Efficacy of Platelet-Rich Plasma in the Treatment of Equine Tendon and Ligament Injuries: A Systematic Review of Clinical and Experimental Studies



Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Review Protocol
2.1.1. PICO Strategy
2.1.2. Eligibility Criteria for Publications and Protocol for Data Collection, Screening, and Inclusion
2.2. Summarizing the Articles
2.3. Platelet-Rich Plasma Quality
2.4. Bias Risk Assessment
3. Results
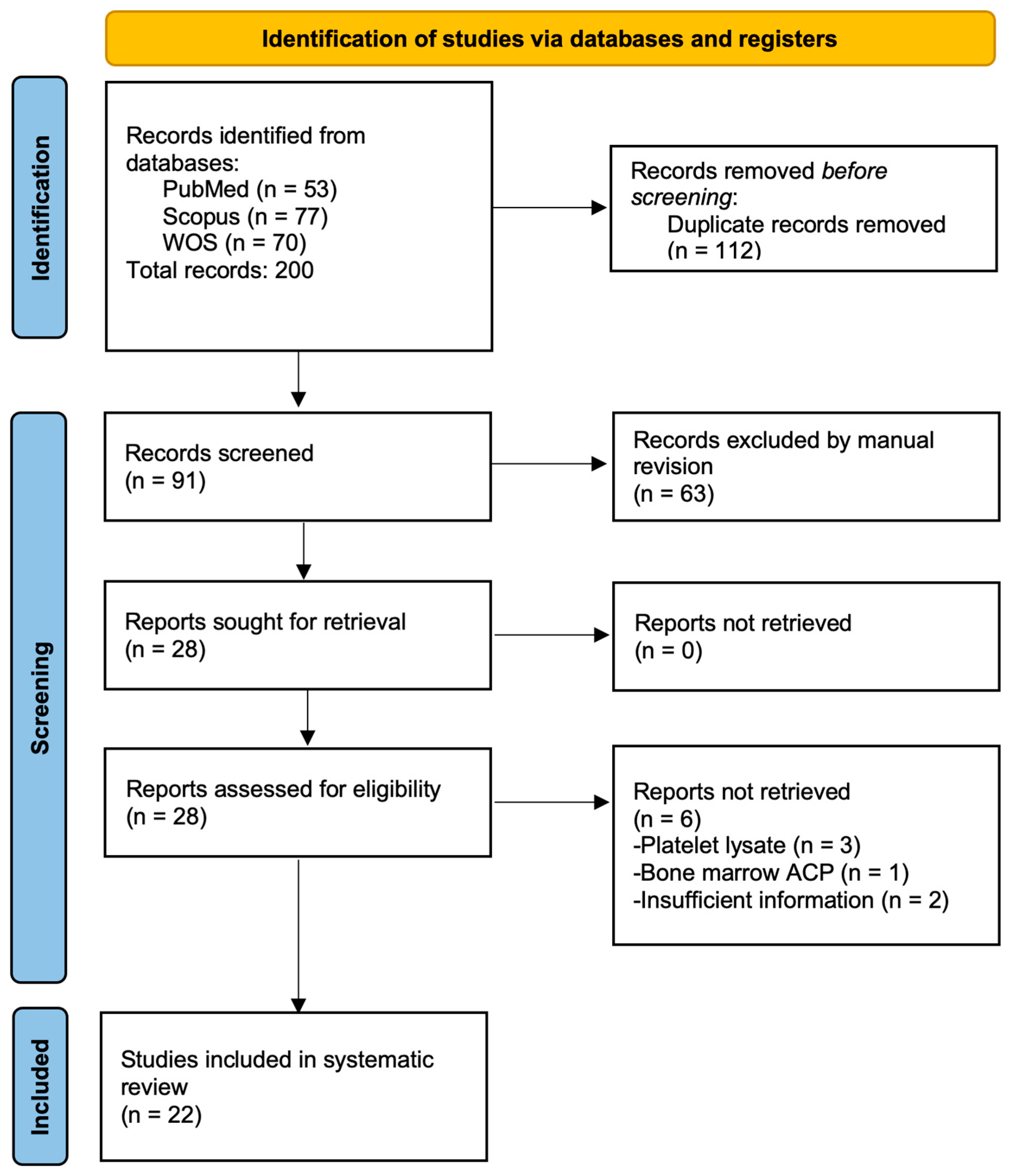
3.1. General Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Type, Number of Animals, and Objectives | Study Design | Results and Adverse Effects | Length of Follow-Up | Outcome |
|---|---|---|---|---|---|
| Argüelles et al. [18] | Case series; 5 horses, 2 with superficial digital flexor tendon tendinopathy (SDFTT) and 3 with proximal desmitis of the suspensory ligament (PDSL). Objective: To evaluate the effect of autologous platelet-rich plasma (PRP) on lameness scores and ultrasound (US) changes. | 4–5 mL of PRP was injected intralesionally (IL) 3 times at 2-week intervals; US and lameness evaluations were performed prior to each treatment. | Improvements in lameness and US appearance in SDFTT cases. Clinical improvement but no US changes in PDSL cases. No side effects were reported. | 20 months | Positive |
| Castelijns et al. [37] | Case series; 11 horses with 18 suspensory ligament (SL) branch (SLB) injuries. To evaluate the effect of an autologous PRP product on lameness scores and US changes. | 2.5 mL of PRP obtained by a gravitational method was injected IL only once per affected structure. Horses were evaluated by a lameness examination and US before and 3 months after treatment | A good US appearance was noted in 8 horses at 3 months. Ten horses were not lame after 3 months. Five horses returned to full work, 1 to a lower level, 3 retired, 1 was still recovering, and 1 died of unrelated causes at 3 years. No side effects were reported. | 36 months | Positive |
| Georg et al. [38] | Case series; 7 horses, 5 with SDFTT, 1 with inferior check ligament injury, and 1 with tendinopathy of the deep digital flexor tendon (DDFTT). To evaluate the effect of an autologous PRP product (autologous conditioned plasma (ACP)) on lameness scores and US changes. | 2–4 mL of PRP obtained by a semiautomated kit was injected IL only once per affected structure. Horses were evaluated by a lameness examination and US before and 2 and 3 weeks after treatment. | In general, all horses showed improvement of the US appearance at 3 weeks after treatment. All horses returned to the previous workload or full training at 9 months. No adverse effects were reported. | 10–13 months | Positive |
| Waselau et al. [17] | Case series; 9 horses with midbody SL desmitis (MSD). The aim was to evaluate the effect of one IL PRP dose by US examination and follow-up of race performance over three years. | 7–12 mL PRP was injected IL, followed by controlled exercise. Horses were monitored by US. | A total of 100% returned to racing between 28 and 68 weeks. Nine horses raced during first and second years, while only five raced during the third year. No adverse effects were reported. | 36 months | Positive |
| Zuffova et al. [39] | Case series; 22 horses with SDFTT. The aim was to evaluate the effectiveness of PRP in treating SDFT lesions by US and return to racing. | The PRP volume was injected IL according to the size of the lesion. Only one PRP dose was injected. | PRP shortened the rehabilitation time, and increased the return to racing. No adverse effects. | Up to 48 months | Positive |
| Study | Study Type, Number of Animals, and Objectives | Study Design | Results and Adverse Effects | Length of Follow-Up | Outcome |
|---|---|---|---|---|---|
| Beerts et al. [40] | Case series; 104 horses. The aim was to evaluate the combination of allogeneic mesenchymal stem cells (MSCs) and PRP by US and lameness examinations in 68 horses with SLD and 36 with SDFTT. | One IL injection of 2–3 × 106 allogeneic MSCs (1 mL) plus 1 mL of PRP. Horses were evaluated at 6 and 12 weeks, and 12 and 24 months. | At 24 months, 82.4% of horses with SLD and 85.7% with SDFTT maintained competition levels. Some horses (14.7% with SL and 14.3% with SDFT) relapsed and retired. No major adverse effects were reported. | 24 months | Positive |
| Guercio et al. [41] | Case series; 9 horses with SDFTT. The aim was to evaluate the combination of adipose-derived MSCs (AD-MSCs) plus PRP by US and clinical follow-up. | One only dose of 1 × 106 autologous AD-MSCs mixed with 5–10 mL of PRP was injected IL. Horses were evaluated by US at 1, 2, and 4 months. | Seven horses resumed their normal competitive activity after 9 months. Two horses were reinjured. No adverse effects. | 9 months | Positive |
