

Evaluation of Resin Infiltration, Fluoride and the Biomimetic Mineralization of CPP-ACP in Protecting Enamel after Orthodontic Inter-Proximal Enamel Reduction

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Inclusion and Exclusion Criteria
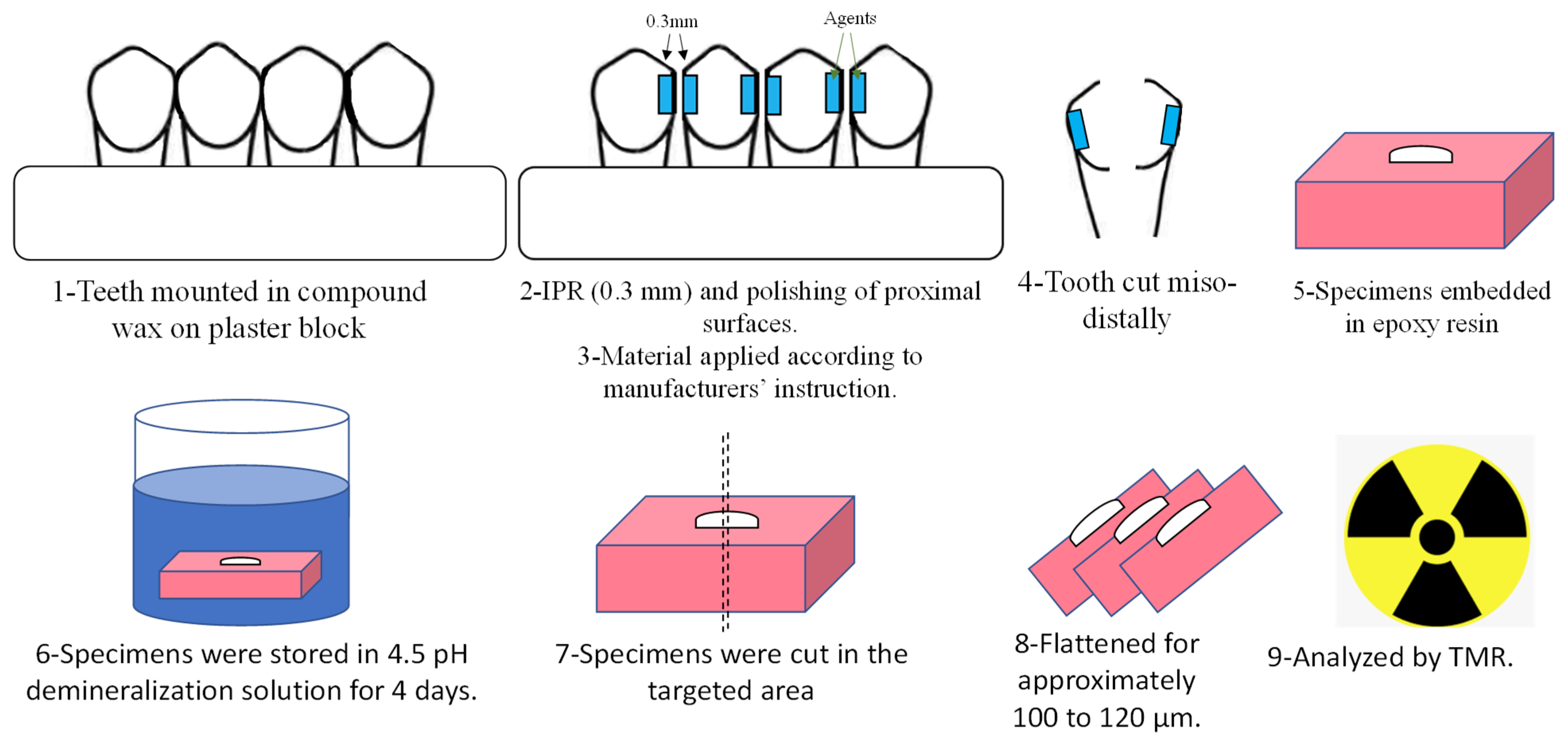
2.2. Sample Preparation and Groups
2.3. Storage of the Specimens
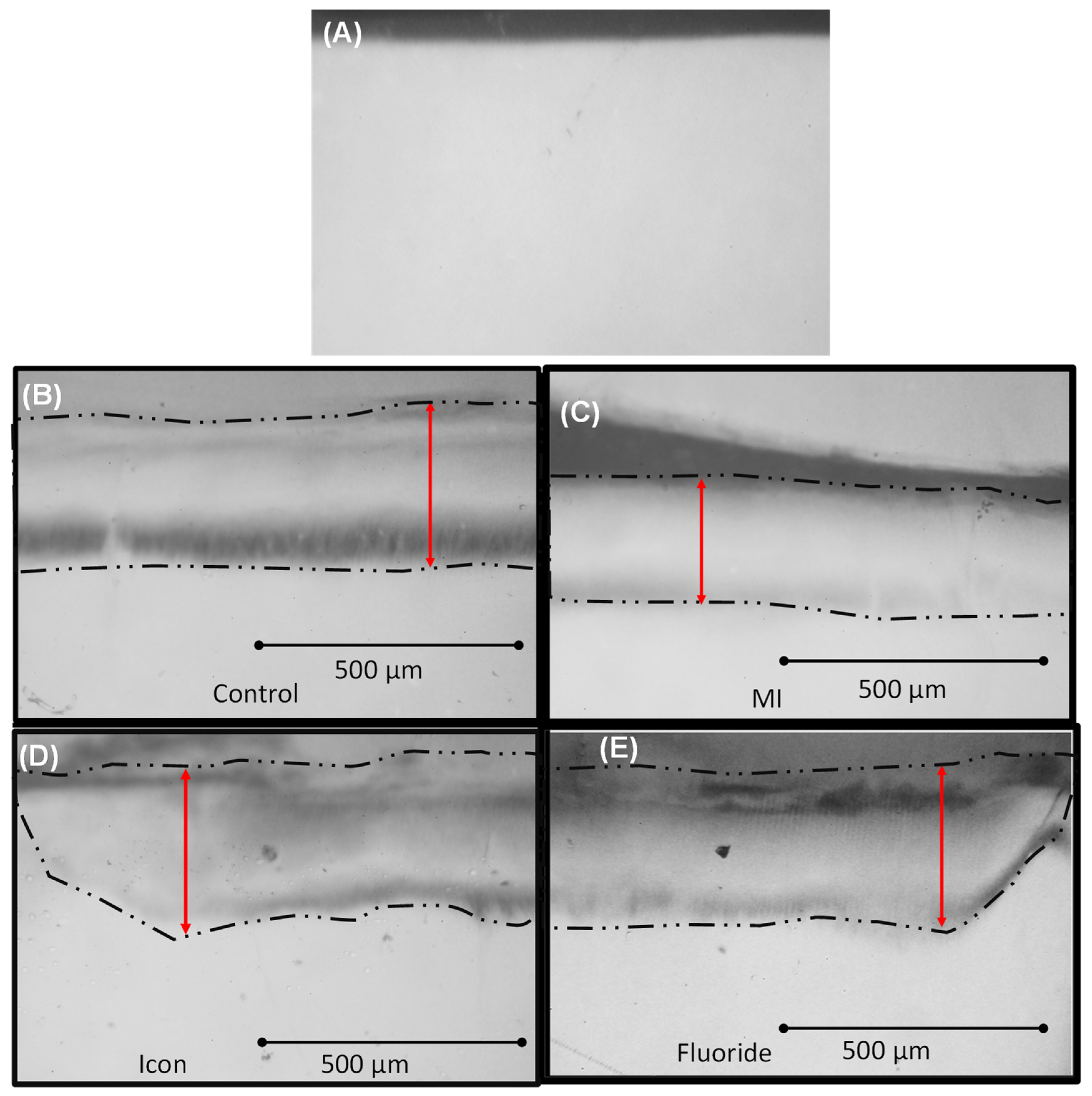
2.4. Transverse Microradiography (TMR) Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Bazi, S.M.; Abbassy, M.A.; Bakry, A.S.; Merdad, L.A.; Hassan, A.H. Effects of chlorhexidine (gel) application on bacterial levels and orthodontic brackets during orthodontic treatment. J. Oral Sci. 2016, 58, 35–42. [Google Scholar] [CrossRef]
- Pinto, A.S.; Alves, L.S.; Maltz, M.; Susin, C.; Zenkner, J.E.A. Does the Duration of Fixed Orthodontic Treatment Affect Caries Activity among Adolescents and Young Adults? Caries Res. 2018, 52, 463–467. [Google Scholar] [CrossRef]
- Khachatryan, G.; Markaryan, M.; Vardanyan, I.; Manrikyan, M.; Manrikyan, G. Morphological Characteristics and Prevention of Tooth Enamel Demineralization during Orthodontic Treatment with Non-Removable Appliances. Int. J. Environ. Res. Public Health 2022, 20, 540. [Google Scholar] [CrossRef]
- Sadyrin, E.; Swain, M.; Mitrin, B.; Rzhepakovsky, I.; Nikolaev, A.; Irkha, V.; Yogina, D.; Lyanguzov, N.; Maksyukov, S.; Aizikovich, S. Characterization of Enamel and Dentine about a White Spot Lesion: Mechanical Properties, Mineral Density, Microstructure and Molecular Composition. Nanomaterials 2020, 10, 1889. [Google Scholar] [CrossRef]
- Bakry, A.S.; Abbassy, M.A.; Alharkan, H.F.; Basuhail, S.; Al-Ghamdi, K.; Hill, R. A novel fluoride containing bioactive glass paste is capable of re-mineralizing early caries lesions. Materials 2018, 11, 1636. [Google Scholar] [CrossRef] [PubMed]
- Abbassy, M.A.; Bakry, A.S.; Hill, R.; Hassan, A.H. Fluoride bioactive glass paste improves bond durability and remineralizes tooth structure prior to adhesive restoration. Dent. Mater. 2021, 37, 71–80. [Google Scholar] [CrossRef]
- Abbassy, M.A.; Bakry, A.S.; Almoabady, E.H.; Almusally, S.M.; Hassan, A.H. Characterization of a novel enamel sealer for bioactive remineralization of white spot lesions. J. Dent. 2021, 109, 103663. [Google Scholar] [CrossRef]
