Abstract
Obesity is a risk factor for coronary atherosclerosis. However, the influence of adipose tissue in carotid atherosclerosis is not completely understood. No systematic review/meta-analysis was previously performed to understand if obesity is a risk factor for carotid atherosclerosis. This paper aims to provide an opportunistic review of the association between obesity and carotid atherosclerosis and define the role of the different adipose tissue depots in the characteristics of carotid stenosis. The databases PubMed and Cochrane Library were searched on 15–27 April and 19 May 2021. A total of 1750 articles published between 1985 and 2019 were identified, 64 were preselected, and 38 papers (35,339 subjects) were included in the final review. The most frequent methods used to determine obesity were anthropometric measures. Carotid plaque was mostly characterized by ultrasound. Overall obesity and visceral fat were not associated with the presence of carotid plaque when evaluated separately. Waist-hip ratio, however, was a significant anthropometric measure associated with the prevalence of carotid plaques. As it reflected the ratio of visceral and subcutaneous adipose tissue, the balance between these depots could impact the prevalence of carotid plaques.
1. Introduction
The worldwide prevalence of obesity has increased in the past decades. Obesity is an independent risk factor for atherosclerosis, stroke, and cardiovascular disease [1,2,3]. Cardiovascular outcomes and mortality are more dependent on fat distribution than on the total amount of adipose tissue [1]. Previous studies demonstrated that a higher ratio of visceral adipose tissue (VAT) to subcutaneous adipose tissue (SAT) was associated with an increased risk of poor cardiovascular outcomes [1]. VAT is metabolically active and secret adipokines that cause vascular inflammation and insulin resistance [2]. Conversely, SAT is associated with a neutral or even beneficial metabolic impact [2].
Increased abdominal VAT/SAT ratio was inversely correlated with the extent and severity of coronary artery plaques, higher total mortality, and incidence of major adverse cardiac events (MACE) [1,2].
The influence of obesity on carotid atherosclerosis disease remains unclear [4]. No previous systematic review/metanalyses evaluated the relationship between obesity on carotid atherosclerosis.
2. Methods
2.1. Data Sources and Search
The PubMed and Cochrane Library databases were searched on 15–27th of April and 19 May 2021. The query was as follows:
(‘Carotid artery stenosis OR ‘Carotid artery atherosclerosis’) AND (‘visceral adipose tissue’ OR ‘visceral fat’ OR ‘fat tissue’ OR ‘Obesity’ OR ‘subcutaneous adipose tissue’ OR ‘subcutaneous fat’).
This review was conducted according to established methods for reviews in cardiovascular medicine (PRISMA criteria).
2.2. Inclusion and Exclusion Criteria
Studies were included in the current opportunistic review if they met the following criteria: (1) correlating general obesity, VAT, or SAT with the prevalence of carotid artery plaque, (2) evaluating the influence of general obesity, VAT/SAT on carotid artery symptomatology, (3) retrospective or prospective observational clinical studies, (4) performed in humans, (5) full-text available, (6) studies published in English, French, Spanish, and Portuguese.
Other studies were excluded for the following reasons: (1) analyzing intima-media thickness, (2) performed in children, (3) studies reported only as abstracts or with incomplete data, letters, reviews, case reports, nonclinical studies, (4) reviews or meta-analysis.
If the studies had overlapping subjects, the one with the largest sample size was included in the final analysis.
No attempt was made to contact the authors of the included studies to enquire about missing or incomplete data. No studies were excluded because of concerns about missing data.
2.3. Data Extraction—Outcomes-Definitions
After removing the duplicated articles, two authors (J.F. and A.C.) independently selected the full-text articles after screening the title and abstract. Disagreements were resolved by consensus.
For each study, the subsequent data were collected: first author, year of publication, country of the research center, type of study design, total number of patients, age, men (percentages), aims, inclusion and exclusion criteria, and main conclusions (Table 1, Table 2 and Table 3).

Table 1.
Characteristics of the studies included in the opportunistic review.
Table 2.
Study aims, inclusion and exclusion criteria, methods to study adipose tissue.
Table 3.
Data collected about carotid plaque and conclusion.
Concerning the adipose tissue, the following information was recorded: the method used to determine the overall obesity, the VAT, and SAT (Table 3).
The information collected about carotid stenosis were: imaging methods used to determine the presence of carotid stenosis; the definition of carotid plaque; the grade of carotid stenosis; and if the carotid plaque was symptomatic (Table 3).
The quality of each study was assessed by one author (J. F.) using the MINORS (methodological index for non-randomized studies) criteria (see supplement material) [41]. Each item was scored as 0 (not reported), 1 (reported but inadequate), or 2 (re-ported and adequate). The global ideal score is 16 for non-comparative studies and 24 for comparative studies [41]. The final classification is presented in Table 1.
3. Results
A total of 1750 articles were found, and after removing duplicates, 1201 articles were left, as shown in Figure 1 [42,43,44,45,46,47,48,49].
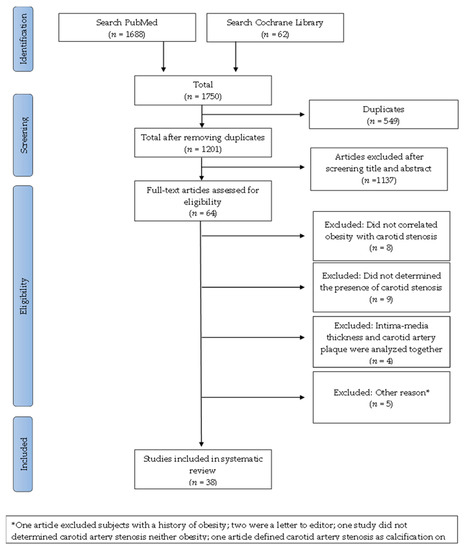
Figure 1.
Flow diagram for this opportunistic review that aims to analyze the correlation between obesity and carotid atherosclerosis.
Of the 64 papers, 26 were rejected after reading the full text due to the following reasons: eight articles did not correlate obesity with carotid artery stenosis [42,43,44,45,46,47,48,49]; Nine did not determine the presence of carotid artery stenosis [50,51,52,53,54,55,56,57,58]; In four articles, intima-media thickness and carotid artery plaque were both correlated with obesity [59,60,61,62]; One article excluded subjects with a history of obesity [63]; Two papers were a letter to the editor [52,64]; One study did not measure carotid artery stenosis or obesity [65]; One article defined carotid artery stenosis as calcification seen on radiographs [66].
The 38 studies included in this opportunistic review were published in 1985 (one article) and between 2001 and 2019. The studies were conducted in 32 different countries, the majority in Europe (18 papers), eight studies in North America, eight in Asia, two in South America, and two in Africa (Table 1).