| Ricco et al. [42] | Case series; 19 horses with SDFTT. The aim was to evaluate the effect of allogeneic AD-MSCs in combination with autologous PRP by US and performance results. | One only dose of 2–6 mL of PRP containing 2 × 106 AD-MSCs/mL was injected IL. | US improvement at 3 months. Seventeen horses (89.5%) returned to competition, while two (10.5%) were reinjured. No adverse effects were reported. | 24 months | Positive |
| Torricelli et al. [43] | Case series; 13 horses, 12 with SLD and 1 with SDFTT. The aim was to evaluate the effect of autologous bone marrow mononuclear cells (BMMNCs) plus PRP by US, lameness examination, and performance results. | One only dose of 4–7 mL of BMMNCs (1.9 × 106 cells) and autologous PRP was injected IL. | All horses showed an US improvement. Eleven horses (84.6%) returned to competition. Faster recovery was observed in horses treated with PRP with more than 750 × 103/µL platelets (2.8 ± 0.4 months) with respect to horses who received less concentrated PRP (7.9± 4.3 months). No adverse effects. | 12 months | Positive |
| Study | Study Type, Number of Animals, and Objectives | Study Design | Results and Adverse Effects | Length of Follow-Up | Outcome |
|---|---|---|---|---|---|
| Garrett et al. [44] | Randomized clinical trial; 39 horses with proximal sesamoiditis and associated SL branch desmitis (SLBD). The aim was to compare the effects of PRP and a saline solution (SS) by US and performance results. | Horses were randomized to receive a single 3 mL dose of PRP (treatment group) or 3 mL of SS (control group). Racing performance was followed for 2, 3, and 4 years. | PRP horses more likely to race at 2 years old. No significant difference in racing performance was observed at 3 and 4 years. | 36 months | Positive |
| Geburek et al. [45] | Randomized controlled clinical trial; 20 horses with SDFTT. The aim was to compare the effects of PRP and SS by US and performance results. | Horses were randomized to receive a single 3 mL dose of PRP (treatment group) or 3 mL of SS (control group). US and clinical evaluations were performed at 5 intervals up to 24 weeks. | The PRP group showed an earlier reduction in lameness and improved matrix organization. No significant difference in the cross-sectional area was observed. A total of 80% of PRP horses returned to the previous or higher level vs. 50% of control horses at 12 months. | 24 months | Positive |
| Giunta et al. [46] | Prospective randomized trial; 100 horses with PSD. The aim was to compare PRP with extracorporeal shockwave therapy (EST) by US, lameness examination, and performance results. | Horses were randomly allotted to receive 3–6 mL of autologous PRP or EST (800 pulses). The PRP group included 47 horses, 19 with affected forelimbs and 28 with affected hindlimbs. The EST group included 49 horses, 14 with affected forelimbs and 35 with affected hindlimbs. Horses were evaluated at 4 days, 6 months, and 12 months. | EST improved short-term lameness more than PRP. At one year, EST had a higher return-to-work rate overall. PRP showed better outcomes in horses with severe ultrasound changes. EST associated with a 3.8x higher return to work at 1 year. | 12 months | Negative |
| Maleas and Mageed [47] | Randomized controlled multicentric clinical trial; 93 horses with chronic hindlimb PSLD. The aim was to compare the effect of autologous PRP with a bone marrow aspirate concentrate (BMAC) by clinical, US, and performance results. | Horses were allocated into 3 groups, Control (exercise only, n = 22), 2–4 mL of PRP (n = 46), and 2–4 mL of BMAC (n = 25), and evaluated at 6, 12, and 18 months. | BMAC yielded better lameness scores than PRP; 84% of BMAC horses were sound. Both BMAC and PRP were significantly better than controlled exercise alone for treating chronic hindlimb PSD. BMAC appeared to lead to better short- and long-term outcomes (soundness) than PRP. The cytology of BMAC did not predict outcomes. No adverse effects were reported. | 18 months | Negative |
| Study | Study Type, Number of Animals, and Objectives | Study Design | Results and Adverse Effects | Length of Follow-up | Outcome |
|---|---|---|---|---|---|
| Bosch et al. [50] | Experimental, placebo-controlled study of 6 clinically healthy horses. The effect of PRP on standardized, surgically induced lesions in the forelimb SDFTs was evaluated at 24 weeks from treatment by biochemical, biomechanical and histology analyses. | Surgically induced forelimb SDFT lesions were randomly treated with a single dose of 3 mL of autologous PRP or SS. Horses were maintained on an exercise protocol, and euthanasia was performed at 24 weeks. | The PRP group had significantly higher collagen, GAG, and DNA contents. An improved tensile strength and elastic modulus were observed in the PRP group. Histology revealed a better structural organization and higher metabolic activity in the PRP group. | 24 weeks | Positive |