- Fiori, A.; Minervini, G.; Nucci, L.; D’Apuzzo, F.; Perillo, L.; Grassia, V. Predictability of crowding resolution in clear aligner treatment. Prog. Orthod. 2022, 23, 43. [Google Scholar] [CrossRef]
- Kodaka, T.; Kuroiwa, M.; Higashi, S. Structural and distribution patterns of surface ‘prismless’ enamel in human permanent teeth. Caries Res. 1991, 25, 7–20. [Google Scholar] [CrossRef]
- Vicente, A.; Ortiz-Ruiz, A.J.; González-Paz, B.M.; Martínez-Beneyto, Y.; Bravo-González, L.A. Effectiveness of a toothpaste and a serum containing calcium silicate on protecting the enamel after interproximal reduction against demineralization. Sci. Rep. 2021, 11, 834. [Google Scholar] [CrossRef]
- Chudasama, D.; Sheridan, J. Guidelines for contemporary air-rotor stripping. J. Clin. Orthod. 2007, 41, 315–320. [Google Scholar]
- Zachrisson, B.; Minster, L.; Ogaard, B.; Birkhed, D. Dental health assessed after interproximal enamel reduction: Caries risk in posterior teeth. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 90–98. [Google Scholar] [CrossRef]
- Radlanski, R.; Jager, A.; Schwestka, R.; Bertzbach, F. Plaque accumulations caused by interdental stripping. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 416–420. [Google Scholar] [CrossRef]
- Bakry, A.; Abbassy, M. Increasing the efficiency of CPP-ACP to remineralize enamel white spot lesions. J. Dent. 2018, 76, 52–57. [Google Scholar] [CrossRef]
- Hamba, H.; Nikaido, T.; Inoue, G.; Sadr, A.; Tagami, J. Effects of CPP-ACP with sodium fluoride on inhibition of bovine enamel demineralization: A quantitative assessment using micro-computed tomography. J. Dent. 2011, 39, 405–413. [Google Scholar] [CrossRef]
- Paris, S.; Schwendicke, F.; Seddig, S.; Muller, W.; Dorfer, C.; Meyer-Lueckel, H. Micro-hardness and mineral loss of enamel lesions after infiltration with various resins: Influence of infiltrant composition and application frequency in vitro. J. Dent. 2013, 41, 543–548. [Google Scholar] [CrossRef]
- Keyes, P.H. The infectious and transmissible nature of experimental dental caries. Findings and implications. Arch. Oral Biol. 1960, 1, 304–320. [Google Scholar] [CrossRef]
- Jarjoura, K.; Gagnon, G.; Nieberg, L. Caries risk after interproximal enamel reduction. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 26–30. [Google Scholar] [CrossRef]
