

Risk Factors of Secondary Cardiovascular Events in a Multi-Ethnic Asian Population with Acute Myocardial Infarction: A Retrospective Cohort Study from Malaysia
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Malaysian Acute Vascular Events Risk (MAVERIK) Study and the Study Population
2.2. MACE Outcome
2.3. Baseline Characteristics and Exposures
2.4. Statistical Analysis
3. Results
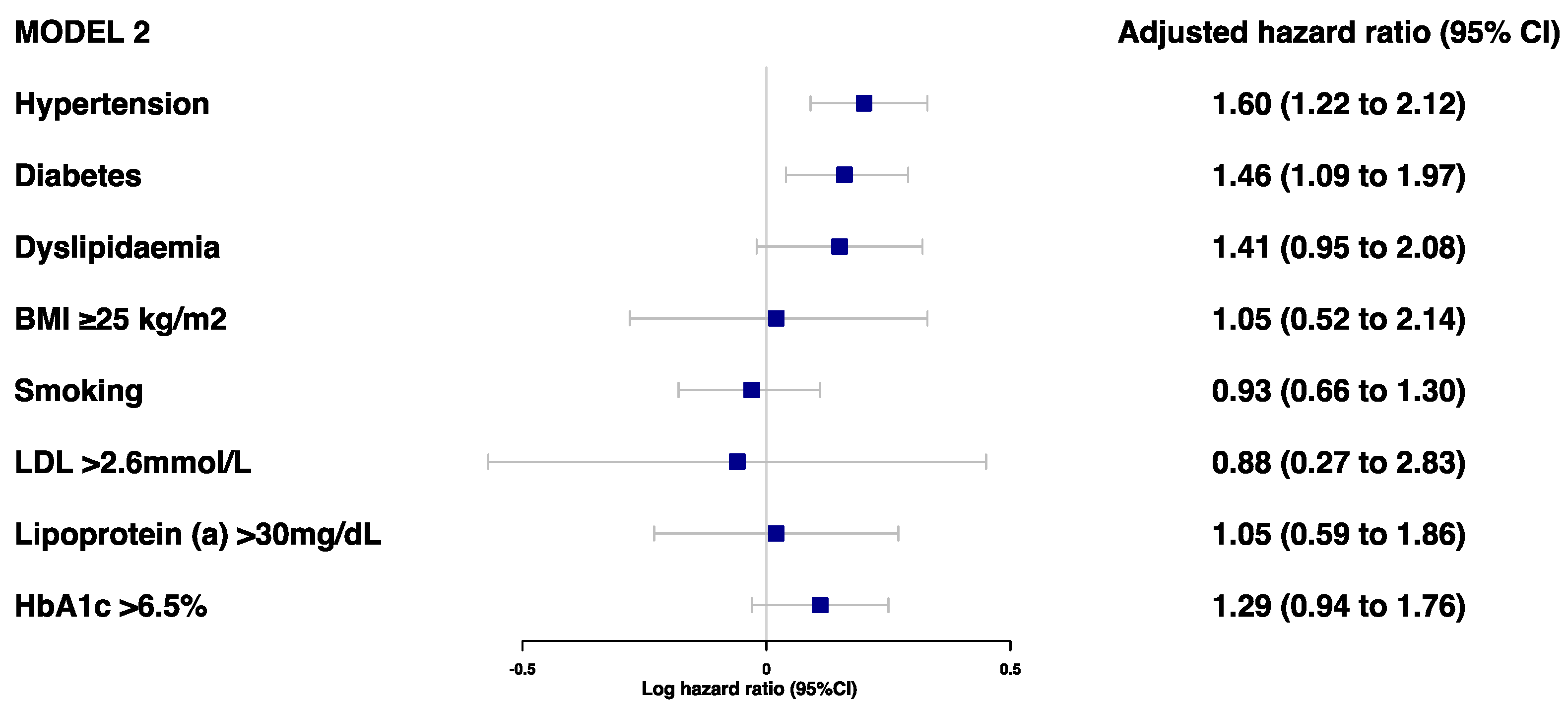
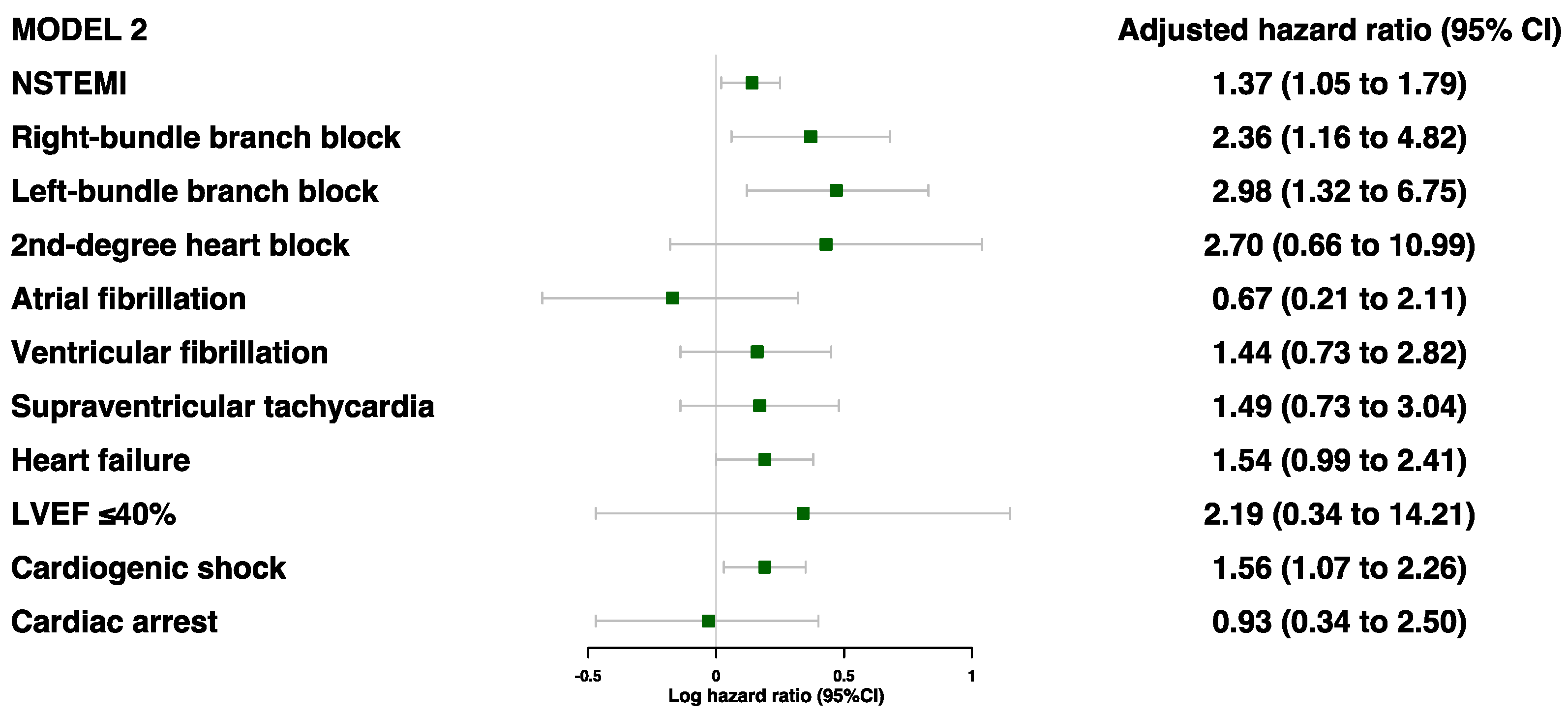
3.1. Risk Factors Associated with MACE
3.2. Risk Factors Associated with MACE by Demographics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peters, S.A.E.; Colantonio, L.D.; Dai, Y.; Zhao, H.; Bittner, V.; Farkouh, M.E.; Dluzniewski, P.; Poudel, B.; Muntner, P.; Woodward, M. Trends in Recurrent Coronary Heart Disease After Myocardial Infarction Among US Women and Men Between 2008 and 2017. Circulation 2021, 143, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Johansson, S.; Rosengren, A.; Young, K.; Jennings, E. Mortality and morbidity trends after the first year in survivors of acute myocardial infarction: A systematic review. BMC Cardiovasc. Disord. 2017, 17, 53. [Google Scholar] [CrossRef] [PubMed]
- Meadows, T.A.; Bhatt, D.L.; Cannon, C.P.; Gersh, B.J.; Röther, J.; Goto, S.; Liau, C.