
Heart Failure—Do We Need New Drugs or Have Them Already? A Case of Coenzyme Q10



Abstract
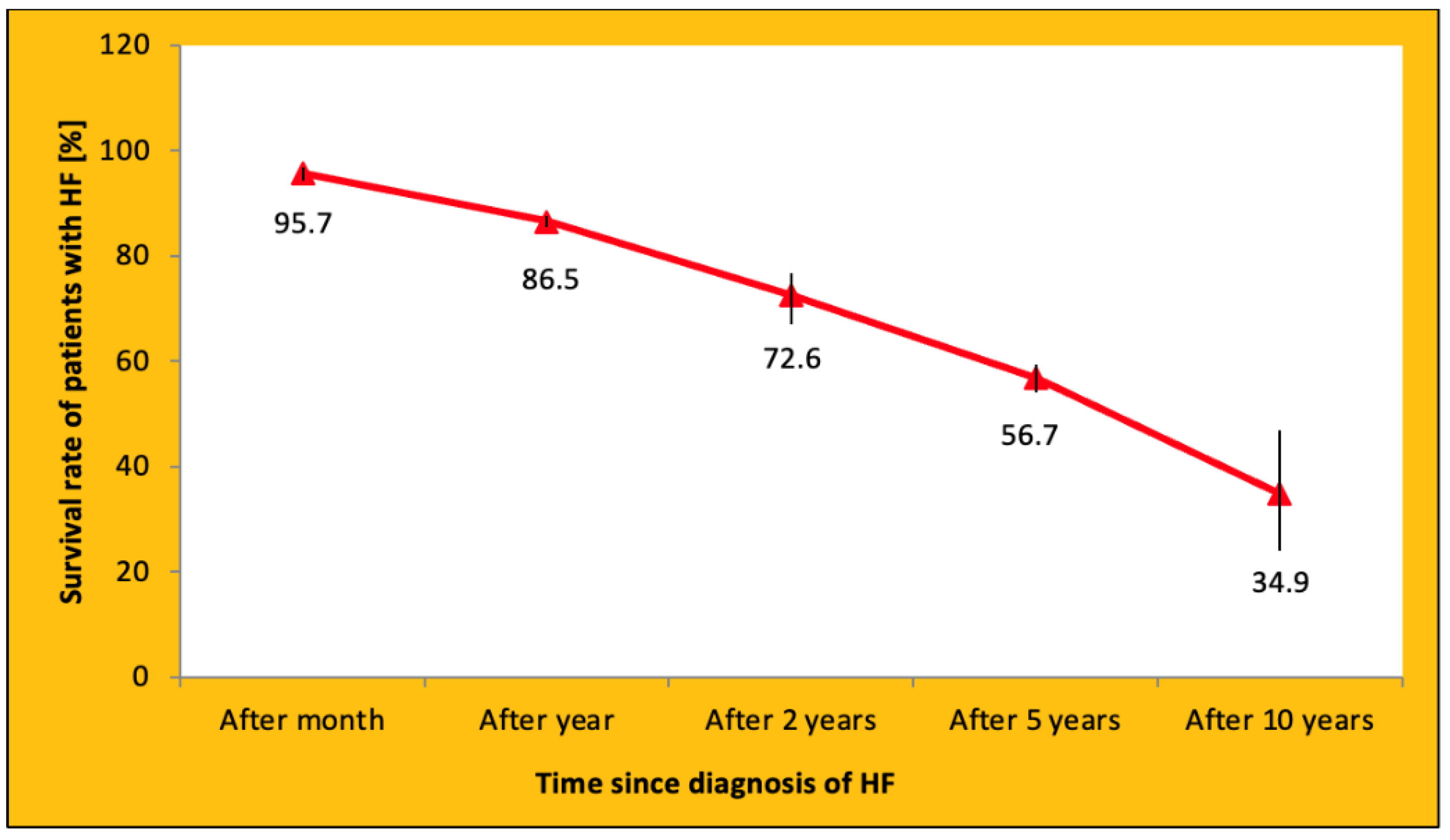
1. Heart Failure—A Civilization Disease
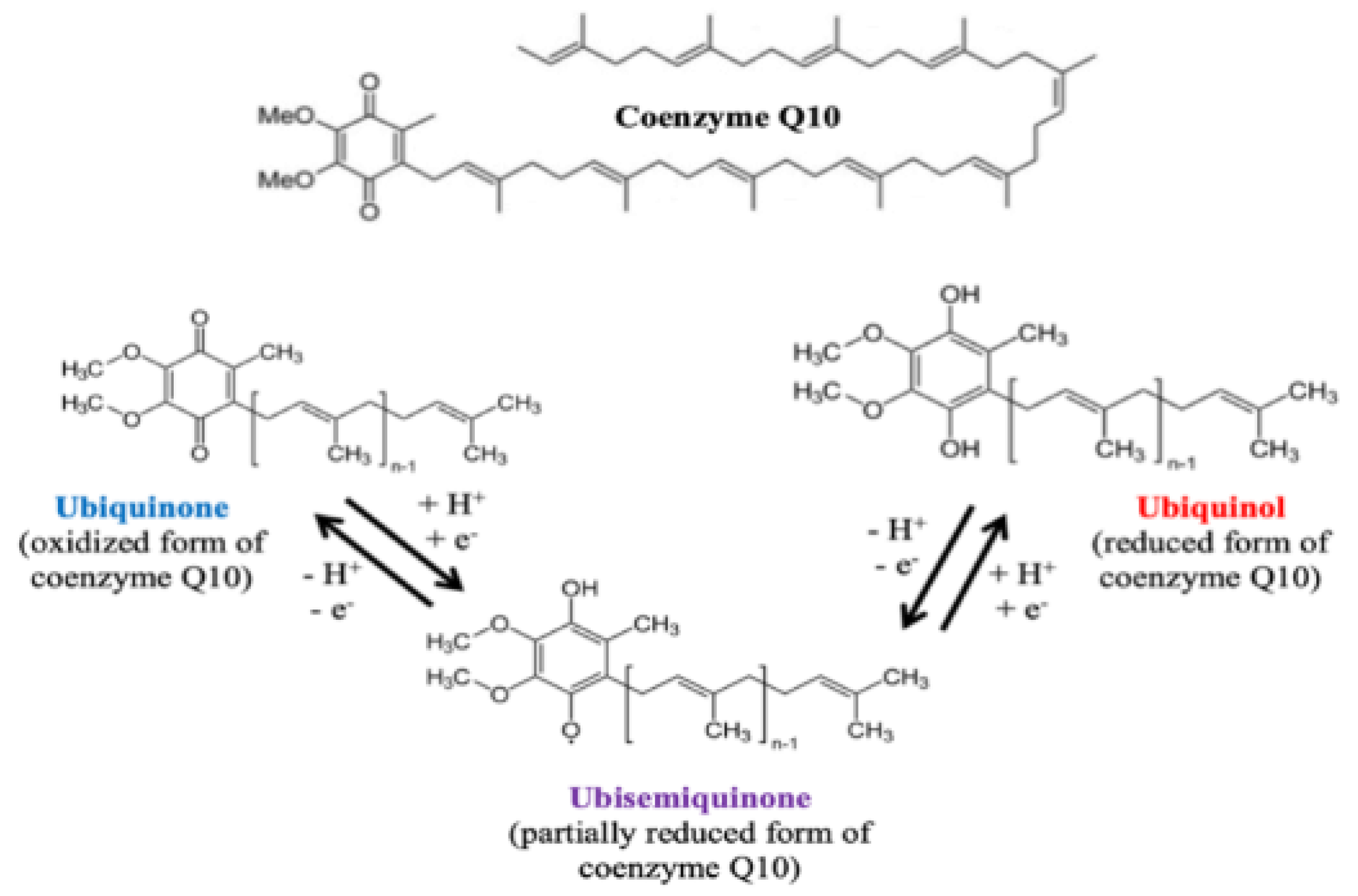
2. Coenzyme Q10—Brief Biochemical Overview
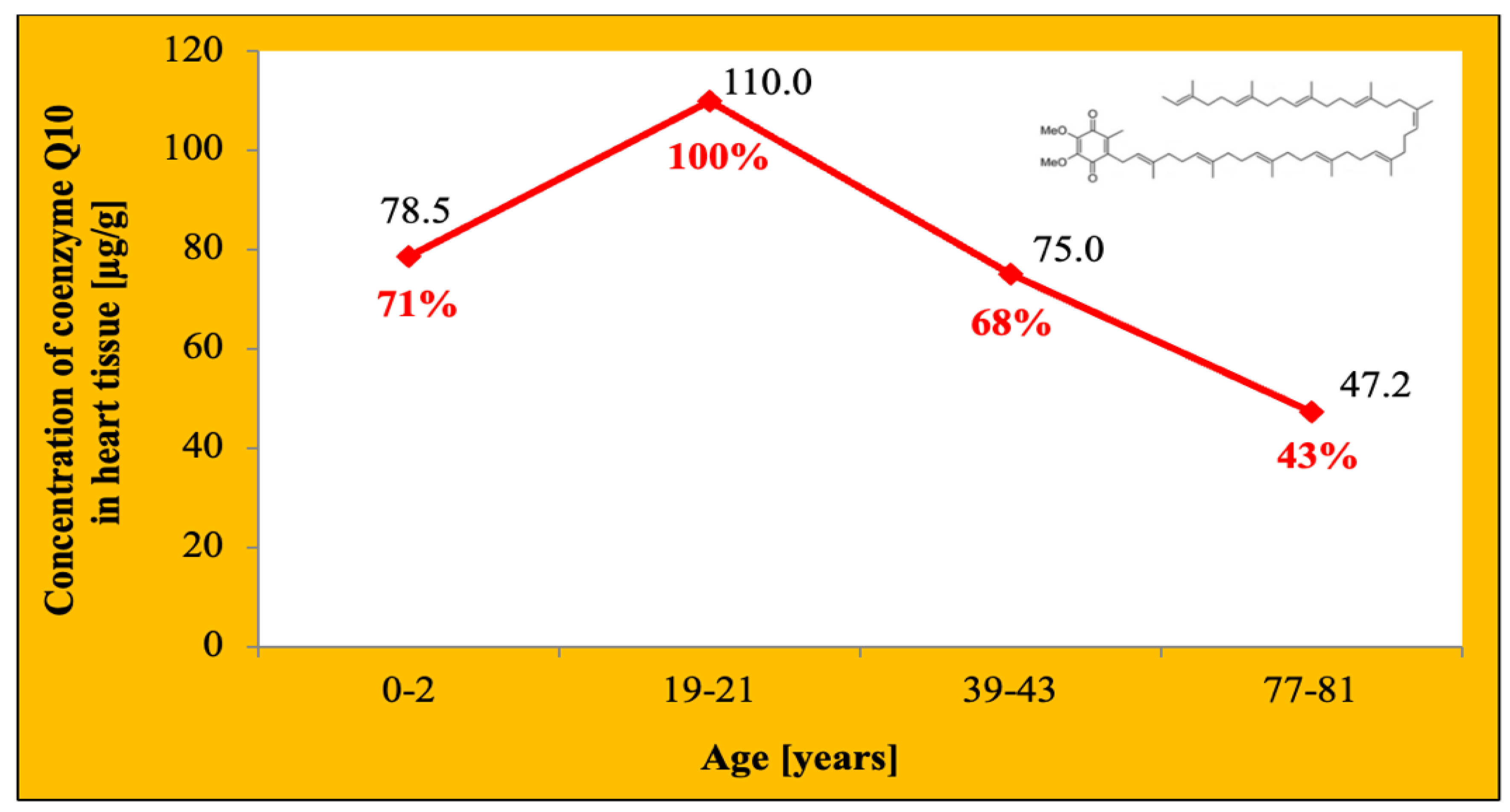
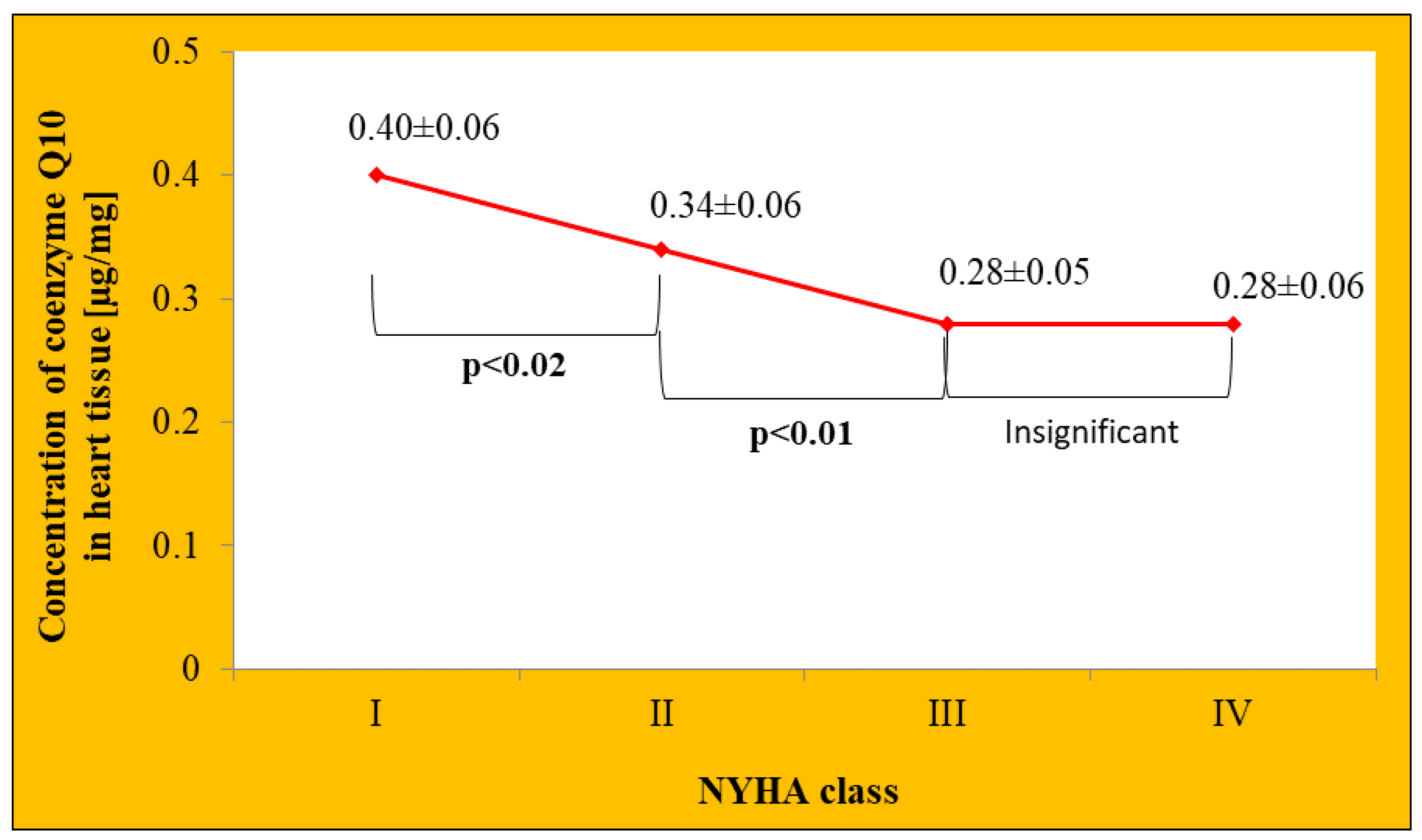
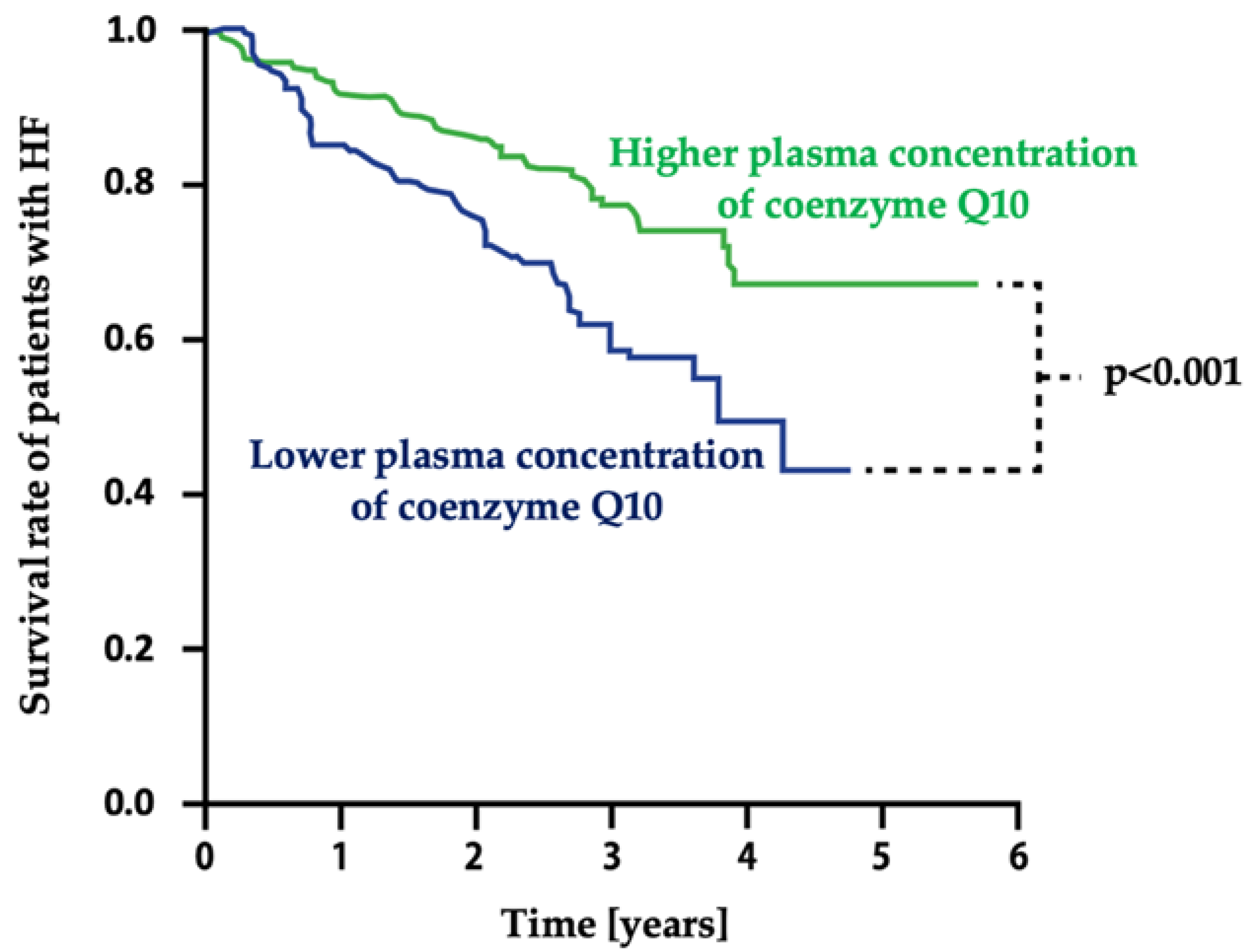
3. Coenzyme Q10 Level in Heart Failure
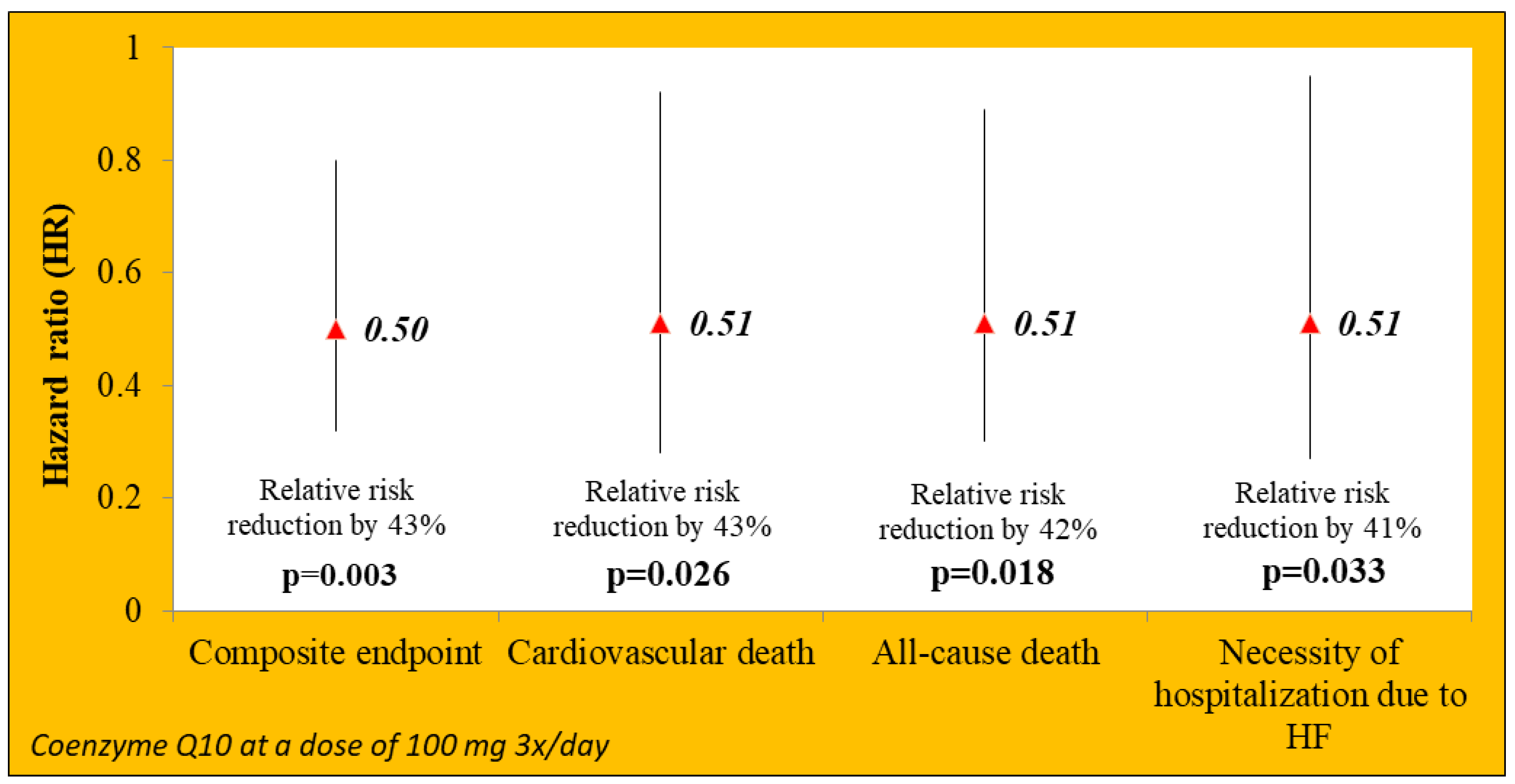
4. Coenzyme Q10 Supplementation in HF—Evidence from Clinical Studies
5. Relationship between Statins and Coenzyme Q10
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2022, cvac013. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Zhong, W.; Shu, J.; Abu Mach, A.; Lotan, D.; Grupper, A.; Younis, A. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur. J. Prev. Cardiol. 2021, 28, 1682–1690. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Sanchis-Gomar, F. Global epidemiology and future trends of heart failure. AME Med. J. 2020, 5, 15. [Google Scholar] [CrossRef]
- Yang, H.; Negishi, K.; Otahal, P.; Marwick, T.H. Clinical prediction of incident heart failure risk: A systematic review and meta-analysis. Open Heart 2015, 2, e000222. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 1 April 2022).
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Timmis, A.; Vardas, P.; Townsend, N.; Torbica, A.; Katus, H.; De Smedt, D.; Gale, C.P.; Maggioni, A.P.; Petersen, S.E.; Huculeci, R.; et al. European Society of Cardiology: Cardiovascular disease statistics 2021. Eur. Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef]
- Jones, N.R.; Roalfe, K.A.; Adoki, I.; Hobbs, F.D.R.; Taylor, C.J. Survival of patients with chronic heart failure in the community: A systematic review and meta-analysis. Eur. J. Heart Fail. 2019, 21, 1306–1325. [Google Scholar] [CrossRef]
- Rabanal-Ruiz, Y.; Llanos-González, E.; Alcain, F.J. The use of coenzyme Q10 in cardiovascular diseases. Antioxidants 2021, 10, 755. [Google Scholar] [CrossRef]
- Surma, S.; Filipiak, K.J. Underestimated therapies: Coenzyme Q10 in heart failure. Terapia 2021, 9, 80–87, (In Polish, only abstract in English). [Google Scholar]
- Stefely, J.A.; Pagliarini, D.J. Biochemistry of mitochondrial coenzyme Q biosynthesis. Trends Biochem. Sci. 2017, 42, 824–843. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Mariscal, F.M.; de la Cruz-Ares, S.; Torres-Peña, J.D.; Alcalá-Diaz, J.F.; Yubero-Serrano, E.M.; López-Miranda, J. Coenzyme Q(10) and cardiovascular diseases. Antioxidants 2021, 10, 906. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Mariscal, F.M.; Arenas-de Larriva, A.P.; Limia-Perez, L.; Romero-Cabrera, J.L.; Yubero-Serrano, E.M.; López-Miranda, J. Coenzyme Q10 supplementation for the reduction of oxidative stress: Clinical implications in the treatment of chronic diseases. Int. J. Mol. Sci. 2020, 21, 7870. [Google Scholar] [CrossRef] [PubMed]
- Martelli, A.; Testai, L.; Colletti, A.; Cicero, A.F.G. Coenzyme Q 10: Clinical applications in cardiovascular diseases. Antioxidants 2020, 9, 341. [Google Scholar] [CrossRef]
- Hidalgo-Gutiérrez, A.; González-García, P.; Díaz-Casado, M.E.; Barriocanal-Casado, E.; López-Herrador, S.; Quinzii, C.M.; López, L.C. Metabolic targets of coenzyme Q10 in mitochondria. Antioxidants 2021, 10, 520. [Google Scholar] [CrossRef]
