
Association between Cognitive Impairment Severity and Polypharmacy in Older Patients with Atrial Fibrillation: A Retrospective Study Using Inpatient Data from a Specialised Geriatric Hospital

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Data Sources
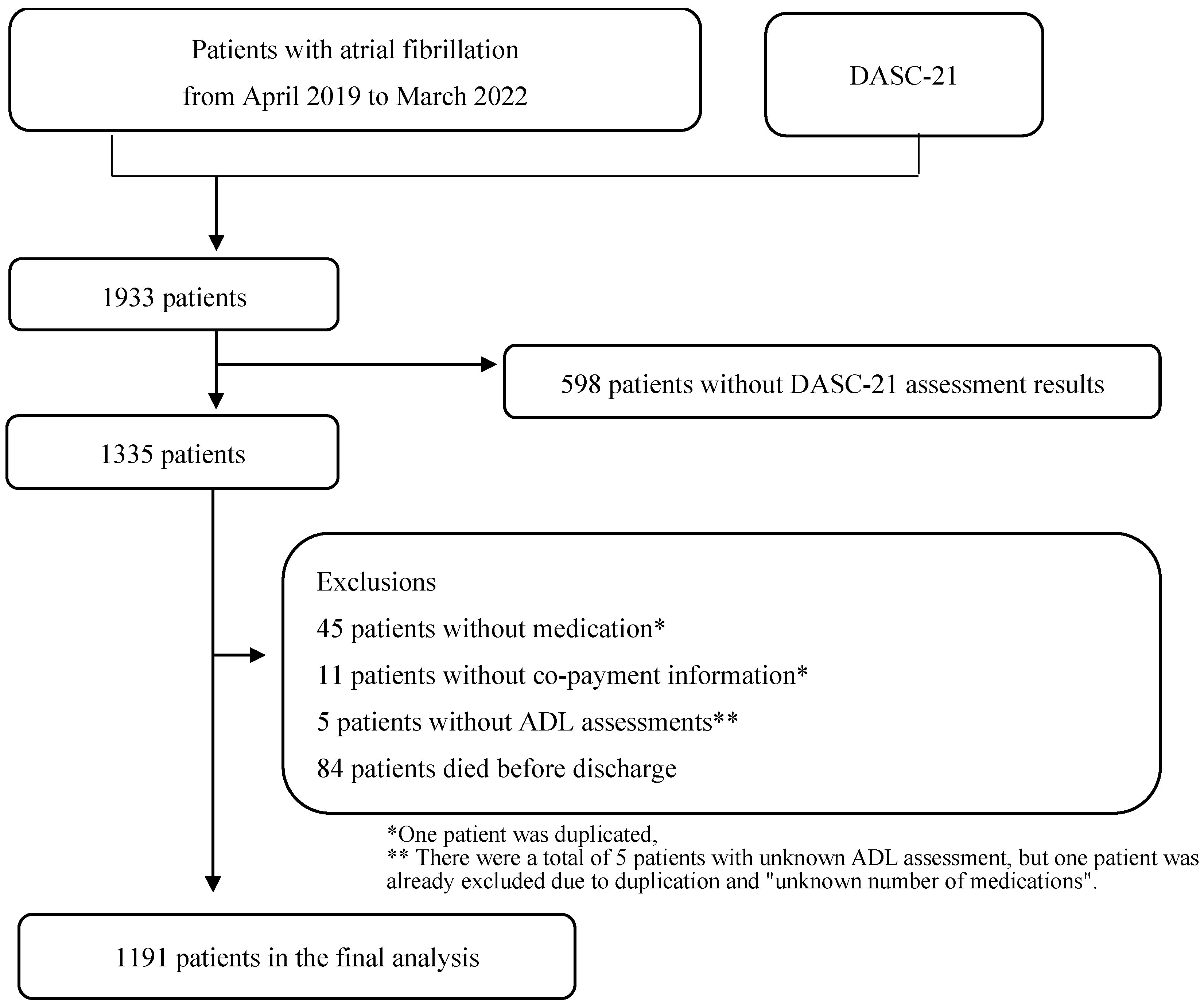
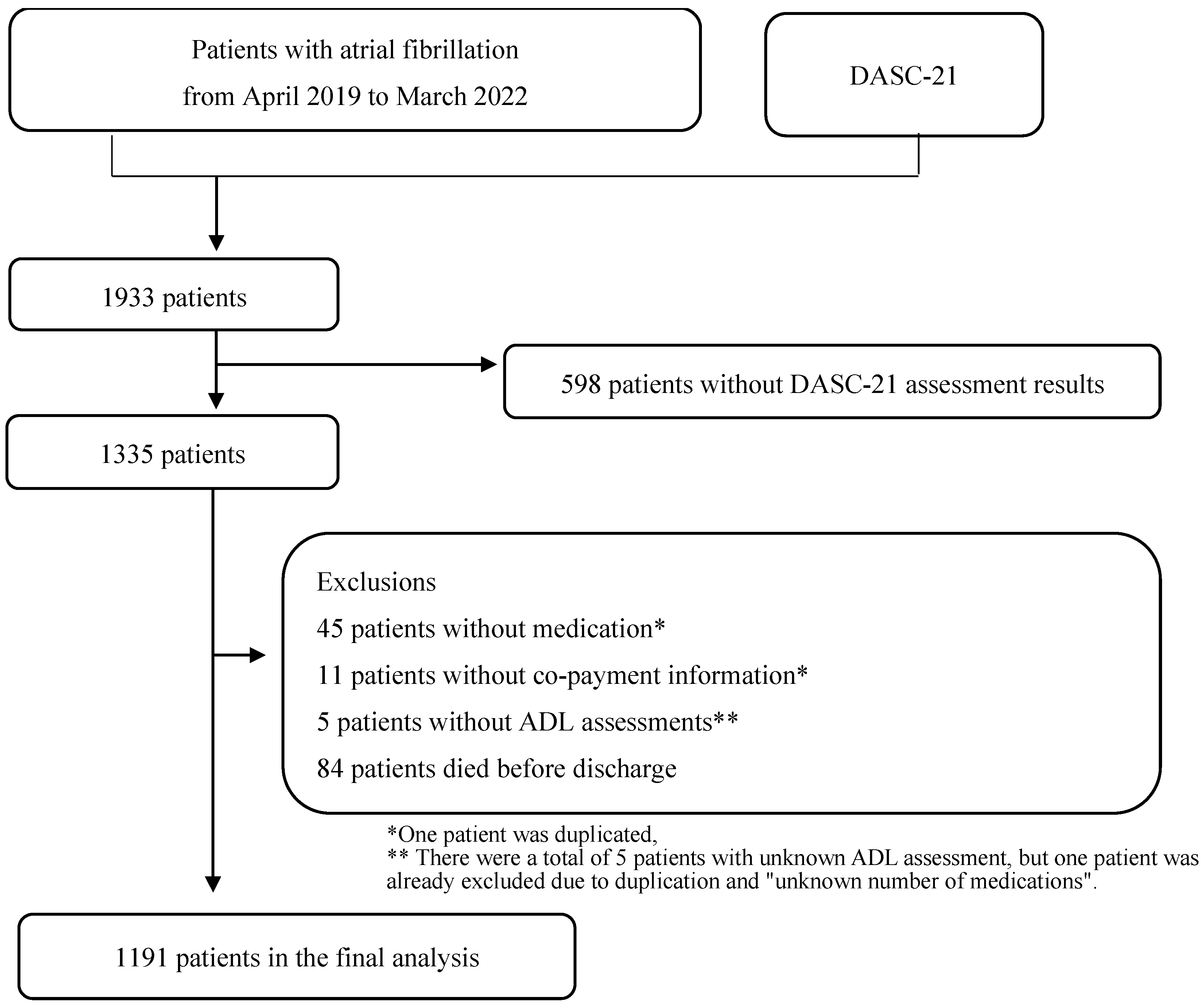
2.2. Study Population
2.3. Ethics Consideration
2.4. Variables
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Rollason, V.; Vogt, N. Reduction of polypharmacy in the elderly: A systematic review of the role of the pharmacist. Drugs Aging 2003, 20, 817–832. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.E.; Seymour, D.G.; Primrose, W.R. A systematic literature review of factors affecting outcome in older medical patients admitted to hospital. Age Ageing 2004, 33, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Frazier, S.C. Health outcomes and polypharmacy in elderly individuals: An integrated literature review. J. Gerontol. Nurs. 2005, 31, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Yadesa, T.M.; Kitutu, F.E.; Deyno, S.; Ogwang, P.W.; Tamukong, R.; Alele, P.E. Prevalence, characteristics and predicting risk factors of adverse drug reactions among hospitalized older adults: A systematic review and meta-analysis. SAGE Open Med. 2021, 9, 20503121211039100. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef]
- 2019 American Geriatrics Society Beers Criteria® Update Expert Panel; Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J.; et al. American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Scott, I.A.; Hilmer, S.N.; Reeve, E.; Potter, K.; Le Couteur, D.; Rigby, D.; Gnjidic, D.; Del Mar, C.B.; Roughhead, E.E.; Page, A.; et al. Reducing inappropriate polypharmacy: The process of deprescribing. JAMA Intern. Med. 2015, 175, 827–834. [Google Scholar] [CrossRef]
