securely deleted thereafter, in accordance with institutional data retention policies and GDPR regulations.
3.5. Intervention Facilitator Qualifications and Training
Intervention sessions are delivered by certified modern dance educators meeting the following minimum qualifications: (1) bachelor’s degree or equivalent certification in dance or somatic movement; (2) minimum two years prior teaching experience with recreational adult populations; (3) formal training in mindfulness-based practices (MBSR certification, 200 h yoga teacher training, or safety-aware somatic training). Trauma-informed training is optional for facilitators with relevant background but not required, as the protocol maintains clear pedagogical boundaries; and (4) current CPR/First Aid certification. Prior to participant contact, each facilitator completes a 12 h standardized training module based on the Intervention Protocol Manual (Supplementary S1 [27]) and participates in 1–2 mock teaching sessions observed by the principal investigator, with written feedback incorporated before first participant session delivery.
Prior to each session, facilitators complete environmental standardization checklists documenting: studio temperature (17–22 °C), illumination (300–500 lux, LED flicker-free), acoustic baseline (≤50 dB), floor conditions (sprung or semi-sprung surface), room dimensions and participant spacing (3.5–4.0 m2 per participant), and confirmation of clear emergency exit pathways and visible first aid kit location (detailed specifications in Supplementary File S2 [27]).
Session attendance is recorded by the facilitator at each weekly session. If a participant misses a session, the site coordinator contacts them within 48 h to understand reasons and reschedule a make-up session if feasible, preferably within the same phase. Participants missing more than two consecutive sessions receive additional follow-up contact to assess barriers and provide support (childcare resources, transportation assistance, schedule accommodation).
Facilitators complete standardized fidelity checklists immediately post-session documenting: completion of all eight components, actual duration of each component, deviations from protocol with justification, participant engagement level, and any adverse events or clinical concerns. Facilitators also maintain a reflective journal after each session documenting session flow, participant engagement, emotional atmosphere, personal reflections on facilitation quality, adaptations made, and any participant concerns. Reflection journals are reviewed weekly during supervision.
Facilitators meet with a designated supervisor (principal investigator or designated research staff) for weekly 1 h supervision sessions (or biweekly if multiple facilitators). Supervision includes fidelity review, problem-solving regarding participant responses or challenges, discussion of participant safety concerns, facilitator well-being and support needs, and any protocol adaptations with documented justification.
3.6. Mid-Intervention Qualitative Assessment (T1, Week 8)
At Week 8, qualitative data collection captures participants’ lived experience at the intervention midpoint, creating a comparative baseline for the post-intervention assessment. A purposive subsample of approximately 30 intervention participants is selected via maximum variation sampling (varying by age, gender, prior experience, and baseline distress). These participants complete a 20–30 min interview exploring six core phenomenological domains (embodied awareness, emotional regulation, nervous system activation, relational connection, meaning-making, and movement confidence). The interview guide (Supplementary File S3) [27] specifically probes shifts in embodied experience attributed to the first two phases (Foundations and Embodied Exploration), allowing for longitudinal tracking of the learning trajectory.
Cumulative weekly journals from Weeks 1 to 8 are collected to form the Phase 1 and Phase 2 dataset. Unlike retrospective interviews, these entries provide real-time, week-by-week accounts of the embodied learning process before the onset of the final Expressive Integration phase (full journaling prompts available in Supplementary File S3 [27]). Control group participants do not engage in interviews or journaling.
3.7. Post-Intervention Assessment (T2, Week 12)
At Week 12, all randomized participants complete the final assessment to evaluate intervention outcomes and longitudinal progression. Both intervention and control groups complete the identical battery of five outcome measures administered at baseline (T0), following standard administration procedures to ensure comparability. The same subsample of participants interviewed at T1 completes a second semi-structured interview (20–30 min). The T2 guide (Supplementary File S3) [27] retains the core phenomenological domains but pivots the inquiry toward integration and transformation. Participants reflect on their trajectory across the full 12-week period, enabling an analysis that compares T1 (midpoint) and T2 (endpoint) narratives to map the developmental arc from early somatic grounding to late-phase creative expression.
Intervention participants complete a final journal entry (Supplementary File S3) [27] specifically designed to export a retrospective comparison between their Week 1 and Week 12 embodied states. This completes the qualitative dataset, which is then stratified into three Phase-aligned segments (Weeks 1–4, 5–8, 9–12) for Reflexive Thematic Analysis (coding framework detailed in Supplementary File S3 [27]).
