

Parameter Optimization, Morphological and Histological Characteristics of Accurate Bone Ablation by Femtosecond Laser: An In Vitro Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation of Sheep Tibiae Specimens
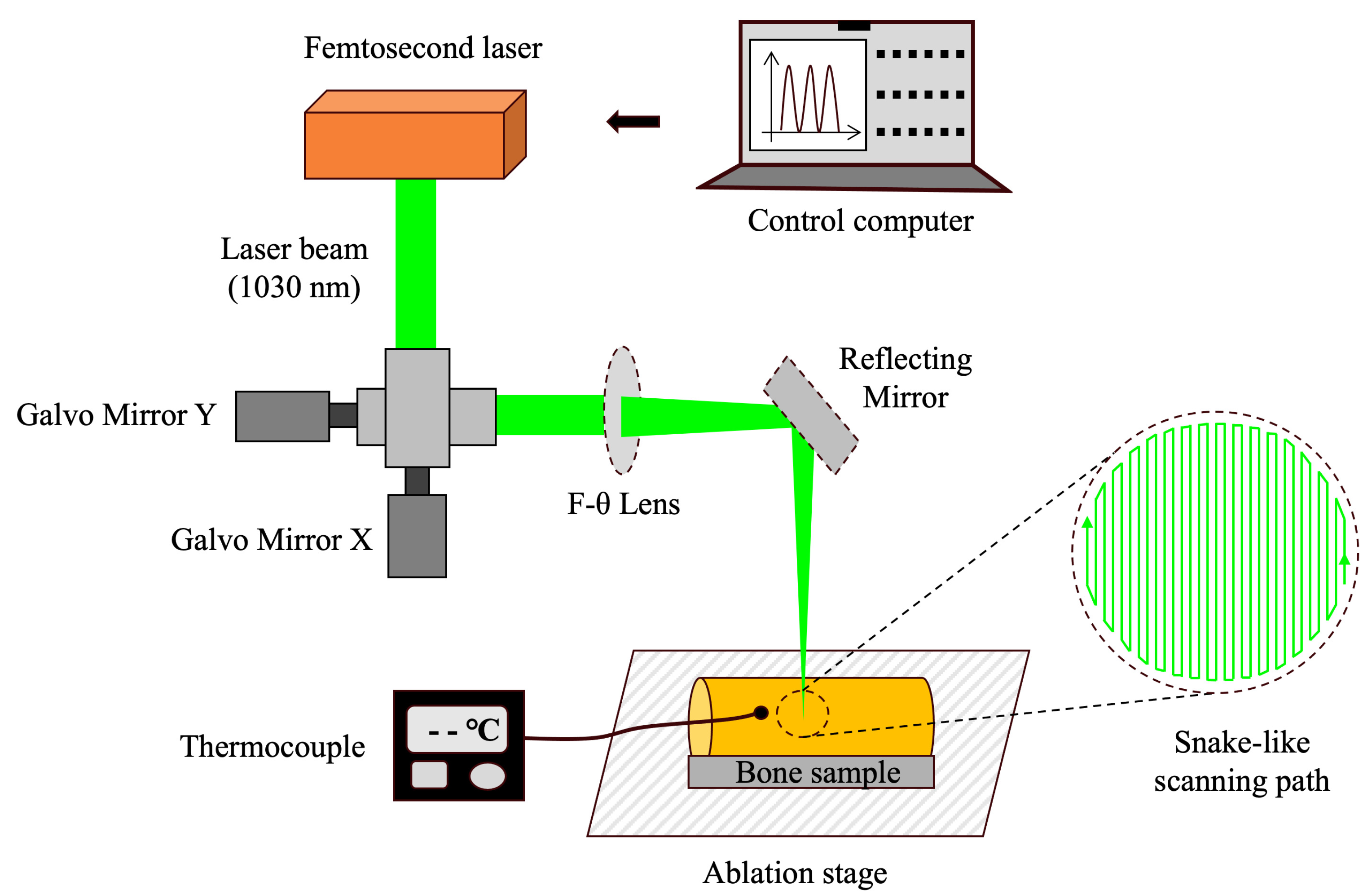
2.2. Cavity Preparation by Femtosecond Laser and Temperature Monitoring
2.3. Comparison of Ablation Efficiency and Surface Roughness Among Four Laser Sets
2.4. Comparison of Morphology and Elemental Composition Among Four Laser Sets
2.5. Morphological Comparison Between Laser and Bur Group
2.6. Histological Comparison Between Laser and Bur Group
2.7. Statistical Analysis
3. Results
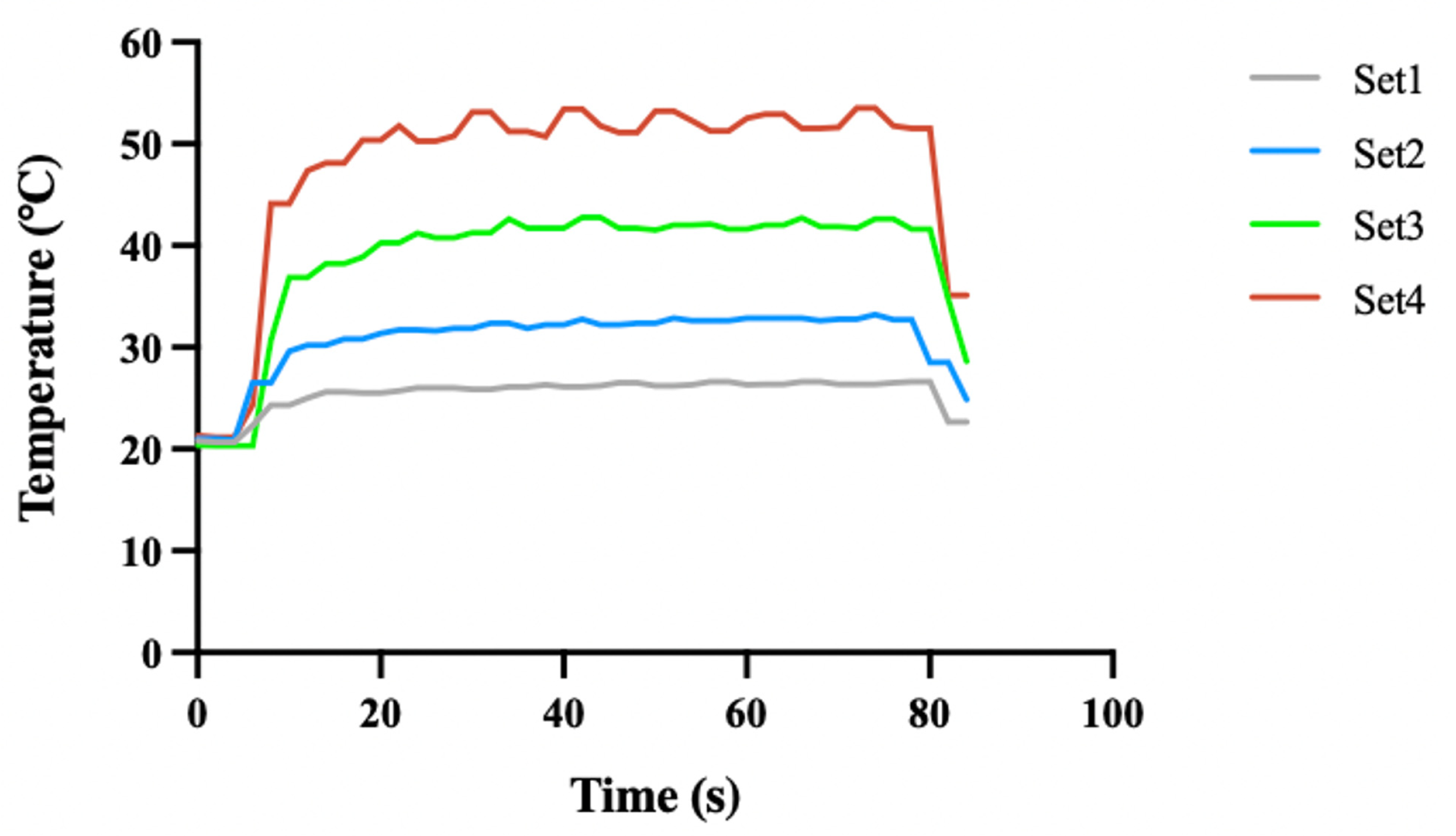
3.1. The Temperature Changes of Bone Surface During Laser Ablation
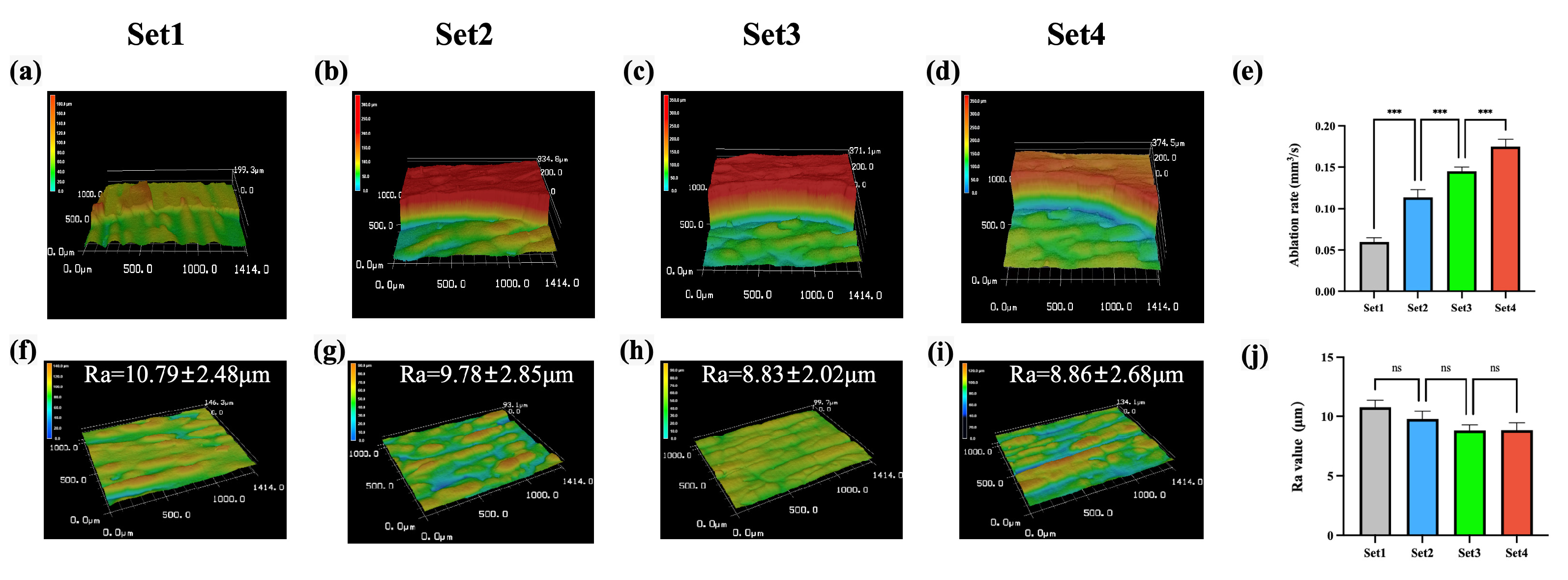
3.2. Comparison of Ablation Efficiency and Surface Roughness Among Four Laser Sets
3.3. Comparison of Morphology and Elemental Composition Among Four Laser Sets
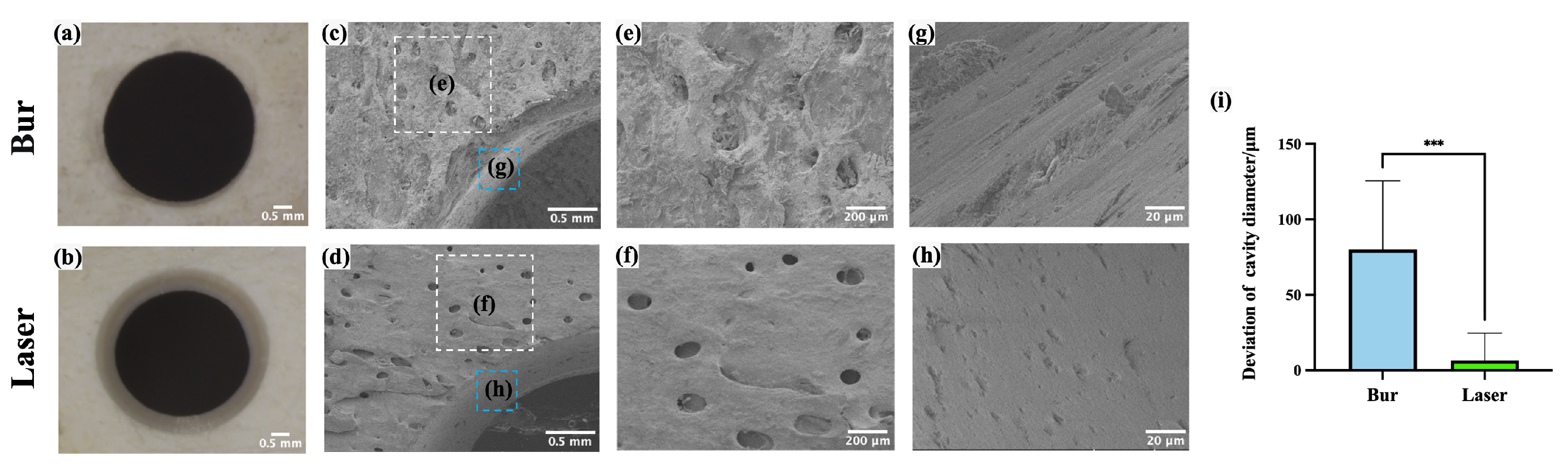
3.4. Morphological Comparison Between Laser and Bur Group
3.5. Histological Comparison Between Laser and Bur Group
4. Discussion
5. Conclusions
- The optimized femtosecond laser energy density in this study met the requirements of safety, efficiency, and accuracy for clinical applications.
- The robot-controlled femtosecond laser system enabled automatic, safe, accurate, efficient, and clean ablation of bone tissue, demonstrating significant potential for clinical applications in bone surgery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krawczyk, A.; Kuropka, P.; Kuryszko, J.; Wall, A.; Dragan, S.; Kulej, M. Experimental studies on the effect of osteotomy technique on the bone regeneration in distraction osteogenesis. Bone 2007, 40, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Nooh, N.; Abdullah, W.A.; Grawish, M.E.