

Newborn Screening Long-Term Follow-Up Clinics (Continuity Clinics) in the Philippines during the COVID-19 Pandemic: Continuing Quality Patient Care
 , ,
, ,  and
and
Abstract
1. Introduction
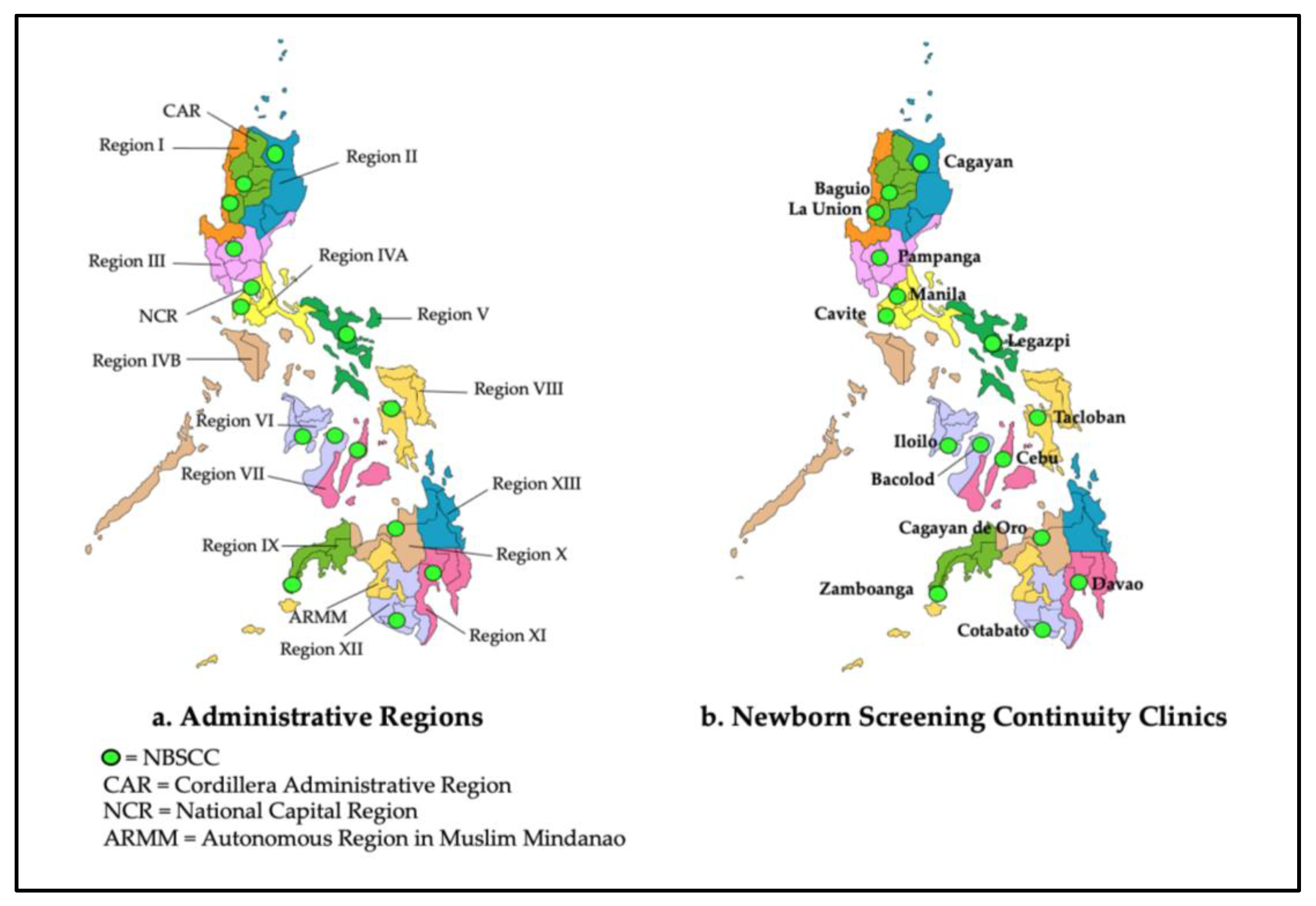
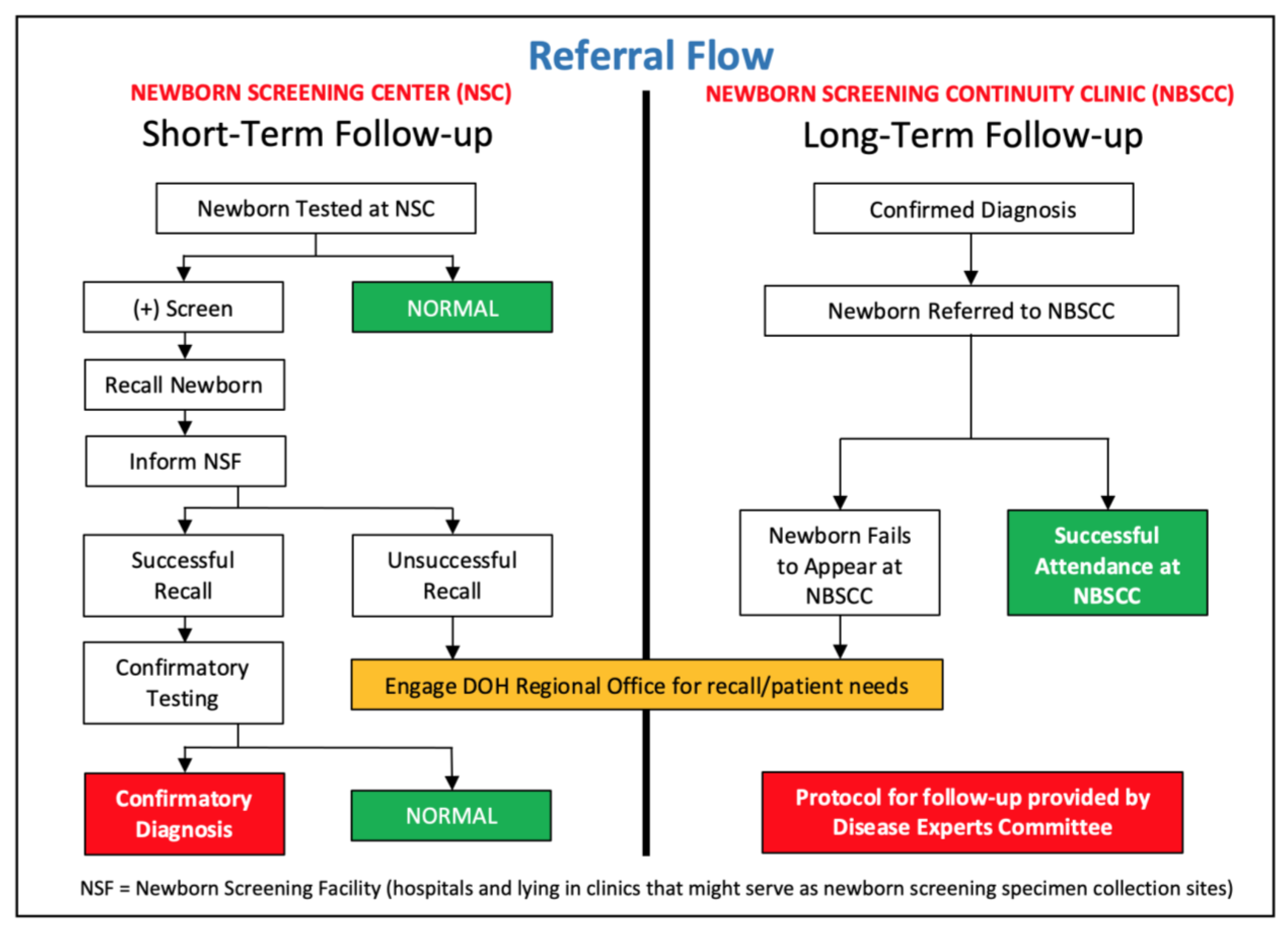
1.1. The Philippine Newborn Screening Program
1.2. The COVID-19 Pandemic
2. Materials and Methods
3. Results
3.1. Challenges to the NBSCC’s Operational Capacity
3.2. Challenges with Patient Communications
3.3. Challenges to Health Staff and Patient Safety
3.4. NBSCC Statistics
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAH | Congenital adrenal hyperplasia |
| CH | Congenital hypothyroidism |
| CHD | Center for Health Development |
| COVID-19 | Coronavirus Disease 2019 |
| DOH | Department of Health |
| NBS | Newborn bloodspot screening |
| NBSCC | Newborn screening continuity clinic (long-term follow-up) |
| NSC | Newborn Screening Center (screening laboratory) |
| NSF | Newborn Screening Facility (screening specimen collection site) |
| PNSP | Philippine Newborn Screening Program |
References
- Padilla, C.D.; Domingo, C.F. Implementation of newborn screening in the Philippines. Philipp. J. Pediatr. 2002, 51, 2–10. [Google Scholar]
- Padilla, C. Newborn screening in the Philippines. Southeast Asia J. Trop. Med. Public Health 2003, 34 (Suppl. 3), 87–88. [Google Scholar]
- Therrell, B.L. US newborn screening policy dilemmas for the twenty-first century. Mol. Genet. Metab. 2001, 74, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Administrative Order 2014-0035—Implementing Guidelines on the Setting-Up of Newborn Screening Continuity Clinics. Available online: https://newbornscreening.ph/images/stories/ResourcesDOHPolicies/AO%20No.%202014-0035.pdf (accessed on 2 September 2020).