- Hamba, H.; Nikaido, T.; Sadr, A.; Nakashima, S.; Tagami, J. Enamel lesion parameter correlations between polychromatic micro-CT and TMR. J. Dent. Res. 2012, 91, 586–591. [Google Scholar] [CrossRef]
- Bakry, A.; Abbassy, M. The efficacy of a bioglass (45S5) paste temporary filling used to remineralize enamel surfaces prior to bonding procedures. J. Dent. 2019, 85, 33–38. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Said, S.M.; Ekambaram, M.; Yiu, C. Effect of different fluoride varnishes on remineralization of artificial enamel carious lesions. Int. J. Paediatr. Dent. 2017, 27, 163–173. [Google Scholar] [CrossRef]
- Kilic, M.; Gurbuz, T. Evaluation of the effects of different remineralisation agents on initial enamel lesions by scanning electron microscope and energy-distributed X-ray analysis. Int. J. Clin. Pract. 2021, 75, e14299. [Google Scholar] [CrossRef]
- Bakhsh, T.; Bakry, A.; Mandurah, M.; Abbassy, M. Novel evaluation and treatment techniques for white spot lesions. An in vitro study. Orthod. Craniofacial Res. 2017, 20, 170–176. [Google Scholar] [CrossRef]
- Reynolds, E.; Cai, F.; Cochrane, N.; Shen, P.; Walker, G.; Morgan, M.; Reynolds, C. Fluoride and casein phosphopeptide-amorphous calcium phosphate. J. Dent. Res. 2008, 87, 344–348. [Google Scholar] [CrossRef]
- Peng, Y.; Qian, Z.; Ting, Z.; Jie, F.; Xiaomei, X.; Li, M. The effect of resin infiltration vs. fluoride varnish in enhancing enamel surface conditions after interproximal reduction. Dent. Mater. J. 2016, 35, 756–761. [Google Scholar] [CrossRef]
- Meganck, J.; Kozloff, K.; Thornton, M.; Broski, S.; Goldstein, S. Beam hardening artifacts in micro-computed tomography scanning can be reduced by X-ray beam filtration and the resulting images can be used to accurately measure BMD. Bone 2009, 45, 1104–1116. [Google Scholar] [CrossRef]
- Schwass, D.; Swain, M.; Purton, D.; Leichter, J. A system of calibrating microtomography for use in caries research. Caries Res. 2009, 43, 314–321. [Google Scholar] [CrossRef]
- Newbury, D.E.; Ritchie, N.W.M. Is Scanning Electron Microscopy/Energy Dispersive X-ray Spectrometry (SEM/EDS) Quantitative? Scanning 2013, 35, 141–168. [Google Scholar] [CrossRef]