- Frankenthal, D.; Lerman, Y.; Kalendaryev, E.; Lerman, Y. Intervention with the screening tool of older persons potentially inappropriate prescriptions/screening tool to alert doctors to right treatment criteria in elderly residents of a chronic geriatric facility: A randomized clinical trial. J. Am. Geriatr. Soc. 2014, 62, 1658–1665. [Google Scholar] [CrossRef]
- Ravn-Nielsen, L.V.; Duckert, M.-L.; Lund, M.L.; Henriksen, J.P.; Nielsen, M.L.; Eriksen, C.S.; Buck, T.C.; Pottergard, A.; Hansen, M.R.; Hallas, J. Effect of an in-hospital multifaceted clinical pharmacist intervention on the risk of readmission: A randomized clinical trial. JAMA Intern. Med. 2018, 178, 375–382. [Google Scholar] [CrossRef]
- Gutiérrez-Valencia, M.; Izquierdo, M.; Beobide-Telleria, I.; Ferro-Uriguen, A.; Alonso-Renedo, J.; Casas-Herrero, Á.; Martínez-Velilla, N. Medicine optimization strategy in an acute geriatric unit: The pharmacist in the geriatric team. Geriatr. Gerontol. Int. 2019, 19, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Hatano, M.; Mizuno, T.; Arakawa, Y.; Inagaki, R.; Kato, A.; Matsuzaki, H.; Mizokami, F.; Koseki, T.; Yamada, S. Efficacy of a pharmacist team clinical medication review in older adults: A prospective and retrospective observational study. Biol. Pharm. Bull. 2022, 45, 1166–1171. [Google Scholar] [CrossRef] [PubMed]
- Stuijt, C.C.M.; Franssen, E.J.F.; Egberts, A.C.G.; Hudson, S.A. Appropriateness of prescribing among elderly patients in a Dutch residential home: Observational study of outcomes after a pharmacist-led medication review. Drugs Aging 2008, 25, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Seong, H.-J.; Lee, K.; Kim, B.-H.; Son, Y.-J. Cognitive impairment is independently associated with non-adherence to antithrombotic therapy in older patients with atrial fibrillation. Int. J. Environ. Res. Public Health 2019, 16, 2698. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.L.; Boustani, M.A.; Skopelja, E.N.; Gao, S.; Unverzagt, F.W.; Murray, M.D. Medication adherence in older adults with cognitive impairment: A systematic evidence-based review. Am. J. Geriatr. Pharmacother. 2012, 10, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.H.; Shin, D.W.; Chang, S.-A.; Lee, J.E.; Jeong, S.-M.; Kim, S.H.; Yun, J.M.; Son, K. Association between cognitive impairment and poor antihypertensive medication adherence in elderly hypertensive patients without dementia. Sci. Rep. 2018, 8, 11688. [Google Scholar] [CrossRef]
- Salas, M.; In’t Veld, B.A.; van der Linden, P.D.; Hofman, A.; Breteleer, M.; Stricker, B.H. Impaired cognitive function and compliance with antihypertensive drugs in elderly: The Rotterdam Study. Clin. Pharmacol. Ther. 2001, 70, 561–566. [Google Scholar] [CrossRef]
- Stuck, A.E.; Siu, A.L.; Wieland, G.D.; Adams, J.; Rubenstein, L.Z. Comprehensive geriatric assessment: A meta-analysis of controlled trials. Lancet 1993, 342, 1032–1036. [Google Scholar] [CrossRef]
- Devons, C.A.J. Comprehensive geriatric assessment: Making the most of the aging years. Curr. Opin. Clin. Nutr. Metab. Care 2002, 5, 19–24. [Google Scholar] [CrossRef]
- Unutmaz, G.D.; Soysal, P.; Tuven, B.; Isik, A.T. Costs of medication in older patients: Before and after comprehensive geriatric assessment. Clin. Interv. Aging 2018, 13, 607–613. [Google Scholar] [CrossRef]
- Sergi, G.; De Rui, M.; Sarti, S.; Manzato, E. Polypharmacy in the elderly: Can comprehensive geriatric assessment reduce inappropriate medication use? Drugs Aging 2011, 28, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Hosoi, T.; Yamana, H.; Tamiya, H.; Matsui, H.; Fushimi, K.; Akishita, M.; Yasunaga, H.; Ogawa, S. Association between comprehensive geriatric assessment and polypharmacy at discharge in patients with ischaemic stroke: A nationwide, retrospective, cohort study. eClinicalMedicine 2022, 50, 101528. [Google Scholar] [CrossRef] [PubMed]