| Bosch et al. [48] | Experimental, placebo-controlled study of 6 clinically healthy horses. The aim was to evaluate the effect of PRP on neovascularization by color Doppler US (CDUS) and immunohistochemistry in surgically induced lesions in the forelimb SDFTs. | Surgically induced forelimb SDFT lesions were randomly treated with a single dose of 3 mL of autologous PRP or SS. Horses were maintained on an exercise protocol, and euthanasia was performed at 24 weeks. Limbs were scanned at 1 week after surgery, just before the PRP or placebo injection, and at 2, 3, 5, 8, 12, 18 and 24 weeks after surgery. Tendon samples were prepared for an immunohistochemical analysis of Factor VIII. | The PRP group showed significantly higher blood flow and vessel formation than the placebo group, except at week 5. Factor VIII staining confirmed more organized vascular structures. | 24 weeks | Positive |
| Bosch et al. [49] | Experimental, placebo-controlled study of 6 clinically healthy horses. The aim was to evaluate the effect of PRP by an analysis of computerized ultrasound images and histology in surgically induced lesions in the forelimb SDFTs. | Surgically induced forelimb SDFT lesions were randomly treated with a single dose of 3 mL of autologous PRP or SS. Horses were maintained on an exercise protocol, and euthanasia was performed at 24 weeks. Limbs were scanned at 1 week after surgery, just before the PRP or placebo injection, and at 2, 3, 5, 8, 12, 18 and 24 weeks after surgery. | The PRP group showed superior healing, with an 80% collagen orientation compared to 60% for the placebo group. PRP improved fibrillogenesis and structural organization and reduced inflammation. The ultrasonographic analysis confirmed accelerated tendon repair, supporting PRP as an effective treatment. | 24 weeks | Positive |
| Figueiredo et al. [51] | Experimental, placebo-controlled study of 6 clinically healthy horses. The effect of PRP on standardized, surgically induced lesions in fore- and hindlimb SLs. The aim was to evaluate the effect of PRP using US, morphological, and morphometric analyses of the repaired tissue. | Surgically induced SL lesions were randomly treated with 2.5 mL of PRP or SS. US was performed on days 10, 30, and 60. On day 46, biopsies of scar tissue were taken for a histological analysis. | PRP-treated suspensory ligament lesions showed improved healing with improved echogenicity, increased neovascularization, and increased type I collagen levels. | 46 days | Positive |
| Maia et al. [53] | Experimental, placebo-controlled study of 6 clinically healthy horses. The aim was to evaluate the effect of PRP on collagenase-induced tendinitis by a US examination. | Tendinitis was induced in the forelimb SDFTs by a collagenase injection. PRP (2.5 mL) or saline was applied. The US evaluation was performed at 48 h and days 7, 12, 14, 21, 28, 35, and 42. | The PRP group showed a greater lesion reduction, improved echogenicity, and better collagen fiber alignment compared to controls. US assessments at multiple time points confirmed smaller lesion cross-sectional areas in the PRP group. | 42 days | Positive |
| Maia et al. [52] | Experimental, placebo-controlled study of 6 clinically healthy horses. The aim was to evaluate the effect of PRP on collagenase-induced tendinitis by a histology analysis. | Tendinitis was induced in the forelimb SDFTs by a collagenase injection. PRP (2.5 mL) or saline was applied. After 36 days, biopsy and histology assessed the fibroblast density, neovascularization, and tissue organization. | The PRP group showed a better collagen fiber alignment, higher fibroblast density, and moderate neovascularization. Histology revealed more organized tissue repair in PRP-treated tendons, although fibroblast and vessel counts were not significantly different from controls. | 36 days | Positive |
| Zandim et al. [54] | Experimental, placebo-controlled study of 6 clinically healthy horses. The aim was to evaluate the effect of PRP on collagenase-induced tendinitis by histologic and morphometric changes and immunohistochemistry of Factor VIII expression. | Tendinitis was induced in the forelimb SDFTs by a collagenase injection. PRP (1.8 mL) or saline was applied. Biopsies were taken at 3 and 16 days for histologic, morphometric, and immunohistochemical analyses. | No significant differences were found between PRP- and saline-treated tendons in collagen organization, fibroblast density, vascularization, or Factor VIII expression. PRP did not accelerate tendon healing, highlighting the need for further studies on its efficacy. | 16 days | Neutral |
