
CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Imaging Follow-Up
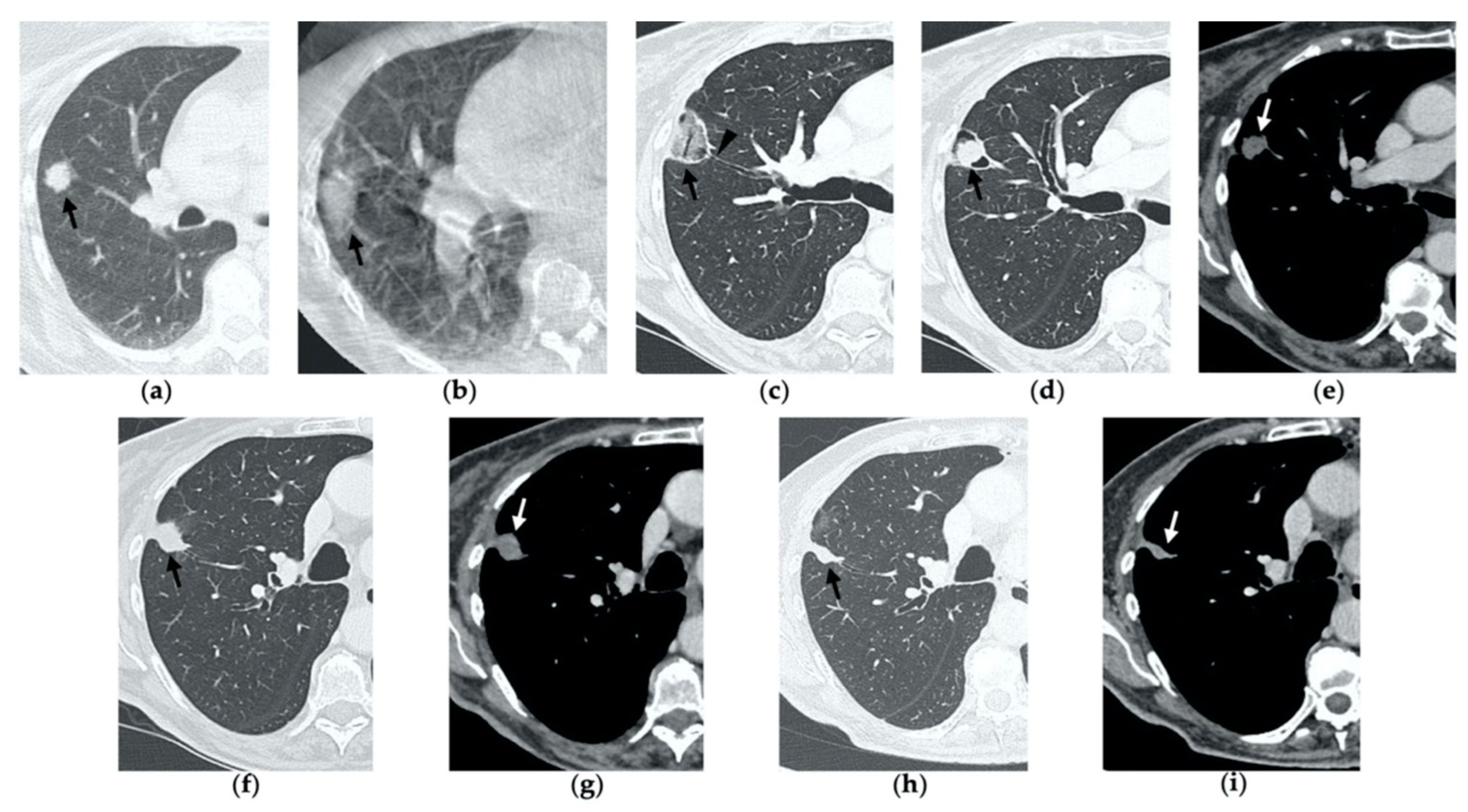
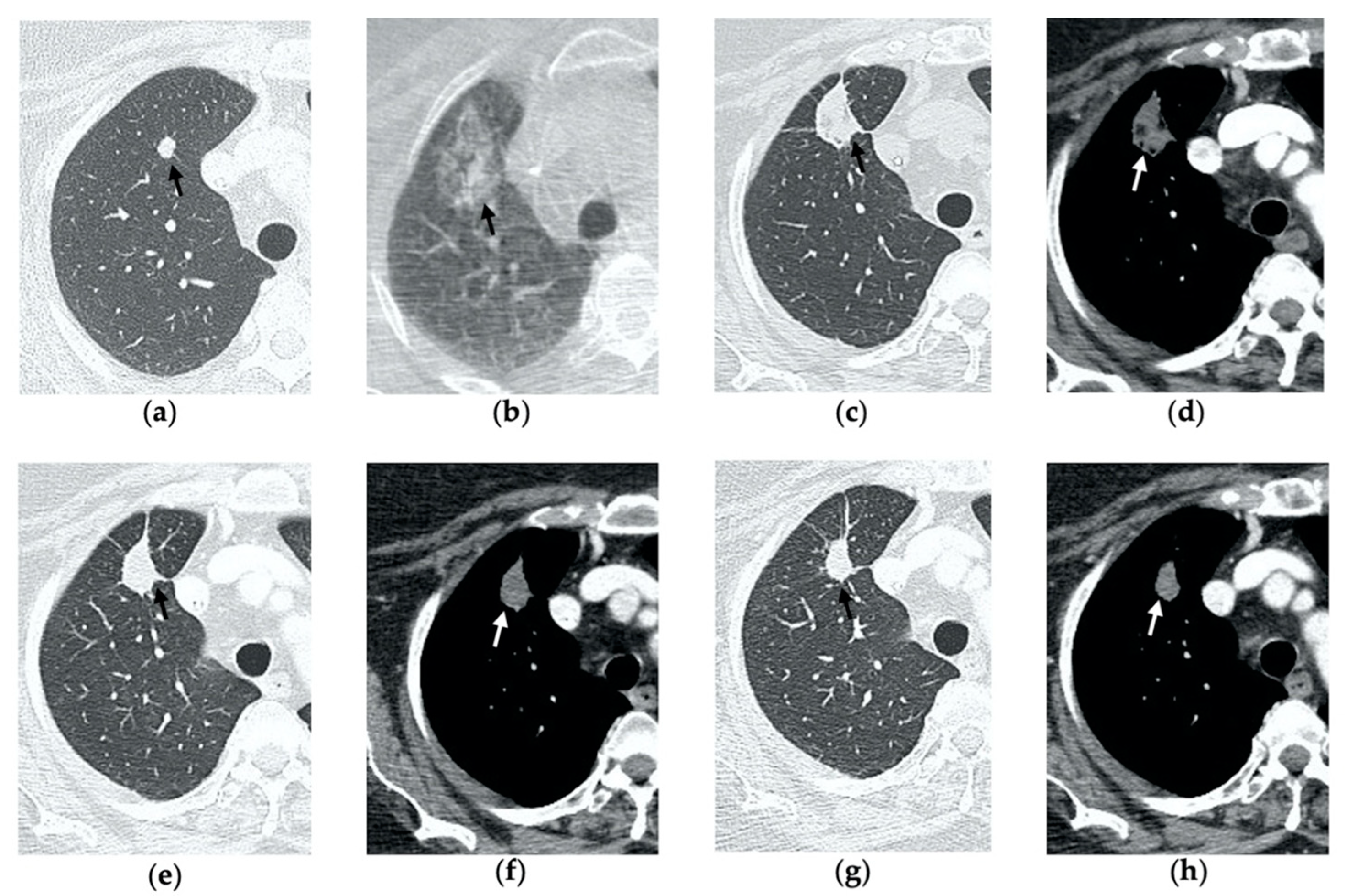
3. Normal Imaging Features
3.1. Post-Procedural Cone-Beam CT
3.2. Contrast-Enhanced CT at 1 Month
3.3. Contrast-Enhanced CT at 3 Months
3.4. Contrast-Enhanced CT at 6 Months
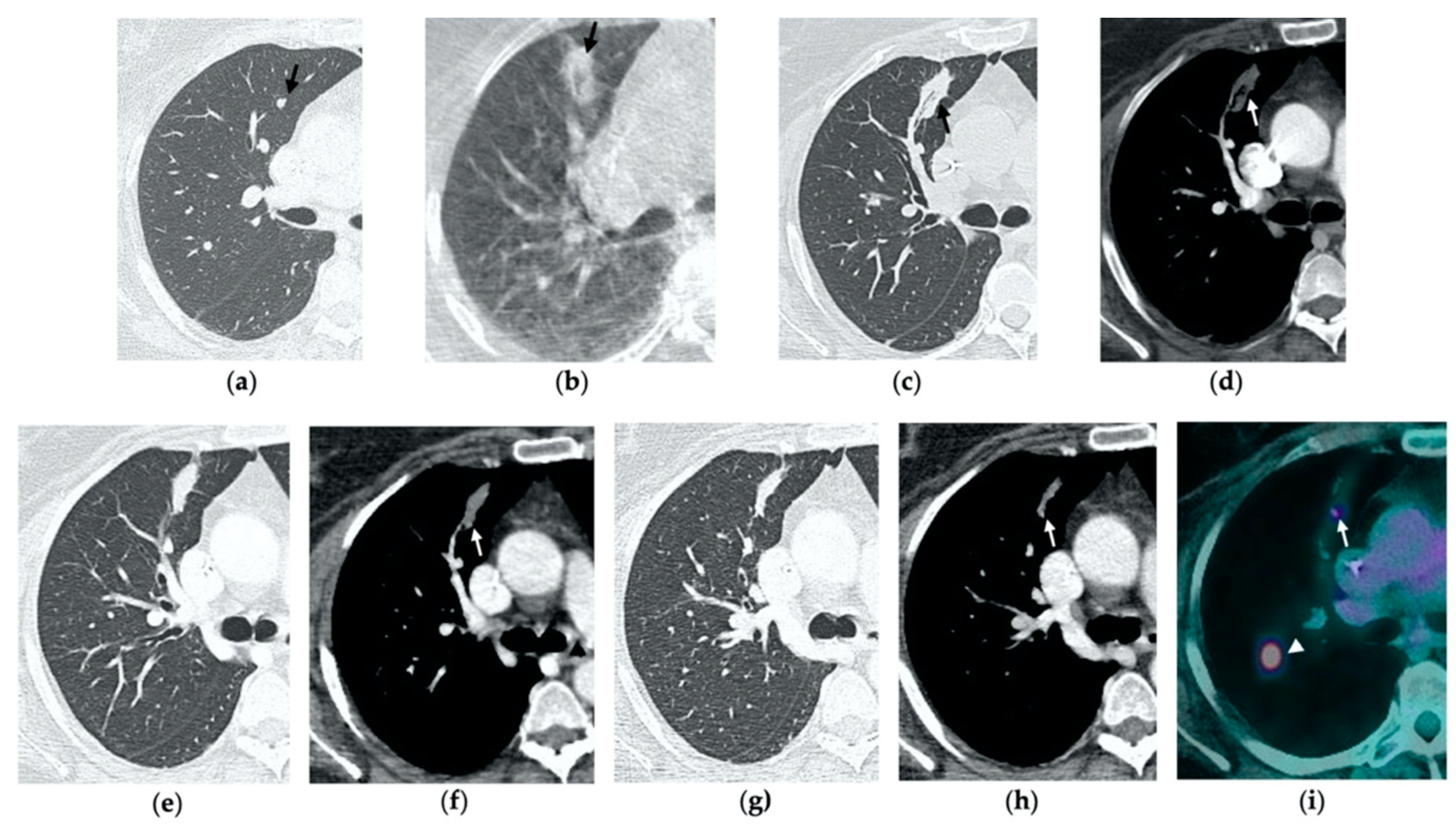
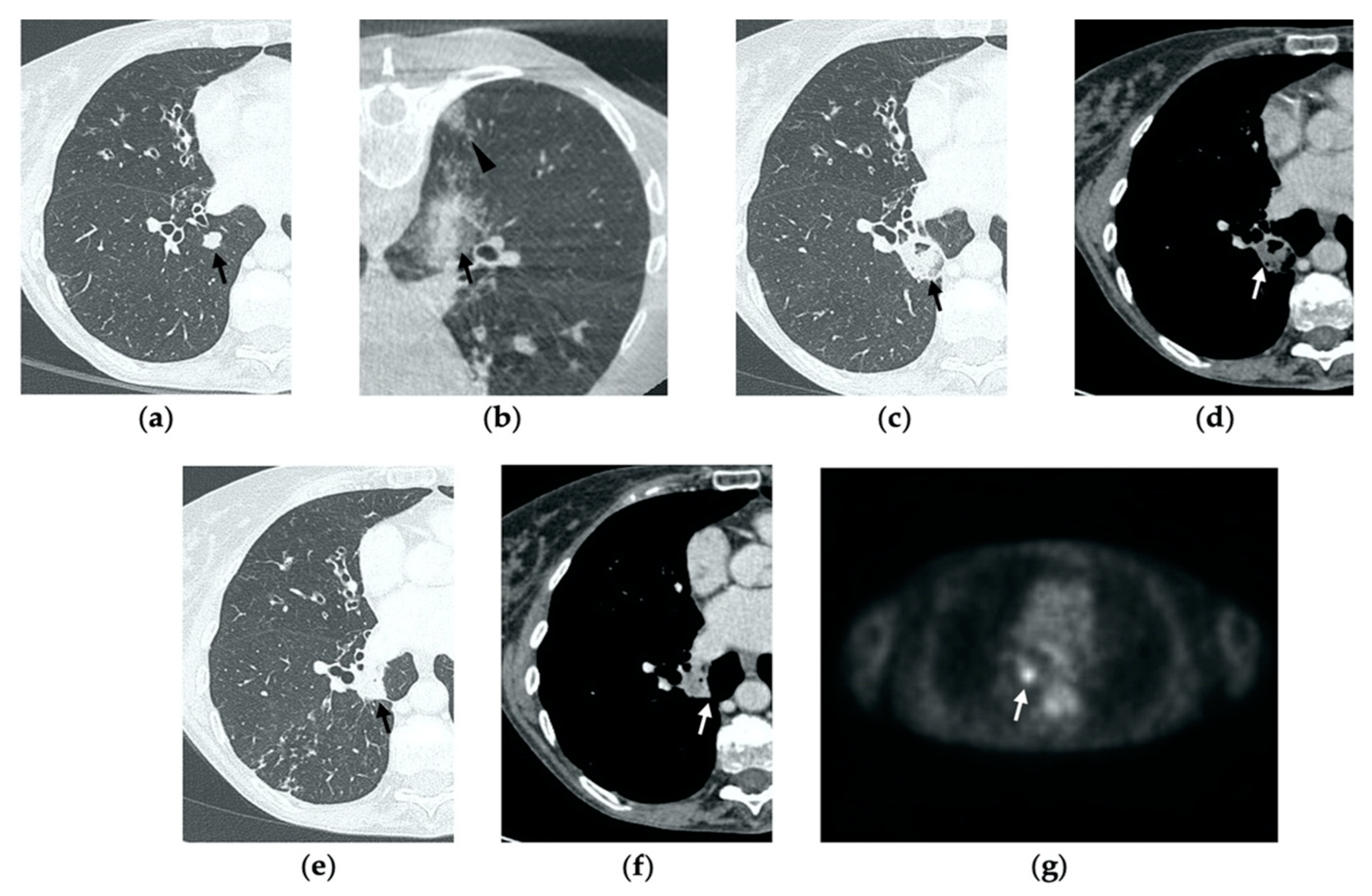
4. Residual or Recurrent Disease
5. Early Complications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, C.M.; Brunelli, A.; Callister, M.E.; Franks, K.N. Multimodality Treatment of Advanced Non-small Cell Lung Cancer: Where are we with the Evidence? Curr. Surg. Rep. 2018, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ager, B.J.; Wells, S.M.; Gruhl, J.D.; Stoddard, G.J.; Tao, R.; Kokeny, K.E.; Hitchcock, Y.J. Stereotactic body radiotherapy versus percutaneous local tumor ablation for early-stage non-small cell lung cancer. Lung Cancer 2019, 138, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, B.; Cao, P.; Wang, W.; Wang, W.; Chang, H.; Li, N.; Li, X.; Zhao, X.; Li, Y. Comparison between computed tomography-guided percutaneous microwave ablation and thoracoscopic lobectomy for stage I non-small cell lung cancer. Thorac. Cancer 2018, 9, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Watson, R.A.; Tol, I.; Gunawardana, S.; Tsakok, M. Is microwave ablation an alternative to stereotactic ablative body radiotherapy in patients with inoperable early-stage primary lung cancer? Interact. Cardiovasc. Thorac. Surg. 2019, 29, 539–543. [Google Scholar] [CrossRef]