- Testai, L.; Martelli, A.; Flori, L.; Cicero, A.F.; Colletti, A. Coenzyme Q 10: Clinical applications beyond cardiovascular diseases. Nutrients 2021, 13, 1697. [Google Scholar] [CrossRef]
- Di Lorenzo, A.; Iannuzzo, G.; Parlato, A.; Cuomo, G.; Testa, C.; Coppola, M.; D′Ambrosio, G.; Oliviero, D.A.; Sarullo, S.; Vitale, G.; et al. Clinical evidence for Q10 coenzyme supplementation in heart failure: From energetics to functional improvement. J. Clin. Med. 2020, 9, 1266. [Google Scholar] [CrossRef]
- Garrido-Maraver, J.; Cordero, M.D.; Oropesa-Avila, M.; Vega, A.F.; de la Mata, M.; Pavon, A.D.; Alcocer-Gomez, E.; Calero, C.P.; Paz, M.V.; Alanis, M.; et al. Clinical applications of coenzyme Q10. Front. Biosci. (Landmark Ed.) 2014, 19, 619–633. [Google Scholar] [CrossRef]
- Zozina, V.I.; Covantev, S.; Goroshko, O.A.; Krasnykh, L.M.; Kukes, V.G. Coenzyme Q10 in cardiovascular and metabolic diseases: Current state of the problem. Curr. Cardiol. Rev. 2018, 14, 164–174. [Google Scholar] [CrossRef]
- Saini, R. Coenzyme Q10: The essential nutrient. J. Pharm. Bioallied Sci. 2011, 3, 466–467. [Google Scholar] [CrossRef]
- Rodick, T.C.; Seibels, D.R.; Babu, J.R.; Higgins, K.W.; Ren, G.; Mathews, S.T. Potential role of coenzyme Q10in health and disease conditions. Nutr. Diet. Suppl. 2018, 10, 1–11. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Karwi, Q.G.; Tian, R.; Wende, A.R.; Abel, E.D. Cardiac energy metabolism in heart failure. Circ. Res. 2021, 128, 1487–1513. [Google Scholar] [CrossRef] [PubMed]
- Kalén, A.; Appelkvist, E.L.; Dallner, G. Age-related changes in the lipid compositions of rat and human tissues. Lipids 1989, 24, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Onur, S.; Niklowitz, P.; Jacobs, G.; Lieb, W.; Menke, T.; Döring, F. Association between serum level of ubiquinol and NT-proBNP, a marker for chronic heart failure, in healthy elderly subjects. Biofactors 2015, 41, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Folkers, K.; Vadhanavikit, S.; Mortensen, S.A. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10. Proc. Natl. Acad. Sci. USA 1985, 82, 901–904. [Google Scholar] [CrossRef]
- Molyneux, S.L.; Florkowski, C.M.; George, P.M.; Pilbrow, A.P.; Frampton, C.M.; Lever, M.; Richards, A.M. Coenzyme Q10: An independent predictor of mortality in chronic heart failure. J. Am. Coll. Cardiol. 2008, 52, 1435–1441. [Google Scholar] [CrossRef]
- McMurray, J.J.; Dunselman, P.; Wedel, H.; Cleland, J.G.F.; Lindberg, M.; Hjalmarson, Å.; Kjekshus, J.; Waagstein, F.; Apetrei, E.; Barrios, V.; et al. Coenzyme Q10, Rosuvastatin, and Clinical Outcomes in Heart Failure. J. Am. Coll. Cardiol. 2010, 56, 1196–1204. [Google Scholar] [CrossRef]
- Awad, K.; Sayed, A.; Banach, M. Coenzyme Q 10 reduces infarct size in animal models of myocardial ischemia-reperfusion injury: A meta-analysis and summary of underlying mechanisms. Front. Cardiovasc. Med. 2022, 9, 857364. [Google Scholar] [CrossRef]
- Alehagen, U.; Aaseth, J.; Alexander, J.; Johansson, P. Still reduced cardiovascular mortality 12 years after supplementation with selenium and coenzyme Q10 for four years: A validation of previous 10-year follow-up results of a prospective randomized double-blind placebo-controlled trial in elderly. PLoS ONE 2018, 13, e0193120. [Google Scholar] [CrossRef]