- Lea, S.C.; Watts, K.L.; Davis, N.A.; Panayiotou, B.; Bankart, M.J.; Arora, A.; Chanmbers, R. The potential clinical benefits of medicines optimisation through comprehensive geriatric assessment, carried out by secondary care geriatricians, in a general practice care setting in North Staffordshire, UK: A feasibility study. BMJ Open 2017, 7, e015278. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, P.; Woolford, S.J.; Patel, H.P. Multi-morbidity and polypharmacy in older people: Challenges and opportunities for clinical practice. Geriatrics 2020, 5, 85. [Google Scholar] [CrossRef] [PubMed]
- Awata, S.; Sugiyama, M.; Ito, K.; Ura, C.; Miyamae, F.; Sakuma, N.; Niikawa, H.; Okamuram, T.; Inagaki, H.; Ijuin, M. Development of the dementia assessment sheet for community-based integrated care system. Geriatr. Gerontol. Int. 2016, 16 (Suppl. S1), 123–131. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, C.; Nyfort-Hansen, K.; Rowett, D.; Wong, C.X.; Middeldorp, M.E.; Mahajan, R.; Lau, D.H.; Sanders, P.; Hendriks, J.M. Polypharmacy and health outcomes in atrial fibrillation: A systematic review and meta-analysis. Open Heart 2020, 7, 001257. [Google Scholar] [CrossRef]
- Yamana, H.; Moriwaki, M.; Horiguchi, H.; Kodan, M.; Fushimi, K.; Yasunaga, H. Validity of diagnoses, procedures, and laboratory data in Japanese administrative data. J. Epidemiol. 2017, 27, 476–482. [Google Scholar] [CrossRef]
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and profile of diagnosis procedure combination (DPC): Development of a real data collection system for acute inpatient care in Japan. J. Epidemiol. 2021, 31, 1–11. [Google Scholar] [CrossRef]
- dasc.jp. What Is DASC-21; DASC-21 Manual. Available online: https://dasc.jp/en/about (accessed on 18 January 2023).