-S.; Wilson, P.W.F.; Salette, G.; Smith, S.C.; et al. Ethnic differences in cardiovascular risks and mortality in atherothrombotic disease: Insights from the Reduction of Atherothrombosis for Continued Health (REACH) registry. Mayo Clin. Proc. 2011, 86, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Gijsberts, C.M.; Seneviratna, A.; de Carvalho, L.P.; den Ruijter, H.M.; Vidanapthirana, P.; Sorokin, V.; Stella, P.; Agostoni, P.; Asselbergs, F.W.; Richards, A.M.; et al. Ethnicity Modifies Associations between Cardiovascular Risk Factors and Disease Severity in Parallel Dutch and Singapore Coronary Cohorts. PLoS ONE 2015, 10, e0132278. [Google Scholar] [CrossRef]
- Vyas, M.V.; Chaturvedi, N.; Hughes, A.D.; Marmot, M.; Tillin, T. Cardiovascular disease recurrence and long-term mortality in a tri-ethnic British cohort. Heart 2021, 107, 996–1002. [Google Scholar] [CrossRef]
- Franey, E.G.; Kritz-Silverstein, D.; Richard, E.L.; Alcaraz, J.E.; Nievergelt, C.M.; Shaffer, R.A.; Bhatnagar, V. Association of Race and Major Adverse Cardiac Events (MACE): The Atherosclerosis Risk in Communities (ARIC) Cohort. J. Aging Res. 2020, 2020, 7417242. [Google Scholar] [CrossRef]
- Federation, I.D. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- Oliva, R.V. A Review on the Status of Hypertension in Six Southeast Asian Countries. Hypertens. J. 2019, 5, 45–48. [Google Scholar] [CrossRef]
- Lam, C.S.P. Heart failure in Southeast Asia: Facts and numbers. ESC Heart Fail. 2015, 2, 46–49. [Google Scholar] [CrossRef]
- Dans, A.; Ng, N.; Varghese, C.; Tai, E.S.; Firestone, R.; Bonita, R. The rise of chronic non-communicable diseases in southeast Asia: Time for action. Lancet 2011, 377, 680–689. [Google Scholar] [CrossRef]