- Meyer-Lueckel, H.; Paris, S.; Mueller, J.; Colfen, H.; Kielbassa, A. Influence of the application time on the penetration of different dental adhesives and a fissure sealant into artificial subsurface lesions in bovine enamel. Dent. Mater. 2006, 22, 22–28. [Google Scholar] [CrossRef]
- Meyer-Lueckel, H.; Chatzidakis, A.; Naumann, M.; Dorfer, C.; Paris, S. Influence of application time on penetration of an infiltrant into natural enamel caries. J. Dent. 2011, 39, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Giulio, A.; Matteo, Z.; Serena, I.; Silvia, M.; Luigi, C. In vitro evaluation of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) effect on stripped enamel surfaces. A SEM investigation. J. Dent. 2009, 37, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Cross, K.; Huq, N.; Stanton, D.; Sum, M.; Reynolds, E. NMR studies of a novel calcium, phosphate and fluoride delivery vehicle-alpha(S1)-casein(59-79) by stabilized amorphous calcium fluoride phosphate nanocomplexes. Biomaterials 2004, 25, 5061–5069. [Google Scholar] [CrossRef]
- Cross, K.; Huq, N.; Palamara, J.; Perich, J.; Reynolds, E. Physicochemical characterization of casein phosphopeptide-amorphous calcium phosphate nanocomplexes. J. Biol. Chem. 2005, 280, 15362–15369. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, N.; Cai, F.; Huq, N.; Burrow, M.; Reynolds, E. New approaches to enhanced remineralization of tooth enamel. J. Dent. Res. 2010, 89, 1187–1197. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Materials | Composition | Procedures |
|---|---|---|
| MI varnish (GC) | 30–50% polybinyl acetate, 10–30% hydrogenated rosin, 20–30% ethanol, 1–8% sodium fluoride, 1–5% silicon dioxide | Applied and left undisturbed for 24 h After 24 h MI varnish was carefully removed using a surgical blade without touching surface Wiped by wet gauze Soaked in 50% acetone solution for 5 min |
| Icon–Etch (DMG) | 15% hydrochloric acid, water, pyrogenic silica, surfactant, pigments | Apply the gel and leave it for 2 min Remove excess material with a cotton roll Rinse with water for 30 s Dry with oil—free and water—free air |
| Icon–Dry (DMG) | Ethanol 99% | Apply an ample amount of material and left it set for 30 s Dry with oil—free and water—free air |