- Xia, L.; Nordman, T.; Olsson, J.M.; Damdimopoulos, A.; Bjorkhem-Bergman, L.; Nalvarte, I.; Erikson, L.C.; Arnér, E.S.J.; Spyrou, J.; Bjornstedt, M.; et al. The mammalian cytosolic selenoenzyme thioredoxin reductase reduces ubiquinone. A novel mechanism for defense against oxidative stress. J. Biol. Chem. 2003, 278, 2141–2146. [Google Scholar] [CrossRef]
- De la Bella-Garzón, R.; Fernández-Portero, C.; Alarcón, D.; Amián, J.G.; López-Lluch, G. Levels of plasma coenzyme Q10 are associated with physical capacity and cardiovascular risk in the elderly. Antioxidants 2022, 11, 279. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Lin, Y.C.; Huang, Y.C.; Ko, Y.W.; Hsia, S.; Lin, P.T. The relationship between coenzyme Q10, oxidative stress, and antioxidant enzymes activities and coronary artery disease. Sci. World J. 2012, 2012, 792756. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Mao, Q.; Cao, J.; Wang, Y.; Zhou, X.; Fan, L. Effects of coenzyme Q10 on vascular endothelial function in humans: A meta-analysis of randomized controlled trials. Atherosclerosis 2012, 221, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, R.; Akbari, M.; Sharifi, N.; Lankarani, K.B.; Moosazadeh, M.; Kolahdooz, F.; Taghizadeh, M.; Asemi, Z. The effects of coenzyme Q10 supplementation on blood pressures among patients with metabolic diseases: A systematic review and meta-analysis of randomized controlled trials. High Blood Press Cardiovas. Prev. 2018, 25, 41–50. [Google Scholar] [CrossRef]
- Sharifi, N.; Tabrizi, R.; Moosazadeh, M.; Mirhosseini, N.; Lankarani, K.B.; Akbari, M.; Chamani, M.; Kolahdooz, F.; Asemi, Z. The effects of coenzyme Q10 supplementation on lipid profiles among patients with metabolic diseases: A systematic review and meta-analysis of randomized controlled trials. Curr. Pharm. Des. 2018, 24, 2729–2742. [Google Scholar] [CrossRef]
- Jorat, M.V.; Tabrizi, R.; Mirhosseini, N.; Lankarani, K.B.; Akbari, M.; Heydari, S.T.; Mottaghi, R.; Asemi, Z. The effects of coenzyme Q10 supplementation on lipid profiles among patients with coronary artery disease: A systematic review and meta-analysis of randomized controlled trials. Lipids Health Dis. 2018, 17, 230. [Google Scholar] [CrossRef]
- Akbari, A.; Mobini, G.R.; Agah, S.; Morvaridzadeh, M.; Omidi, A.; Potter, E.; Fazelian, S.; Ardehali, S.H.; Daneshzad, E.; Dehghani, S. Coenzyme Q10 supplementation and oxidative stress parameters: A systematic review and meta-analysis of clinical trials. Eur. J. Clin. Pharmacol. 2020, 76, 1483–1499. [Google Scholar] [CrossRef]
- Dludla, P.V.; Orlando, P.; Silvestri, S.; Marcheggiani, F.; Cirilli, I.; Nyambuya, T.M.; Mxinwa, V.; Mokgalaboni, K.; Nkambule, B.B.; Johnson, R.; et al. Coenzyme Q10 supplementation improves adipokine levels and alleviates inflammation and lipid peroxidation in conditions of metabolic syndrome: A meta-analysis of randomized controlled trials. Int. J. Mol. Sci. 2020, 21, 3247. [Google Scholar] [CrossRef]
- Zhai, J.; Bo, Y.; Lu, Y.; Liu, C.; Zhang, L. Effects of coenzyme Q10 on markers of inflammation: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0170172. [Google Scholar] [CrossRef]
- Fan, L.; Feng, Y.; Chen, G.C.; Qin, L.Q.; Fu, C.L.; Chen, L.H. Effects of coenzyme Q10 supplementation on inflammatory markers: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2017, 119, 128–136. [Google Scholar] [CrossRef]
- Hargreaves, I.P.; Mantle, D. Coenzyme Q10 supplementation in fibrosis and aging. Adv. Exp. Med. Biol. 2019, 1178, 103–112. [Google Scholar] [PubMed]