| Study | Study Type, Number of Animals, and Objectives | Study Design | Results and Adverse Effects | Length of Follow-Up | Outcome |
|---|---|---|---|---|---|
| Carvalho et al. [55] | Experimental study of 8 horses. The aim was to evaluate the effects of AD-MSCs) suspended in PRP on collagenase-induced forelimb SDFT tendonitis using ultrasound, histopathology, immunohistochemistry, and gene expression analyses. | Forelimb SDFT lesions were treated with 10 × 106 AD-MSCs suspended in 1 mL autologous PRP or SS (control). US monitoring was performed every two weeks for 16 weeks, followed by biopsy and histologic and molecular analyses. | AD-MSC + PRP prevented lesion progression, improved collagen fiber organization, and reduced inflammation. US showed improved healing in treated tendons. Gene expression levels for collagen and tenogenic markers were not significantly different between groups. | 16 weeks | Positive |
| Romero et al. [56] | Experimental study of 12 horses. The aim was to compare the effects of BM-MSCs, AD-MSCs, and PRP on surgically induced SDFT lesions using ultrasound, histology, and gene expression analyses. | Lesions were treated with BM-MSCs (20 × 106 cells suspended in 7 mL of lactated Ringer’s solution (LRS)), AD-MSCs (20 × 106 cells suspended in 7 mL of LRS), PRP (7 mL), or the control (7 mL of LRS). Healing was monitored by ultrasound at 2, 6, 10, 20, and 45 weeks, followed by histopathology and a molecular analysis. | BM-MSCs showed an earlier improvement in echogenicity (week 6), while all treatments outperformed controls by week 10. PRP and AD-MSCs showed similar healing results, both improving ultrasound echogenicity and outperforming controls. Histology confirmed improved collagen fiber alignment in all treated tendons, with BM-MSCs showing superior effects compared to PRP and AT-MSCs. The gene expression analysis revealed increased levels of COL1A1, tenascin, and matrix metalloproteinases in BM-MSC-treated tendons, suggesting enhanced tissue regeneration. PRP and AT-MSCs showed a moderate upregulation of tenogenic markers, although less than BM-MSCs. | 45 weeks | Neutral |
3.2. Platelet-Rich Plasma Quality
| Characteristic (C) * | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 |
| Argüelles et al. [18] | AUT | SC, 75 mL of fresh WB | Double centrifugation tube method | 120× g/5 min, then 240× g/5 min. Room temperature | PRP collected from the buffy coat. | NR | 250 ± 71.8 × 103 PLTs/µL; TGF-β1: 1251 pg/ml | NR | Calcium chloride | 3 intralesional (IL) injections of 5–8 mL of PRP at 2-week intervals |
| Castelijns et al. [37] | AUT | ACD, 55 mL of fresh WB | Gravitational filter system | NA | E-PET set, Pall Corporation filter, NY, USA. Platelets were captured via a filter and back-flushed with harvest solution. L-PRP | 92.8 ± 3.5 × 103 PLTs/µL; 5.6 ± 1.3 ×103 WBCs/µL | 648 ± 312.6 × 103 PLTs/µL; 21.4 ± 5.2 WBCs ×103/µL. L-PRP | 6.9 ± 1.9-fold increase | NR | 2.5 mL of PRP IL; 1 injection |
| Georg et al. [38] | AUT | 15 mL of WB | Semiautomated kit. Single centrifugation | NR | ACP double syringe Arthrex, Germany. PRP was collected from the buffy coat. P-PRP | 144 × 103 PLTs/µL; 8.71 × WBCs 103/µL | 178.5 × 103/PLTs µL; 1.01 × 10 3 WBCs/µL. P-PRP | 1.3-fold increase | NR | 2–4 mL of PRP IL, with 1–2 injections |
| Waselau et al. [17] | AUT | ACD, 50 mL of WB | Semiautomated kit. Single centrifugation | 2100× g/9 min | Secquire, PPAI Medical, FL, USA. PRP was collected from the buffy coat. | 155 × 103 PLTs/µL | 1370 × 103 PLTs/µL | 8.7-fold increase | Bovine thrombin | 7–12 mL of PRP IL; 1 injection |
| Zuffova et al. [39] | AUT | CPDA, 50 mL of WB | Single centrifugation tube method | 1500 rpm/5 min | PRP was collected from the buffy coat. | 87.8 ± 18.5 × 103 PLTs/µL | 544.8 ± 244.2 × 103 PLTs/µL | 5.6-fold increase | Calcium chloride | The PRP volume was relative to the size of the lesion; 1 dose IL |
| Characteristic (C) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 |
| Beerts et al. [40] | ALL | CPDA-1, 300 mL of WB | Multiple centrifugation steps | NR | PRP was collected from the buffy coat. P-PRP | NR | 100–150 × 103 PLTs/µL, 0.1 × 103 WBCs/µL. P-PRP | NR | NR | 1 mL of PRP/allogeneic MSCs; 1 injection |
| Guercio et al. [41] | AUT | SC, 250 mL of WB | Double centrifugation | 180× g for 10 min, then 1200× g for 10 min | Platelets were collected from the buffy coat. | NR | 1000 × 103 platelets/µL | NR | NR | 5–10 mL of PRP/AD-MSCs; 1 injection IL |
| Ricco et al. [42] | AUT | CPD | Double centrifugation in 50 mL tubes. | 150× g/30 min, then 800× g/15 min at 4 °C | The platelet pellet was collected after centrifugation. | NR | 1000 × 103 PLTs/µL | NR | NR | 2–6 mL of PRP with 2 × 106 ASCs/mL |