- Kojima, T.; Mizukami, K.; Tomita, N.; Arai, H.; Ohrui, T.; Eto, M.; Takeya, Y.; Isaka, Y.; Rakugi, H.; Sudo, N.; et al. Screening Tool for Older Persons’ Appropriate Prescriptions for Japanese: Report of the Japan Geriatrics Society Working Group on “Guidelines for medical treatment and its safety in the elderly”. Geriatr. Gerontol. Int. 2016, 16, 983–1001. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-H.; Saunders, L.D.; Beck, C.A.; Feasby, T.; Ghali, W. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Fried, T.R.; Mecca, M.C. Medication Appropriateness in Vulnerable Older Adults: Healthy Skepticism of Appropriate Polypharmacy. J. Am. Geriatr. Soc. 2019, 67, 1123–1127. [Google Scholar] [CrossRef] [PubMed]
- Vordenberg, S.E.; Malani, P.N.; Kullgren, J.T. Polypharmacy and deprescribing. JAMA 2023, 330, 672. [Google Scholar] [CrossRef] [PubMed]
- Krishnaswami, A.; Steinman, M.A.; Goyal, P.; Zullo, A.R.; Anderson, T.S.; Birtcher, K.K.; Goodlin, S.J.; Maurer, M.S.; Alexander, K.P.; Rich, M.W.; et al. Deprescribing in Older Adults With Cardiovascular Disease. J. Am. Coll. Cardiol. 2019, 73, 2584–2595. [Google Scholar] [CrossRef] [PubMed]
- Ouellet, G.M.; Fried, T.R.; Gilstrap, L.G.; O’Leary, J.R.; Austin, A.M.; Skinner, J.S.; Cohen, A.B. Anticoagulant use for atrial fibrillation among persons with advanced dementia at the end of life. JAMA Intern. Med. 2021, 181, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Paque, K.; De Schreye, R.; Elseviers, M.; Stichele, R.V.; Pardon, K.; Dilles, T.; Christiaens, T.; Deliens, L.; Cohen, J. Discontinuation of medications at the end of life: A population study in Belgium, based on linked administrative databases. Br J. Clin. Pharmacol. 2019, 85, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Tjia, J.; Cutrona, S.L.; Peterson, D.; Reed, G.; Andrade, S.E.; Mitchell, S.L. Statin discontinuation in nursing home residents with advanced dementia. J. Am. Geriatr. Soc. 2014, 62, 2095–2101. [Google Scholar] [CrossRef] [PubMed]
- Kutner, J.S.; Blatchford, P.J.; Taylor, D.H., Jr.; Ritchie, C.S.; Bull, J.H.; Fairclough, D.L.; Hanson, L.C.; LeBlanc, T.W.; Samsa, G.P.; Wolf, S.; et al. Safety and benefit of discontinuing statin therapy in the setting of advanced, life-limiting illness: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 691–700. [Google Scholar] [CrossRef]
- 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2023, 71, 2052–2081. [Google Scholar] [CrossRef]
- Ravindrarajah, R.; Hazra, N.C.; Hamada, S.; Charlton, J.; Jackson, S.H.D.; Dregan, A.; Gulliford, M.C. Systolic blood pressure trajectory, frailty, and all-cause mortality >80 years of age: Cohort study using electronic health records. Circulation 2017, 135, 2357–2368. [Google Scholar] [CrossRef]
- Goyal, P.; Bryan, J.; Kneifati-Hayek, J.; Sterling, M.R.; Banerjee, S.; Maurer, M.S.; Lachs, M.S.; Safford, M.M. Association between functional impairment and medication burden in adults with heart failure. J. Am. Geriatr. Soc. 2019, 67, 284–291. [Google Scholar] [CrossRef]