The qualitative strategy at T2 focuses on triangulation: phase-specific journal themes are cross-referenced with longitudinal interview narratives to construct a mechanistic explanation of embodied change. Control group participants complete only the quantitative assessment, preserving the distinction between outcome evaluation (quantitative/comparative) and process evaluation (qualitative/descriptive).
4. Expected Results
Based on the integrated theoretical framework (polyvagal theory, motor learning science, embodied phenomenology) and the structured 12–week protocol design, the following outcomes are expected:
Quantitative outcomes. Intervention participants are expected to demonstrate significantly greater improvements from baseline to post-intervention compared with controls on primary outcome measures: increased life satisfaction and subjective happiness, decreased psychological distress, and enhanced mindful attentional capacity and leisure involvement. These improvements are hypothesized to reflect the intervention’s integration of nervous system regulation (breath-movement synchronization), embodied awareness practices, and relational belonging within the dance context.
Qualitative outcomes. Phenomenological analysis of interview and journal data is expected to reveal a progressive developmental arc across the three intervention phases. Early-phase reflections are anticipated to center on foundational somatic awareness and nervous system regulation; mid-phase reflections to incorporate relational presence and emotional attunement; and late-phase reflections to synthesize embodied learning, relational connection, and authentic expression into coherent narratives of transformation. Control group reflections are expected to remain focused on conventional dance engagement (technique, enjoyment) without the developmental trajectory or transformational narratives anticipated in the intervention group. Individual variability in response will be examined descriptively to identify participant and contextual factors influencing intervention responsiveness.
5. Discussion
This protocol synthesizes empirical evidence from seven converging research domains to address a significant methodological gap in recreational dance research. Harrison et al. [6] established mindfulness-acceptance-commitment feasibility in professional dancers but revealed limitations in sample size and intervention duration. Christensen et al. [1] identified six fundamental dance components but noted underdeveloped sequencing principles, motivating the present protocol’s three-phase pedagogical structure. Dwarika et al. [59] documented methodological gaps including weak standardization and reporting fidelity. Zafeiroudi et al. [3] conducted a scoping review identifying critical gaps in theoretical integration, incomplete operationalization of intervention components, limited methodological rigor, and variable fidelity monitoring. Marich & Howell [5] established that dance and music are core mechanisms through which mindfulness-based movement produces emotional, spiritual, and psychological benefits. Porges’ polyvagal theory [8,9] provides the neuroscientific foundation for nervous system safety-based learning as a prerequisite for motor skill acquisition. Schmidt et al.’s motor learning science [14] establishes that skill consolidation occurs in phases, aligning the protocol’s three-phase structure with cognitive, associative, and autonomous motor learning stages.
Although the present protocol is grounded in Harrison et al.’s [7] theoretical framework regarding mindfulness-acceptance-commitment interventions in dancers, it differs in three dimensions. The population differs in that Harrison et al. examined 16 professional ballet dancers with limited time for mindfulness practice, whereas the present protocol targets recreational dancers who are motivated by intrinsic satisfaction rather than professional demands. The intervention structure also differs, replacing six standalone 30 min sessions with 12 sessions of 90–100 min with mindfulness embedded directly within structured choreography rather than as parallel practice. The theoretical framework extends substantially by integrating polyvagal theory and motor learning science directly into pedagogical structure and using a broad spectrum of psychological and qualitative measures, and phenomenological interviews for multidimensional assessment, whereas Harrison et al. [7] implemented only the MAC model with athlete-specific measures. Where Harrison et al. [7] found no statistically significant differences attributed to small sample size and brief duration, the present protocol addresses these limitations with 114 participants and doubles the intervention length, with embedded integration expected to enhance adherence and efficacy.
Harrison et al. [7] applied an autonomous Mindfulness-Acceptance-Commitment model originally developed for professionals, whereas the present protocol embeds MAC philosophy within a substantially more comprehensive framework structured around three integrated theoretical components. Polyvagal Theory directs every movement choice and environmental perception through neuroception and the Social Engagement System as the foundation for co-regulated learning. Motor Learning Science guides progressive challenge titration within each participant’s window of tolerance through three hierarchical phases named Foundational, Embodied Exploration, and Expressive Integration, which are designed to maintain nervous system regulation while increasing technical complexity. Embodied Phenomenology operationalizes qualitative assessment through journals and semi-structured interviews incorporating Interpretative Phenomenological Analysis, targeting somatic awareness, nervous system resilience, technical confidence, authentic creative expression, relational belonging, and embodied meaning-making. Through this integration, the protocol develops MAC from a standalone psychological intervention into an indivisible structure threaded through all eight class components, with each movement explicitly linked to neuroscientific rationale and somatic awareness.