- Liu, T.; Song, D.; Dong, J.; Zhu, P.; Liu, J.; Liu, W.; Ma, X.; Zhao, L.; Ling, S. Current understanding of the pathophysiology of myocardial fibrosis and its quantitative assessment in heart failure. Front. Physiol. 2017, 8, 238. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; McCarty, M.F.; O′Keefe, J.H. Coenzyme Q10 deficiency can be expected to compromise Sirt1 activity. Open Heart 2022, 9, e001927. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.M.; Tsai, J.Y.; Chen, Y.C.; Huang, C.Y.; Hsu, H.L.; Weng, C.F.; Shih, C.C.; Hsu, C.P. Downregulation of Sirt1 as aging change in advanced heart failure. J. Biomed. Sci. 2014, 21, 57. [Google Scholar] [CrossRef] [PubMed]
- Hashiba, K.; Kuramoto, K.; Ishimi, Z.; et al. Coenzyme-Q10. Heart (Japanese) 1972, 4, 1579–1589. [Google Scholar]
- Langsjoen, P.H.; Vadhanavikit, S.; Folkers, K. Response of patients in classes III and IV of cardiomyopathy to therapy in a blind and crossover trial with coenzyme Q10. Proc. Natl. Acad. Sci. USA 1985, 82, 4240–4244. [Google Scholar] [CrossRef]
- Morisco, C.; Trimarco, B.; Condorelli, M. Effect of coenzyme Q10 therapy in patients with congestive heart failure: A long-term multicenter randomized study. J. Mol. Med. 1993, 71, 134–136. [Google Scholar] [CrossRef]
- Rengo, F.; Abete, P.; Landino, P.; Leosco, D.; Covelluzzi, F.; Vitale, D.; Fedi, V.; Ferrara, N. Role of metabolic therapy in cardiovascular disease. J. Mol. Med. 1993, 71, 124–128. [Google Scholar] [CrossRef]
- Baggio, E.; Gandini, R.; Plancher, A.C.; Passeri, M.; Carmosino, G. Italian multicenter study on the safety and efficacy of coenzyme Q10 as adjunctive therapy in heart failure. CoQ10 Drug Surveillance Investigators. Mol. Asp. Med. 1994, 15, S287–S294. [Google Scholar] [CrossRef]
- Morisco, C.; Nappi, A.; Argenziano, L.; Sarno, D.; Fonatana, D.; Imbriaco, M.; Nicolai, E.; Romano, M.; Rosiello, G.; Cuocolo, A. Noninvasive evaluation of cardiac hemodynamics during exercise in patients with chronic heart failure: Effects of short-term coenzyme Q10 treatment. Mol. Asp. Med. 1994, 15, 155–163. [Google Scholar] [CrossRef]
- Hofman-Bang, C.; Rehnqvist, N.; Swedberg, K.; Wiklund, I.; Åström, H. Coenzyme Q10 as an adjunctive in the treatment of chronic congestive heart failure. J. Card. Fail. 1995, 1, 101–107. [Google Scholar] [CrossRef]
- Watson, P.S.; Scalia, G.M.; Galbraith, A.; Burstow, D.J.; Bett, N.; Aroney, C.N. Lack of effect of coenzyme Q on left ventricular function in patients with congestive heart failure. J. Am. Coll. Cardiol. 1999, 33, 1549–1552. [Google Scholar] [CrossRef]
- Munkholm, H.; Hansen, H.H.T.; Rasmussen, K. Coenzyme Q10 treatment in serious heart failure. BioFactors 1999, 9, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Khatta, M.; Alexander, B.S.; Krichten, C.M.; Fisher, M.L.; Freudenberger, R.; Robinson, S.W.; Gottlieb, S.S. The effect of coenzyme Q10 in patients with congestive heart failure. Ann. Intern. Med. 2000, 132, 636–640. [Google Scholar] [CrossRef]
- Keogh, A.; Fenton, S.; Leslie, C.; Aboyoun, C.; Macdonald, P.; Zhao, Y.C.; Bailey, M.; Rosenfeldt, F. Randomised double-blind, placebo-controlled trial of coenzyme Q, therapy in class II and III systolic heart failure. Heart Lung Circ. 2003, 12, 135–141. [Google Scholar] [CrossRef]
- Sinatra, S.T.; Berman, M. Coenzyme Q10 in patients with end-stage heart failure awaiting cardiac transplantation: A randomized, placebo-controlled study. Clin. Cardiol. 2004, 27, 26–30. [Google Scholar] [CrossRef][Green Version]