- Kuzuya, M.; Hirakawa, Y.; Suzuki, Y.; Iwata, M.; Enoki, H.; Hasegawa, J.; Iguchi, A. Association between unmet needs for medication support and all-cause hospitalization in community-dwelling disabled elderly people. J. Am. Geriatr. Soc. 2008, 56, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.E.; Birge, S.J. Cognitive dysfunction, medication management, and the risk of readmission in hospital inpatients. J. Am. Geriatr. Soc. 2016, 64, 1464–1468. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Romiti, G.F.; Vitolo, M.; Harrison, S.L.; Lane, D.A.; Fauchier, L.; Marin, F.; Näbauer, M.; Potpara, T.S.; Dan, G.-A.; et al. Epidemiology and impact of frailty in patients with atrial fibrillation in Europe. Age Ageing 2022, 51, afac192. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Barba, B.; Navarrete-Reyes, A.P.; Avila-Funes, J.A. Are geriatric syndromes associated with reluctance to initiate oral anticoagulation therapy in elderly adults with nonvalvular atrial fibrillation? J. Am. Geriatr. Soc. 2013, 61, 2236–2237. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| All | ≤5 Medications | >6 Medications | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n = 1191 | n = 267 | n = 924 | |||||
| Sex, male, n (%) | 584 | 49.0% | 142 | 53.2% | 442 | 47.8% | 0.1236 |
| Age, years, n (%) | 0.0135 * | ||||||
| ≤74 | 186 | 15.6% | 55 | 20.6% | 131 | 14.2% | |
| 75–84 | 477 | 40.1% | 91 | 34.1% | 386 | 41.8% | |
| ≥85 | 528 | 44.3% | 121 | 45.3% | 407 | 44.1% | |
| BMI, kg/m2, n (%) | 0.0280 * | ||||||
| <18.5 | 197 | 16.5% | 55 | 20.6% | 142 | 15.4% | |
| ≥18.5 to <25 | 716 | 60.1% | 163 | 61.1% | 553 | 59.9% | |
| ≥25 | 278 | 23.3% | 49 | 18.4% | 229 | 24.8% | |
| Length of hospital stay, days, n (%) | 0.4102 | ||||||
| ≤7 | 340 | 28.6% | 82 | 30.7% | 258 | 27.9% | |
| 8 to 14 | 273 | 22.9% | 67 | 25.1% | 206 | 22.3% | |
| 15 to 25 | 281 | 23.6% | 60 | 22.5% | 221 | 23.9% | |
| ≥26 | 297 | 24.9% | 58 | 21.7% | 239 | 25.9% | |
| Hospitalisation pathway, n (%) | 0.1408 | ||||||
| Household | 1060 | 89.0% | 231 | 86.5% | 829 | 89.7% | |
| Transfer | 131 | 11.0% | 36 | 13.5% | 95 | 10.3% | |
| Emergency hospitalisation, n (%) | 738 | 62.0% | 177 | 66.3% | 561 | 60.7% | 0.0982 |
| Discharge destination, n (%) | 0.0013 * | ||||||
| Household | 868 | 72.9% | 174 | 65.2% | 694 | 75.1% | |
| Transfer | 323 | 27.1% | 93 | 34.8% | 230 | 24.9% | |
| Patient co-payment rate, n (%) | 0.0194 * | ||||||
| 0% | 64 | 5.4% | 12 | 4.5% | 52 | 5.6% | |
| 10% | 930 | 78.1% | 196 | 73.4% | 734 | 79.4% | |
| 30% | 197 | 16.5% | 59 | 22.1% | 138 | 14.9% | |
| Charlson Comorbidity Index, n (%) | 0.0003 * | ||||||
| 0 | 120 | 10.1% | 37 | 13.9% | 83 | 9.0% | |
| 1 or 2 | 686 | 57.6% | 169 | 63.3% | 517 | 56.0% | |
| ≥3 | 385 | 32.3% | 61 | 22.8% | 324 | 35.1% | |
| Comorbidities, n (%) | |||||||
| Connective tissue disease/rheumatic disease | 22 | 1.9% | 4 | 4.8% | 18 | 3.7% | 0.6306 |
| Peptic ulcer disease | 97 | 8.1% | 17 | 20.5% | 80 | 16.6% | 0.2280 |