- Li, J.; Dong, Y.; Wu, T.; Tong, N. Differences between Western and Asian type 2 diabetes patients in the incidence of vascular complications and mortality: A systematic review of randomized controlled trials on lowering blood glucose. J. Diabetes 2016, 8, 824–833. [Google Scholar] [CrossRef]
- Chowdhury, R.; Mohd Noh, M.F.; Ismail, S.R.; van Daalen, K.R.; Kamaruddin, P.S.N.M.; Zulkiply, S.H.; Azizul, N.H.; Khalid, N.M.; Ali, A.; Idris, I.M.; et al. The Malaysian Acute Vascular Events Risk (MAVERIK) study: A resource to study genetic and other determinants of first-ever myocardial infarction in Malaysia. J. Med. Internet Res. 2022, 11, e31885. [Google Scholar]
- Ministry of Health Malaysia. Management of Non-St Elevation Myocardial Infarction. In Clinical Practice Guidelines; National Heart Association of Malaysia, 2021; Available online: https://www.malaysianheart.org/files/61447c5be413d.pdf (accessed on 20 April 2023).
- Ministry of Health Malaysia. Management of Acute St Segment Elevation Myocardial Infarction. In Clinical Practise Guidelines; National Heart Association Malaysia, 2019; Available online: https://www.malaysianheart.org/files/5dd785088d471.pdf (accessed on 20 April 2023).
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia. Management of Dyslipidaemia. Clinical Practice Guidelines. 2017. Available online: https://www.moh.gov.my/moh/resources/Penerbitan/CPG/CARDIOVASCULAR/4.pdf (accessed on 20 April 2023).