- Belardinelli, R.; Lacalaprice, F.; Solenghi, M.; Seddaiu, G.; Principi, F.; Tiano, L.; Littarru, G.P.; Muçaj, A. Coenzyme Q10 and exercise training in chronic heart failure. Eur. Heart J. 2006, 27, 2675–2681. [Google Scholar] [CrossRef]
- Langsjoen, P.H.; Langsjoen, A.M. Supplemental ubiquinol in patients with advanced congestive heart failure. Biofactors 2008, 32, 119–128. [Google Scholar] [CrossRef]
- Fumagalli, S.; Fattirolli, F.; Guarducci, L.; Cellai, T.; Baldasseroni, S.; Tarantini, F.; Di Bari, M.; Masotti, G.; Marchionni, N. Coenzyme Q10 terclatrate and creatine in chronic heart failure: A randomized, placebo-controlled, double-blind study. Clin. Cardiol. 2011, 34, 211–217. [Google Scholar] [CrossRef]
- Turk, S.; Baki, A.; Solak, Y.; Kayrak, M.; Atalay, H.; Gaipov, A.; Aribas, A.; Akilli, H.; Biyik, Z.; Okudan, N.; et al. Coenzyme Q10 supplementation and diastolic heart functions in hemodialysis patients: A randomized double-blind placebo-controlled trial. Hemodial. Int. 2013, 17, 374–381. [Google Scholar] [CrossRef]
- Pourmoghaddas, M.; Rabbani, M.; Shahabi, J.; Garakyaraghi, M.; Khanjani, R.; Hedayat, P. Combination of atorvastatin/coenzyme Q10 as adjunctive treatment in congestive heart failure: A double-blind randomized placebo-controlled clinical trial. ARYA Atheroscler. 2014, 10, 1–5. [Google Scholar] [PubMed]
- Mortensen, S.A.; Rosenfeldt, F.; Kumar, A.; Dolliner, P.; Filipiak, K.J.; Pella, D.; Alehagen, U.; Steurer, G.; Littarru, G.P. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure. JACC Heart Fail. 2014, 2, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Kebbati, A.H.; Zhang, Y.; Tang, Y.; Okello, E.; Huang, C. Effect of coenzyme Q10 on the incidence of atrial fibrillation in patients with heart failure. J. Investig. Med. 2015, 63, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Sobirin, M.A.; Herry, Y.; Sofia, S.N.; Uddin, I.; Rifqi, S.; Tsutsui, H. Effects of coenzyme Q10 supplementation on diastolic function in patients with heart failure with preserved ejection fraction. Drug Discov. Ther. 2019, 13, 38–46. [Google Scholar] [CrossRef]
- Mortensen, A.L.; Rosenfeldt, F.; Filipiak, K.J. Effect of coenzyme Q10 in Europeans with chronic heart failure: A sub-group analysis of the Q-SYMBIO randomized double-blind trial. Cardiol. J. 2019, 26, 147–156. [Google Scholar] [CrossRef]
- Kawashima, C.; Matsuzawa, Y.; Konishi, M.; Akiyama, E.; Suzuki, H.; Sato, R.; Nakahashi, H.; Kikuchi, S.; Kimura, Y.; Maejima, N.; et al. Ubiquinol improves endothelial function in patients with heart failure with reduced ejection fraction: A single-center, randomized double-blind placebo-controlled crossover pilot study. Am. J. Cardiovasc. Drugs 2020, 20, 363–372. [Google Scholar] [CrossRef]
- Samuel, T.Y.; Hasin, T.; Gotsman, I.; Weitzman, T.; Ben Ivgi, F.; Dadon, Z.; Asher, E.; Amir, O.; Glikson, M.; Alcalai, R.; et al. Coenzyme Q10 in the treatment of heart failure with preserved ejection fraction: A prospective, randomized, double-blind, placebo-controlled trial. Drugs R D 2022, 22, 25–33. [Google Scholar] [CrossRef]
- Lei, L.; Liu, Y. Efficacy of coenzyme Q10 in patients with cardiac failure: A meta-analysis of clinical trials. BMC Cardiovasc. Disord. 2017, 17, 196. [Google Scholar] [CrossRef]