- Kurilova, I.; Gonzalez-Aguirre, A.; Beets-Tan, R.G.; Erinjeri, J.; Petre, E.N.; Gonen, M.; Bains, M.; Kemeny, N.E.; Solomon, S.B.; Sofocleous, C.T.; et al. Microwave Ablation in the Management of Colorectal Cancer Pulmonary Metastases. Cardiovasc. Interv. Radiol. 2018, 41, 1530–1544. [Google Scholar] [CrossRef]
- Dupuy, D.E. Image-guided thermal ablation of lung malignancies. Radiology 2011, 260, 633–655. [Google Scholar] [CrossRef]
- Wolf, F.J.; Grand, D.J.; Machan, J.T.; DiPetrillo, T.A.; Mayo-Smith, W.W.; Dupuy, D.E. Microwave Ablation of Lung Malignancies: Effectiveness, CT Findings, and Safety in 50 Patients. Radiology 2008, 247, 871–879. [Google Scholar] [CrossRef]
- Vogl, T.J.; Naguib, N.N.; Gruber-Rouh, T.; Koitka, K.; Lehnert, T.; Nour-Eldin, N.-E.A. Microwave ablation therapy: Clinical utility in treatment of pulmonary metastases. Radiology 2011, 261, 643–651, correction in Radiology 2013, 266, 1000. [Google Scholar] [CrossRef]
- Vogl, T.J.; Basten, L.M.; Nour-Eldin, N.-E.A.; Kaltenbach, B.; Alckermann, H.; Naguib, N.N.N. Microwave Ablation (MWA) of Pulmonary Neoplasms: Clinical Performance of High-Frequency MWA with Spatial Energy Control Versus Conventional Low-Frequency MWA. Am. J. Roentgenol. 2019, 213, 1388–1396. [Google Scholar] [CrossRef]
- Vogl, T.J.; Nour-Eldin, N.-E.A.; Albrecht, M.H.; Kaltenbach, B.; Hohenforst-Schmidt, W.; Lin, H.; Panahi, B.; Eichler, K.; Gruber-Rouh, T.; Roman, A. Thermal Ablation of Lung Tumors: Focus on Microwave Ablation, RöFo—Fortschritte Auf Dem Geb. Röntgenstrahlen Bildgeb. Verfahr 2017, 189, 828–843. [Google Scholar] [CrossRef] [Green Version]
