
Reduction in Acquisition Time and Improvement in Image Quality in T2-Weighted MR Imaging of Musculoskeletal Tumors of the Extremities Using a Novel Deep Learning-Based Reconstruction Technique in a Turbo Spin Echo (TSE) Sequence

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. MRI Examination Protocols
2.3. Image Analysis
2.4. Lesion Assessment
2.5. Statistical Evaluation
2.6. Deep Learning Reconstruction
3. Results
3.1. Patient Cohort
3.2. Image Analysis
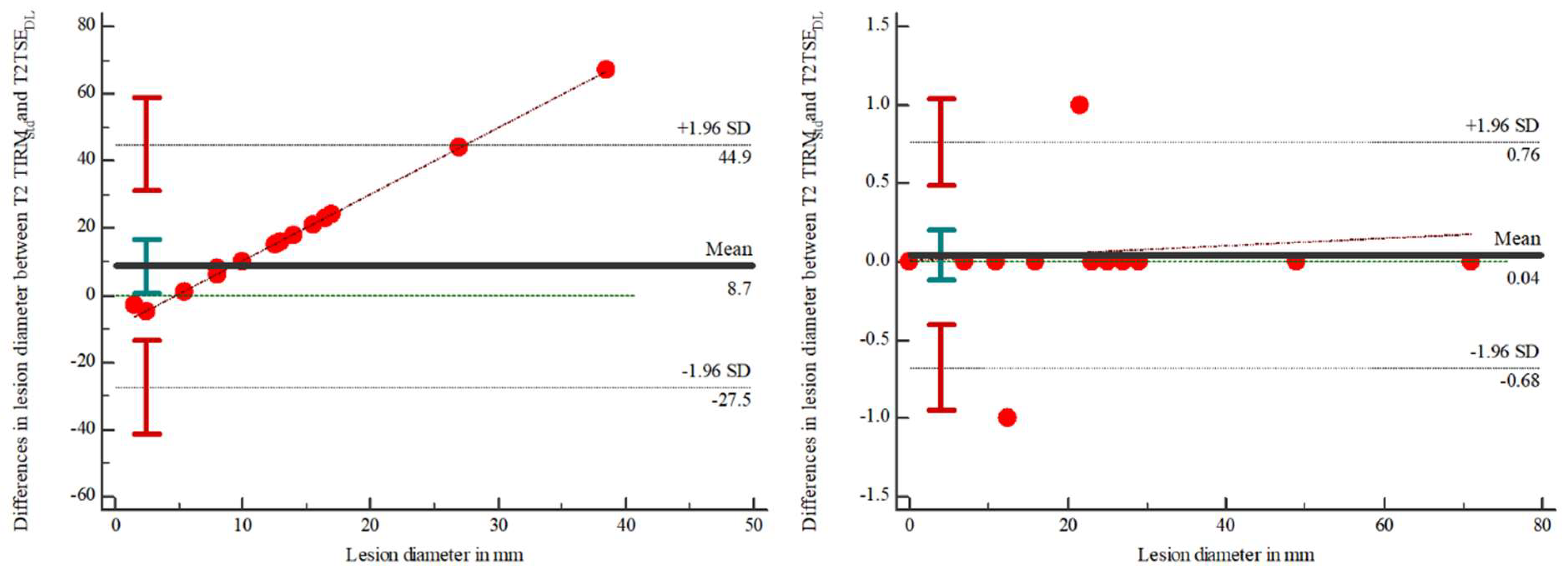
3.3. Lesion Assessment
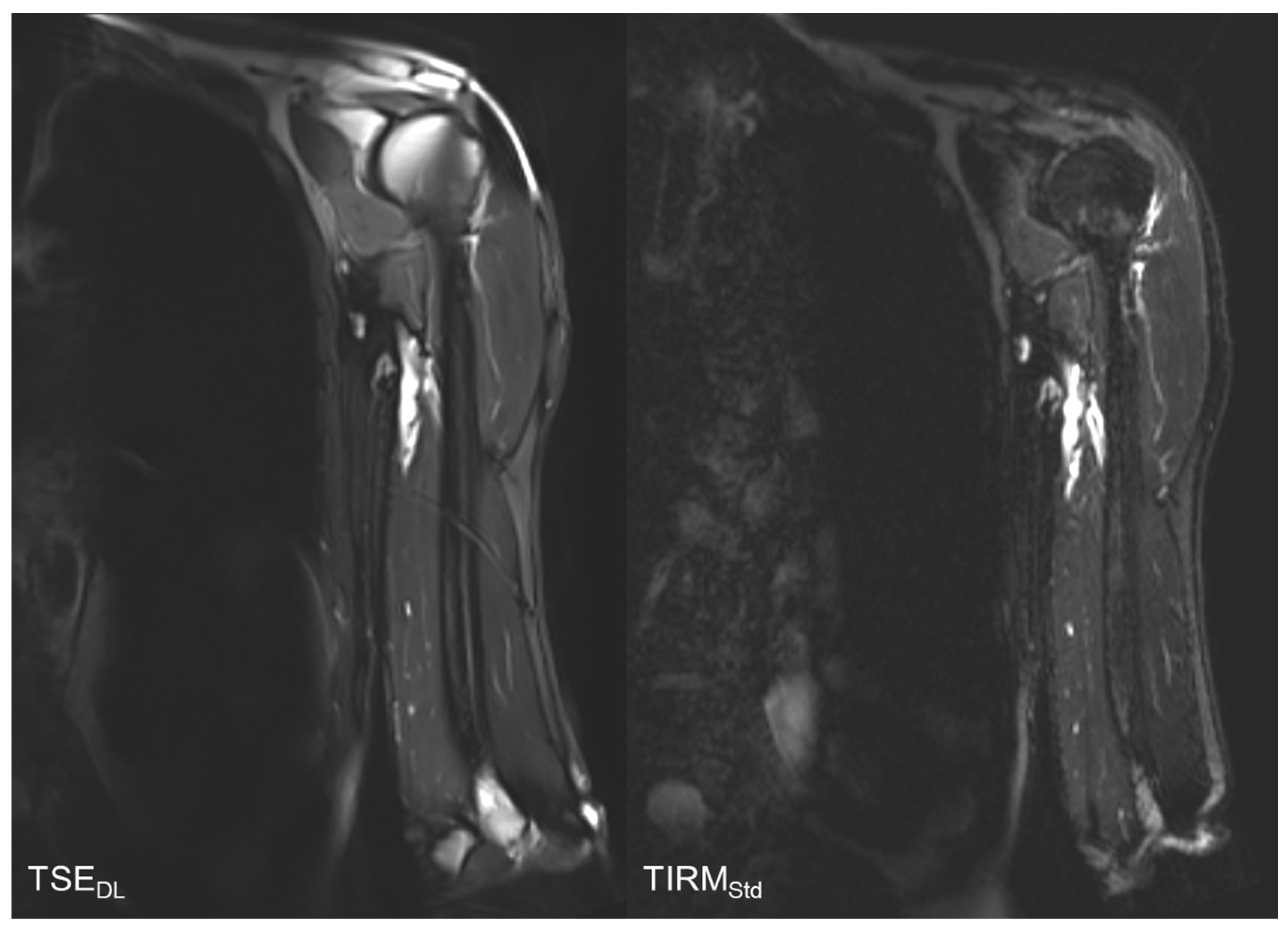
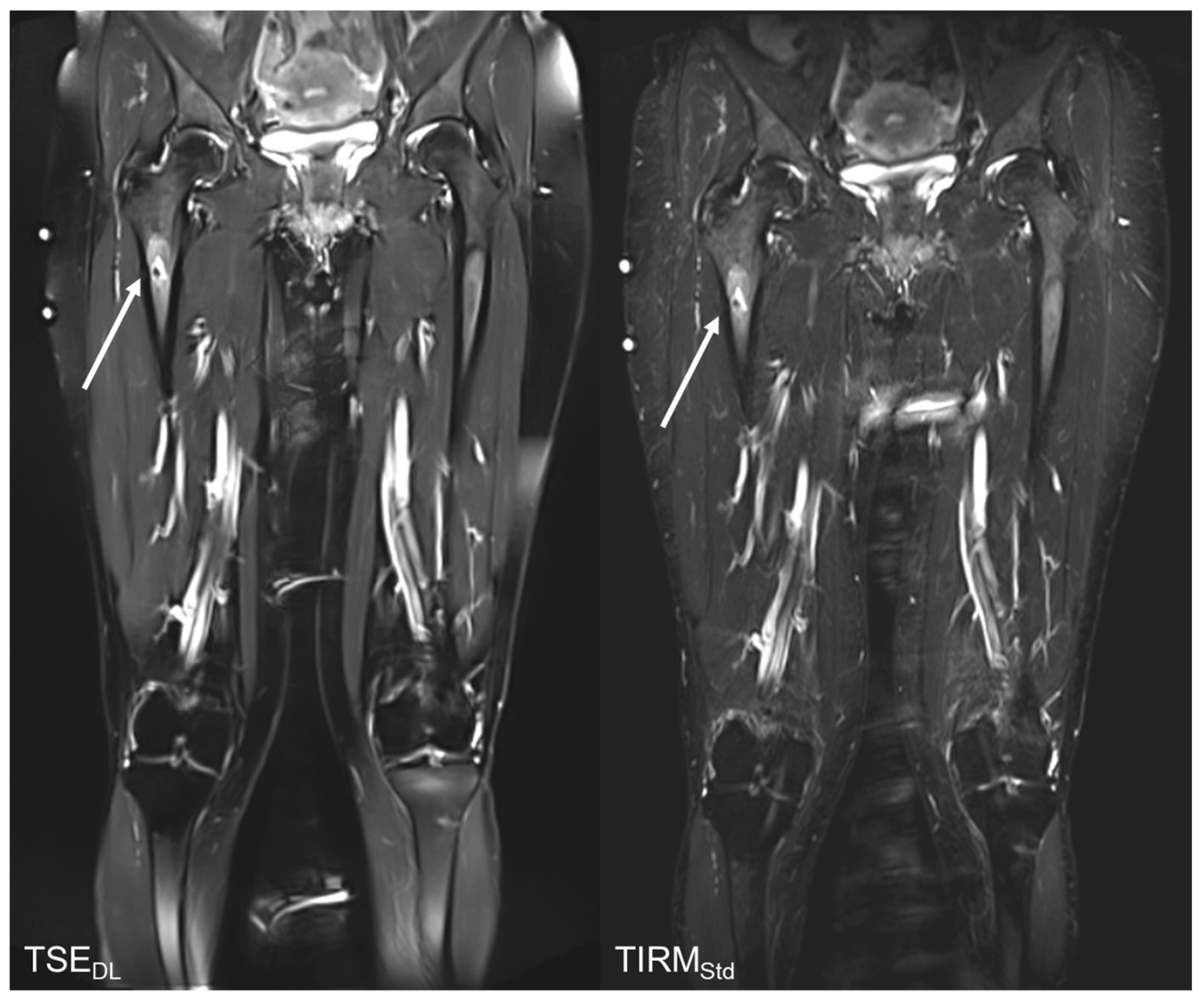
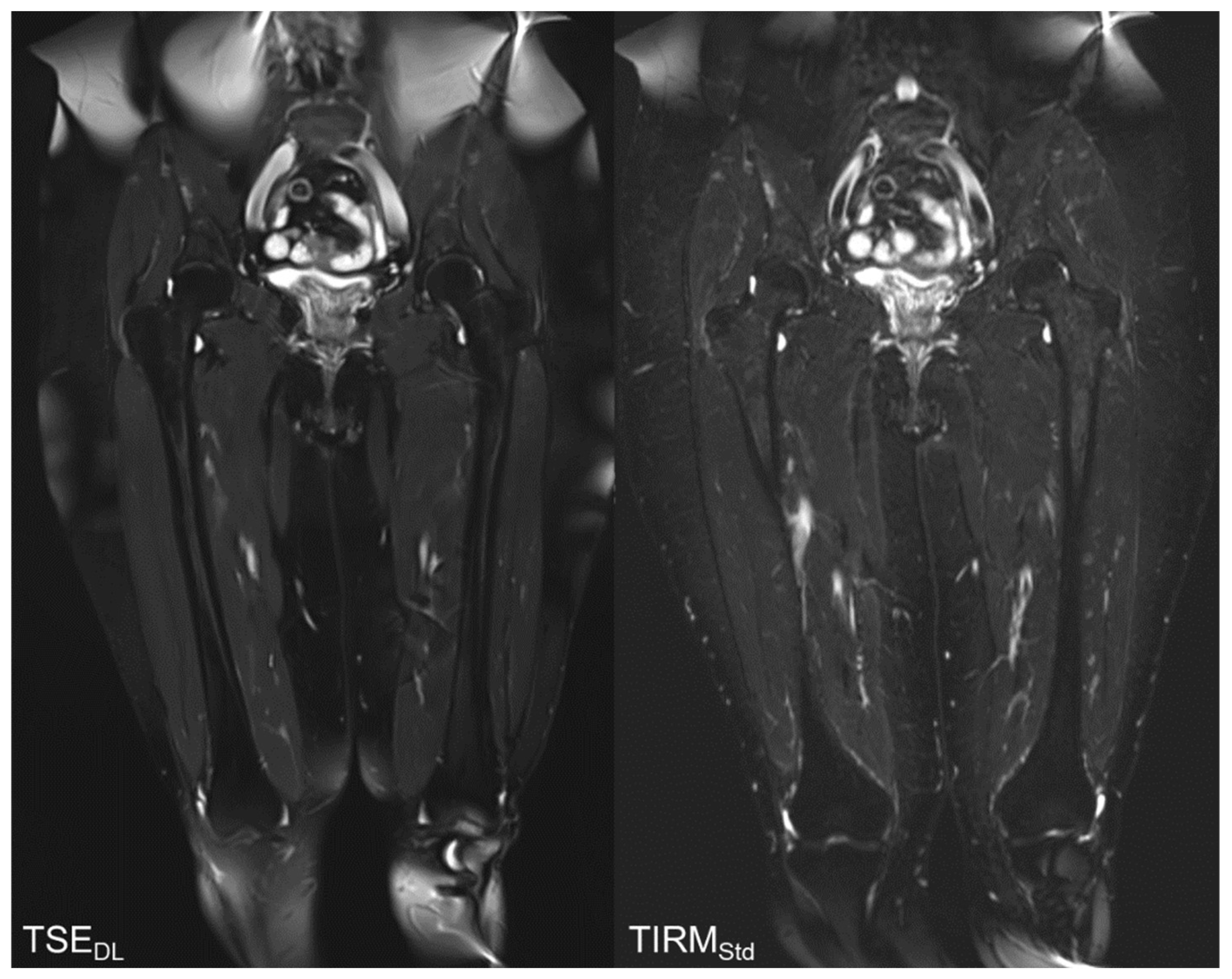
3.4. Qualitative Image Analysis
3.5. Subgroup Analysis
3.6. Acquisition Time
3.6.1. 1.5 Tesla Scanners
3.6.2. 3 Tesla Scanners
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| CNN | Convolutional neural network |
| DL | Deep Learning |
| FA | Flip Angle |
| pc | post-contrast |
| SNR | Signal-to-Noise Ratio |
| Std | Standard |
| T2 TSEDL | T2-weighted turbo deep learning accelerated spin echo sequence |
| TA | Time of Acquisition |
| T2w | T2-weighted |
| tra | transversal |
| TSE | Turbo spin echo |
| TSEStd | standard Turbo spin echo sequence |
| TIRM | Turbo inversion recovery magnitude |
| TIRMStd | standard Turbo inversion recovery magnitude sequence |
References