-A.; Ramalingam, S.; Hassan, G.; Javed, F.; Al-Hezaimi, K. Evaluation of bone regenerative capacity following distraction osteogenesis of goat mandibles using two different bone cutting techniques. J. Cranio-Maxillofac. Surg. 2014, 42, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Akhbar, M.F.A.; Yusoff, A.R. Multi—objective optimization of surgical drill bit to minimize thermal damage in bone-drilling. Appl. Therm. Eng. 2019, 157, 113594. [Google Scholar] [CrossRef]
- Akhbar, M.F.A. Thermomechanical damage in cortical bone caused by margins of surgical drill bit: A finite element analysis. Comput. Methods Programs Biomed. 2023, 231, 107361. [Google Scholar] [CrossRef]
- Baek, K.; Deibel, W.; Marinov, D.; Griessen, M.; Dard, M.; Bruno, A.; Zeilhofer, H.; Cattin, P.; Juergens, P. A comparative investigation of bone surface after cutting with mechanical tools and Er:YAG laser. Lasers Surg. Med. 2015, 47, 426–432. [Google Scholar] [CrossRef]
- Esteves, J.C.; Marcantonio, E., Jr.; de Souza Faloni, A.P.; Rocha, F.R.; Marcantonio, R.A.; Wilk, K.; Intini, G. Dynamics of bone healing after osteotomy with piezosurgery or conventional drilling—Histomorphometrical, immunohistochemical, and molecular analysis. J. Transl. Med. 2013, 11, 221. [Google Scholar] [CrossRef]
- Ueki, K.; Nakagawa, K.; Marukawa, K.; Yamamoto, E. Le Fort I osteotomy using an ultrasonic bone curette to fracture the pterygoid plates. J. Cranio-Maxillofac. Surg. 2004, 32, 381–386. [Google Scholar] [CrossRef]