Christensen et al. [1] identified six fundamental dance components (rhythm/music, sociality, technique/fitness, connection, flow/mindfulness, esthetic emotions) but noted heterogeneous outcomes across dance styles, suggesting that components alone are insufficient without developmental sequencing. This protocol operationalizes such sequencing through a three-phase structure (Foundations Weeks 1–4, Embodied Exploration Weeks 5–8, Expressive Integration Weeks 9–12), a contribution that develops Christensen’s framework. Importantly, this phased architecture aligns with motor learning science consolidation windows: Phase 1 establishes parasympathetic foundation (cognitive motor learning stage). Based on motor learning principles [14], Phase 2 was designed to span a period optimal for motor memory consolidation, and Phase 3 operationalizes automaticity (autonomous motor learning stage). This theoretical alignment permits empirical testing of motor learning principles within dance pedagogy—a mechanistic investigation that Christensen [1] identified as lacking.
Dwarika et al. [59] identified critical reporting and methodological gaps in dance mental skills interventions: inconsistent intervention duration (6 weeks to 1 year), lack of standardization in content delivery, and weak methodological design overall. This protocol directly addresses these gaps through operationalization of the TIDieR (Template for Intervention Description and Replication) framework [27]. All eight standardized components are documented with facilitator language, duration, environmental specifications, and theoretical grounding. This represents a methodological advancement.
However, the protocol recognize uncertainty regarding polyvagal theory’s neuroanatomical foundations. While polyvagal theory [8] provides the overarching framework for nervous system safety-based learning, recent neuroscientific debate has questioned specific anatomical claims [9]. The protocol operates pragmatically: it operationalizes polyvagal principles (progressive cultivation of parasympathetic tone, nervous system flexibility, and social engagement) as a pedagogical framework, while remaining open to evolving neuroscientific understanding. This permits the protocol’s validity to rest primarily on empirical outcomes rather than neuroanatomical confirmation.
While Zafeiroudi et al. [3] identified ten promising dance-based mindfulness interventions in recreational contexts, this scoping review simultaneously revealed critical gaps: lack of systematic theoretical integration, incomplete operationalization of intervention components, limited methodological rigor in design and outcome measurement, and variable fidelity monitoring. This protocol directly addresses each gap through a theoretically grounded, methodologically rigorous, and systematically monitored approach to recreational dance-mindfulness intervention in adults.
By combining RCT design with TIDieR operationalization, theoretical integration, refined outcome measurement, and proactive fidelity monitoring, this protocol advances the field from exploratory pilots and qualitative case studies toward systematic, replicable, evidence-based dance-mindfulness pedagogy. The results will provide the empirical foundation needed to establish recreational dance-mindfulness as a validated, standardized, and scalable approach to supporting psychological well-being, embodied awareness, and authentic self-expression in community populations.
The protocol combines quantitative hypothesis testing (does the intervention improve psychological outcomes?) with qualitative phenomenological exploration (how do participants experience embodied transformation?) and qualitative data comprise semi-structured interviews analyzed via Interpretative Phenomenological Analysis (IPA) [40,41], plus weekly journaling analyzed via Reflexive Thematic Analysis [42,43] with phase-specific coding. This dual approach addresses Christensen’s [1] observation that what exactly is driving positive effects remains unclear in dance research. Of ten studies in Zafeiroudi et al.’s [3] review, only three employed mixed methods; most were purely quantitative or purely qualitative. This protocol’s simultaneous hypothesis-testing and mechanistic exploration is rare in recreational dance research.
This protocol includes comprehensive within-intervention assessment (T0, T1, T2 spanning all three motor learning phases) with weekly journaling documenting embodied progression. However, the protocol lacks post-intervention follow-up assessment beyond Week 12 to evaluate behavioral maintenance and sustained effects. While motor learning consolidation occurs within 6–12 weeks [14], generalization to daily life requires follow-up at 3, 6, 12 months post-intervention. Future research must employ extended follow-up protocols to establish sustainability, directly addressing Duberg et al.’s [60] evidence for maintained effects at 20 months.