- Papworth, K.E.; Arroyo, V.M.; Styring, E.; Zaikova, O.; Melin, B.S.; Lupo, P.J. Soft-tissue sarcoma in adolescents and young adults compared with older adults: A report among 5000 patients from the Scandinavian Sarcoma Group Central Register. Cancer 2019, 125, 3595–3602. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, A.C.; Gronchi, A.; Cardona, K. Soft-tissue sarcoma in adults: An update on the current state of histiotype-specific management in an era of personalized medicine. CA A Cancer J. Clin. 2020, 70, 200–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stramare, R.; Beltrame, V.; Gazzola, M.; Gerardi, M.; Scattolin, G.; Coran, A.; Faccinetto, A.; Rastrelli, M.; Rossi, C.R. Imaging of soft-tissue tumors. J. Magn. Reson. Imaging 2013, 37, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.M.; de Cesar Netto, C.; Schon, L.C.; Fritz, J. Metal Artifact Reduction Magnetic Resonance Imaging Around Arthroplasty Implants: The Negative Effect of Long Echo Trains on the Implant-Related Artifact. Investig. Radiol. 2017, 52, 310–316. [Google Scholar] [CrossRef]
- Bangerter, N.K.; Taylor, M.D.; Tarbox, G.J.; Palmer, A.; Park, D.J. Quantitative techniques for musculoskeletal MRI at 7 Tesla. Quant. Imaging Med. Surg. 2016, 6, 715–730. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, L.; Harish, M.; Hargreaves, B.; Staroswiecki, E.; Gold, G. Advances in musculoskeletal MRI: Technical considerations. J. Magn. Reson. Imaging 2012, 36, 775–787. [Google Scholar] [CrossRef] [Green Version]
- Gassenmaier, S.; Küstner, T.; Nickel, D.; Herrmann, J.; Hoffmann, R.; Almansour, H.; Afat, S.; Nikolaou, K.; Othman, A.E. Deep Learning Applications in Magnetic Resonance Imaging: Has the Future Become Present? Diagnostics 2021, 11, 2181. [Google Scholar] [CrossRef]