- Martini, M.; Röhrig, A.; Reich, R.H.; Messing-Jünger, M. Comparison between piezosurgery and conventional osteotomy in cranioplasty with fronto-orbital advancement. J. Cranio-Maxillofac. Surg. 2017, 45, 395–400. [Google Scholar] [CrossRef]
- Pavlíková, G.; Foltán, R.; Burian, M.; Horká, E.; Adámek, S.; Hejčl, A.; Hanzelka, T.; Šedý, J. Piezosurgery prevents brain tissue damage: An experimental study on a new rat model. Int. J. Oral Maxillofac. Surg. 2011, 40, 840–844. [Google Scholar] [CrossRef]
- McGuire, C.M.; Boudreau, C.M.; Prabhu, N.B.; Hong, P.F.; Bezuhly, M.F. Piezosurgery versus Conventional Cutting Techniques in Craniofacial Surgery: A Systematic Review and Meta-Analysis. Plast. Reconstr. Surg. 2022, 149, 183–195. [Google Scholar] [CrossRef]
- Spinelli, G.; Lazzeri, D.; Conti, M.; Agostini, T.; Mannelli, G. Comparison of piezosurgery and traditional saw in bimaxillary orthognathic surgery. J. Cranio-Maxillofac. Surg. 2014, 42, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Goldman, L.; Hornby, P.; Meyer, R.; Goldman, B. Impact of the Laser on Dental Caries. Nature 1964, 203, 417. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, H.; Bernal, L.M.B.; Hamidi, A.; Droneau, A.; Canbaz, F.; Guzman, R.; Jacques, S.L.; Cattin, P.C.; Zam, A. Combined Nd:YAG and Er:YAG lasers for real-time closed-loop tissue-specific laser osteotomy. Biomed. Opt. Express 2020, 11, 1790–1807. [Google Scholar] [CrossRef] [PubMed]
- Ha, T.T.; Thieringer, F.M.; Bammerlin, M.; Cordier, D. High Precision Bone Cutting by Er: YAG Lasers Might Minimize the Invasiveness of Navigated Brain Biopsies. Front. Oncol. 2021, 11, 690374. [Google Scholar] [CrossRef] [PubMed]
- Fried, N.M.; Fried, D. Comparison of Er:YAG and 9.6-?m TE CO2 lasers for ablation of skull tissue. Lasers Surg. Med. 2001, 28, 335–343. [Google Scholar] [CrossRef]