- Padilla, C.D.; Therrell, B.L.; Panol, K.A.R.; Suarez, R.C.N.; Reyes, M.E.L.; Jomento, C.M.; Maceda, E.B.G.; Lising, J.A.C.; Beltran, F.D.E.; Orbillo, L.L. Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in newborn screening system quality. Int. J. Neonatal Screen. 2020, 6, 95. [Google Scholar] [CrossRef] [PubMed]
- Newborn Screening Reference Center. Manual of Operations for Newborn Screening Continuity Clinics. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/nbsccmanops.pdf (accessed on 17 October 2022).
- Department of Health—National Center for Disease Prevention and Control. Memorandum on Newborn Screening Grant for Pediatric Endocrinologists and Clinical Geneticists. Available online: https://newbornscreening.ph/images/stories/ResourcesDOHPolicies/doh.newborn%20screening%20grant%20for%20pediatric%20endocrinologists%20and%20clinical%20geneticists.pdf (accessed on 17 October 2022).
- World Health Organization. WHO Characterizes COVID-19 as a Pandemic. 31 July 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 2 September 2020).
- Legaspi, G.D.; Omar, A.T., 2nd; Baticulon, R.E.; Salonga, A.E.M.; Gaddi, M.J.S.; Hong, M.A.C.; Seng, K.S.; Khu, K.J.O. Letter to the Editor “Service and Training during the COVID-19 Pandemic: Perspectives from a Neurosurgical Center in the Philippines”. World Neurosurg. 2020, 139, 741–743. [Google Scholar] [CrossRef] [PubMed]
- Amit, A.M.L.; Pepito, V.C.F.; Dayrit, M.M. Early response to COVID-19 in the Philippines. West. Pac. Surveill. Response J. 2021, 12, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Dancel, R. The Straits Times. Cebu City Looms as Philippines’ New COVID-19 Epicentre. Available online: https://www.straitstimes.com/asia/se-asia/cebu-city-looms-as-philippines-new-covid-19-epicentre (accessed on 22 November 2022).
- Cole, B. National Academy of Social Insurance. The Impact of the Covid-19 Pandemic on access to health care. Health Policy Brief. 2020, 17, 1–31. [Google Scholar]
- Hirabayashi, K.; UNICEF East Asia and Pacific. The Impact of COVID-19 on Routine Vaccinations. Available online: https://www.unicef.org/eap/stories/impact-covid-19-routine-vaccinations (accessed on 22 November 2022).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Tumulak, M.J.R.; Pascua, A.V.; Jover, E.J.M.; Guerbo, R.J.; Canoy, G.M.R.; Laurino, M.Y. Genetic counseling in the time of COVID-19: The Philippine experience with telegenetics. J. Genet. Couns. 2021, 30, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Padilla, C.D.; Therrell, B.L., Jr.; Alcausin, M.M.L.B.; de Castro, R.C., Jr.; Gepte, M.B.P.; Reyes, M.E.L.; Jomento, C.M.; Suarez, R.C.N.; Maceda, E.B.G.; Abarquez, C.G.; et al. Successful implementation of newborn screening for hemoglobin disorders in the Philippines. Int. J. Neonatal Screen. 2021, 7, 30. [Google Scholar] [CrossRef] [PubMed]
- Padilla, C.D.; Therrell, B.L., Jr.; Alcausin, M.M.L.B.; Chiong, M.A.D.; Abacan, M.A.R.; Reyes, M.E.L.; Jomento, C.M.; Dizon-Escoreal, M.T.T.; Canlas, M.A.E.; Abadingo, M.E.; et al. Successful implementation of expanded newborn screening in the Philippines using tandem mass spectrometry. Int. J. Neonatal Screen. 2022, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Newborn Screening Reference Center. Newborn Screening Statistics: National Coverage 2021. Available online: https://newbornscreening.ph/index.php?option=com_content&view=article&id=83:nbs-statistics&catid=32:statistics&Itemid=57 (accessed on 21 December 2022).