While Marich & Howell [5] identified dance and music as core therapeutic mechanisms and Porges [8] emphasizes nervous system dysregulation as the underlying pathology, this protocol lacks direct psychophysiological assessment. The present protocol prioritizes accessibility and scalability (no biomarkers) at the expense of mechanistic clarity.
Christensen [1] documented substantial variation in dance modality effects (e.g., Argentine Tango reduces Parkinson symptoms; Waltz does not), suggesting that dance style is a critical moderating variable. This protocol specifies ISTD modern dance within Greek recreational settings. Generalizability to other dance styles, geographic contexts, socioeconomic populations, or cultural adaptations is limited [3,61]. Comparative research examining this protocol’s model against yoga and tai-chi and other mind–body movement is critical for understanding whether common pedagogical principles (phase-based nervous system scaffolding, motor learning optimization, somatic reflection) generalize across embodied traditions and should be added in future research.
The protocol’s structured design offers significant advantages for educational and community implementation. Universities could integrate this model into recreation curricula, repositioning dance toward comprehensive well-being practice. High schools could adapt it for health curricula. Community centers could deliver this protocol with modest facilitator training (12 h standardized module). Dance educators increasingly pursue MBSR teacher certification (intensive), yoga teacher training (200 h), or trauma-informed somatic training, credentials that naturally dovetail with this protocol. The protocol positions evidence-based embodied practice as implementable in understaffed community settings where clinical providers are unavailable, while maintaining rigor through explicit fidelity monitoring.
This evidence base, demonstrating that systematic nervous system development combined with motor learning, somatic reflection, and relational engagement produces measurable psychological improvements, carries implications extending beyond dance. Additionally, the integrative model could adapt for recreational yoga (sequencing poses across three phases: parasympathetic establishment, technical refinement, esthetic exploration), tai-chi and qigong (systematizing existing contemplative structure), and Pilates (operationalizing nervous system principles underlying practice). The contribution demonstrates that underlying pedagogical structures (phase-based nervous system scaffolding, motor learning optimization, somatic inquiry, relational attunement) may optimize outcomes across practices.
University wellness programs could implement this protocol with undergraduate peer educators, providing cost-effective, evidence-based intervention aligned with return-on-investment metrics (improved life satisfaction, reduced psychological distress, enhanced attention, increased leisure involvement translating into improved productivity and retention). For clinical and community mental health, this protocol demonstrates that recreational embodied practice produces measurable psychological benefits without clinical diagnosis framing, addressing Zhang and Wei’s [4] observation that movement-based approaches leverage mind–body connection but often lack rigorous evidence. This positions evidence-based embodied practice as prevention/well-being promotion complementing (not replacing) clinical treatment, with implications for health equity.
6. Conclusions
This protocol outlines a comprehensive, evidence-informed 12-week integrated dance-mindfulness intervention designed to systematically operationalize polyvagal theory, motor learning science, somatic education, and embodied phenomenology into coherent pedagogical practice. Grounded in principles of progressive nervous system development, technical skill optimization, and relational attunement, the proposed three-phase framework addresses a critical gap in recreational dance education by bridging abstract neuroscientific theory and concrete teaching methodology. The intervention responds to what recreational dancers authentically seek: nervous system resilience, embodied confidence, authentic creative expression, and social belonging—motivations that are largely absent from both clinical and elite professional dance research.
If supported by future data, this approach may offer a replicable and adaptable model for transforming recreational dance from technical skill development alone toward a comprehensive well-being practice grounded in contemporary neuroscience and embodied meaning-making. Beyond recreational dance, findings will inform contemplative movement education broadly (yoga, tai-chi, Pilates, qigong) and clarify scalability across educational, community, and clinical settings, with implications for integrating neuroscience-informed embodied practice into diverse organizational contexts. This protocol contributes to evidence-based pedagogical innovation by demonstrating that systematic integration of nervous system regulation, motor learning, somatic reflection, and relational engagement produces superior psychological and embodied outcomes compared to traditional dance instruction alone, fundamentally advancing how movement education serves adult psychological well-being and authentic self-expression.
Supplementary Materials
The following supporting information can be downloaded at: https://doi.org/10.5281/zenodo.18713796 [27], Supplementary File S1: Intervention Protocol Manual; Supplementary File S2: Facilitator Guidelines and Safety Standard Operating Procedures (SOP); Supplementary File S3: Journaling Prompts & Interview Guide. Qualitative Coding Framework; Supplementary File S4: Fidelity Tools; Supplementary File S5: Consent Form; Supplementary File S6: TIDieR Checklist; Supplementary File S7: SPIRIT Checklist; Supplementary File S8: Ethics Committee Approval Documentation.