- Trongtorsak, A.; Kongnatthasate, K.; Susantitaphong, P.; Kittipibul, V.; Ariyachaipanich, A. Effect of coenzyme Q10 on left ventricular remodeling and mortality in patients with heart failure: A meta-analysis. J. Am. Coll. Cardiol. 2017, 69, 707. [Google Scholar] [CrossRef]
- Claxton, L.; Simmonds, M.; Beresford, L.; Cubbon, R.; Dayer, M.; Gottlieb, S.S.; Hartshorne-Evans, N.; Kilroy, B.; Llewellyn, A.; Rothery, C.; et al. Coenzyme Q10 to manage chronic heart failure with a reduced ejection fraction: A systematic review and economic evaluation. Health Technol. Assess. 2022, 26, 1–128. [Google Scholar] [CrossRef]
- Jafari, M.; Mousavi, S.M.; Asgharzadeh, A.; Yazdani, N. Coenzyme Q10 in the treatment of heart failure: A systematic review of systematic reviews. Indian Heart J. 2018, 70, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Al Saadi, T.; Assaf, Y.; Farwati, M.; Turkmani, K.; Al-Mouakeh, A.; Shebli, B.; Khoja, M.; Essali, A.; Madmani, M.E. Coenzyme Q10 for heart failure. Cochrane Database Syst. Rev. 2021, 2, CD008684. [Google Scholar]
- Filipiak, K.J. Koenzym Q10 w niewydolności serca—W oczekiwaniu na nowe wytyczne dotyczące leczenia niewydolności serca. Kardiol. Pol. 2015, 73, 36–37. [Google Scholar] [CrossRef]
- Mantle, D. Coenzyme Q10 supplementation for the treatment and prevention of heart failure. Br. J. Cardiol. 2015, 22, 68. [Google Scholar]
- Surma, S.; Rakowski, M.; Banach, M. The role of high doses of atorvastatin or rosuvastatin in the treatment of cardiovascular diseases. Świat Med. Farm. 2021, 11/12, 10–21, (In Polish, only abstract in English). [Google Scholar]
- Florkowski, C.M.; Molyneux, S.L.; Young, J.M. Coenzyme Q10 and congestive heart failure; an evolving evidence base. Kardiol. Pol. 2015, 73, 73–79. [Google Scholar] [CrossRef][Green Version]
- Roger, V.L. Epidemiology of heart failure: A contemporary perspective. Circ. Res. 2021, 128, 1421–1434. [Google Scholar] [CrossRef]
- Banach, M.; Serban, C.; Ursoniu, S.; Rysz, J.; Muntner, P.; Toth, P.P.; Jones, S.R.; Rizzo, M.; Glasser, S.P.; Watts, G.F.; et al. Statin therapy and plasma coenzyme Q10 concentrations-A systematic review and meta-analysis of placebo-controlled trials. Pharmacol. Res. 2015, 99, 329–336. [Google Scholar] [CrossRef]
- Qu, H.; Meng, Y.Y.; Chai, H.; Liang, F.; Zhang, J.Y.; Gao, Z.Y.; Shi, D.Z. The effect of statin treatment on circulating coenzyme Q10 concentrations: An updated meta-analysis of randomized controlled trials. Eur. J. Med. Res. 2018, 23, 57. [Google Scholar] [CrossRef]
- Kjekshus, J.; Apetrei, E.; Barrios, V.; Böhm, M.; Cleland, J.G.; Cornel, J.H.; Dunselman, P.; Dunselman, P.; Fonseca, C.; Goudev, A.; et al. Rosuvastatin in older patients with systolic heart failure. N. Engl. J. Med. 2007, 357, 2248–2261. [Google Scholar] [CrossRef]
- Tavazzi, L.; Maggioni, A.P.; Marchioli, R.; Barlera, S.; Franzosi, M.G.; Latini, R.; Lucci, D.; Nicolosi, G.L.; Porcu, M.; Tognoni, G. Effect of n-3 polyunsaturated fatty acids in patients with chronic heart failure (the GISSI-HF trial): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 1223–1230. [Google Scholar] [PubMed]
- Safitri, N.; Alaina, M.F.; Pitaloka, D.A.E.; Abdulah, R. A narrative review of statin-induced rhabdomyolysis: Molecular mechanism, risk factors, and management. Drug Healthc. Patient Saf. 2021, 13, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.; Guo, M.; Chai, H.; Wang, W.T.; Gao, Z.Y.; Shi, D.Z. Effects of coenzyme Q10 on statin-induced myopathy: An updated meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2018, 7, e009835. [Google Scholar] [CrossRef] [PubMed]