- Hosseini, S.A.H.; Zhang, C.; Weingärtner, S.; Moeller, S.; Stuber, M.; Ugurbil, K.; Akçakaya, M. Accelerated coronary MRI with sRAKI: A database-free self-consistent neural network k-space reconstruction for arbitrary undersampling. PLoS ONE 2020, 15, e0229418. [Google Scholar] [CrossRef] [Green Version]
- Schmidhuber, J. Deep Learning in Neural Networks: An Overview. Neural Netw. 2015, 61, 85–117. [Google Scholar] [CrossRef] [Green Version]
- Lundervold, A.S.; Lundervold, A. An overview of deep learning in medical imaging focusing on MRI. Z. Med. Phys. 2019, 29, 102–127. [Google Scholar] [CrossRef]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, G.; Jiang, B.; Tong, L.; Xie, Y.; Zaharchuk, G.; Wintermark, M. Applications of Deep Learning to Neuro-Imaging Techniques. Front. Neurol. 2019, 10, 869. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Phang, J.; Park, J.; Shen, Y.; Huang, Z.; Zorin, M.; Jastrzebski, S.; Fevry, T.; Katsnelson, J.; Kim, E.; et al. Deep Neural Networks Improve Radiologists’ Performance in Breast Cancer Screening. IEEE Trans. Med. Imaging 2019, 39, 1184–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Wang, H.; Huang, Y.; Yan, B.; Chang, Z.; Liu, Z.; Zhao, M.; Cui, L.; Song, J.; Li, F. Trends in the application of deep learning networks in medical image analysis: Evolution between 2012 and 2020. Eur. J. Radiol. 2022, 146, 110069. [Google Scholar] [CrossRef]
- Zhou, Z.; Chen, S.; Balu, N.; Chu, B.; Zhao, X.; Sun, J.; Mossa-Basha, M.; Hatsukami, T.; Börnert, P.; Yuan, C. Neural network enhanced 3D turbo spin echo for MR intracranial vessel wall imaging. Magn. Reson. Imaging 2021, 78, 7–17. [Google Scholar] [CrossRef]