Analyzing the studies included in this opportunist review by regions, there was a higher number of papers describing a positive association between obesity and carotid plaque characteristics in the research work performed in Asia and Africa. However, just two papers were identified from Africa. The majority of papers included were from Europe, where 10 papers found a relationship and an equal number did not.
- -
- The majority of the studies (34) were cross-sectional, and four were longitudinal.
- -
- A total of 35,339 subjects (49.20% men) were included: 26,492 from Europe, 4239 from Asia, 3859 from North America, 384 from South America, and 365 from Africa (Table 1). Some studies only included a specific group of patients: Type 2 diabetes (5 papers), women (4), patients with an autoimmune disease (4), or hypertension (3) (Table 2).
The authors used different methods to determine the quantity of adipose tissue and to characterize the atherosclerotic plaque. The most frequent method used to determine obesity was anthropometric measures: Thirty-three articles assessed overall obesity with BMI, 19 evaluated visceral obesity with WC, and 11 estimated the relationship between the visceral and subcutaneous adipose tissue with WHR (Table 2). Six authors used medical imaging to quantify the VAT and SAT: Four authors used CT scans [3,8,26,31], one author used ultrasound [40], and another MRI [28]. Other methods were used: bioimpedance (three papers) [9,17,37]; dual-energy X-ray absorptiometry (two) [3,36]; and DXA (one) [8] (Table 2). In one paper, omental, mesenteric, mesocolon, and perirenal fat were dissected after the autopsy and weighed [33]. The VAT was the sum of the omental, mesenteric, mesocolon, and perirenal fat [33].
The carotid plaque was evaluated with ultrasound in 19 articles, with doppler ultrasound in 12 papers, and with MRI in three articles (Table 3).
Two articles analyzed the histological composition of the carotid plaque (number of macrophages, foam cells, cap characteristics, and the quantity of lipids and calcium) [4,19]. One study determined the area of the cadavers of the largest atheroma plaque in the carotid artery of cadavers to calculate the stenosis index [33].
The carotid plaque was defined in most papers as a focal structure encroaching the vessel lumen or as a widening in the intima media-thickness (Table 3). However, there was no homogeneity in the definition, and different publications used different measures of intima-media thickness to define a plaque (Table 3). Sixteen articles only analyzed asymptomatic carotid plaques, six papers studied both symptomatic and asymptomatic, and two articles symptomatic. Fourteen articles did not specify if the carotid artery caused symptomatology. (Table 3). This opportunistic review included 1533 symptomatic and 19,799 asymptomatic patients.
3.1. Overall Obesity and the Prevalence of Carotid Plaques
Overall obesity, determined by BMI, was not associated with the presence of carotid plaques in 15 papers, totaling 13,215 patients (Figure 2) [3,9,10,12,14,15,18,21,25,28,30,31,35,39,40].
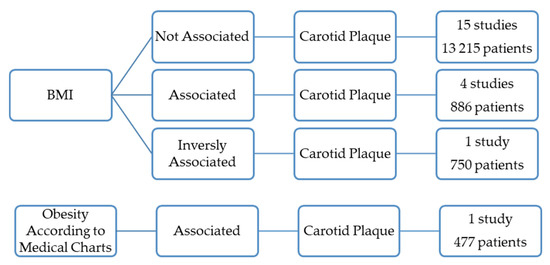
Figure 2.
Results of the studies that correlate overall obesity with the presence of the carotid atherosclerotic plaques.
Five studies (1363 patients) found, however, a positive association between the prevalence of carotid plaques and overall obesity (Figure 2) [5,11,16,27,34].
One of these was a prevalence study conducted on 474 healthy residents in Northeast China [27]. This study sought to determine the risk factors associated with carotid atherosclerosis identified by ultrasound. However, there was no definition of atherosclerotic plaque [27]. The prevalence was significantly higher in obese females than in the control females. Obesity was defined as BMI ≥ 28 kg/m2 [27]. The study included 231 males, and no association was found for this gender [27].
Another study conducted on 144 women with systemic lupus erythematous found that the prevalence of carotid artery plaque was significantly associated with obesity, determined by BMI [11].
The oldest study included in this review included 477 patients who performed angiography or Doppler ultrasound and concluded that obesity was significantly more frequent in patients with internal artery occlusion or stenosis than in controls. Obesity was defined according to medical charts [5].
Two papers totaling 268 patients found that the prevalence of carotid plaques was associated with overall obesity determined by BMI [16,34].
However, one paper with 750 individuals concluded that the prevalence of carotid artery plaques was inversely related to BMI (Figure 2) [7].
3.2. Overall Obesity and the Characteristics of the Carotid Plaques
Three papers suggested that overall obesity could be associated with carotid plaque instability (Figure 3) [4,24,36].
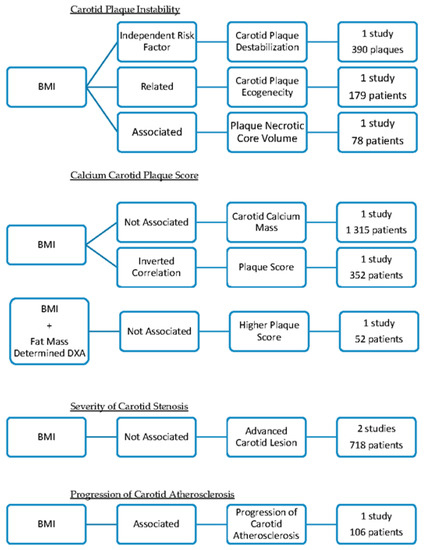
Figure 3.
Summary of the studies that correlate overall obesity with the characteristics of the carotid atherosclerotic plaques.
- (1).
- Histological analysis of carotid plaques (390) concluded that obesity, defined as BMI ≥ 30 kg/m2 was an independent risk factor for carotid plaque destabilization, particularly in males [4]. Obesity was correlated with the presence of unstable carotid plaques, characterized by a high degree of inflammation, thinning, and rupture of the cap [4].
- (2).
- One study analyzed the plaque echogenicity by gray-scale median using ultrasound and concluded that low gray-scale median values were related to high BMI [24]. Plaques with a low gray-scale median had a higher probability of causing embolization and symptoms. This research included 179 diabetic patients [24].
- (3).
- One research paper found that obesity (BMI > 30.0 kg/m2) was associated with increased carotid plaque necrotic core volume and calcification independently of diabetes mellitus status [36]. The carotid plaque composition was assessed by magnetic resonance imaging. Obesity was determined by BMI [36]. The study included 78 patients with short-duration Type 2 diabetes mellitus and 91 sex- and aged-matched control subjects [36].