| Torricelli et al. [43] | AUT | SC, 50 mL of WB | Double centrifugation | 200× g/5 min, then 1000× g/15 min | PRP was collected from the buffy coat. | 144 × 103 PLT/µL | 751 × 103 PLTs/µL; TGF-β1, 3055 pg/mL; PDGF-AB, 357.1 pg/mL; VEGF, 169.1 pg/mL; IGF, 289.2 pg/mL; EGF, 4.6 pg/mL; and IL-1β, 3.9 pg/mL | 5.4-fold increase | Calcium chloride | 4–7 mL of PRP/BMMNCs; 1 injection IL |
| Characteristic (C) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 |
| Garrett et al. [44] | AUT | ACD, 55 mL of WB | Semiautomated kit. Single centrifugation | 1744× g/15 min | PRP was collected from the buffy coat. GPS II Platelet Concentrate Separation Kit, Biomet Inc, IN, USA | 214 ± 113 × 103 PLTs/µL | 966 ± 189 × 103 PLTs/µL | 5.2-fold increase | Non-activated | 3 mL of PRP or saline; 1 dose IL |
| Geburek et al. [45] | AUT | ACD-A, 54 mL of WB | Semiautomated kit. Double centrifugation | 900× g/3 min, then 1470× g/10 min | PRP was collected from the buffy coat. Osteokine®, PRP preparation system, Orthogen, Düsseldorf, Germany | 157.3 ± 35.9 × 103 PLTs/µL; 7.5 ± 1.5 × 103 WBCs/µL | 892.37 ± 364.7 × 103 PLTs/µL; 14.1 ± 7.0 × 103 WBCs/µL. L-PRP | 5.67-fold increase | Non-activated | 3 mL of PRP or saline; 1 dose IL |
| Giunta et al. [46] | AUT | NR | Semiautomated kit. | NR | Arthrex ACP system, FL, USA | NR | NR | NR | NR | 3–6 mL of PRP; 1 dose IL |
| Maleas and Mageed [47] | AUT | 55 mL of WB | Gravitational filter system | NR | E-PET set, Pall Corporation filter, NY, USA. L-PRP | NR | 495 ± 364.7 × 103 PLTs/µL | NR | NR | 2–4 mL of PRP; 1 dose IL |
| Characteristic (C) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 |
| Bosch et al. [48] | AUT | SC | Semiautomated kit. Single centrifugation | NR | PRP was collected from the buffy coat. GPS II Biomet, IN, USA | NR | 639.7 ± 103.2 × 103 PLTs/µL; 42.1 ± 16.7 × 103 WBCs/µL; TGF-β, 4810.9 ± 1530.5 pg/mL; PDGF-, 5000 ± 830 pg/mL. L-PRP | 3.78-fold increase | NR | Single injection, 3 mL of PRP per tendon |
| Bosch et al. [49] | AUT | NR | Semiautomated kit. Single centrifugation | NR | PRP was collected from the buffy coat. GPS II Biomet, IN, USA | NR | NR | NR | NR | Single injection, 3 mL of PRP per tendon |
| Bosch et al. [50] | AUT | NR | Semiautomated kit. Single centrifugation | NR | PRP was collected from the buffy coat. GPS II Biomet, IN, USA | NR | 639.7 ± 103.2 × 103 PLTs/µL; 42.1 ± 16.7 × 103 WBCs/µL; TGF-β, 4810.9 ± 1530.5 pg/mL; PDGF-, 5000 ± 830 pg/mL. L-PRP | 3.78-fold increase | NR | Single injection, 3 mL of PRP per tendon |
| Figueiredo et al. [51] | AUT | NR | Double centrifugation tube method | 120× g/5 min, then 240× g/5 min | PRP was collected from the buffy coat. | NR | 300× 103 PLTs/µL; 2.0 × 103 WBCs/µL. P-PRP | NR | Non-activated | Single injection, 2.5 mL of PRP |
| Maia et al. [52] | AUT | SC, 81 mL of WB | Double centrifugation method | 120× g/5 min, then 473× g/5 min | PRP was collected from the buffy coat. | NR | 300–500 × 103 PLTs/µL | NR | Calcium chloride | Single injection, 2.5 mL of PRP per tendon |
| Maia et al. [53] | AUT | SC, 81 mL of WB | Double centrifugation method | 120× g/5 min, then 473× g/5 min. | PRP was collected from the buffy coat. | NR | 300–500 × 103 PLTs/µL | NR | Calcium chloride | Single injection, 2.5 mL of PRP per tendon |
| Zandim et al. [54] | AUT | SC | Double centrifugation method | 120× g/5 min, then 240× g/5 min | PRP was collected from the buffy coat. | 164.5 ± 9.89 ×103 PLTs/µL | 368.3 ± 39.7 ×103 PLTs/µL | NR | Non-activated | Single injection, 1.8 mL of PRP per tendon |
| Characteristic (C) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 |
| Carvalho et al. [55] | AUT | NR | Double centrifugation tube method | 120× g/5 min, then 240× g/5 min | NR | NR | 321 × 103 PLTs/µL; 2.3 × 103 WBCs/µL. P-PRP | NR | NR | Single injection, 1 mL of PRP/MSCs |
| Romero et al. [56] | AUT | SC | Double centrifugation tube method | 120× g/5 min, then 240× g/5 min | PRP was collected from the buffy coat. | NR | 263.3 ± 99.9 ×103 PLTs/µL; 8.9 ± 2.5 × 103 WBCs/µL. L-PRP | NR | Non-activated | Single injection, 7 mL of PRP per tendon |
| Characteristic (C) | Overall Score | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Type of Study | Treatment | C1 | C2 | C3 | C4 | C5 | C6 | C7 | C8 | C9 | C10 | |
| Argüelles et al. [18] | Case series | Only PRP | 10 | 10 | 10 | 10 | 10 | 0 | 7 | 0 | 10 | 10 | 77 |
| Castelijns et al. [37] | Case series | Only PRP | 10 | 10 | 10 | 10 | 10 | 10 | 7 | 10 | 0 | 10 | 87 |
| Georg et al. [38] | Case series | Only PRP | 10 | 7 | 10 | 0 | 10 | 10 | 7 | 10 | 0 | 10 | 74 |
| Waselau et al. [17] | Case series | Only PRP | 10 | 10 | 10 | 10 | 10 | 5 | 3 | 10 | 10 | 10 | 88 |
| Zuffova et al. [39] | Case series | Only PRP | 10 | 10 | 10 | 5 | 10 | 5 | 3 | 10 | 10 | 10 | 83 |
| Beerts et al. [40] | Case series | PRP/MSCs | 10 | 10 | 10 | 0 | 10 | 0 | 7 | 0 | 0 | 10 | 57 |