{kind=link}
{kind=link}
| Category | Year | |||
|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2021 | |
| Annual number of endorsed newborns (referred from NSCs) | 459 | 476 | 1171 | 643 |
| Cumulative endorsed newborns (long-term care monitoring) | 4229 | 4705 | 5876 | 6519 |
| Annual number of expired cases (died while in long-term care) | 10 | 22 | 46 | 17 |
| Annual number discharged (diagnosed clinically normal) | 17 | 18 | 29 | 8 |
| Actual newborn census [endorsed − (expired + discharged)] | 3991 | 4427 | 5523 | 6141 |
| Number contacted (contact with patient made within 6 months) | 2819 | 3107 | 4138 | 4717 |
| Percentage contacted [(number contacted/actual census) × 100%] | 70.6% | 70.2% | 74.9% | 76.8% |
| Annual unresponsive patients (patient contact lost for over 6 months) | 304 | 148 | 65 | 39 |
| Challenges | Strategies |
|---|---|
| Limited or complete disruption of clinic hours |
|
| Distribution of medical food, supplies, and medicine |
|
| Safety of both NBSCC staff and patients during face-to-face consultations |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maceda, E.B.G.; Abadingo, M.E.; Panol, K.A.R.; Beltran, F.D.E.; Valdez-Acosta, I.R.C.; Taquiqui, G.D.; Gawigawen, S.B.; Macalino, M.V.L.; Aguirre-Aguinaldo, L.M.S.M.; Flores-Declaro, M.A.; et al. Newborn Screening Long-Term Follow-Up Clinics (Continuity Clinics) in the Philippines during the COVID-19 Pandemic: Continuing Quality Patient Care. Int. J. Neonatal Screen. 2023, 9, 2. https://doi.org/10.3390/ijns9010002
Maceda EBG, Abadingo ME, Panol KAR, Beltran FDE, Valdez-Acosta IRC, Taquiqui GD, Gawigawen SB, Macalino MVL, Aguirre-Aguinaldo LMSM, Flores-Declaro MA, et al. Newborn Screening Long-Term Follow-Up Clinics (Continuity Clinics) in the Philippines during the COVID-19 Pandemic: Continuing Quality Patient Care. International Journal of Neonatal Screening. 2023; 9(1):2. https://doi.org/10.3390/ijns9010002
Chicago/Turabian StyleMaceda, Ebner Bon G., Michelle E. Abadingo, Karen Asuncion R. Panol, Frederick David E. Beltran, Ivy Rose C. Valdez-Acosta, Grandelee D. Taquiqui, Sharon B. Gawigawen, Maria Victoria L. Macalino, Laura Maria Soledad M. Aguirre-Aguinaldo, Marive A. Flores-Declaro, and et al. 2023. "Newborn Screening Long-Term Follow-Up Clinics (Continuity Clinics) in the Philippines during the COVID-19 Pandemic: Continuing Quality Patient Care" International Journal of Neonatal Screening 9, no. 1: 2. https://doi.org/10.3390/ijns9010002
APA StyleMaceda, E. B. G., Abadingo, M. E., Panol, K. A. R., Beltran, F. D. E., Valdez-Acosta, I. R. C., Taquiqui, G. D., Gawigawen, S. B., Macalino, M. V. L., Aguirre-Aguinaldo, L. M. S. M., Flores-Declaro, M. A., Ventilacion, K. J. V., Boligao, M. R. A. S. R., Honor, N. G., Ellong, M. S., Ocho-Ortencio, R. D., Beley, G. J., Bondoc-Eran, M. C. N., Therrell, B. L., Jr., & Padilla, C. D. (2023). Newborn Screening Long-Term Follow-Up Clinics (Continuity Clinics) in the Philippines during the COVID-19 Pandemic: Continuing Quality Patient Care. International Journal of Neonatal Screening, 9(1), 2. https://doi.org/10.3390/ijns9010002