This opportunistic review identified three articles that found that obesity did not correlate with calcium score or carotid plaque score (Figure 3) [8,26,37].
- (1).
- No association was found between BMI and calcium mass score of the carotid arteries determined with a CT scan [26]. This study was performed on 1315 diabetic patients [26].
- (2).
- One study found that the measures of adiposity (BMI, the systemic fat mass, and the fat-free mass determined with DXA) were not significantly different in patients with higher plaques score [8]. For each segment, the degree of plaque was graded as follows: 0 = no plaque; 1 = 1 small plaque. <30% of vessel diameter; 2 = 1 medium plaque between 30% of vessel diameter or multiple small plaques; and 3 = 1 large plaque >50% of the vessel diameter or multiple plaques with at least 1 medium plaque [8]. The grades were summed across the right and left carotid arteries to create an overall measure of the extent of focal plaque [8]. This study included 52 patients [8].
- (3).
- One paper found an inverse correlation between BMI and plaque score, defined as the total plaque thickness for the visualization sites in the IMT measurement on the right and left size [37]. The study was performed on 352 rheumatoid arthritis patients [37].
Two different papers did not find any relation between BMI and the severity of atherosclerotic plaque (Figure 3) [19,23].
- (1).
- A histological study analyzed the relationship between obesity and the severity of atherosclerosis carotid plaque [19]. The atherosclerotic lesions were described according to the American Heart Association classification [19]. BMI did not independently predict the risk of developing advanced carotid atherosclerotic lesions (including 185 cadavers of men and women) [19].
- (2).
- No association was found between obesity (BMI > 27 kg/m2) and carotid stenosis ≥ 50% (determined with NASCET criteria) in 533 patients [23]. In this study, there was no association between obesity and symptomatic carotid stenosis [23].
Another paper concluded that obesity (determined by BMI) was associated with the progression of carotid atherosclerosis, studied with magnetic resonance [29]. This research project determined the change in the carotid artery wall in 106 hyperlipidemic participants during the course of treatment with statins (Figure 3) [29].
3.3. Visceral Adipose Tissue and the Prevalence of Carotid Plaque
Nineteen articles analyzed the relationship between VAT and carotid stenosis.
Eight papers performed in 12,444 patients showed no association between waist circumference (WC) and the presence of carotid plaques [9,13,15,16,22,25,35,39,40]. Three studies, however, found that the presence of plaque was associated with WC in 1271 subjects (Figure 4) [7,21].
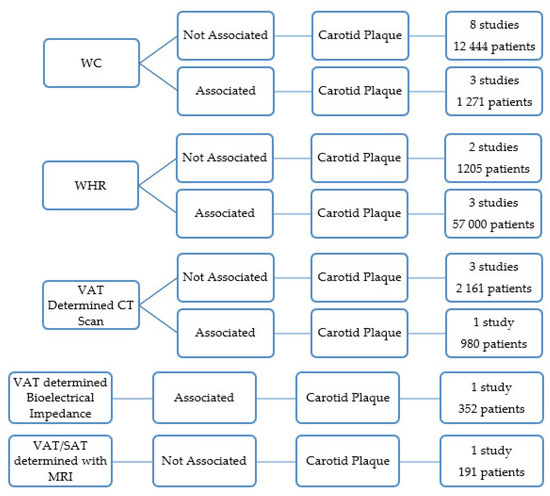
Figure 4.
Results of the papers correlating visceral obesity with the presence of the carotid atherosclerotic plaques.
Three other studies that included 5 700 subjects found that WHR was associated with the prevalence of carotid plaques (Figure 4) [15,35,38].
WHR was significantly related to the presence of carotid artery plaque in African Caucasian women, whereas none of the obesity measures were associated with carotid artery plaque in black women [18]. The study was limited to 203 African black and African Caucasian women who met the American College of Rheumatology criteria for rheumatoid arthritis (Figure 4) [18].
In two research works, there was no association between WHR and the presence of carotid plaques (1205 subjects) (Figure 4) [9,28].
A research work analyzed the relationship between new anthropometric measures that reflected the quantity of abdominal adipose tissue and the carotid plaque [39]. The anthropometric measures were the A Body Shape Index (ABSI) and Body Roundness Index (BRI) [39]. ABSI was independently associated with the presence of carotid atherosclerotic plaque. The study included 468 subjects with arterial hypertension [39].
Four articles used CT scans to quantify the VAT and another used MRI [3,8,26,28,31]. The VAT area determined with a CT scan in 980 healthy Japanese was independently associated with cervical plaque [31]. In three studies with 2161 subjects, the VAT area determined with a CT scan was not associated with the presence of carotid plaques [3,8,26]. One paper published the relationship between VAT and SAT as determined by MRI and the presence of carotid plaque [28]. The study included 191 subjects, and no relation was found between the variables (Figure 4) [28].
One paper concluded that VAT measured with bioelectrical impedance was associated with a higher prevalence of atherosclerotic carotid plaques [37]. This study was limited to 352 patients with rheumatoid arthritis (Figure 4) [37].
3.4. Visceral Adipose Tissue and the Characteristics of the Carotid Plaque
A research work of 112 subjects found that increased fat mass (determined with bioimpedance) correlates with carotid plaque vulnerability, as expressed by the gray scale median score (Figure 5) [17].
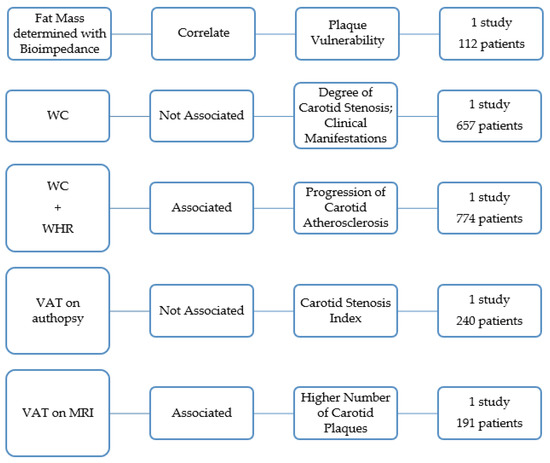
Figure 5.
Overview of the studies that analyze the association between visceral obesity and the characteristics of the carotid atherosclerotic plaques.
A research work determined WC in 657 patients with symptoms of cerebral ischemia and carotid stenosis of ≥50% [20]. The author concluded that patients with and without abdominal obesity did not significantly differ either in the degree of carotid stenosis or in the degree of its clinical manifestation [20]. Haberka also reached a similar conclusion determining the central obesity with WC and ultrasound [8]. In this study, the amount of visceral fat was not related to carotid stenosis severity (Figure 5) [40].