| Guercio et al. [41] | Case series | PRP/AD-MSCs | 10 | 10 | 10 | 7 | 10 | 0 | 3 | 0 | 0 | 10 | 60 |
| Ricco et al. [42] | Case series | PRP/AD-MSCs | 10 | 3 | 10 | 10 | 10 | 0 | 3 | 0 | 0 | 10 | 56 |
| Torricelli et al. [43] | Case series | PRP/BMMNCs | 10 | 10 | 10 | 7 | 10 | 5 | 7 | 10 | 10 | 10 | 89 |
| Garrett et al. [44] | RCT | PRP or SS | 10 | 10 | 10 | 7 | 10 | 5 | 3 | 10 | 10 | 10 | 85 |
| Geburek et al. [45] | RCT | PRP or SS | 10 | 10 | 10 | 7 | 10 | 10 | 7 | 10 | 10 | 10 | 94 |
| Giunta et al. [46] | RCT | PRP or EST | 10 | 0 | 10 | 0 | 10 | 0 | 0 | 0 | 0 | 10 | 40 |
| Maleas and Mageed [47] | RCT | PRP or BMAC | 10 | 7 | 10 | 0 | 10 | 0 | 3 | 0 | 0 | 10 | 50 |
| Bosch et al. [50] | RES | Only PRP | 10 | 3 | 10 | 0 | 10 | 0 | 10 | 10 | 0 | 10 | 63 |
| Bosch et al. [48] | RES | Only PRP | 10 | 0 | 10 | 0 | 10 | 0 | 0 | 0 | 0 | 10 | 40 |
| Bosch et al. [49] | RES | Only PRP | 10 | 0 | 10 | 0 | 10 | 0 | 10 | 10 | 0 | 10 | 60 |
| Figueiredo et al. [51] | RES | Only PRP | 10 | 0 | 10 | 7 | 10 | 0 | 7 | 0 | 10 | 10 | 64 |
| Maia et al. [53] | RES | Only PRP | 10 | 10 | 10 | 7 | 10 | 0 | 3 | 0 | 10 | 10 | 70 |
| Maia et al. [52] | RES | Only PRP | 10 | 10 | 10 | 7 | 10 | 0 | 3 | 0 | 10 | 10 | 70 |
| Zandim et al. [54] | RES | Only PRP | 10 | 3 | 10 | 7 | 10 | 5 | 3 | 0 | 10 | 10 | 68 |
| Carvalho et al. [55] | RES | PRP/MSCs | 10 | 0 | 10 | 7 | 10 | 0 | 7 | 0 | 0 | 10 | 54 |
| Romero et al. [56] | RES | PRP/MSCs | 10 | 3 | 10 | 7 | 10 | 0 | 7 | 0 | 10 | 10 | 67 |
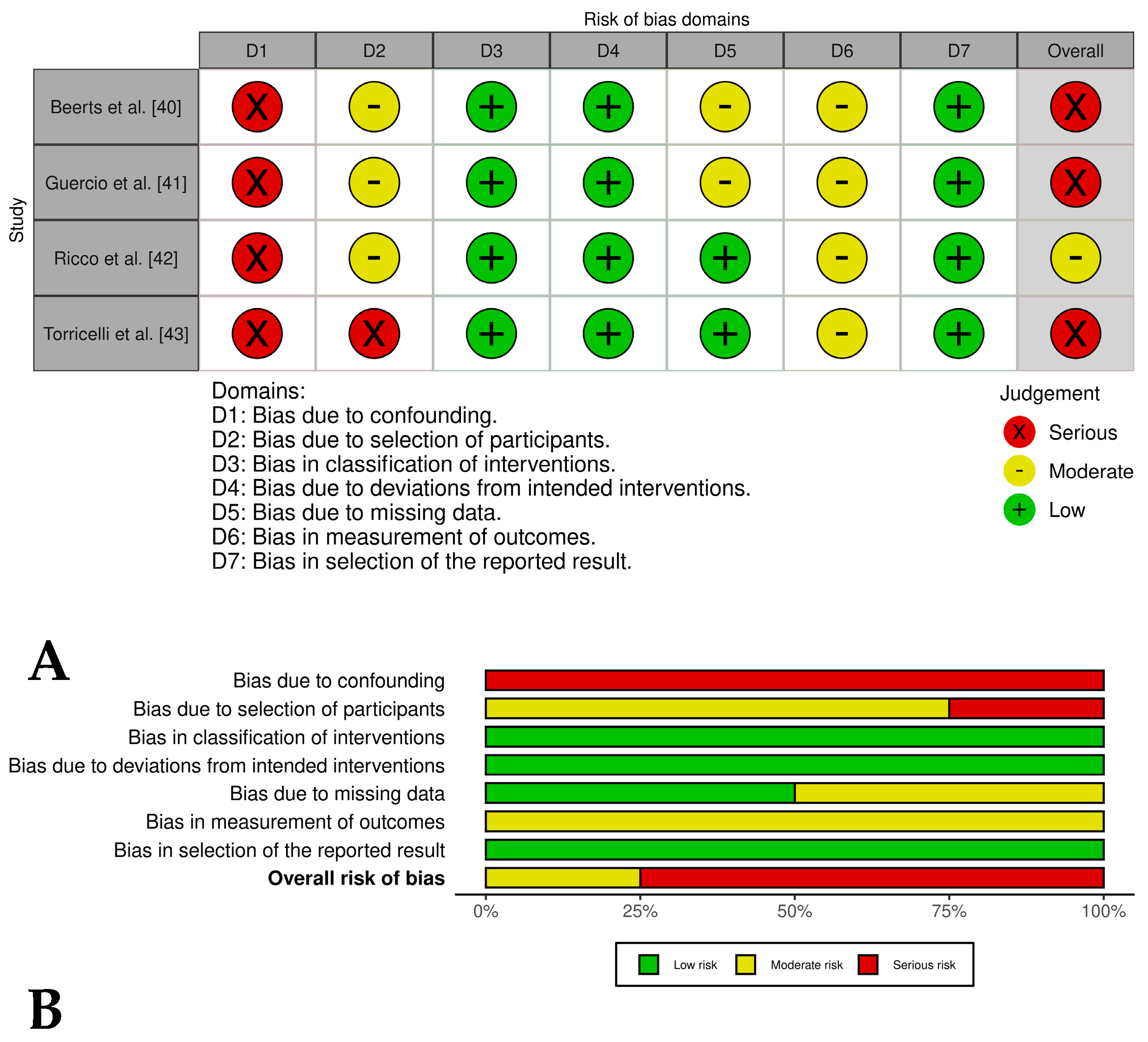
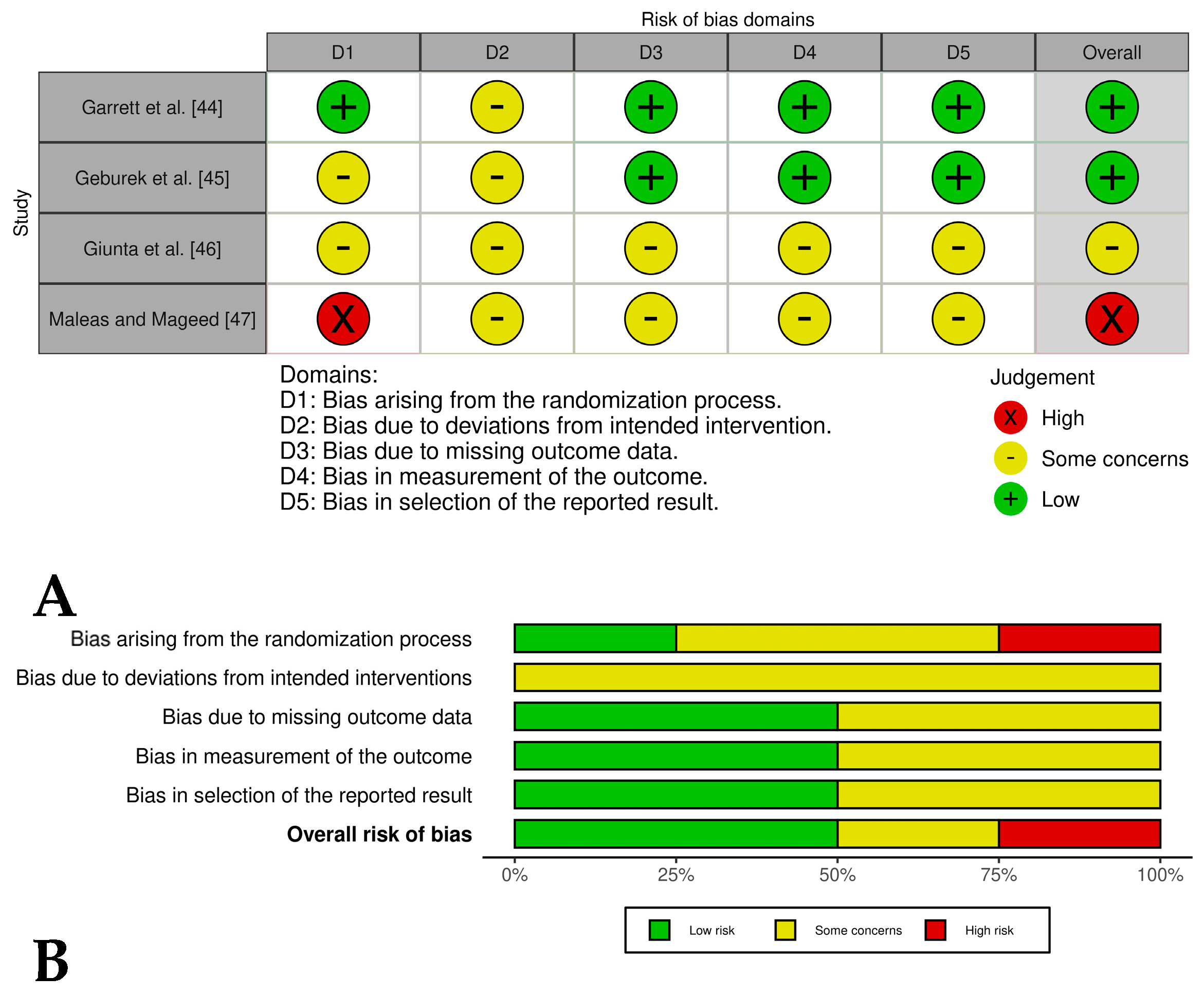
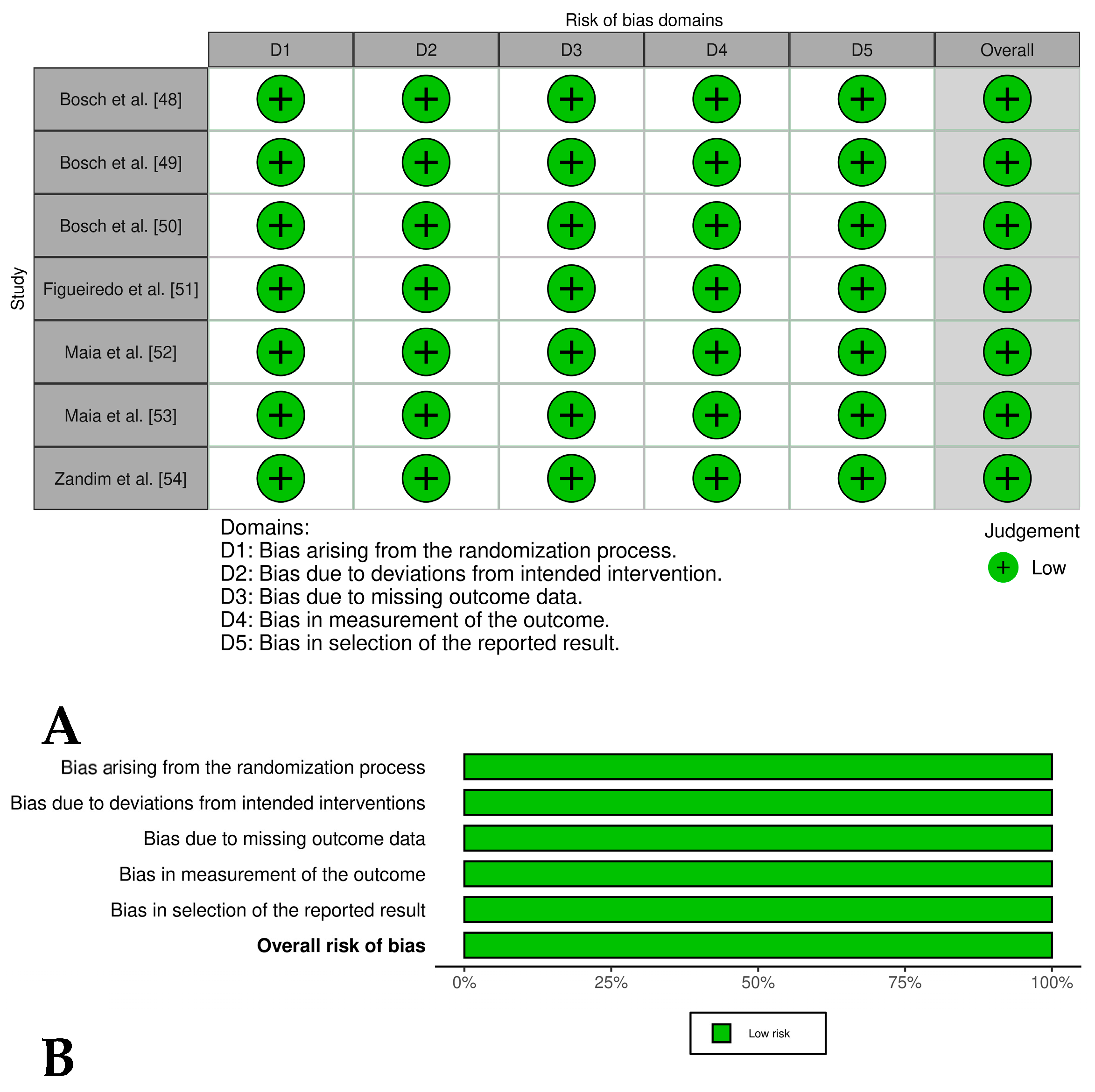
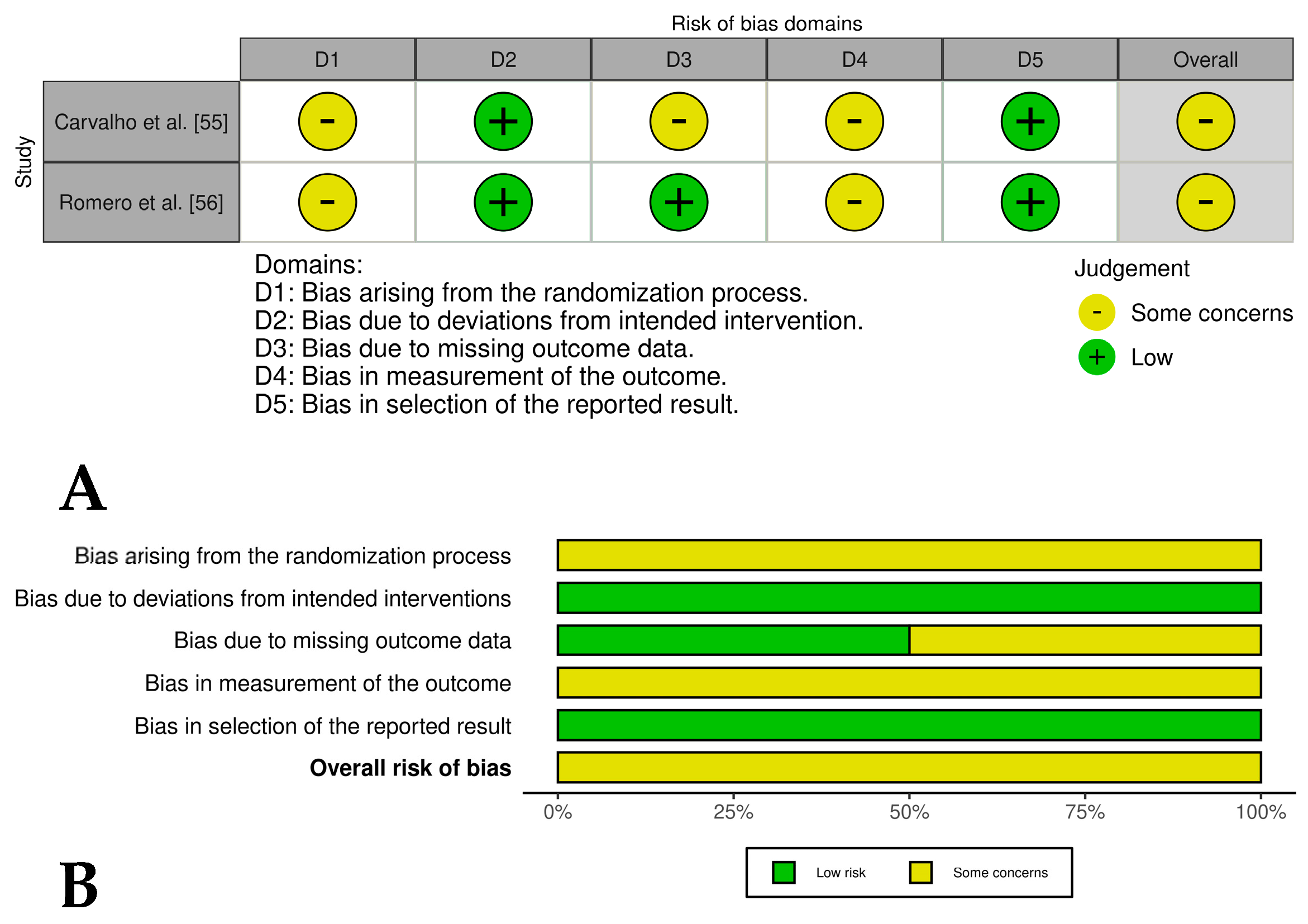
3.3. Bias Risk Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACD | Acid citrate dextrose |
| ACP | Autologous conditioned plasma |
| AD-MSCs | Adipose-derived mesenchymal stem cells |
| ALL | Allogeneic |
| AUT | Autologous |
| BMMNCs | Bone marrow mononuclear cells |
| CDUS | Color Doppler ultrasound |
| COL1A1 | Collagen type I alpha 1 chain |
| CPDA | Citrate phosphate dextrose adenine |
| DDFT | Deep digital flexor tendon |
| EGF | Epidermal growth factor |
| EST | Extracorporeal shockwave therapy |
| GFs | Growth factors |
| GAG | Glycosaminoglycan |
| HGF | Hepatocyte growth factor |
| IFN-γ | Interferon gamma |
| IGFs | Insulin-like growth factors |
| IL-1β | Interleukin-1 beta |
| IL-4 | Interleukin-4 |
| IL-10 | Interleukin-10 |
| IL | Intralesional |
| L-PRP | Leukocyte and platelet-rich plasma |
| MMPs | Matrix metalloproteinases |
| MSD | Midbody suspensory ligament desmitis |
| NF-κB | Nuclear factor kappa B |
| PDGFs | Platelet-derived growth factors |
| PICO | Population, intervention, comparison, outcome |
| PLT | Platelet |
| PRG | Platelet-rich gel |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PRP | Platelet-rich plasma |
| P-PRP | Pure platelet-rich plasma |
| PSLD | Proximal suspensory ligament desmitis |
| ROBINS-I | Risk of bias in non-randomized studies of interventions |
| RoB2.0 | Risk of bias 2 (tool for randomized trials) |
| ROVIS | Risk-of-bias VISualization tool |
| SC | sodium citrate |
| SDFT | Superficial digital flexor tendon |
| SDFTT | Superficial digital flexor tendon tendinopathy |
| SL | Suspensory ligament |
| SLBD | Suspensory ligament branch desmitis |
| SLD | Suspensory ligament desmitis |
| TGF-β1 | Transforming growth factor beta 1 |
| TNF-α | Tumor necrosis factor alpha |
| US | Ultrasound |
| VEGF | Vascular endothelial growth factor |
| WB | Whole blood |
| WBC | White blood cell |
References
- Dakin, S.G.; Dudhia, J.; Smith, R.K. Resolving an inflammatory concept: The importance of inflammation and resolution in tendinopathy. Veter-Immunol. Immunopathol. 2014, 158, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Dakin, S.G.; Dudhia, J.; Smith, R.K.W. Science in brief: Resolving tendon inflammation. A new perspective. Equine Veter. J. 2013, 45, 398–400. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.K.W.; McIlwraith, C.W. “One Health” in tendinopathy research: Current concepts. J. Orthop. Res. 2021, 39, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Clegg, P.D. Musculoskeletal disease and injury, now and in the future. Part 2: Tendon and ligament injuries. Equine Veter. J. 2012, 44, 371–375. [Google Scholar] [CrossRef]
- Kasashima, Y.; Takahashi, T.; Smith, R.K.W.; Goodship, A.E.; Kuwano, A.; Ueno, T.; Hirano, S. Prevalence of superficial digital flexor tendonitis and suspensory desmitis in Japanese Thoroughbred flat racehorses in 1999. Equine Veter. J. 2004, 36, 346–350. [Google Scholar] [CrossRef]
- USDA. National Economic Cost of Equine Lameness, Colic, and Equine Protozoal Myeloencephalitis in the United States; USDA APHIS Centers of Epidemiology and Animal Health: Fort Collins, CO, USA, 2001.