| Diabetes without complications | 279 | 23.4% | 45 | 54.2% | 234 | 48.5% | 0.004 * |
| Diabetes with complications | 77 | 6.5% | 4 | 4.8% | 73 | 15.1% | 0.0002 * |
| Renal disease | 90 | 7.6% | 13 | 15.7% | 77 | 16.0% | 0.0592 |
| Concomitant medication, n (%) | |||||||
| Antithrombotic | 894 | 75.1% | 174 | 65.2% | 720 | 77.9% | <0.0001 * |
| Benzodiazepines | 152 | 12.8% | 10 | 3.7% | 142 | 15.4% | <0.0001 * |
| STOPP-J ** | 167 | 14.0% | 15 | 5.6% | 152 | 16.5% | <0.0001 * |
| Proton pump inhibitor | 799 | 67.1% | 107 | 40.1% | 692 | 74.9% | <0.0001 * |
| Statins | 410 | 34.4% | 35 | 13.1% | 375 | 40.6% | <0.0001 * |
| Number of medications, median (IQR) | 8.0 | (6–11) | 4.0 | (3–5) | 9.0 | (8–12) | <0.0001 * |
| DASC-21 total scores, median (IQR) | 28.0 | (23–45) | 28.0 | (22–51) | 28.5 | (23–44) | 0.8235 |
| DASC-21 dementia severity 4 classification | 0.0005 * | ||||||
| Normal | 649 | 54.5% | 146 | 54.7% | 503 | 54.4% | |
| Mild | 158 | 13.3% | 24 | 9.0% | 134 | 14.5% | |
| Moderate | 351 | 29.5% | 81 | 30.3% | 270 | 29.2% | |
| Severe | 33 | 2.8% | 16 | 6.0% | 17 | 1.8% | |
| Variables | >6 Medications | >8 Medications | >10 Medications | |||
|---|---|---|---|---|---|---|
| aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | |
| Sex, male | 0.82 (0.59–1.13) | 0.219 | 0.82 (0.62–1.07) | 0.147 | 1.02 (0.78–1.34) | 0.860 |
| Age, years, ref ≤ 74 | ||||||
| 75–84 | 1.87 (1.20–2.91) | 0.006 | 1.49 (1.01–2.20) | 0.047 | 1.47 (0.99–2.19) | 0.057 |
| ≥85 | 2.08 (1.28–3.37) | 0.003 | 1.42 (0.93–2.16) | 0.105 | 1.55 (1.01–2.40) | 0.045 |
| BMI, kg/m2, ref < 18.5 | ||||||
| 18.5–25 | 1.11 (0.73–1.68) | 0.624 | 1.03 (0.71–1.49) | 0.860 | 1.18 (0.80–1.74) | 0.398 |
| >25 | 1.45 (0.86–2.47) | 0.167 | 1.33 (0.85–2.08) | 0.216 | 1.38 (0.88–2.18) | 0.161 |
| Length of hospitalisation, days | ||||||
| ≥ 26 | 1.95 (1.29–2.94) | 0.002 | 1.80 (1.28–2.53) | <0.001 | 1.69 (1.21–2.37) | 0.002 |
| Hospitalisation pathway | ||||||
| Transfer | 1.50 (0.85–2.65) | 0.165 | 1.47 (0.90–2.40) | 0.120 | 1.25 (0.75–2.07) | 0.388 |
| Emergency hospitalisation | 0.81 (0.56–1.16) | 0.248 | 0.85 (0.62–1.15) | 0.285 | 0.92 (0.68–1.25) | 0.603 |
| Discharge destination | ||||||
| Transfer | 0.50 (0.32–0.78) | 0.002 | 0.64 (0.43–0.93) | 0.020 | 0.63 (0.43–0.93) | 0.020 |
| CCI, ref = 0 | ||||||
| 1–2 | 1.19 (0.73–1.94) | 0.479 | 1.18 (0.76–1.84) | 0.461 | 1.35 (0.83–2.19) | 0.225 |
| ≥3 | 1.76 (0.98–3.15) | 0.058 | 1.60 (0.96–2.66) | 0.074 | 1.63 (0.95–2.81) | 0.077 |
| Comorbidities | ||||||
| Connective tissue disease/rheumatic disease | 0.96 (0.30–3.09) | 0.951 | 1.66 (0.60–4.58) | 0.328 | 3.16 (1.23–8.08) | 0.017 |
| Peptic ulcer disease | 1.14 (0.62–2.09) | 0.679 | 1.21 (0.74–1.99) | 0.439 | 1.41 (0.89–2.26) | 0.146 |
| Diabetes without complications | 1.48 (0.99–2.22) | 0.058 | 1.57 (1.13–2.18) | 0.007 | 1.28 (0.94–1.76) | 0.122 |
| Diabetes with complications | 4.46 (1.50–13.2) | 0.007 | 3.60 (1.78–7.24) | <0.001 | 2.90 (1.68–5.03) | <0.001 |