- Lv, J.; Yang, M.; Zhang, J.; Wang, X. Respiratory motion correction for free-breathing 3D abdominal MRI using CNN-based image registration: A feasibility study. Br. J. Radiol. 2018, 91, 20170788. [Google Scholar] [CrossRef]
- Herrmann, J.; Gassenmaier, S.; Nickel, D.; Arberet, S.; Afat, S.; Lingg, A.; Kündel, M.; Othman, A.E. Diagnostic Confidence and Feasibility of a Deep Learning Accelerated HASTE Sequence of the Abdomen in a Single Breath-Hold. Investig. Radiol. 2021, 56, 313–319. [Google Scholar] [CrossRef]
- Gassenmaier, S.; Afat, S.; Nickel, M.; Mostapha, M.; Herrmann, J.; Almansour, H.; Nikolaou, K.; Othman, A. Accelerated T2-Weighted TSE Imaging of the Prostate Using Deep Learning Image Reconstruction: A Prospective Comparison with Standard T2-Weighted TSE Imaging. Cancers 2021, 13, 3593. [Google Scholar] [CrossRef]
- Afat, S.; Wessling, D.; Afat, C.; Nickel, D.; Arberet, S.; Herrmann, J.; Othman, A.E.; Gassenmaier, S. Analysis of a Deep Learning-Based Superresolution Algorithm Tailored to Partial Fourier Gradient Echo Sequences of the Abdomen at 1.5 T: Reduction of Breath-Hold Time and Improvement of Image Quality. Investig. Radiol. 2022, 57, 157–162. [Google Scholar] [CrossRef]
- Chan, W.P. Magnetic resonance imaging of soft-tissue tumors of the extremities: A practical approach. World J. Radiol. 2013, 5, 455–459. [Google Scholar] [CrossRef]