A study in 774 men without atherosclerosis showed that abdominal obesity, as indicated by high WHR and high WC, was associated with accelerated progression of carotid atherosclerosis independent of overall obesity and other risk factors in middle-aged men with no prior atherosclerotic diseases (Figure 5) [6].
An autopsy study with 240 deceased subjects concluded that VAT was not associated with carotid artery stenosis index [33]. The VAT was the sum of the weight of the omental, mesenteric, mesocolon and perirenal fat [33]. The largest atheroma plaque in the carotid artery was determined [33]. The stenosis index was calculated by subtracting the lumen area from the outer area, dividing the difference by the outer area, and multiplying the result by 100 (Figure 5) [33].
One paper showed that subjects with the highest amount of VAT were more prone to have more than one carotid plaque compared to participants showing the highest values of SAT or other conventional anthropometric indices [28]. The quantity of VAT and SAT was quantified by MRI in 191 subjects (Figure 5) [28].
3.5. Subcutaneous Adipose Tissue and Carotid Plaque
Six studies evaluated SAT, and none found any relationship with carotid plaques [3,8,26,28,31,40].
4. Discussion and Conclusions
To the best of our knowledge, this is the first opportunistic review analyzing the relationship between obesity and carotid artery disease.
The general assumption emerging from our analysis suggests no association between overall obesity (determined with BMI) or visceral obesity (determined in the majority of the studies with WC) and the presence of carotid plaque. However, three studies (5700 patients) found that WHR was associated with the prevalence of carotid plaques [15,35,38]. BMI is not always a measure of fatness. Individuals with more muscle mass may be incorrectly classified as obese [67]. BMI has poor specificity for excess adiposity, and it does not characterize the excess of centrally distributed obesity [68]. Low BMI values may also be associated with the loss of lean body mass (muscle) [68]. In contrast with BMI, WC and WHR specifically address abdominal obesity and correlate better with overall atherosclerotic disease prevalence [68]. WC and WHR may correlate better with body fatness [67] and may more accurately reflect the additional risk conferred by obesity [68]; actually, they are more associated with mortality and cardiovascular events than BMI [68].
Although WC is well-described as a measure of VAT and a marker of obesity’s associated metabolic risks, WHR has superior performance in estimating atherosclerotic risk [68]. One possible explanation is that WHR is an indexed value (to lower body girth) and provides a more precise assessment of relative central adiposity across the spectrum of body size, compared with WC [68]. WHR is considered the main anthropometric measure of central obesity [15,35,38]. Another explanation is that increased hip circumference may protect against atherosclerosis [68]. Fat in the lower body may function as a protective reservoir against ectopic (abdominal) adiposity [68]. WHR is independently associated with prevalent atherosclerosis and provides better dis- crimination than either BMI or WC [68].
There is a correlation between the WHR and the ratio of VAT-to-SAT cross-sectional area (quantified by CT images taken in the abdominal region) [69]. VAT is an endocrine organ that can secrete adipokines, including cytokines and chemokines [70,71]. VAT is associated with cardiovascular disease and can be used as a cardiometabolic risk marker, while SAT has a beneficial metabolic impact in the opposite direction [71]. Abdominal visceral fat correlates with the prevalence of coronary artery disease and mortality. Subcutaneous fat may play a protective role against the development of coronary artery disease by improving insulin sensitivity or the secretion of adipokines. The VAT/SAT ratio is a unique parameter relevant to vascular inflammation or poor cardiovascular outcomes [71,72]. VAT/SAT ratio is associated with a higher total mortality and incidence of MACE, independently of traditional vascular risk factors, and with the presence of obstructive coronary artery disease [2].
In this review, we found a relationship between obesity and other characteristics of carotid atherosclerotic plaque. Overall obesity (738 patients) [4,24,36] and an increase in fat mass (112 patients) [17] were associated with carotid plaque instability. Obesity and visceral fat (880 patients) are correlated with the progression of carotid atherosclerosis [6,29]. However, no study related obesity to carotid artery symptomatology.
Studies conducted with cardiac patients found that obesity was also positively associated with the progression of coronary plaque [72,73]. Excess VAT is correlated with higher serum levels of fasting glucose, triglycerides, lower HDL cholesterol, greater prevalence of hypertension, tobacco use, and artery inflammation [72,73]. The systemic inflammation causes endothelial dysfunction, formation, and progression of atherosclerotic plaques [73,74]. Importantly, inflammation is also responsible for atherosclerotic plaque instability [43]. These biological facts could also explain why in this opportunistic review, we found that obesity did not correlate with calcium score, carotid plaque score [8,26,37], or the severity of atherosclerotic plaque [19,20,23,40].
None of the studies included in this review found any relationship between SAT and carotid plaques [3,8,26,28,31,40]. Further studies to characterize the subcutaneous fat should be developed.
4.1. Strengths and Limitations
A key strength of this review is the standardized data extraction, the quality assessment procedures, and searches conducted by two authors. This manuscript covers a broader range of patients and countries from 1985 to 2019 (most articles were published in the last 10 years). It includes published research in English, French, Portuguese, and Spanish language journals. The main limitation of this revision is that it did not conduct a meta-analysis. The articles included are not homogenous. There are different definitions of carotid plaque and obesity. The authors included different subjects and used different methods to determine obesity and carotid plaque. The opportunistic review included observational studies, and its bias was not entirely avoided.
Another bias of this study is the inability to determine the impact of obesity on atherosclerotic plaque independently of the cardiovascular risk. Obesity can increase the prevalence of certain factors such as dyslipidemia which contributes to atherosclerosis. However, there was no description of cardiovascular risk factors in all included papers.
Another limitation is that two research questions were not answered: (i). We did not find the relation between VAT and symptomatic carotid artery disease (ii). neither was the role played by subcutaneous tissue in carotid stenosis.
4.2. Implications for Practice
The results of the current investigation provide key information for practice. First, the importance of determining the WHR to infer the relation between VAT and SAT. The BMI, more frequently used in clinical activity, can erroneously represent the cardiovascular risk. Secondly, it may be useful to address obese patients to increase lean body mass. This study also has an impact on future research. The authors should use rigorous methods to determine obesity to homogenize the results, and facilitate the comparisons accurately. The role of subcutaneous tissue in carotid atherosclerosis still needs more investigations to clearly determine its role in vascular diseases. The relationship between obesity, subcutaneous fat, and carotid symptomatology should be more deeply investigated. Behavioral and pharmacological interventions could be developed to decrease the VAT/SAT ratio. Studies focused on obesity and inflammation could be important in atherosclerosis control.