- Fraile, A.P.; González-Cubero, E.; Martínez-Flórez, S.; Olivera, E.R.; Villar-Suárez, V. Regenerative Medicine Applied to Musculoskeletal Diseases in Equines: A Systematic Review. Veter. Sci. 2023, 10, 666. [Google Scholar] [CrossRef]
- O’brien, C.; Marr, N.; Thorpe, C. Microdamage in the equine superficial digital flexor tendon. Equine Veter. J. 2021, 53, 417–430. [Google Scholar] [CrossRef]
- Hosaka, Y.; Kirisawa, R.; Yamamoto, E.; Ueda, H.; Iwai, H.; Takehana, K. Localization of cytokines in tendinocytes of the superficial digital flexor tendon in the horse. J. Veter. Med. Sci. 2002, 64, 945–947. [Google Scholar] [CrossRef]
- Reis, I.L.; Lopes, B.; Sousa, P.; Sousa, A.C.; Caseiro, A.R.; Mendonça, C.M.; Santos, J.M.; Atayde, L.M.; Alvites, R.D.; Maurício, A.C. Equine Musculoskeletal Pathologies: Clinical Approaches and Therapeutical Perspectives—A Review. Veter. Sci. 2024, 11, 190. [Google Scholar] [CrossRef]
- Sharma, P.; Maffulli, N. Tendon injury and tendinopathy: Healing and repair. J. Bone Jt. Surg. Am. 2005, 87, 187–202. [Google Scholar]
- M’cloud, W.R.C.; Guzmán, K.E.; Panek, C.L.; Colbath, A.C. Stem cells and platelet-rich plasma for the treatment of naturally occurring equine tendon and ligament injuries: A systematic review and meta-analysis. J. Am. Veter. Med. Assoc. 2024, 262, S50–S60. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Yang, L.; Labens, R.; Gao, Y.; Zhu, Y.; Li, J. A systematic review and meta-analysis of the efficacy of platelet-rich plasma products for treatment of equine joint disease. Equine Veter. J. 2024, 56, 858–869. [Google Scholar] [CrossRef]
- Garbin, L.C.; Lopez, C.; Carmona, J.U. A Critical Overview of the Use of Platelet-Rich Plasma in Equine Medicine Over the Last Decade. Front. Veter. Sci. 2021, 8, 641818. [Google Scholar] [CrossRef]
- Castillo-Franz, C.; López, C.; Carmona, J. Evaluation of the Catabolic and Anabolic Gene Expression Effects and Histology Changes induced by Platelet-Rich Gel Supernatants in Equine Suspensory Ligament Explants Challenged with Lipopolysaccharide. MLTJ-Muscle Ligaments Tendons J. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Castillo-Franz, C.; López, C.; Álvarez, M.E.; Giraldo, C.E.; Carmona, J.U. Anti-inflammatory effects of two platelet-rich gel supernatants in an in vitro system of ligament desmitis. Muscles Ligaments Tendons J. (MLTJ) 2019, 9, 506–516. [Google Scholar] [CrossRef]
- Waselau, M.; Sutter, W.W.; Genovese, R.L.; Bertone, A.L. Intralesional injection of platelet-rich plasma followed by controlled exercise for treatment of midbody suspensory ligament desmitis in Standardbred racehorses. J. Am. Veter. Med. Assoc. 2008, 232, 1515–1520. [Google Scholar] [CrossRef]
- Argüelles, D.; Carmona, J.U.; Climent, F.; Muñoz, E.; Prades, M. Autologous platelet concentrates as a treatment for musculoskeletal lesions in five horses. Veter. Rec. 2008, 162, 208–211. [Google Scholar] [CrossRef]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Andia, I.; Zumstein, M.A.; Zhang, C.-Q.; Pinto, N.R.; Bielecki, T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: Current consensus, clinical implications and perspectives. Muscles Ligaments Tendons J. 2014, 4, 3–9. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.M.d.C.; Pimenta, C.A.d.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Latino-Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Harrison, P.; Alsousou, J. Studies on platelet rich plasma—New editorial policy for “Platelets”. Platelets 2020, 31, 281–282. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Romagnoli, N.; Rinnovati, R.; Ricciardi, G.; Lambertini, C.; Spinella, G.; Spadari, A. Clinical Evaluation of Intralesional Injection of Platelet-Rich Plasma for the Treatment of Proximal Suspensory Ligament Desmitis in Horses. J. Equine Veter. Sci. 2015, 35, 141–146. [Google Scholar] [CrossRef]
- Scala, M.; Lenarduzzi, S.; Spagnolo, F.; Trapasso, M.; Ottonello, C.; Muraglia, A.; Barla, A.; Squillario, M.; Strada, P. Regenerative Medicine for the Treatment of Teno-desmic Injuries of the Equine. A Series of 150 Horses Treated with Platelet-derived Growth Factors. In Vivo 2014, 28, 1119–1123. [Google Scholar] [PubMed]
- Künneke, A.; Jaugstetter, H.; Heyers, P. Bone marrow—Autologous conditioned plasma (BM-ACP) in equine medicine—First clinical experience of a new, autologous therapy in the treatment of tendon diseases in horses. Pferdeheilkunde 2008, 24, 519–523. [Google Scholar] [CrossRef]
- Witte, S.; Dedman, C.; Harriss, F.; Kelly, G.; Chang, Y.-M.; Witte, T. Comparison of treatment outcomes for superficial digital flexor tendonitis in National Hunt racehorses. Veter. J. 2016, 216, 157–163. [Google Scholar] [CrossRef]
- Marycz, K.; Toker, N.Y.; Grzesiak, J.; Wrzeszcz, K.; Golonka, P. The therapeutic effect of autogenic adipose derived stem cells combined with autogenic platelet rich plasma in tendons disorders hi horses in vitro and in vivo research. J. Anim. Vet. Adv. 2012, 11, 4324–4331. [Google Scholar]
- Castelijns, G.; Crawford, A.; Schaffer, J.; Ortolano, G.A.; Beauregard, T.; Smith, R.K.W. Evaluation of a filter-prepared platelet concentrate for the treatment of suspensory branch injuries in horses. Veter. Comp. Orthop. Traumatol. 2011, 24, 363–369. [Google Scholar] [CrossRef]
- Georg, R.; Maria, C.; Gisela, A.; Bianca, C. Autologous conditioned plasma as therapy of tendon and ligament lesions in seven horses. J. Veter. Sci. 2010, 11, 173–175. [Google Scholar] [CrossRef]
- Zuffova, K.; Krisova, S.; Zert, Z. Platelet rich plasma treatment of superficial digital flexor tendon lesions in racing Thoroughbreds. Veter. Med. 2013, 58, 230–239. [Google Scholar] [CrossRef]
- Beerts, C.; Suls, M.; Broeckx, S.Y.; Seys, B.; Vandenberghe, A.; Declercq, J.; Duchateau, L.; Vidal, M.A.; Spaas, J.H. Tenogenically Induced Allogeneic Peripheral Blood Mesenchymal Stem Cells in Allogeneic Platelet-Rich Plasma: 2-Year Follow-up after Tendon or Ligament Treatment in Horses. Front. Veter. Sci. 2017, 4, 158. [Google Scholar] [CrossRef]
- Guercio, A.; Di Marco, P.; Casella, S.; Russotto, L.; Puglisi, F.; Majolino, C.; Giudice, E.; Di Bella, S.; Purpari, G.; Cannella, V.; et al. Mesenchymal Stem Cells Derived From Subcutaneous Fat and Platelet-Rich Plasma Used in Athletic Horses With Lameness of the Superficial Digital Flexor Tendon. J. Equine Veter. Sci. 2015, 35, 19–26. [Google Scholar] [CrossRef]
- Ricco’, S.; Renzi, S.; Del Bue, M.; Conti, V.; Merli, E.; Ramoni, R.; Lucarelli, E.; Gnudi, G.; Ferrari, M.; Grolli, S. Allogeneic adipose tissue-derived mesenchymal stem cells in combination with platelet rich plasma are safe and effective in the therapy of superficial digital flexor tendonitis in the horse. Int. J. Immunopathol. Pharmacol. 2013, 26, 61–68. [Google Scholar] [CrossRef]
- Torricelli, P.; Fini, M.; Filardo, G.; Tschon, M.; Pischedda, M.; Pacorini, A.; Kon, E.; Giardino, R. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. Int. Orthop. 2011, 35, 1569–1576. [Google Scholar] [CrossRef]
- Garrett, K.S.; Bramlage, L.R.; Spike-Pierce, D.L.; Cohen, N.D. Injection of platelet- and leukocyte-rich plasma at the junction of the proximal sesamoid bone and the suspensory ligament branch for treatment of yearling Thoroughbreds with proximal sesamoid bone inflammation and associated suspensory ligament branch desmitis. J. Am. Veter. Med. Assoc. 2013, 243, 120–125. [Google Scholar] [CrossRef]