- Strakas, D.; Gutknecht, N. Erbium lasers in operative dentistry—A literature review. Lasers Dent. Sci. 2018, 2, 125–136. [Google Scholar] [CrossRef]
- Kesler, G.; Shvero, D.K.; Tov, Y.S.; Romanos, G. Platelet Derived Growth Factor Secretion and Bone Healing After Er:YAG Laser Bone Irradiation. J. Oral Implant. 2011, 37, 195–204. [Google Scholar] [CrossRef]
- Wieger, V.; Zoppel, S.; Wintner, E. Ultrashort pulse laser osteotomy. Laser Phys. 2007, 17, 438–442. [Google Scholar] [CrossRef]
- Canteli, D.; Muñoz-García, C.; Morales, M.; Márquez, A.; Lauzurica, S.; Arregui, J.; Lazkoz, A.; Molpeceres, C. Thermal Effects in the Ablation of Bovine Cortical Bone with Pulsed Laser Sources. Materials 2019, 12, 2916. [Google Scholar] [CrossRef]
- Banerjee, S.; Pantawane, M.V.; Dahotre, N.B. Ex-vivo parametric study of laser ablation-based drilling of cortical bone. Lasers Med. Sci. 2024, 39, 157. [Google Scholar] [CrossRef]
- Zezell, D.M.; Ana, P.A. High power lasers and their interaction with biological tissues. In Lasers in Dentistry: Guide for Clinical Practice; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 11–18. [Google Scholar] [CrossRef]
- Gabrić, D.; Aumiler, D.; Vuletić, M.; Gjorgievska, E.; Blašković, M.; Mladenov, M.; Pavlić, V. Thermal Evaluation by Infrared Thermography Measurement of Osteotomies Performed with Er:YAG Laser, Piezosurgery and Surgical Drill—An Animal Study. Materials 2021, 14, 3051. [Google Scholar] [CrossRef] [PubMed]