4.3. Concluding Remarks
Considering the data analyzed, obesity and visceral obesity were not associated with the presence of carotid plaque. The ratio between VAT and SAT could influence the prevalence of carotid plaques. Obesity could be related to carotid plaque instability and progression, but its association with carotid symptomatology has not been proved and should be investigated in future studies.
Author Contributions
Conceptualization, J.F.; Writing—original draft preparation, J.F. and A.C.; Formal Analysis, J.F. and A.C.; Investigation, J.F., P.C. and I.V.; Design, P.C.; Writing—review and editing, P.C., A.L.-F., A.M. (Amílcar Mesquita), J.C., A.M. (Armando Mansilha) and M.C.-N.; Validation, P.C., I.V., C.C., C.S., A.L.-F., A.M. (Amílcar Mesquita), J.C., A.M. (Armando Mansilha) and M.C.-N.; Supervision, A.M. (Armando Mansilha). All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Portuguese Society of Vascular Surgery. This work was developed under the scope of project NORTE-01-0145-FEDER- 000013, supported by the Northern Portugal Regional Operational Programme (NORTE 2020) under the Portugal Partnership Agreement, through the European Regional Development Fund (FEDER), and by National funds, through the Foundation for Science and Technology (FCT)—project UIDB/50026/2020 and UIDP/50026/2020.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
We thank Rita Alonso for structuration of this article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
BMI—body mass index; BSA—body surface area BRI—body roundness index; ABSI—a body shape index; CT scan—computerized tomography scan; DXA—Dual-energy X-ray absorptiometry; HC—hip circumference; IMT—intima-media thickness; MACE—major adverse cardiac events; MINORS—methodological index for non-randomized studies; MRI—magnetic resonance imaging; NA—not applicable; NASCET—North American symptomatic carotid endarterectomy trial; VAT—visceral adipose tissue; SAT—subcutaneous adipose tissue; WC—waist circumference; WHR—waist-to-hip ratio; WHtR—waist-to-height ratio.
References
- Tanaka, T.; Kishi, S.; Ninomiya, K.; Tomii, D.; Koseki, K.; Sato, Y.; Okuno, T.; Sato, K.; Koike, H.; Yahagi, K.; et al. Impact of abdominal fat distribution, visceral fat, and subcutaneous fat on coronary plaque scores assessed by 320-row computed tomography coronary angiography. Atherosclerosis 2019, 287, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Ladeiras-Lopes, R.; Sampaio, F.; Bettencourt, N.; Fontes-Carvalho, R.; Ferreira, N.; Leite-Moreira, A.; Gama, V. The Ratio Between Visceral and Subcutaneous Abdominal Fat Assessed by Computed Tomography Is an Independent Predictor of Mortality and Cardiac Events. Rev. Española De Cardiol. 2017, 70, 331–337. [Google Scholar] [CrossRef]
- Lear, S.; Humphries, K.; Kohli, S.; Frohlich, J.; Birmingham, C.; Mancini, J. Visceral Adipose Tissue, a Potential Risk Factor for Carotid Atherosclerosis Results of the Multicultural Community Health Assessment Trial (M-CHAT). Stroke 2007, 38, 2422–2429. [Google Scholar] [CrossRef] [PubMed]
- Rovella, V.; Anemona, L.; Cardellini, M.; Scimeca, M.; Saggini, A.; Santeusanio, G.; Bonanno, E.; Montanaro, M.; Legramante, I.M.; Ippoliti, A.; et al. The role of obesity in carotid plaque instability: Interaction with age, gender, and cardiovascular risk factors. Cardiovasc. Diabetol. 2018, 17, 1–9. [Google Scholar] [CrossRef]
- Bogousslavsky, J.; Regli, F.; Melle, V. Risk factores and Concomitants of Internal Carotid Artery Occlusion or Stenosis. Arch. Neuril. 1985, 42, 864–867. [Google Scholar] [CrossRef]
- Lakka, T.; Lakka, M.; Salomen, R.; Kaplan, G.; Salomen, J. Abdominal obesity is associated with accelerated progression of carotid atherosclerosis in men. Atherosclerosis 2001, 154, 497–505. [Google Scholar] [CrossRef]
- Hunt, K.J.; Duggirala, R.; Göring, H.H.; Williams, J.T.; Almasy, L.; Blangero, J.; O’Leary, D.H.; Stern, M.P. Genetic Basis of Variation in Carotid Artery Plaque in the San Antonio Family Heart Study. Stroke 2002, 33, 2775–2780. [Google Scholar] [CrossRef]
- Hegazi, R.A.; Sutton-Tyrrell, K.; Evans, R.W.; Kuller, L.H.; Belle, S.; Yamamoto, M.; Edmundowicz, D.; Kelley, D.E. Relationship of Adiposity to Subclinical Atherosclerosis in Obese Patients with Type 2 Diabetes. Obes. Res. 2002, 11, 1597–1605. [Google Scholar] [CrossRef]
- Czernichow, S.; Bertrais, S.; Oppert, J.-M.; Galan, P.; Blacher, J.; Ducimetière, P.; Hercberg, S.; Zureik, M. Body composition and fat repartition in relation to structure and function of large arteries in middle-aged adults (the SU.VI.MAX study). Int. J. Obes. 2005, 29, 826–832. [Google Scholar] [CrossRef]
- Hadjiev, D.; Mineva, P.; Vukov, M. Multiple modifiable risk factores for first ischemic stroke: A population-based epidemiological study. Eur. J. Neurol. 2003, 10, 577–582. [Google Scholar] [CrossRef]
- De Souza, A. Atherosclerotic plaque in carotid arteries in systemic lupus erythematosus: Frequency and associated risk factors. São Paulo Med. J. 2005, 123, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Montalcini, T.; Gorgone, G.; Gazzaruso, C.; Sesti, G.; Perticone, F.; Pujia, A. Carotid atherosclerosis associated to metabolic syndrome but not BMI in healthy menopausal women. Diabetes Res. Clin. Pract. 2007, 76, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Kwon, H.-M.; Roh, J.-K. Metabolic syndrome is more associated with intracranial atherosclerosis than extracranial atherosclerosis. Eur. J. Neurol. 2007, 14, 379–386. [Google Scholar] [CrossRef]