- Guan, W.; Cao, J.; Steffen, B.T.; Post, W.S.; Stein, J.H.; Tattersall, M.C.; Kaufman, J.D.; McConnell, J.P.; Hoefner, D.M.; Warnick, R.; et al. Race is a key variable in assigning lipoprotein(a) cutoff values for coronary heart disease risk assessment: The Multi-Ethnic Study of Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 996–1001. [Google Scholar] [CrossRef]
- Purnell, J.Q.; Feingold, K.R.; Anawalt, B.; Boyce, A.; Chrousos, G.; de Herder, W.W.; Dhatariya, K.; Dungan, K.; Grossman, A.; Hershman, J.M.; et al. Definitions, Classification, and Epidemiology of Obesity; Endotext; MDText.com, Inc.: Dartmouth, MA, USA, 2018. [Google Scholar]
- Chapman Shah, A.S.V.; Lee, K.K.; Anand, A.; Francis, O.; Adamson, P.; McAllister, D.A.; Strachan, F.E.; Newby, D.E.; Mills, N.L. Long-Term Outcomes in Patients with Type 2 Myocardial Infarction and Myocardial Injury. Circulation 2018, 137, 1236–1245. [Google Scholar] [CrossRef]
- Ahmad, W.; Sim, K. Annual Report of the Ncvd-Acs Registry, 2014–2015; National Cardiovascular Disease Database: Kuala Lumpur, Malaysia, 2017. [Google Scholar]
- Song, J.; Murugiah, K.; Hu, S.; Gao, Y.; Li, X.; Krumholz, H.M.; Zheng, X. Incidence, predictors, and prognostic impact of recurrent acute myocardial infarction in China. Heart 2021, 107, 313–318. [Google Scholar] [CrossRef]
- Smolina, K.; Wright, F.L.; Rayner, M.; Goldacre, M.J. Long-Term Survival and Recurrence After Acute Myocardial Infarction in England, 2004 to 2010. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 532–540. [Google Scholar] [CrossRef]
- Yeo, K.K.; Zheng, H.; Chow, K.Y.; Ahmad, A.; Chan, B.P.L.; Chang, H.M.; Chong, E.; Chua, T.S.J.; Foo, D.C.G.; Low, L.P.; et al. Comparative analysis of recurrent events after presentation with an index myocardial infarction or ischaemic stroke. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 234–242. [Google Scholar] [CrossRef]
- Ang, C.S.; Chan, K.M. A Review of Coronary Artery Disease Research in Malaysia. Med. J. Malays. 2016, 71 (Suppl. 1), 42–57. [Google Scholar]
- Chen, D.Y.; Li, C.Y.; Hsieh, M.J.; Chen, C.C.; Hsieh, I.C.; Chen, T.H.; Chen, S.W.; Wang, C.Y.; Chang, S.H.; Lee, C.H.; et al. Predictors of subsequent myocardial infarction, stroke, and death in stable post-myocardial infarction patients: A nationwide cohort study. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 634–642. [Google Scholar] [CrossRef]
- Nair, R.; Johnson, M.; Kravitz, K.; Huded, C.; Rajeswaran, J.; Anabila, M.; Blackstone, E.; Menon, V.; Lincoff, A.M.; Kapadia, S.; et al. Characteristics and Outcomes of Early Recurrent Myocardial Infarction After Acute Myocardial Infarction. J. Am. Heart Assoc. 2021, 10, e019270. [Google Scholar] [CrossRef]
- Radovanovic, D.; Maurer, L.; Bertel, O.; Witassek, F.; Urban, P.; Stauffer, J.-C.; Pedrazzini, G.; Erne, P. Treatment and outcomes of patients with recurrent myocardial infarction: A prospective observational cohort study. J. Cardiol. 2016, 68, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.M.; Abdallah, M.S.; Huded, C.; Johnson, M.J.; Kravitz, K.; Rajeswaran, J.; Anabila, M.; Blackstone, E.; Lincoff, A.; Menon, V.; et al. Recurrent myocardial infarction after STEMI VS. NSTEMI. J. Am. Coll. Cardiol. 2020, 75, 228. [Google Scholar] [CrossRef]