- Steinke, K.; Haghighi, K.S.; Wulf, S.; Morris, D.L. Effect of vessel diameter on the creation of ovine lung radiofrequency lesions in vivo: Preliminary results. J. Surg. Res. 2005, 124, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Gillams, A.R.; Lees, W.R. Radiofrequency ablation of lung metastases: Factors influencing success. Eur. Radiol. 2008, 18, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Abtin, F.G.; Eradat, J.; Gutierrez, A.J.; Lee, C.; Fishbein, M.C.; Suh, R.D. Radiofrequency Ablation of Lung Tumors: Imaging Features of the Postablation Zone. RadioGraphics 2012, 32, 947–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egashira, Y.; Singh, S.; Bandula, S.; Illing, R. Percutaneous High-Energy Microwave Ablation for the Treatment of Pulmonary Tumors: A Retrospective Single-Center Experience. J. Vasc. Interv. Radiol. 2016, 27, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Chheang, S.; Abtin, F.; Guteirrez, A.; Genshaft, S.; Suh, R. Imaging Features following Thermal Ablation of Lung Malignancies. Semin. Interv. Radiol. 2013, 30, 157–168. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, A.; Nakamura, K.; Matsuoka, T.; Toyoshima, M.; Okuma, T.; Oyama, Y.; Ikura, Y.; Ueda, M.; Inoue, Y. Radiofrequency Ablation in a Porcine Lung Model: Correlation between CT and Histopathologic Findings. Am. J. Roentgenol. 2005, 185, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, J.; Miyachi, H.; Takase, K.; Matsuhashi, T.; Yamada, T.; Sato, A.; Saito, H.; Ishibashi, T.; Endoh, M.; Higano, S.; et al. Time-related Changes in Computed Tomographic Appearance and Pathologic Findings after Radiofrequency Ablation of the Rabbit Lung: Preliminary Experimental Study. J. Vasc. Interv. Radiol. 2005, 16, 1719–1726. [Google Scholar] [CrossRef]