- Qu, W.; Shang, J.; Liu, L.; Xu, D.; Du, P.; Liu, Z. Comparative study on the incision healing of the palatal mucosa by using Er:YAG laser or traditional scalpel in the SD rats. Lasers Med. Sci. 2018, 33, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Bali, S.J.; Hodge, C.; Lawless, M.; Roberts, T.V.; Sutton, G. Early Experience with the Femtosecond Laser for Cataract Surgery. Ophthalmology 2012, 119, 891–899. [Google Scholar] [CrossRef]
- Berk, T.A.; Schlenker, M.B.; Campos-Möller, X.; Pereira, A.M.; Ahmed, I.I.K. Visual and Refractive Outcomes in Manual versus Femtosecond Laser–Assisted Cataract Surgery: A Single-Center Retrospective Cohort Analysis of 1838 Eyes. Ophthalmology 2018, 125, 1172–1180. [Google Scholar] [CrossRef]
- Al-Bourgol, S.; Machinet, G.; Bakkali, A.; Faucon, M.; Gemini, L. Real-Time Monitoring of Thermal Phenomena during Femtosecond Ablation of Bone Tissue for Process Control. Bioengineering 2024, 11, 309. [Google Scholar] [CrossRef]
- An, R.; Khadar, G.W.; Wilk, E.I.; Emigh, B.; Haugen, H.K.; Wohl, G.R.; Dunlop, B.; Anvari, M.; Hayward, J.E.; Fang, Q. Ultrafast laser ablation and machining large-size structures on porcine bone. J. Biomed. Opt. 2013, 18, 070504. [Google Scholar] [CrossRef]
- Girard, B.; Yu, D.; Armstrong, M.; Wilson, B.; Clokie, C.; Miller, R.D. Effects of femtosecond laser irradiation on osseous tissues. Lasers Surg. Med. 2007, 39, 273–285. [Google Scholar] [CrossRef]
- McCaughey, R.G.; Sun, H.; Rothholtz, V.S.; Juhasz, T.; Wong, B.J.F. Femtosecond laser ablation of the stapes. J. Biomed. Opt. 2009, 14, 024040. [Google Scholar] [CrossRef]
- Su, E.; Sun, H.; Juhasz, T.; Wong, B.J.F. Preclinical investigations of articular cartilage ablation with femtosecond and pulsed infrared lasers as an alternative to microfracture surgery. J. Biomed. Opt. 2014, 19, 098001. [Google Scholar] [CrossRef]