- Raizner, A.E.; Quiñones, M.A. Coenzyme Q10 for patients with cardiovascular disease: JACC Focus Seminar. J. Am. Coll. Cardiol. 2021, 77, 609–619. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, 895–1032. [Google Scholar] [CrossRef]
- Atherton, J.J.; Sindone, A.; De Pasquale, C.G.; Driscoll, A.; MacDonald, P.S.; Hopper, I.; Kistler, P.M.; Briffa, T.; Wong, J.; Abhayaratna, W.; et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Guidelines for the Prevention, Detection, and Management of Heart Failure in Australia 2018. Heart Lung Circ. 2018, 27, 1123–1208. [Google Scholar] [CrossRef]
- Mortensen, S.A. Coenzyme Q10—will this natural substance become a guideline-directed adjunctive therapy in heart failure? Letter to the Editor. JACC Heart Fail. 2015, 3, 270. [Google Scholar] [CrossRef]
- Mantle, D.; Dybring, A. Bioavailability of coenzyme Q10: An overview of the absorption process and subsequent metabolism. Antioxidants 2020, 9, 386. [Google Scholar] [CrossRef]
- Cirilli, I.; Damiani, E.; Dludla, P.V.; Hargreaves, I.; Marcheggiani, F.; Millichap, L.E.; Orlando, P.; Silvestri, S.; Tiano, L. Role of ooenzyme Q10 in health and disease: An update on the last 10 years (2010–2020). Antioxidants 2021, 10, 1325. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coenzyme Q10 Function |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Author, Year; Ref. # | Type of Study | Sample Size | Intervention | Key Findings | Effects |
|---|---|---|---|---|---|
| Langsjoen P.H. et al., 1985; [47] | Double-blind and double-crossover trial | 18 patients with HF; NYHA class: III-IV | CQ10 33 mg 3×/day per 3 months | Significant improvement of:
|  |
| Morisco C. et al., 1993; [48] | Double-blind placebo-controlled trial | 641 HFrEF patients NYHA class: III–IV | CQ10 50 mg 2×/day or 3×/day vs. placebo per 1 year |
| |
| Rengo F. et al., 1993; [49] | Single-blind placebo randomized trial | 60 HFrEF patients NYHA class: III | CQ10 100 mg/day vs. placebo per 7 months |
| |
| Baggio E. et al., 1994; [50] | Multicenter, open, non-comparative trial | 2664 HF patients NYHA class: II and III | CQ10 50–150 mg/day per 3 months | Significant improvement in:
| |
| Morisco C. et al., 1994; [51] | Double-blind RCT | 6 patients with chronic HF NYHA class: II-IV | CQ10 50 mg 3×/day or placebo per 4 weeks |
| |
| Hofman-Bang C. et al., 1995; [52] | Double-blind, crossover placebo-controlled trial | 79 patients with stable HFrEF | CQ10 50 mg 3×/day vs. placebo per 3 months | Significant improvement in:
| |
| Watson P.S. et al., 1998; [53] | Double-blind, crossover placebo-controlled trial | 30 patients with HFrEF | CQ10 33 mg 3×/day vs. placebo per 3 months | No significantly difference in:
|  |
| Munkholm H. et al., 1999; [54] | Double-blind placebo-controlled randomized trial | 22 patients with HF NYHA class: II and III | CQ10 100 mg 2×/day vs. placebo per 1 year | Improvement of:
| |
| Khatta M. et al., 2000; [55] | Double-blind RCT | 55 patients with HFrEF NYHA class: III and IV | CQ10 200 mg/day vs. placebo per 6 months | No significantly difference in:
| |
| Keogh A. et al., 2003; [56] | Double-blind RCT | 39 patients with HFrEF NYHA class: II and III | CQ10 50 mg 3×/day vs. placebo per 3 months |