- Carrick, D.; Haig, C.; Maznyczka, A.M.; Carberry, J.; Mangion, K.; Ahmed, N.; May, V.T.Y.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; et al. Hypertension, Microvascular Pathology, and Prognosis After an Acute Myocardial Infarction. Hypertension 2018, 72, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Higashi, Y.; Kihara, Y.; Noma, K. Endothelial dysfunction and hypertension in aging. Hypertens. Res. 2012, 35, 1039–1047. [Google Scholar] [CrossRef]
- Kemp, C.D.; Conte, J.V. The pathophysiology of heart failure. Cardiovasc. Pathol. 2012, 21, 365–371. [Google Scholar] [CrossRef]
- Dokken, B.B. The Pathophysiology of Cardiovascular Disease and Diabetes: Beyond Blood Pressure and Lipids. Diabetes Spectr. 2008, 21, 160–165. [Google Scholar] [CrossRef]
- Rasoul, S.; Ottervanger, J.P.; Timmer, J.R.; Yokota, S.; de Boer, M.J.; van ’t Hof, A.W. Impact of diabetes on outcome in patients with non-ST-elevation myocardial infarction. Eur. J. Intern. Med. 2011, 22, 89–92. [Google Scholar] [CrossRef]
- Cui, J.; Liu, Y.; Li, Y.; Xu, F.; Liu, Y. Type 2 Diabetes and Myocardial Infarction: Recent Clinical Evidence and Perspective. Front. Cardiovasc. Med. 2021, 8, 644189. [Google Scholar] [CrossRef]
- Dei Cas, A.; Khan, S.S.; Butler, J.; Mentz, R.J.; Bonow, R.O.; Avogaro, A.; Tschoepe, D.; Doehner, W.; Greene, S.J.; Senni, M.; et al. Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail. 2015, 3, 136–145. [Google Scholar] [CrossRef]
- Dal Canto, E.; Ceriello, A.; Rydén, L.; Ferrini, M.; Hansen, T.B.; Schnell, O.; Standl, E.; Beulens, J.W. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur. J. Prev. Cardiol. 2019, 26 (Suppl. 2), 25–32. [Google Scholar] [CrossRef]
- Paneni, F.; Costantino, S.; Cosentino, F. Insulin resistance, diabetes, and cardiovascular risk. Curr. Atheroscler. Rep. 2014, 16, 419. [Google Scholar] [CrossRef]
- Zhang, Y.; Hu, G.; Yuan, Z.; Chen, L. Glycosylated hemoglobin in relationship to cardiovascular outcomes and death in patients with type 2 diabetes: A systematic review and meta-analysis. PLoS ONE 2012, 7, e42551. [Google Scholar] [CrossRef]
- Institute for Public Health. National Health Morbidity Survey 2019. Non-Communicable Diseases: Risk Factors and Other Health Problems; Technical Report; National Institutes of Health (NIH), Ministry of Health Malaysia: Shah Alam, Malaysia, 2019; Volume 1.
- Park, H.W.; Yoon, C.H.; Kang, S.H.; Choi, D.J.; Kim, H.S.; Cho, M.C.; Kim, Y.J.; Chae, S.C.; Yoon, J.H.; Gwon, H.C.; et al. Early- and late-term clinical outcome and their predictors in patients with ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction. Int. J. Cardiol. 2013, 169, 254–261. [Google Scholar] [CrossRef]
- Kong, G.; Chew, N.W.S.; Ng, C.H.; Chin, Y.H.; Lim, O.Z.H.; Ambhore, A.; Ng, G.; Kong, W.; Poh, K.K.; Foo, R.; et al. Prognostic Outcomes in Acute Myocardial Infarction Patients Without Standard Modifiable Risk Factors: A Multiethnic Study of 8,680 Asian Patients. Front. Cardiovasc. Med. 2022, 9, 869168. [Google Scholar] [CrossRef]
- Schmitt, J.; Duray, G.; Gersh, B.J.; Hohnloser, S.H. Atrial fibrillation in acute myocardial infarction: A systematic review of the incidence, clinical features and prognostic implications. Eur. Heart J. 2009, 30, 1038–1045. [Google Scholar] [CrossRef]