- Geburek, F.; Gaus, M.; van Schie, H.T.M.; Rohn, K.; Stadler, P.M. Effect of intralesional platelet-rich plasma (PRP) treatment on clinical and ultrasonographic parameters in equine naturally occurring superficial digital flexor tendinopathies—A randomized prospective controlled clinical trial. BMC Veter. Res. 2016, 12, 191. [Google Scholar] [CrossRef]
- Giunta, K.; Donnell, J.R.; Donnell, A.D.; Frisbie, D.D. Prospective randomized comparison of platelet rich plasma to extracorporeal shockwave therapy for treatment of proximal suspensory pain in western performance horses. Res. Veter. Sci. 2019, 126, 38–44. [Google Scholar] [CrossRef]
- Maleas, G.; Mageed, M. Effectiveness of Platelet-Rich Plasma and Bone Marrow Aspirate Concentrate as Treatments for Chronic Hindlimb Proximal Suspensory Desmopathy. Front. Veter. Sci. 2021, 8, 678453. [Google Scholar] [CrossRef]
- Bosch, G.; Moleman, M.; Barneveld, A.; van Weeren, P.R.; van Schie, H.T.M. The effect of platelet-rich plasma on the neovascularization of surgically created equine superficial digital flexor tendon lesions. Scand. J. Med. Sci. Sports 2011, 21, 554–561. [Google Scholar] [CrossRef]
- Bosch, G.; van Weeren, P.R.; Barneveld, A.; van Schie, H.T. Computerised analysis of standardised ultrasonographic images to monitor the repair of surgically created core lesions in equine superficial digital flexor tendons following treatment with intratendinous platelet rich plasma or placebo. Veter. J. 2009, 187, 92–98. [Google Scholar] [CrossRef]
- Bosch, G.; van Schie, H.T.M.; de Groot, M.W.; Cadby, J.A.; van de Lest, C.H.A.; Barneveld, A.; van Weeren, P.R. Effects of platelet-rich plasma on the quality of repair of mechanically induced core lesions in equine superficial digital flexor tendons: A placebo-controlled experimental study. J. Orthop. Res. 2010, 28, 211–217. [Google Scholar] [CrossRef]
- Figueiredo, M.A.F.; Alves, G.E.S.; Michel, A.F.R.M.; Lima, A.E.; Wenceslau, A.A.; Ferreira, M.L.; Clark, R.M.O.; Ayres, M.C.C. Effect of platelet rich plasma therapy in the repair of experimental lesions of the suspensory ligament in horses. Rev. Bras. Med. Vet. 2016, 38, 85–92. [Google Scholar]
- Maia, L.; de Souza, M.V.; Júnior, J.I.R.; de Oliveira, A.C.; Alves, G.E.S.; Benjamin, L.d.A.; Silva, Y.F.R.S.; Zandim, B.M.; Moreira, J.D.C.L. Platelet-Rich Plasma in the Treatment of Induced Tendinopathy in Horses: Histologic Evaluation. J. Equine Veter. Sci. 2009, 29, 618–626. [Google Scholar] [CrossRef]
- Maia, L.; Souza, M.V.D.; Alves, G.E.; Júnior, J.I.; Oliveira, A.C.D.; Zandim, B.M.; da Silva, Y.F. Platelet-rich plasma in the treatment of induced tendinitis in equines: Ultrasonographic evaluation. Pesqui. Vet. Bras. 2009, 29, 241–245. [Google Scholar] [CrossRef]
- Zandim, B.M.; De Souza, M.V.; Frassy, L.N.; Vilória, M.I.V.; Maia, L.; Fonseca, C.C.; Valente, F.L.; Moreira, J.d.C.L.; Magalhães, P.C. Immunohistochemistry of factor VIII, histology and morphometry in equine tendon treated with platelet-rich plasma. Rev. Bras. Med. Vet. 2013, 35, 169–184. [Google Scholar]
- Carvalho, A.d.M.; Badial, P.R.; Álvarez, L.E.C.; Yamada, A.L.M.; Borges, A.S.; Deffune, E.; Hussni, C.A.; Alves, A.L.G. Equine tendonitis therapy using mesenchymal stem cells and platelet concentrates: A randomized controlled trial. Stem Cell Res. Ther. 2013, 4, 85. [Google Scholar] [CrossRef]
- Romero, A.; Barrachina, L.; Ranera, B.; Remacha, A.; Moreno, B.; de Blas, I.; Sanz, A.; Vázquez, F.; Vitoria, A.; Junquera, C.; et al. Comparison of autologous bone marrow and adipose tissue derived mesenchymal stem cells, and platelet rich plasma, for treating surgically induced lesions of the equine superficial digital flexor tendon. Veter. J. 2017, 224, 76–84. [Google Scholar] [CrossRef]
- McCarrel, T.M.; Minas, T.; Fortier, L.A. Optimization of leukocyte concentration in platelet-rich plasma for the treatment of tendinopathy. J. Bone Jt. Surg. 2012, 94, e143. [Google Scholar] [CrossRef]
- Giraldo, C.E.; Álvarez, M.E.; Carmona, J.U. Influence of calcium salts and bovine thrombin on growth factor release from equine platelet-rich gel supernatants. Veter. Comp. Orthop. Traumatol. 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Textor, J.A.; Tablin, F. Intra-articular use of a platelet-rich product in normal horses: Clinical signs and cytologic responses. Veter. Surg. 2013, 42, 499–510. [Google Scholar] [CrossRef]
- Textor, J.A.; Tablin, F. Activation of equine platelet-rich plasma: Comparison of methods and characterization of equine autologous thrombin. Veter. Surg. 2012, 41, 784–794. [Google Scholar] [CrossRef]
- Tsiapalis, D.; O’driscoll, L. Mesenchymal Stem Cell Derived Extracellular Vesicles for Tissue Engineering and Regenerative Medicine Applications. Cells 2020, 9, 991. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, H.-S. Extracellular Vesicles in Regenerative Medicine: Potentials and Challenges. Tissue Eng. Regen. Med. 2021, 18, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Burnouf, T.; Chou, M.-L.; Lundy, D.J.; Chuang, E.-Y.; Tseng, C.-L.; Goubran, H. Expanding applications of allogeneic platelets, platelet lysates, and platelet extracellular vesicles in cell therapy, regenerative medicine, and targeted drug delivery. J. Biomed. Sci. 2023, 30, 79. [Google Scholar] [CrossRef] [PubMed]
- Nazaroff, J.; Oyadomari, S.; Brown, N.; Wang, D. Reporting in clinical studies on platelet-rich plasma therapy among all medical specialties: A systematic review of Level I and II studies. PLoS ONE 2021, 16, e0250007. [Google Scholar] [CrossRef]
- Chahla, J.; Cinque, M.E.; Piuzzi, N.S.; Mannava, S.; Geeslin, A.G.; Murray, I.R.; Dornan, G.J.; Muschler, G.F.; LaPrade, R.F. A Call for Standardization in Platelet-Rich Plasma Preparation Protocols and Composition Reporting: A Systematic Review of the Clinical Orthopaedic Literature. J. Bone Jt. Surg. Am. 2017, 99, 1769–1779. [Google Scholar] [CrossRef]
- Murray, I.R.; Geeslin, A.G.; Goudie, E.B.; Petrigliano, F.A.; LaPrade, R.F. Minimum Information for Studies Evaluating Biologics in Orthopaedics (MIBO): Platelet-Rich Plasma and Mesenchymal Stem Cells. J. Bone Jt. Surg. 2017, 99, 809–819. [Google Scholar] [CrossRef]
- Paul, J.; Barari, M. Meta-analysis and traditional systematic literature reviews—What, why, when, where, and how? Psychol. Mark. 2022, 39, 1099–1115. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carmona, J.U.; López, C. Efficacy of Platelet-Rich Plasma in the Treatment of Equine Tendon and Ligament Injuries: A Systematic Review of Clinical and Experimental Studies. Vet. Sci. 2025, 12, 382. https://doi.org/10.3390/vetsci12040382
Carmona JU, López C. Efficacy of Platelet-Rich Plasma in the Treatment of Equine Tendon and Ligament Injuries: A Systematic Review of Clinical and Experimental Studies. Veterinary Sciences. 2025; 12(4):382. https://doi.org/10.3390/vetsci12040382
Chicago/Turabian StyleCarmona, Jorge U., and Catalina López. 2025. "Efficacy of Platelet-Rich Plasma in the Treatment of Equine Tendon and Ligament Injuries: A Systematic Review of Clinical and Experimental Studies" Veterinary Sciences 12, no. 4: 382. https://doi.org/10.3390/vetsci12040382
APA StyleCarmona, J. U., & López, C. (2025). Efficacy of Platelet-Rich Plasma in the Treatment of Equine Tendon and Ligament Injuries: A Systematic Review of Clinical and Experimental Studies. Veterinary Sciences, 12(4), 382. https://doi.org/10.3390/vetsci12040382