- Wu, M.; Ren, A.; Xu, D.; Peng, X.; Ye, X.; Li, A. Diagnostic Performance of Elastography in Malignant Soft Tissue Tumors: A Systematic Review and Meta-analysis. Ultrasound Med. Biol. 2021, 47, 855–868. [Google Scholar] [CrossRef] [PubMed]
- Grimer, R.J.; Briggs, T.W.R.; Arora, R.; Gabl, M.; Pechlaner, S.; Lutz, M. Earlier diagnosis of bone and soft-tissue tumours. J. Bone Jt. Surg. Br. Vol. 2010, 92, 1489–1492. [Google Scholar] [CrossRef] [Green Version]
- Parlak, Ş.; Ergen, F.B.; Yüksel, G.Y.; Karakaya, J.; Aydın, G.B.; Kösemehmetoğlu, K.; Aydıngöz, Ü. Diffusion-weighted imaging for the differentiation of Ewing sarcoma from osteosarcoma. Skeletal. Radiol. 2021, 50, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- Henninger, B.; Glodny, B.; Rudisch, A.; Trieb, T.; Loizides, A.; Putzer, D.; Judmaier, W.; Schocke, M.F. Ewing sarcoma versus osteomyelitis: Differential diagnosis with magnetic resonance imaging. Skelet. Radiol. 2013, 42, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Gassenmaier, S.; Afat, S.; Nickel, D.; Mostapha, M.; Herrmann, J.; Othman, A.E. Deep learning–accelerated T2-weighted imaging of the prostate: Reduction of acquisition time and improvement of image quality. Eur. J. Radiol. 2021, 137, 109600. [Google Scholar] [CrossRef] [PubMed]
- Fang, Z.; Chen, Y.; Liu, M.; Xiang, L.; Zhang, Q.; Wang, Q.; Lin, W.; Shen, D. Deep Learning for Fast and Spatially Constrained Tissue Quantification from Highly Accelerated Data in Magnetic Resonance Fingerprinting. IEEE Trans. Med. Imaging 2019, 38, 2364–2374. [Google Scholar] [CrossRef]