- Tan, N.Y.; Witt, C.M.; Oh, J.K.; Cha, Y.-M. Left Bundle Branch Block. Circ. Arrhythmia Electrophysiol. 2020, 13, e008239. [Google Scholar] [CrossRef]
- Macfarlane, P.W. New Ecg Criteria for Acute Myocardial Infarction in Patients with Left Bundle Branch Block. J. Am. Heart Assoc. 2020, 9, e017119. [Google Scholar] [CrossRef]
- Agarwala, A.; Satish, P.; Al Rifai, M.; Mehta, A.; Cainzos-Achirica, M.; Shah, N.S.; Kanaya, A.; Sharma, G.; Dixon, D.; Blumenthal, R.; et al. Identification and Management of Atherosclerotic Cardiovascular Disease Risk in South Asian Populations in the U.S. JACC Adv. 2023, 2, 100258. [Google Scholar] [CrossRef]
- Patel, A.P.; Wang, M.; Kartoun, U.; Ng, K.; Khera, A.V. Quantifying and Understanding the Higher Risk of Atherosclerotic Cardiovascular Disease Among South Asian Individuals: Results from the UK Biobank Prospective Cohort Study. Circulation 2021, 144, 410–422. [Google Scholar] [CrossRef]
- Shah, K.S.; Patel, J.; Al Rifai, M.; Agarwala, A.; Bhatt, A.B.; Levitzky, Y.S.; Palaniappan, L. Cardiovascular Risk Management in the South Asian Patient: A Review. Health Sci. Rev. 2022, 4, 100045. [Google Scholar] [CrossRef]
- Chaudhry, S.I.; Khan, R.F.; Chen, J.; Dharmarajan, K.; Dodson, J.A.; Masoudi, F.A.; Wang, Y.; Krumholz, H.M. National Trends in Recurrent AMI Hospitalizations 1 Year After Acute Myocardial Infarction in Medicare Beneficiaries: 1999–2010. J. Am. Heart Assoc. 2014, 3, e001197. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhai, X.; Xue, M.; Cheng, W.; Hu, H. Prognostic value of lipoprotein (a) level in patients with coronary artery disease: A meta-analysis. Lipids Health Dis. 2019, 18, 150. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.X.; Huang, J.; Li, S.S.; Zhou, L.H.; Yang, M.; Li, Y.; Zhang, A.; Yin, Y.; Zhang, A.; Jia, M.; et al. Elevated lipoprotein(a) and genetic polymorphisms in the LPA gene may predict cardiovascular events. Sci. Rep. 2022, 12, 3588. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Wolski, K.; Cho, L.; Nicholls, S.J.; Kastelein, J.; Leitersdorf, E.; Landmesser, U.; Blaha, M.; Lincoff, M.; Morishita, R.; et al. Lipoprotein(a) levels in a global population with established atherosclerotic cardiovascular disease. Open Heart 2022, 9, e002060. [Google Scholar] [CrossRef]
- Patel, A.P.; Wang, M.; Pirruccello, J.P.; Ellinor, P.T.; Ng, K.; Kathiresan, S.; Khera, A.V. Lp(a) (Lipoprotein[a]) Concentrations and Incident Atherosclerotic Cardiovascular Disease. Arteriosclerosis Thromb. Vasc. Biol. 2021, 41, 465–474. [Google Scholar] [CrossRef]
- Ahmad, W.A.W. (Ed.) Annual Report of the NCVD-ACS Registry, 2018–2019; National Cardiovascular Disease Database: Kuala Lumpur, Malaysia, 2022. [Google Scholar]
- Mehta, L.S.; Beckie, T.M.; DeVon, H.A.; Grines, C.L.; Krumholz, H.M.; Johnson, M.N.; Lindley, K.J.; Vaccarino, V.; Wang, T.Y.; Watson, K.E.; et al. Acute Myocardial Infarction in Women. Circulation 2016, 133, 916–947. [Google Scholar] [CrossRef]
- Leischik, R.; Dworrak, B.; Strauss, M.; Przybylek, B.; Dworrak, T.; Schöne, D.; Horlitz, M.; Mügge, A. Plasticity of Health. Ger. J. Med. 2016, 1, 1–17. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total Population |
|---|---|
| Demography, n (%) | |
| Age, ≤50 years | 768 (47.5%) |
| Male sex | 1476 (91.2%) |
| Ethnicity | |