- Irace, C.; Scavelli, F.; Carallo, C.; Serra, R.; Cortese, C.; Gnasso, A. Body mass index, metabolic syndrome and carotid atherosclerosis. Coron. Artery Dis. 2009, 20, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Ho, S.; Chan, S.; Woo, J.; Ahuja, A. Carotid atherosclerosis and the risk factors in early postmenopausal Chinese women. Maturitas 2009, 63, 233–239. [Google Scholar] [CrossRef]
- Terzis, I.D.; Papamichail, C.; Psaltopoulou, T.; Georgiopoulos, G.A.; Lipsou, N.; Chatzidou, S.; Kontoyiannis, D.; Kollias, G.; Iacovidou, N.; Zakopoulos, N.; et al. Long-Term BMI Changes Since Adolescence and Markers of Early and Advanced Subclinical Atherosclerosis. Obesity 2011, 20, 414–420. [Google Scholar] [CrossRef]
- Kadoglou, N.P.E.; Sailer, N.; Moumtzouoglou, A.; Kapelouzou, A.; Gerasimidis, T.; Kostakis, A.; Liapis, C.D. Adipokines: A novel link between adiposity and carotid plaque vulnerability. Eur. J. Clin. Investig. 2012, 42, 1278–1286. [Google Scholar] [CrossRef]
- Solomon, A.; Norton, G.R.; Woodiwiss, A.J.; Dessein, P.H. Obesity and carotid atherosclerosis in African black and Caucasian women with established rheumatoid arthritis: A cross-sectional study. Arthritis Res. Ther. 2012, 14, R67. [Google Scholar] [CrossRef]
- Rodríguez-Flores, M.; Rodríguez-Saldaña, J.; Cantú-Brito, C.; Aguirre-García, J.; Alejandro, G. Prevalence and severity of atherosclerosis in different arterial territories and its relation with obesity. Cardiovasc. Pathol. 2013, 22, 332–338. [Google Scholar] [CrossRef]
- Maksimovic, M.; Vlajinac, H.; Radak, D.; Marinkovic, J.; Maksimovic, J.; Jorga, J. Relationship between Abdominal Obesity and Other Cardiovascular Risk Factors: Cross Sectional Study of Patients with Symptomatic Carotid Disease. Srp. Arh. Celok. Lek. 2013, 141, 460–465. [Google Scholar] [CrossRef]
- Galarza-Delgado, D.A.; Esquivel-Valerio, J.A.; Garza-Elizondo, M.A.; Góngora-Rivera, F.; Muñoz-De Hoyos, J.L.; Serna-Pena, G. Carotid atherosclerosis in patients with rheumatoid arthritis and rheumatoid nodules. Reum. Clin. 2013, 9, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Cuspidi, C.; Sala, C.; Lonati, L.; Negri, F.; Rescaldani, M.; Re, A.; Meani, S.; Mancia, G. Metabolic syndrome, left ventricular hypertrophy and carotid atherosclerosis in hypertension: A gender-based study. Blood Press. 2013, 22, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Chiquete, E.; Torres-Octavo, B.; Cano-Nigenda, V.; Valle-Rojas, D.; Domínguez-Moreno, R.; Tolosa-Tort, P.; Flórez-Cardona, J.A.; Flores-Silva, F.; Reyes-Melo, I.; Higuera-Calleja, J.; et al. Caracterización de factores asociados con estenosis carotídea en una población de alto riesgo. Rev. Neurol. 2014, 58, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Irie, Y.; Katakami, N.; Kaneto, H.; Takahara, M.; Sakamoto, K.; Kosugi, K.; Shimomura, I. The risk factors associated with ultrasonic tissue characterization of carotid plaque in type 2 diabetic patients. J. Diabetes Its Complicat. 2014, 28, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.; Liang, Y.; Jiang, H.; Cai, C.; Sun, B.; Qiu, C. Metebolic Syndrome and Subclinical Carotid Atherosclerosis Among Chinese Elderly People Living in a Rural Community. Metab. Syndr. Relat. Disord. 2014, 12, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Hsu, F.-C.; Bowden, N.W.; Xu, J.; Smith, S.C.; Wagenknecht, L.E.; Comeau, M.E.; Divers, J.; Register, T.C.; Carr, J.J.; et al. Relationships Between Measures of Adiposity with Subclinical Atherosclerosis in Patients with Type 2 Diabetes. Obesity 2016, 24, 1810–1818. [Google Scholar] [CrossRef]
- Pan, X.; Lai, Y.; Gu, J.; Wang, H.; Liu, A.; Shan, Z. Factors Significantly Associated with the Increased Prevalence of Carotid Atherosclerosis in a Northeast Chinese Middle-aged and Elderly Population. Medicine 2016, 95, 1–7. [Google Scholar] [CrossRef]
- Radmard, A.R.; Poustchi, H.; Ansari, L.; Khorasanizadeh, F.; Yoonessi, A.; Taheri, A.P.H.; Rahmanian, M.S.; Jafari, E.; Malekzadeh, R.; Merat, S. Abdominal fat distribution and carotid atherosclerosis in a general population: A semi-automated methods using magnetic resonance imaging. Jpn. J. Radiol. 2016, 34, 414–422. [Google Scholar] [CrossRef]
- Sandfort, V.; Lai, S.; Ahlman, M.A.; Mallek, M.; Liu, S.; Sibley, C.T.; Turkbey, E.B.; Lima, J.A.C.; Bluemke, D.A. Obesity Is Associated with Progression of Atherosclerosis During Statin Treatment. J. Am. Heart Assoc. 2016, 5, e003621. [Google Scholar] [CrossRef]
- Mitevska, I.; Baneva, N.; Bosevski, M.; Kostovska, E. Prevalence of risk factors and asymptomatic carotid atherosclerosis in diabetic patients screened for silent myocardial ischemia by SPECT myocardial imaging. Nucl. Med. Ver. 2017, 20, 3–9. [Google Scholar] [CrossRef][Green Version]
- Higuchi, S.; Kabeya, Y.; Kato, K. Visceral-to-subcutaneous fat ratio is independently related to small and large cerebrovascular lesions even in healthy subjects. Atherosclerosis 2017, 259, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Gerdts, E.; Losi, M.A.; D’Amato, A.D.; Manzi, M.V.; Canciello, G.; Trimarco, V.; De Luca, N.; Simonse, G.; Izzo, R. Differential effect of obesity on prevalence of cardiac and carotid target organ damage in hypertension (The Campania Salute Network). Int. J. Cardiol. 2017, 244, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, A.; Suemoto, C.K.; Farias-Itao, D.S.; Campos, F.M.; Silva, K.C.S.; Bittencourt, M.S.; Grinberg, L.T.; Leite, R.E.P.; Ferretti-Rebustini, R.E.L.; Farfel, J.M.; et al. Morphometric measurements of systemic atherosclerosis and visceral fat: Evidence from na autopsy study. PLoS ONE 2017, 12, e0186630. [Google Scholar] [CrossRef]