| Icon–Infiltrant (DMG) | TEGDMA—based resin, initiators and stabilizers | Apply an ample amount of Icon—Infiltrant onto the etched surface Let Icon—Infiltrant set for 3 min Remove excess material with a cotton roll and dental floss Light—cure Icon—Infiltrant for 40 s Repeat the application and let set for 1 min, followed by curing for 40 s |
| Nupro® Acidulated Phosphate Fluoride (DENTSPLY) | 2.59% sodium fluoride (1.23% fluoride ion) | Remove excess material with a cotton roll and dental floss, and light—cure for a minimum of 40 s Apply and leave undisturbed for 4 min Wipe with wet gauze |
| Control Udemineralized | Control Demineralized | Icon | Fluoride | MI Varnish | ||
|---|---|---|---|---|---|---|
| ∆ Z (Vol% × µm) | Mean | 0 | 2699.47 | 2309.43 | 2405.94 | 1441.28 * |
| Standard deviation | 0 | 529.35 | 533.03 | 199.16 | 287.18 | |
| Lesion depth (µm) | Mean | 0 | 226.04 | 203.73 | 226.47 | 136.97 ** |
| Standard deviation | 0 | 34.62 | 30.14 | 21.76 | 20.06 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almansouri, N.; Bakry, A.S.; Abbassy, M.A.; Linjawi, A.I.; Hassan, A.H. Evaluation of Resin Infiltration, Fluoride and the Biomimetic Mineralization of CPP-ACP in Protecting Enamel after Orthodontic Inter-Proximal Enamel Reduction. Biomimetics 2023, 8, 82. https://doi.org/10.3390/biomimetics8010082
Almansouri N, Bakry AS, Abbassy MA, Linjawi AI, Hassan AH. Evaluation of Resin Infiltration, Fluoride and the Biomimetic Mineralization of CPP-ACP in Protecting Enamel after Orthodontic Inter-Proximal Enamel Reduction. Biomimetics. 2023; 8(1):82. https://doi.org/10.3390/biomimetics8010082
Chicago/Turabian StyleAlmansouri, Naser, Ahmed Samir Bakry, Mona Aly Abbassy, Amal Ibrahim Linjawi, and Ali Habib Hassan. 2023. "Evaluation of Resin Infiltration, Fluoride and the Biomimetic Mineralization of CPP-ACP in Protecting Enamel after Orthodontic Inter-Proximal Enamel Reduction" Biomimetics 8, no. 1: 82. https://doi.org/10.3390/biomimetics8010082
APA StyleAlmansouri, N., Bakry, A. S., Abbassy, M. A., Linjawi, A. I., & Hassan, A. H. (2023). Evaluation of Resin Infiltration, Fluoride and the Biomimetic Mineralization of CPP-ACP in Protecting Enamel after Orthodontic Inter-Proximal Enamel Reduction. Biomimetics, 8(1), 82. https://doi.org/10.3390/biomimetics8010082