- Shanbhogue, K.; Tong, A.; Smereka, P.; Nickel, D.; Arberet, S.; Anthopolos, R.; Chandarana, H. Accelerated single-shot T2-weighted fat-suppressed (FS) MRI of the liver with deep learning–based image reconstruction: Qualitative and quantitative comparison of image quality with conventional T2-weighted FS sequence. Eur. Radiol. 2021, 31, 8447–8457. [Google Scholar] [CrossRef]
- Reshadi, H.; Rouhani, A.; Mohajerzadeh, S.; Moosa, M.; Elmi, A. Prevalence of malignant soft tissue tumors in extremities: An epidemiological study in syria. Arch. Bone Jt. Surg. 2014, 2, 106–110. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence | T2 TIRMStd Coronal | T2 TSEDL Coronal | Sequence | T2 TIRMStd Coronal | T2 TSEDL Coronal |
|---|---|---|---|---|---|
| TE [ms] | 71 | 71 | TE [ms] | 74 | 74 |
| TR [ms] | 5440 | 5880 | TR [ms] | 6030 | 6200 |
| FA [°] | 150 | 140 | FA [°] | 150 | 140 |
| TA [min:s] | 2:34 min | 1:06 min | TA [min:s] | 2:50 min | 1:10 min |
| Slice thickness [mm] | 5.0 | 5.0 | Slice thickness [mm] | 5.0 | 5.0 |
| FOV (mm2) | 460 x 460 | 460 x 460 | FOV (mm2) | 460 x 460 | 460 x 460 |
| Sequence | T2 TIRMStd Coronal | T2 TSEDL Coronal | Sequence | T2 TIRMStd Coronal | T2 TSEDL Coronal |
|---|---|---|---|---|---|
| TE [ms] | 71 | 71 | TE [ms] | 74 | 74 |
| TR [ms] | 5440 | 6060 | TR [ms] | 6030 | 6200 |
| FA [°] | 150 | 140 | FA [°] | 150 | 140 |
| TA [min:s] | 2:34 min | 1:14 min | TA [min:s] | 2:50 min | 1:10 min |
| Slice thickness [mm] | 5.0 | 5.0 | Slice thickness [mm] | 5.0 | 5.0 |
| FOV (mm2) | 500 x 500 | 500 x 500 | FOV (mm2) | 500 x 500 | 500 |
| Patients (Male/Female), n | 23 (16/7) |
|---|---|
| Age, mean ± SD (range), y | total: 60 ± 16 (30–86) |