Author Contributions
Conceptualization, A.Z.; methodology, A.Z.; software, A.Z., I.T. and C.K.; validation, A.Z., I.T. and C.K.; formal analysis, A.Z.; investigation, A.Z., I.T. and C.K.; resources, A.Z., I.T. and C.K.; data curation, A.Z. and C.K.; writing—original draft preparation, A.Z.; writing—review and editing, A.Z., I.T. and C.K.; visualization, A.Z.; supervision, A.Z.; project administration, A.Z. All authors have read and agreed to the published version of the manuscript.
Funding
No external funding was received for this study. Internal support provided by University of Thessaly (publication fee support; Protocol No. 37931/25/GP).
Institutional Review Board Statement
The study protocol has been reviewed and approved by the Internal Ethics Committee (IEC) of the Department of Physical Education and Sport Science (DPESS), University of Thessaly, (1-2/4.6.2025, Protocol Number.: 2581), and is registered with ClinicalTrials.gov (registration number: NCT07262177) with the brief title “Dance-Mindfulness Intervention for Well-Being in Recreational Adults-DanceMind”. The study will be conducted in full accordance with the ethical principles outlined in the Declaration of Helsinki and complies with the applicable national and European data protection laws. All participants will provide written informed consent prior to their involvement, and personal information will be handled confidentially in accordance with the General Data Protection Regulation.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author, due to ethical and privacy reasons.
Acknowledgments
The research is conducted in the operating framework of the University of Thessaly Innovation, Technology Transfer Unit and Entrepreneurship Center “One Planet Thessaly”, under the “University of Thessaly Grants for Scientific Publication Support” action and is funded by the Special Account of Research Grants of the University of Thessaly.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CONSORT | Consolidated Standards of Reporting Trials |
| CPR | Cardiopulmonary Resuscitation |
| DASS-21 | Depression Anxiety Stress Scales-21 |
| dB | Decibels (sound level) |
| DPESS | Department of Physical Education and Sport Science |
| GDPR | General Data Protection Regulation |
| Hz | Hertz (frequency) |
| ICC | Intraclass Correlation Coefficient |
| IEC | Internal Ethics Committee |
| IRB | Institutional Review Board |
| IPA | Interpretative Phenomenological Analysis |
| ISTD | Imperial Society of Teachers of Dancing |
| LIS | Leisure Involvement Scale |
| lux | Lux (illumination measurement) |
| MAAS | Mindful Attention Awareness Scale |
| MBSR | Mindfulness-Based Stress Reduction |
| P1 | Phase 1 (Weeks 1–4) |
| P2 | Phase 2 (Weeks 5–8) |
| P3 | Phase 3 (Weeks 9–12) |
| PI | Principle Investigator |
| PVT | Polyvagal Theory |
| RCT | Randomized Controlled Trial |
| RTA | Reflexive Thematic Analysis |
| S1–S8 | Supplementary Files S1–S8 |
| SHS | Subjective Happiness Scale |
| SPA | Sensation, Perspective, Agency |
| SPIRIT | Standard Protocol Items: Recommendations for Interventional Trials |
| SWLS | Satisfaction With Life Scale |
| T0 | Baseline assessment (Week 0) |
| T1 | Mid-intervention assessment (Week 8) |
| T2 | Post-intervention assessment (Week 12) |
| TIDieR | Template for Intervention Description and Replication |
| UTH | University of Thessaly |
References
- Christensen, J.F.; Vartanian, M.; Sancho-Escanero, L.; Khorsandi, S.; Yazdi, S.H.N.; Farahi, F.; Borhani, K.; Gomila, A. A Practice-Inspired Mindset for Researching the Psychophysiological and Medical Health Effects of Recreational Dance (Dance Sport). Front. Psychol. 2021, 11, 588948. [Google Scholar] [CrossRef] [PubMed]