- Crocetti, L.; Bozzi, E.; Faviana, P.; Cioni, D.; Della Pina, C.; Sbrana, A.; Fontanini, G.; Lencioni, R. Thermal ablation of lung tissue: In Vivo experimental comparison of microwave and radiofrequency. Cardiovasc. Interv. Radiol. 2010, 33, 818–827. [Google Scholar] [CrossRef]
- Nour-Eldin, N.E.; Naguib, N.N.; Mack, M.; Abskharon, J.E.; Vogl, T.J. Pulmonary hemorrhage complicating radiofrequency ablation, from mild hemoptysis to life-threatening pattern. Eur. Radiol. 2011, 21, 197–204. [Google Scholar] [CrossRef]
- Zheng, A.; Wang, X.; Yang, X.; Wang, W.; Huang, G.; Gai, Y.; Ye, X. Major complications after lung microwave ablation: A single-center experience on 204 sessions. Ann. Thorac. Surg. 2014, 98, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Brace, C.L.; Diaz, T.A.; Hinshaw, J.L.; Lee, F.T. Tissue contraction caused by radiofrequency and microwave ablation: A laboratory study in liver and lung. J. Vasc. Interv. Radiol. 2010, 21, 1280–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, C.M.; Abbott, G.F.; Greene, R.E.; Shepard, J.-A.O.; Vummidi, D.; Digumarthy, S.R. Imaging pulmonary infection: Classic signs and patterns. AJR Am. J. Roentgenol. 2014, 202, 479–492, correction in AJR Am. J. Roentgenol. 2014, 202, 1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Digumarthy, S.R.; Kalra, M.K.; Lanuti, M.; Shepard, J.A. Reversible locoregional lymph node enlargement after radiofrequency ablation of lung tumors. AJR Am. J. Roentgenol. 2010, 194, 1250–1256. [Google Scholar] [CrossRef]