- Omisore, A.; Famurewa, O.; Komolafe, M.; Asaleya, C.; Fawale, M.; Afolabi, B. Association of traditional cardiovascular risk factors with carotid atherosclerosis among adults at a teaching hospital in South-western Nigeria. Cardiovasc. J. Afr. 2018, 28, 183–188. [Google Scholar] [CrossRef]
- Imahori, Y.; Mathiesen, E.B.; Leon, D.A.; Hopstock, L.A.; Hughes, A.D.; Johnsen, S.H.; Jørgensen, L.; Emaus, N.; Morgan, K.E. The contribution of obesity to carotid atherosclerotic plaque burden in a general population sample in Norway: The Tromsø Study. Atherosclerosis 2018, 273, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Laugesen, E.; Høyem, P.; Thrysoe, S.; Hansen, E.S.S.; Mikkelsen, A.F.S.; Kerwin, W.S.; Poulsen, P.L.; Hansen, T.K.; Kim, W.Y. Negative Carotid Artery Remodeling in Early Type 2 Diabetes Mellitus and Increased Carotid Plaque Vulnerability in Obesity as Assessed by Magnetic Resonance Imaging. J. Am. Heart Assoc. 2018, 7, e008677. [Google Scholar] [CrossRef]
- Yoshida, T.; Hashimoto, M.; Kawahara, R.; Yamamoto, H.; Tanaka, M.; Ito, H.; Masuda, I.; Hosoda, K.; Yamamoto, W.; Uozumi, R.; et al. Non-obese visceral adiposity is associated with the risk of atherosclerosis in Japanede patients with rheumatoid arthritis: A cross-sectional study. Rheumatol. Int. 2018, 38, 1679–1689. [Google Scholar] [CrossRef] [PubMed]
- Scicali, R.; Rosenbaum, D.; Pino, A. Na increased waist-to-hip ratio is a key determinant of a atherosclerotic burden in overweight subjects. Acta Diabetol. 2018, 55, 741–749. [Google Scholar] [CrossRef]
- Geraci, G.; Zammuto, M.; Gaetani, R.; Mattina, A.; D’Ignoto, F.; Geraci, C.; Noto, D.; Averna, M.; Cottone, S.; Mulè, G. Relationship of a Body Shape Index and Body Roundness Index With carotid atherosclerosis in arterial hypertension. Nitrition Metab. Cardiovasc. Dis. 2019, 29, 822–829. [Google Scholar] [CrossRef]
- Haberka, M.; Skilton, M.; Biedroń, M.; Szostak-Janiak, K.; Partyka, M.; Matla, M.; Gąsior, Z. Obesity, visceral adiposity and carotid atherosclerosis. J. Diabetes Its Complicat. 2019, 33, 302–306. [Google Scholar] [CrossRef]
- Buford, T.W.; Anton, S.D.; Judge, A.R.; Marzetti, E.; Wohlgemuth, S.E.; Carter, C.S.; Leeuwenburgh, C.; Pahor, M.; Manini, T.M. Models of accelerated sarcopenia: Critical pieces for solving the puzzle of age-related muscle atrophy. Ageing Res. Rev. 2010, 9, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Puttonen, S.; Kivimäki, M.; Elovainio, M.; Pulkki-Råback, L.; Hintsanen, M.; Vahtera, J.; Telama, R.; Juonala, M.; Viikari, J.S.; Raitakari, O.T.; et al. Shift work in young adults and carotid artery intima–media thickness: The Cardiovascular Risk in Young Finns study. Atherosclerosis 2009, 205, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.L. Cardiovascular risk in minority and underserved women in Appalachian Tennessee: A descriptive study. J. Am. Acad. Nurse Pract. 2010, 22, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Varleta, P.; Concepción, R.; Vargas, P.; Casanova, H. Grosor íntima media carotídeo y asociación con factores de riesgo cardiovascular tradicionales y metabólicos. Ver. Med. Chile 2013, 141, 695–703. [Google Scholar] [CrossRef][Green Version]
- Alkali, N.; Bwala, S.; Akano, A.; Osi-Ogbu, O.; Alabi, P.; Ayeni, O. Stroke risk factors, subtypes, and 30 day case fatality in Abuja, Nigeria. Niger. Med. J. 2013, 54, 129–136. [Google Scholar] [CrossRef]
- Rodríguez-Saldaña, J.; Rodriguez-Flores, M.; Cantú-Brito, C.; Aguirre-Garcia, J. A Pathological Study of the Epidemiology of Atherosclerosis in Mexico City. Cardiol. Res. Pr. 2014, 2014, 2642058. [Google Scholar] [CrossRef]
- Maddaloni, E.; Cavallari, I.; De Pascalis, M.; Keenan, H.; Park, K.; Manfrini, S.; Buzzetti, R.; Patti, G.; Di Sciascio, G.; Pozzilli, P. Relation of Body Circumferences to Cardiometabolic Disease in Overweight-Obese Subjects. Am. J. Cardiol. 2016, 118, 822–827. [Google Scholar] [CrossRef]
- Masson, W.; Siniawski, D.; Toledo, G.; Vita, T.; Fernández, G.; Castillo, S.G.; Valle, J.; Cagide, A. Estimación de la «edad vascular» basada en el índice de masa corporal en una población en prevención primaria. Asociación con la aterosclerosis carotídea subclínica. Med. Clínica 2013, 140, 255–259. [Google Scholar] [CrossRef]
- Serena, J.; Segura, T.; Roquer, J.; García-Gil, M.; Castillo, J. The ARTICO study: Identification of patients at high risk of vascular recurrence after a first non-cardioembolic stroke. BMC Neurol. 2015, 15, 1–7. [Google Scholar] [CrossRef]
- Manchev, I.C.; Mineva, P.P.; Hadjiev, D.I. Prevalence of Stroke Risk Factors and Their Outcomes: A Population-Based Longitudinal Epidemiological Study. Cerebrovasc. Dis. 2001, 12, 303–307. [Google Scholar] [CrossRef]
- Kahraman, S.; Yilmaz, R.; Akinci, D.; Arici, M.; Altun, B.; Erdem, Y.; Yasavul, U.; Turgan, C. U-Shaped Association of Body Mass Index with Inflammation and Atherosclerosis in Hemodialysis Patients. J. Ren. Nutr. 2005, 15, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Matsuhisa, M.; Fujiki, N.; Sakamoto, F.; Tsuji, M.; Fujisawa, N.; Kimura, M.; Ishibashi, R.; Kaneto, H.; Yamasaki, Y.; et al. Is Central Obesity a Good Predictor of Carotid Atherosclerosis in Japanese Type 2 Diabetes with Metabolic Syndrome? Endocrime J. 2007, 54, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Lajunen, T.; Vikatmaa, P.; Bloigu, A.; Ikonen, T.; Lepäntalo, M.; Pussinen, P.J.; Saikku, P.; Leinonen, M. Chlamydial LPS and high-sensitivity CRP levels in serum are associated with an elevated body mass index in patients with cardiovascular disease. Innate Immun. 2008, 14, 375–382. [Google Scholar] [CrossRef] [PubMed]