- Lo, D.D.; Mackanos, M.A.; Chung, M.T.; Hyun, J.S.; Montoro, D.T.; Grova, M.; Liu, C.; Wang, J.; Palanker, D.; Connolly, A.J.; et al. Femtosecond plasma mediated laser ablation has advantages over mechanical osteotomy of cranial bone. Lasers Surg. Med. 2012, 44, 805–814. [Google Scholar] [CrossRef]
- Zhang, J.; Guan, K.; Zhang, Z.; Guan, Y. In vitro evaluation of ultrafast laser drilling large-size holes on sheepshank bone. Opt. Express 2020, 28, 25528–25544. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.; Zhang, L.; Cao, L.; Zheng, J.; Wang, J.; Han, W.; Zhang, H. Laser rapid drilling of bone tissue in minimizing thermal injury and debris towards orthopedic surgery. Mater. Des. 2022, 220, 110895. [Google Scholar] [CrossRef]
- Gemini, L.; Al-Bourgol, S.; Machinet, G.; Bakkali, A.; Faucon, M.; Kling, R. Ablation of Bone Tissue by Femtosecond Laser: A Path to High-Resolution Bone Surgery. Materials 2021, 14, 2429. [Google Scholar] [CrossRef]
- Kerse, C.; Kalaycıoğlu, H.; Elahi, P.; Çetin, B.; Kesim, D.K.; Akçaalan, Ö.; Yavaş, S.; Asik, M.D.; Öktem, B.; Hoogland, H.; et al. Ablation-cooled material removal with ultrafast bursts of pulses. Nature 2016, 537, 84–88. [Google Scholar] [CrossRef]
- Liang, S.; Zheng, J.; Yuan, F. Preliminary study on the osseointegration effects of contactless automated implant cavity preparation via femtosecond laser ablation. Biomed. Opt. Express 2021, 13, 82–92. [Google Scholar] [CrossRef]
- Zheng, J.; Zhang, X.; Zhang, Y.; Yuan, F. Osteoblast differentiation of bone marrow stromal cells by femtosecond laser bone ablation. Biomed. Opt. Express 2020, 11, 885–894. [Google Scholar] [CrossRef]