- Furukawa, K.; Miura, T.; Kato, Y.; Okada, S.; Tsutsui, H.; Shimaltani, H.; Kajiwara, N.; Taira, M.; Saito, M.; Kato, H. Microwave coagulation therapy in canine peripheral lung tissue. J. Surg. Res. 2005, 123, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Splatt, A.M.; Steinke, K. Major complications of high-energy microwave ablation for percutaneous CT-guided treatment of lung malignancies: Single-centre experience after 4 years. J. Med. Imaging Radiat. Oncol. 2015, 59, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Alberti, N.; Buy, W.; Frulio, N.; Montaudon, M.; Canella, M.; Gangi, A.; Crombe, A.; Palussière, J. Rare complications after lung percutaneous radiofrequency ablation: Incidence, risk factors, prevention and management. Eur. J. Radiol. 2016, 85, 1181–1191. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CT Imaging Features | Post-Procedural CBCT | Contrast-Enhanced CT at 1 Month | Contrast-Enhanced CT at 3 Months | Contrast-Enhanced CT at 6 Months |
|---|---|---|---|---|
| Normal | Well-demarcated oval or wedged-shaped area of hazy GGO, larger than the original lesion | Area or consolidation larger than the original lesion, with hypoattenuating bubbles or a cavity with thin walls, no central contrast enhancement, possible linear rim of hyperenhancement | Decrease in size, resolution of cavitation, possible linear rim of hyperenhancement | Decrease in size; fibrosis scarring |
| Suggestive of Recurrence | Tumor exceeding the area of GGO | No consolidation of the ablation site; nodular enhancement | Increase in size, central or nodular enhancement | Increase in size, central or nodular enhancement |