| Bumiputera | 993 (61.4%) |
| Chinese | 242 (15.0%) |
| Indian | 383 (23.7%) |
| Comorbidities, n (%) | |
| Self-reported hypertension | 556 (35.8%) |
| Self-reported diabetes | 448 (28.9%) |
| Self-reported dyslipidemia | 366 (23.6%) |
| Smoking | 942 (61.4%) |
| Body mass index ≥ 25 kg/m2 | 1119 (78.6%) |
| Blood parameters, mean (SD) | |
| Total cholesterol, mmol/L | 5.7 (1.6) |
| Low-density lipoprotein, mmol/L | 4.0 (1.4) |
| High-density lipoprotein, mmol/L | 1.3 (0.4) |
| Triglyceride, mmol/L | 2.2 (1.1) |
| Lipoprotein (a), mmol/L | 33.6 (28.0) |
| HbA1c, % | 7.1 (2.1) |
| Blood parameters, n (%) | |
| LDL > 2.6 mmol/L | 1269 (87.1%) |
| Lipoprotein (a) > 30 mg/dL | 566 (41.4%) |
| HbA1c > 6.5% | 609 (39.9%) |
| Cardiac characteristics, n (%) | |
| NSTEMI | 576 (35.6%) |
| Underwent PCI | 979 (60.5%) |
| STEMI patients with PCI | 670 (64.3%) |
| NSTEMI patients with PCI | 309 (53.6%) |
| Conduction Disturbances | |
| Right-bundle branch block | 26 (1.6%) |
| Left-bundle branch block | 18 (1.1%) |
| First-degree heart block | 8 (0.5%) |
| Second-degree heart block | 6 (0.4%) |
| Complete heart block | 20 (1.2%) |
| Atrial fibrillation | 29 (1.8%) |
| Ventricular fibrillation | 45 (2.8%) |
| Supraventricular tachycardia | 42 (2.6%) |
| Heart failure | 79 (6.4%) |
| LVEF in %, mean (SD) | 47.7 (11.3) |
| LVEF ≤ 40% | 316 (26.7%) |
| LVEF 41–49% | 311 (26.3%) |
| LVEF ≥ 50% | 556 (47.0%) |
| Cardiogenic shock | 161 (10.0%) |
| Cardiac arrest | 31 (1.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismail, S.R.; Mohammad, M.S.F.; Butterworth, A.S.; Chowdhury, R.; Danesh, J.; Di Angelantonio, E.; Griffin, S.J.; Pennells, L.; Wood, A.M.; Md Noh, M.F.; et al. Risk Factors of Secondary Cardiovascular Events in a Multi-Ethnic Asian Population with Acute Myocardial Infarction: A Retrospective Cohort Study from Malaysia. J. Cardiovasc. Dev. Dis. 2023, 10, 250. https://doi.org/10.3390/jcdd10060250
Ismail SR, Mohammad MSF, Butterworth AS, Chowdhury R, Danesh J, Di Angelantonio E, Griffin SJ, Pennells L, Wood AM, Md Noh MF, et al. Risk Factors of Secondary Cardiovascular Events in a Multi-Ethnic Asian Population with Acute Myocardial Infarction: A Retrospective Cohort Study from Malaysia. Journal of Cardiovascular Development and Disease. 2023; 10(6):250. https://doi.org/10.3390/jcdd10060250
Chicago/Turabian StyleIsmail, Sophia Rasheeqa, Mohd Shawal Faizal Mohammad, Adam S. Butterworth, Rajiv Chowdhury, John Danesh, Emanuele Di Angelantonio, Simon J. Griffin, Lisa Pennells, Angela M. Wood, Mohd Fairulnizal Md Noh, and et al. 2023. "Risk Factors of Secondary Cardiovascular Events in a Multi-Ethnic Asian Population with Acute Myocardial Infarction: A Retrospective Cohort Study from Malaysia" Journal of Cardiovascular Development and Disease 10, no. 6: 250. https://doi.org/10.3390/jcdd10060250
APA StyleIsmail, S. R., Mohammad, M. S. F., Butterworth, A. S., Chowdhury, R., Danesh, J., Di Angelantonio, E., Griffin, S. J., Pennells, L., Wood, A. M., Md Noh, M. F., & Shah, S. A. (2023). Risk Factors of Secondary Cardiovascular Events in a Multi-Ethnic Asian Population with Acute Myocardial Infarction: A Retrospective Cohort Study from Malaysia. Journal of Cardiovascular Development and Disease, 10(6), 250. https://doi.org/10.3390/jcdd10060250