| |
| Sinatra S.T. et al., 2004; [57] | RCT | 32 patients with HFrEF awaiting HTx | CQ10 60 mg 2×/day vs. placebo per 3 months |
| |
| Belardinelli R. et al., 2006; [58] | Double-blind, placebo-controlled crossover trial | 23 patients with HF NYHA class: II and III | CQ10 100 mg 4×/day vs. placebo per 4 weeks | Significantly improvement of:
| |
| Langsjoen P.H. and Langsjoen A.M.; 2008; [59] | 7 patients with HF NYHA class: IV | Average of 580 mg/day of ubiquinol (450–900 mg/day) | Mean EF improved from 22% (10–35%) up to 39% (10–60%) and clinical improvement has been remarkable with NYHA class improving from a mean of IV to a mean of II (I to III) | | |
| Fumagalli S. et al., 2011; [60] | Double-blind RCT | 67 patients with stable chronic HF | CQ10 320 mg + creatine 340 mg or placebo once daily per 8 weeks | Improved exercise tolerance, by enhancing peak oxygen consumption (p < 0.05) and quality of life | |
| Turk S. et al., 2013; [61] | Prospective double-blind RCT | 22 hemodialysis patients | CQ10 200 mg/day or placebo per 8 weeks | CQ10 supplementation did not significantly improved diastolic heart functions compared with placebo | |
| Pourmoghaddas M. et al., 2014; [62] | Double-blind RCT | 62 patients with HFrEF NYHA class: II–IV | CQ10 100 mg 2×/day with atorvastatin 10 mg/day vs. placebo per 4 months | Improvement of:
| |
| Mortensen S.A. et al., 2014; [63] Q-SYMBIO Study | Double-blind RCT | 420 patients with HFrEF NYHA class: I–II | CQ10 100 mg 3×/d vs. placebo per 2 years |
| |
| Zhao Q. et al., 2015; [64] | Double-blind RCT | 102 patients with HF | CQ10 2 mg/kg/day divided in 2 or 3 doses for 1 year |
| |
| Sobirin M.A. et al., 2019; [65] | Unblinded RCT | 30 patients with HFpEF | CQ10 100 mg 3×/day per 30 days |
| |
| Mortensen A.L. et al., 2019; [66] Q-SYMBIO Study, European sub-population | Double-blind RCT | 420 patients with moderate to severe HF | CQ10 300 mg/day vs. placebo in addition to standard therapy for 2 years |
| |
| Kawashima C. et al., 2020; [67] | Double-blind RCT | 14 patients with stable HFrEF | CQ10 (ubiquinol) 400 mg/day or placebo per 3 months |
| |
| Samuel T.Y. et al., 2022; [68] | Prospective, double-blind RCT | 39 patients with HFpEF NYHA class: II-IV | CQ10 (ubiquinol) 3×/day or placebo per 4 months | No significant effect of treatment on:
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filipiak, K.J.; Surma, S.; Romańczyk, M.; Okopień, B. Heart Failure—Do We Need New Drugs or Have Them Already? A Case of Coenzyme Q10. J. Cardiovasc. Dev. Dis. 2022, 9, 161. https://doi.org/10.3390/jcdd9050161
Filipiak KJ, Surma S, Romańczyk M, Okopień B. Heart Failure—Do We Need New Drugs or Have Them Already? A Case of Coenzyme Q10. Journal of Cardiovascular Development and Disease. 2022; 9(5):161. https://doi.org/10.3390/jcdd9050161
Chicago/Turabian StyleFilipiak, Krzysztof J., Stanisław Surma, Monika Romańczyk, and Bogusław Okopień. 2022. "Heart Failure—Do We Need New Drugs or Have Them Already? A Case of Coenzyme Q10" Journal of Cardiovascular Development and Disease 9, no. 5: 161. https://doi.org/10.3390/jcdd9050161
APA StyleFilipiak, K. J., Surma, S., Romańczyk, M., & Okopień, B. (2022). Heart Failure—Do We Need New Drugs or Have Them Already? A Case of Coenzyme Q10. Journal of Cardiovascular Development and Disease, 9(5), 161. https://doi.org/10.3390/jcdd9050161