- Zafeiroudi, A.; Karagiorgos, T.; Tsartsapakis, I.; Grivas, G.V.; Kouthouris, C.; Goulimaris, D. Choreographing Well-Being: The Predictive Role of Self-Compassion on Life Satisfaction—A Therapeutic-Based Art Pedagogy Perspective in Recreational Dance. Sports 2025, 13, 223. [Google Scholar] [CrossRef] [PubMed]
- Zafeiroudi, A.; Tsartsapakis, I.; Trigonis, I.; Kouli, O.; Goulimaris, D.; Kouthouris, C. Embodied Mindfulness Through Movement: A Scoping Review of Dance-Based Interventions for Mental Well-Being in Recreational Populations. Healthcare 2025, 13, 2230. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wei, Y. The Role of Dance Movement Therapy in Enhancing Emotional Regulation: A Literature Review. Heliyon 2024, 10, e35733. [Google Scholar] [CrossRef]
- Marich, J.; Howell, T. Dancing Mindfulness: A Phenomenological Investigation of the Emerging Practice. Explore 2015, 11, 346–356. [Google Scholar] [CrossRef]
- Harrison, C. Exploring Wellness: A Self-Report Monitoring Application and Mindfulness Intervention for Professional Ballet Dancers. Ph.D. Thesis, La Trobe University, Victoria, Australia, 2021. [Google Scholar]
- Harrison, C.; Ruddock, S.; Mayes, S.; Cook, J.; O’Halloran, P.; Ferrar, K.; Li, X.; Ruddock, M. A 6-Week Mindfulness-Acceptance-Commitment Intervention to Improve Professional Ballet Dancers’ Psychological States Around Performance. J. Danc. Med. Sci. 2025, 29, 67–76. [Google Scholar] [CrossRef]
- Porges, S.W. Polyvagal Theory: A Science of Safety. Front. Integr. Neurosci. 2022, 16, 871227. [Google Scholar] [CrossRef]
- Porges, S.W. POLYVAGAL THEORY: CURRENT STATUS, CLINICAL APPLICATIONS, AND FUTURE DIRECTIONS. Clin. Neuropsychiatry 2025, 22, 175–191. [Google Scholar] [CrossRef]
- Siegel, D.J.; Drulis, C. An Interpersonal Neurobiology Perspective on the Mind and Mental Health: Personal, Public, and Planetary Well-Being. Ann. Gen. Psychiatry 2023, 22, 5. [Google Scholar] [CrossRef]
- Weissman, D.G.; Mendes, W.B. Correlation of Sympathetic and Parasympathetic Nervous System Activity during Rest and Acute Stress Tasks. Int. J. Psychophysiol. 2021, 162, 60–68. [Google Scholar] [CrossRef]
- Dyck, S.; Klaes, C. Training-Related Changes in Neural Beta Oscillations Associated with Implicit and Explicit Motor Sequence Learning. Sci. Rep. 2024, 14, 6781. [Google Scholar] [CrossRef] [PubMed]
- Dyck, S.; Klaes, C. Faster Implicit Motor Sequence Learning of New Sequences Compatible in Terms of Movement Transitions. Npj Sci. Learn. 2025, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.A.; Lee, T.D.; Winstein, C.; Wulf, G.; Zelaznik, H.N. Motor Control and Learning: A Behavioral Emphasis, 6th ed.; Human Kinetics: Champaign, IL, USA, 2019. [Google Scholar]
- Abuhamdeh, S. Investigating the “Flow” Experience: Key Conceptual and Operational Issues. Front. Psychol. 2020, 11, 158. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A. Csikszentmihalyi, Mihaly. (1990). Flow: The Psychology of Optimal Experience. J. Leis. Res. 1992, 24, 93–94. [Google Scholar] [CrossRef]
- Larsen, K.L.; Stanley, E.A. Leaders’ Windows of Tolerance for Affect Arousal—And Their Effects on Political Decision-Making During COVID-19. Front. Psychol. 2021, 12, 749715. [Google Scholar] [CrossRef]
- McKeown, P. The Breathing Cure: Develop New Habits for a Healthier, Happier, and Longer Life; Humanix Books: West Palm Beach, FL, USA, 2021. [Google Scholar]
- Benítez-Flores, S.; Magallanes, C.A.; Alberton, C.L.; Astorino, T.A. Physiological and Psychological Responses to Three Distinct Exercise Training Regimens Performed in an Outdoor Setting: Acute and Delayed Response. J. Funct. Morphol. Kinesiol. 2021, 6, 44. [Google Scholar] [CrossRef]
- van der Linden, D.; Tops, M.; Bakker, A.B. Go with the Flow: A Neuroscientific View on Being Fully Engaged. Eur. J. Neurosci. 2021, 53, 947–963. [Google Scholar] [CrossRef]