| Renal disease | 1.78 (0.87–3.64) | 0.113 | 1.91 (1.08–3.36) | 0.026 | 1.56 (0.93–2.62) | 0.091 |
| DASC-21 dementia severity 4 classification, ref = severe | ||||||
| Normal | 2.04 (0.84–4.94) | 0.116 | 3.13 (1.23–8.01) | 0.017 | 3.76 (1.04–13.5) | 0.043 |
| Mild | 3.33 (1.29–8.57) | 0.013 | 4.16 (1.58–10.9) | 0.004 | 4.26 (1.16–15.6) | 0.029 |
| Moderate | 2.46 (1.06–5.72) | 0.036 | 3.68 (1.48–9.18) | 0.005 | 3.95 (1.11–14.0) | 0.033 |
| Concomitant medication | ||||||
| Antithrombotic | 2.11 (1.51–2.95) | <0.001 | 2.42 (1.79–3.27) | <0.001 | 2.01 (1.46–2.77) | <0.001 |
| BZs | 5.25 (2.65–10.4) | <0.001 | 4.42 (2.77–7.05) | <0.001 | 4.04 (2.74–5.96) | <0.001 |
| STOPP-J | 4.26 (2.36–7.69) | <0.001 | 2.29 (1.53–3.42) | <0.001 | 1.90 (1.31–2.75) | 0.002 |
| Statins | 4.36 (2.91–6.52) | <0.001 | 3.07 (2.29–4.12) | <0.001 | 2.49 (1.89–3.28) | <0.001 |
| Number of Medications (per 100 Patients), Mean ± SD | Multiple Comparison Analysis *, p-Value | ||||||
|---|---|---|---|---|---|---|---|
| DASC-21 Classification | Normal | Mild | Moderate | Severe | Normal | Mild | Moderate |
| Antithrombotics | 76.7 ± 42.3 | 73.4 ± 44.3 | 73.2 ± 44.3 | 69.6 ± 46.7 | 0.501 | 0.855 | 0.855 |
| Benzodiazepines | 18.0 ± 44.4 | 15.8 ± 41.5 | 7.69 ± 28.7 | 0 | 0.026 | 0.041 | 0.179 |
| STOPP-J medications | 8.9 ± 31.6 | 19.6 ± 41.4 | 21.7 ± 43.9 | 12.1 ± 33.1 | 0.577 | 0.491 | 0.356 |
| Proton pump inhibitors | 67.5 ± 46.9 | 68.4 ± 46.7 | 67.8 ± 46.8 | 45.5 ± 50.6 | 0.017 | 0.023 | 0.018 |
| Statins | 40.5 ± 49.1 | 34.8 ± 47.8 | 25.1 ± 43.4 | 12.1 ± 33.1 | 0.002 | 0.019 | 0.154 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimazaki, Y.; Kishimoto, K.; Ishikawa, J.; Iwakiri, R.; Araki, A.; Imai, S. Association between Cognitive Impairment Severity and Polypharmacy in Older Patients with Atrial Fibrillation: A Retrospective Study Using Inpatient Data from a Specialised Geriatric Hospital. Geriatrics 2024, 9, 15. https://doi.org/10.3390/geriatrics9010015
Shimazaki Y, Kishimoto K, Ishikawa J, Iwakiri R, Araki A, Imai S. Association between Cognitive Impairment Severity and Polypharmacy in Older Patients with Atrial Fibrillation: A Retrospective Study Using Inpatient Data from a Specialised Geriatric Hospital. Geriatrics. 2024; 9(1):15. https://doi.org/10.3390/geriatrics9010015
Chicago/Turabian StyleShimazaki, Yoshitomo, Keiko Kishimoto, Joji Ishikawa, Rika Iwakiri, Atsushi Araki, and Shinobu Imai. 2024. "Association between Cognitive Impairment Severity and Polypharmacy in Older Patients with Atrial Fibrillation: A Retrospective Study Using Inpatient Data from a Specialised Geriatric Hospital" Geriatrics 9, no. 1: 15. https://doi.org/10.3390/geriatrics9010015
APA StyleShimazaki, Y., Kishimoto, K., Ishikawa, J., Iwakiri, R., Araki, A., & Imai, S. (2024). Association between Cognitive Impairment Severity and Polypharmacy in Older Patients with Atrial Fibrillation: A Retrospective Study Using Inpatient Data from a Specialised Geriatric Hospital. Geriatrics, 9(1), 15. https://doi.org/10.3390/geriatrics9010015