- De Michele, M.; Panico, S.; Iannuzzi, A.; Celentano, E.; Ciardullo, A.V.; Galasso, R.; Sacchetti, L.; Zarrilli, F.; Bond, M.G.; Rubba, P. Association of Obesity and Central Fat Distribution with Carotid Artery Wall Thickening in Middle-Aged Women. Stroke 2002, 33, 2923–2928. [Google Scholar] [CrossRef]
- Lind, L.; Siegbahn, A.; Ingelsson, E.; Sundstrom, J.; Arnlov, J. A Detailed Cardiovascular Characterization of Obesity Without the Metabolic Syndrome. Arter. Thromb. Vasc. Biol. 2011, 31, e27–e34. [Google Scholar] [CrossRef]
- Jackson, R.; Sidawy, A.; Amdur, R.; Macsata, R. Obesity is an Independent Risk Factor for Death and Cardiac Complications after Carotid Endarterectomy. J. Am. Coll Surg. 2012, 214, 148–155. [Google Scholar] [CrossRef]
- Abreu, T.; Ferreira, E.; Filho, S.; Sales, K.; Lopes, F.; Oliveira, A. Prevalence of carotid artery calcifications detected on panoramic radiographs and confirmed by Doppler ultrasonography: Their relationship with systemic conditions. Indian J. Dent. Res. 2015, 26, 345–350. [Google Scholar] [CrossRef]
- Yamauchi, T.; Kuno, T.; Takada, H.; Nagura, Y.; Kanmatsuse, K.; Takahashi, S. The impact of visceral fat on multiple risk factors and carotid atherosclerosis in chronic haemodialysis patients. Nephrol. Dial. Transpl. 2003, 18, 1842–1847. [Google Scholar] [CrossRef]
- Hwang, I.; Suh, S.; Seo, A.; Ahn, H.; Yim, E. Association between Metabolic Components and Subclinical Atherosclerosis in Korean Adults. Korean J. Fam. Med. 2012, 33, 229–236. [Google Scholar] [CrossRef]
- Novo, S.; Peritore, A.; Trovato, R.L.; Guarneri, F.P.; Di Lisi, D.; Muratori, I.; Novo, G. Preclinical atherosclerosis and metabolic syndrome increase cardio- and cerebrovascular events rate: A 20-year follow up. Cardiovasc. Diabetol. 2013, 12, 155. [Google Scholar] [CrossRef]
- Wang, X.; Li, W.; Song, F.; Wang, L.; Fu, Q.; Cao, S.; Gan, Y.; Zhang, W.; Yue, W.; Yan, F.; et al. Carotid Atherosclerosis Detected by Ultrasonography: A National Cross-Sectional Study. J. Am. Heart Assoc. 2018, 7, e00870. [Google Scholar] [CrossRef] [PubMed]
- Sforza, E.; Boissier, C.; Martin, M.S.; Feasson, S.; Barthélémy, J.C.; Roche, F. Carotid artery atherosclerosis and sleep disordered breathing in healthy elderly subjects: The Synapse cohort. Sleep Med. 2013, 14, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Egusa, G.; Hara, H.; Yamakido, M. Association of intraabdominal fat and carotid atherosclerosis in non-obese middle-aged men with normal glucose tolerance. Int. J. Obes. 1997, 21, 948–951. [Google Scholar] [CrossRef] [PubMed]
- Nejmanze, P. Differential Effects of Body Adiposity and Serum Lipids on Right and Left Carotid Artery Lesions. Stroke 2003, 34, e185–e186. [Google Scholar]
- Node, K.; Inoue, T.; Boyko, V.; Goldberg, I.; Fisman, E.Z.; Adler, Y.; Schwammenthal, E.; Matas, Z.; Behar, S.; Tenenbaum, A. Long-term effects of peroxisome proliferator-activated receptor ligand bezafibrate on N-terminal pro-B type natriuretic peptide in patients with advanced functional capacity impairment. Cardiovasc. Diabetol. 2009, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, A.; Altman, L. Carotid artery atheromas in postmenopausal womem–Their prevalence on panoramic radiographs and their relationship to atherogenic risk factors. Am. Dent. Assoc. 2001, 132, 1130–1136. [Google Scholar] [CrossRef]
- Wang, H.; Chen, Y.; Eitzman, D. Imaging Body Fat–Techniques and Cardiometabolic Implications. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2217–2223. [Google Scholar] [CrossRef]
- See, R.; Abdullah, S.M.; McGuire, D.K.; Khera, A.; Patel, M.J.; Lindsey, J.B.; Grundy, S.M.; de Lemos, J.A. The Association of Differing Measures of Overweight and Obesity with Prevalent Atherosclerosis-The Dallas Heart Study. J. Am. Coll. Cardiol. 2007, 50, 752–759. [Google Scholar] [CrossRef]
- Shuster, A.; Patlas, M.; Pinthus, J.; Mourtzakis, M. The clinical importance of visceral adiposity: A critical review of methods for visceral adipose tissue analysis. Br. J. Radiol. 2012, 85, 1–10. [Google Scholar] [CrossRef]
- Há, E.; Bauer, R. Emerging Roles for Adipose Tissue in Cardiovascular Disease. Arter. Thromb. Vasc. Biol. 2018, 38, e137–e144. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, Y.; Lu, C.; Zeng, C.; Chang, D.; Ju, S. Correlations between the abdominal fat related parameters and severity of coronary artery disease assessed by computed tomography. Quant. Imaging Med. Surg. 2018, 8, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.L.; Takx, R.A.; MacNabb, M.H.; Abdelbaky, A.; Lavender, Z.R.; Kaplan, R.S.; Truong, Q.A.; Lo, J.; Ghoshhajra, B.B.; Grinspoon, S.K.; et al. Relationship between measures of adiposity, arterial inflammation, and subsequent cardiovascular events. Circ. Cardiovasc. Imaging 2016, 9, e004043. [Google Scholar] [CrossRef] [PubMed]
- Imai, A.; Komatsu, S.; Ohara, T.; Kamata, T.; Yoshida, J.; Miyaji, K.; Takewa, M.; Kodama, K. Visceral abdominal fat accumulation predicts the progression of noncalcified coronary plaque. Atherosclerosis 2012, 222, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.; Libby, P.; Tabas, I. Inflammation and plaque vulnerability. J. Intern. Med. 2015, 278, 483–493. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).