- Bond, K. (Ed.) Dance and the Quality of Life; Springer International Publishing: Cham, Switzerland, 2019; Volume 73, ISBN 978-3-319-95698-5. [Google Scholar]
- Heasman-Cossins, C.; Winter, D.; Juncos, D. Using Vocal Improvisation Within the Vocal Coaching Studio to Mitigate Music Performance Anxiety: An Exploratory Study of Three Cases. Music Sci. 2025, 8, 20592043251327047. [Google Scholar] [CrossRef]
- Braun, N.; Kotera, Y. Influence of Dance on Embodied Self-Awareness and Well-Being: An Interpretative Phenomenological Exploration. J. Creat. Ment. Health 2022, 17, 469–484. [Google Scholar] [CrossRef]
- Picard, K. An Investigation into Learning and Development Associated with Embodied Mindfulness. Doctoral Dissertation, Lesley University, Cambridge, MA, USA, 2018. [Google Scholar]
- Schwender, T.M.; Rudi, H.; Stortz, S. Creating, Framing, Reflecting—Dance as Embodied Reflective Practice in Professional Development for Physical Education Teachers. Front. Educ. 2025, 10, 1542371. [Google Scholar] [CrossRef]
- Imperial Society of Teachers of Dancing. Modern Theatre [Grade Level] Examination Specification; ISTD Publications: London, UK, 2004. [Google Scholar]
- Zafeiroudi, A. Supplementary Files for: Mindful Embodied Movement—A 12-Week Modern Dance-Mindfulness Intervention and Mixed-Methods Randomized Controlled Trial in Recreational Adult Dancers_ Revised 2.0, [Data Set]. Zenodo 2025. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.-W.; Boutron, I.; Hopewell, S.; Moher, D.; Schulz, K.F.; Collins, G.S.; Tunn, R.; Aggarwal, R.; Berkwits, M.; Berlin, J.A.; et al. SPIRIT 2025 Statement: Updated Guideline for Protocols of Randomised Trials. BMJ 2025, 389, e081477. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. J. Clin. Epidemiol. 2010, 63, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Lyrakos, G.N.; Xatziagelaki, E.; Papazafiropoulou, A.K.; Batistaki, C.; Damigos, D.; Mathianakis, G.; Bousboulas, S.; Spinaris, V. 1439 – Translation And Validation Study Of The Satisfaction With Life Scale (Swls) In Greek General Population, Diabetes Mellitus And Patients With Emotional Disorders. Eur. Psychiatry 2013, 28, 28-E759. [Google Scholar] [CrossRef]
- Pezirkianidis, C.; Karakasidou, E.; Lakioti, A.; Stalikas, A.; Galanakis, M. Psychometric Properties of the Depression, Anxiety, Stress Scales-21 (DASS-21) in a Greek Sample. Psychology 2018, 9, 2933–2950. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. Mindful Attention Awareness Scale (MAAS). J. Pers. Soc. Psychol. 2003, 85, 1–20. [Google Scholar] [CrossRef]
- Mantzios, M.; Wilson, J.C.; Giannou, K. Psychometric Properties of the Greek Versions of the Self-Compassion and Mindful Attention and Awareness Scales. Mindfulness 2015, 6, 123–132. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Lepper, H.S. A Measure of Subjective Happiness: Preliminary Reliability and Construct Validation. Soc. Indic. Res. 1999, 46, 137–155. [Google Scholar] [CrossRef]
- Karakasidou, E.; Pezirkianidis, C.; Stalikas, A.; Galanakis, M. Standardization of the Subjective Happiness Scale (SHS) in a Greek Sample. Psychology 2016, 07, 1753–1765. [Google Scholar] [CrossRef]
- Theodorakis, N.D.; Panopoulou, K.; Vlachopoulos, S. Factor Structure and Predictive Ability of the Recreation Involvement Scale. Inq. Sport Phys. Educ. 2007, 5, 405–413. [Google Scholar]
- Smith, J.A.; Flower, P.; Larkin, M. Interpretative Phenomenological Analysis: Theory, Method and Research; Sage: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Smith, J.A.; Fieldsend, M. Interpretative Phenomenological Analysis. In Qualitative Research in Psychology: Expanding Perspectives in Methodology and Design, 2nd ed.; American Psychological Association: Washington, DC, USA, 2021; pp. 147–166. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on Reflexive Thematic Analysis. Qual. Res. Sport. Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Hayfield, N.; Davey, L.; Jenkinson, E. Doing Reflexive Thematic Analysis. In Supporting Research in Counselling and Psychotherapy; Springer International Publishing: Cham, Switzerland, 2022; pp. 19–38. [Google Scholar]