| Complications with Similar Appearance | Parenchymal hemorrhage (poorly demarcated, also along the needle tract) | Abscess (cavity with air-fluid level, thick walls and irregular internal contours, clinics of infection) BPF (hydropneumothorax with/without evidence of communication between a bronchus and the pleural space through the ablation zone) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vespro, V.; Bonanno, M.C.; Andrisani, M.C.; Ierardi, A.M.; Phillips, A.; Tosi, D.; Mendogni, P.; Franzi, S.; Carrafiello, G. CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions. Tomography 2022, 8, 617-626. https://doi.org/10.3390/tomography8020051
Vespro V, Bonanno MC, Andrisani MC, Ierardi AM, Phillips A, Tosi D, Mendogni P, Franzi S, Carrafiello G. CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions. Tomography. 2022; 8(2):617-626. https://doi.org/10.3390/tomography8020051
Chicago/Turabian StyleVespro, Valentina, Maria Chiara Bonanno, Maria Carmela Andrisani, Anna Maria Ierardi, Alice Phillips, Davide Tosi, Paolo Mendogni, Sara Franzi, and Gianpaolo Carrafiello. 2022. "CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions" Tomography 8, no. 2: 617-626. https://doi.org/10.3390/tomography8020051
APA StyleVespro, V., Bonanno, M. C., Andrisani, M. C., Ierardi, A. M., Phillips, A., Tosi, D., Mendogni, P., Franzi, S., & Carrafiello, G. (2022). CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions. Tomography, 8(2), 617-626. https://doi.org/10.3390/tomography8020051