| male: 55 ± 15 (30–81) | |
| female: 70 ± 12 (50–86) | |
| Diagnosis, n | Liposarcoma, 5 |
| Neurinoma, 2 | |
| Leiomyosarcoma, 2 | |
| Lipoma, 2 | |
| Enchondroma, 2 | |
| Unclear mass, 2 | |
| Unclear symptoms needing further specification, 2 | |
| Myxofibrosarcoma, 2 | |
| Pleomorphic sarcoma, 1 | |
| Not otherwise specified sarcoma, 1 | |
| Spindle cell sarcoma, 1 | |
| Ewing sarcoma, 1 |
| Reader 1 | Reader 2 | |||||
|---|---|---|---|---|---|---|
| T2 TIRMStd Median (IQR) | T2 TSEDL Median (IQR) | p-Value | T2 TIRMStd Median (IQR) | T2 TSEDL Median (IQR) | p-Value | |
| Overall Image Quality | ||||||
| IQ | 4 (3–4) | 5 (5–5) | <0.001 | 4 (4–4) | 5 (5–5) | <0.001 |
| Noise | 4 (3–4) | 5 (5–5) | <0.001 | 4 (3–4) | 5 (4–5) | <0.001 |
| Contrast | 4 (3–4) | 5 (5–5) | <0.001 | 4 (4–4) | 5 (4–5) | <0.001 |
| Sharpness | 4 (3–4) | 5 (5–5) | <0.001 | 4 (3–4) | 5 (5–5) | <0.001 |
| Artifacts | 4 (4–4) | 5 (4–5) | 0.013 | 4 (4–4) | 4 (4–5) | 0.542 |
| Reader 1 | Reader 2 | |||||
|---|---|---|---|---|---|---|
| T2 TIRMStd Median (IQR) | T2 TSEDL Median (IQR) | p-Value | T2 TIRMStd Median (IQR) | T2 TSEDL Median (IQR) | p-Value | |
| Lesion Assessment | ||||||
| Lesion size | 22 (13–29) | 22 (12–29) | 0.982 | 22 (13–29) | 22 (12–29) | 0.797 |
| Lesion detectability | 4 (4–5) | 5 (5–5) | <0.001 | 4 (4–5) | 5 (5–5) | 0.003 |