- Karin, J.; Nordin-Bates, S.M. Enhancing Creativity and Managing Perfectionism in Dancers Through Implicit Learning and Sensori-Kinetic Imagery. J. Danc. Educ. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Eichhorn, N. Polyvagal Perspectives: Interventions, Practices, and Strategies. Body Mov. Dance Psychother. 2025, 20, 337–340. [Google Scholar] [CrossRef]
- Price, C.J.; Hooven, C. Interoceptive Awareness Skills for Emotion Regulation: Theory and Approach of Mindful Awareness in Body-Oriented Therapy (MABT). Front. Psychol. 2018, 9, 798. [Google Scholar] [CrossRef]
- Bläsing, B.; Calvo-Merino, B.; Cross, E.S.; Jola, C.; Honisch, J.; Stevens, C.J. Neurocognitive Control in Dance Perception and Performance. Acta Psychol. 2012, 139, 300–308. [Google Scholar] [CrossRef]
- Neufeld, A.T. The Body, Mind, and Trauma: A Case for Trauma-Sensitive Somatic Mindfulness Somatic Mindfulness. Master’s Thesis, Lesley University, Cambridge, MA, USA, 2024. [Google Scholar]
- Payne, P.; Levine, P.A.; Crane-Godreau, M.A. Somatic Experiencing: Using Interoception and Proprioception as Core Elements of Trauma Therapy. Front. Psychol. 2015, 6, 93. [Google Scholar] [CrossRef]
- Pradhapan, P.; Tarvainen, M.P.; Nieminen, T.; Lehtinen, R.; Nikus, K.; Lehtimäki, T.; Kähönen, M.; Viik, J. Effect of Heart Rate Correction on Pre-and Post-Exercise Heart Rate Variability to Predict Risk of Mortality-an Experimental Study on the FINCAVAS Cohort. Front. Physiol. 2014, 5, 208. [Google Scholar] [CrossRef]
- Waterman, A.S. On Intrinsic Motivation, Flow, and Absorption: A New Theoretical Perspective. J. Posit. Psychol. 2025, 20, 644–651. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-Based Stress Reduction (MBSR). Constr. Human Sci. 2003, 8, 73–107. [Google Scholar]
- Paller, K.A. Memory Consolidation: Systems. In Encyclopedia of Neuroscience; Academic Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Botelho, N. Reflection in Motion: An Embodied Approach to Reflection on Practice. Reflective Pract. 2021, 22, 147–158. [Google Scholar] [CrossRef]
- Wiggins, G.A.; Sanjekdar, A. Learning and Consolidation as Re-Representation: Revising the Meaning of Memory. Front. Psychol. 2019, 10, 802. [Google Scholar] [CrossRef]
- Aleixo, A.; Pires, A.P.; Angus, L.; Neto, D.; Vaz, A. A Review of Empirical Studies Investigating Narrative, Emotion and Meaning-Making Modes and Client Process Markers in Psychotherapy. J. Contemp. Psychother. 2021, 51, 31–40. [Google Scholar] [CrossRef]
- Tembrioti, L.; Tsangaridou, N. Reflective Practice in Dance: A Review of the Literature. Res. Danc. Educ. 2014, 15, 4–22. [Google Scholar] [CrossRef]
- Carbone, J.; Diekelmann, S. An Update on Recent Advances in Targeted Memory Reactivation during Sleep. Npj Sci. Learn. 2024, 9, 31. [Google Scholar] [CrossRef]
- Dwarika, M.S.; Quinton, M.L.; Nordin-Bates, S.; Cumming, J. Characteristics of Mental Skills Interventions in Dance: A Mixed Methods Systematic Review Protocol. BMJ Open 2024, 14, e086345. [Google Scholar] [CrossRef]
- Duberg, A.; Hagberg, L.; Sunvisson, H.; Möller, M. Influencing Self-Rated Health among Adolescent Girls with Dance Intervention: A Randomized Controlled Trial. Arch. Pediatr. Adolesc. Med. 2013, 167, 27–31. [Google Scholar] [CrossRef]
- Zafeiroudi, A.; Goulimaris, D.; Alexandris, K.; Yfantidou, G. Segmenting Recreational Dance Communities in Greece: Cultural Identity, Lifelong Engagement, and Inclusive and Participant-Centered Approaches to Dance Programming. Societies 2025, 15, 239. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.