| Diagnostic confidence | 4 (4–4) | 5 (5–5) | <0.001 | 4 (4–4) | 5 (5–5) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wessling, D.; Herrmann, J.; Afat, S.; Nickel, D.; Othman, A.E.; Almansour, H.; Gassenmaier, S. Reduction in Acquisition Time and Improvement in Image Quality in T2-Weighted MR Imaging of Musculoskeletal Tumors of the Extremities Using a Novel Deep Learning-Based Reconstruction Technique in a Turbo Spin Echo (TSE) Sequence. Tomography 2022, 8, 1759-1769. https://doi.org/10.3390/tomography8040148
Wessling D, Herrmann J, Afat S, Nickel D, Othman AE, Almansour H, Gassenmaier S. Reduction in Acquisition Time and Improvement in Image Quality in T2-Weighted MR Imaging of Musculoskeletal Tumors of the Extremities Using a Novel Deep Learning-Based Reconstruction Technique in a Turbo Spin Echo (TSE) Sequence. Tomography. 2022; 8(4):1759-1769. https://doi.org/10.3390/tomography8040148
Chicago/Turabian StyleWessling, Daniel, Judith Herrmann, Saif Afat, Dominik Nickel, Ahmed E. Othman, Haidara Almansour, and Sebastian Gassenmaier. 2022. "Reduction in Acquisition Time and Improvement in Image Quality in T2-Weighted MR Imaging of Musculoskeletal Tumors of the Extremities Using a Novel Deep Learning-Based Reconstruction Technique in a Turbo Spin Echo (TSE) Sequence" Tomography 8, no. 4: 1759-1769. https://doi.org/10.3390/tomography8040148
APA StyleWessling, D., Herrmann, J., Afat, S., Nickel, D., Othman, A. E., Almansour, H., & Gassenmaier, S. (2022). Reduction in Acquisition Time and Improvement in Image Quality in T2-Weighted MR Imaging of Musculoskeletal Tumors of the Extremities Using a Novel Deep Learning-Based Reconstruction Technique in a Turbo Spin Echo (TSE) Sequence. Tomography, 8(4), 1759-1769. https://doi.org/10.3390/tomography8040148