- Rico, M.; Jubera, M.; Blas, A.S.; Roso, L.; Lazkoz, A.; Arregui, J. Improvements on Characterization of the Threshold and Productivity in Femtosecond Laser Ablation of Bone. In Proceedings of the Conference on Lasers and Electro-Optics Europe & European Quantum Electronics Conference (CLEO/Europe-EQEC 2019), Munich, Germany, 23–27 June 2019; p. 1. [Google Scholar] [CrossRef]
- Emigh, B.; An, R.; Hsu, E.M.; Crawford, T.H.R.; Haugen, H.K.; Wohl, G.R.; Hayward, J.E.; Fang, Q. Porcine cortical bone ablation by ultrashort pulsed laser irradiation. J. Biomed. Opt. 2012, 17, 028001. [Google Scholar] [CrossRef]
- Cangueiro, L.T.; Vilar, R.; Botelho do Rego, A.M.; Muralha, V.S.F. Femtosecond laser ablation of bovine cortical bone. J. Biomed. Opt. 2012, 17, 125005. [Google Scholar] [CrossRef]
- Lim, Y.C.; Altman, K.J.; Farson, D.F.; Flores, K.M. Micropillar fabrication on bovine cortical bone by direct-write femtosecond laser ablation. J. Biomed. Opt. 2009, 14, 064021. [Google Scholar] [CrossRef]
- Liu, Y.; Niemz, M. Ablation of femural bone with femtosecond laser pulses—A feasibility study. Lasers Med. Sci. 2007, 22, 171–174. [Google Scholar] [CrossRef]
- Armstrong, W.B.; Neev, J.A.; Da Silva, L.B.; Rubenchik, A.M.; Stuart, B.C. Ultrashort pulse laser ossicular ablation and stapedotomy in cadaveric bone. Lasers Surg. Med. 2002, 30, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Cloutier, M.; Girard, B.; Peel, S.A.; Wilson, D.; Sándor, G.K.; Clokie, C.M.; Miller, D. Calvarial bone wound healing: A comparison between carbide and diamond drills, Er:YAG and Femtosecond lasers with or without BMP-7. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Girard, B.; Cloutier, M.; Wilson, D.; Clokie, C.; Miller, R.; Wilson, B. Microtomographic analysis of healing of femtosecond laser bone calvarial wounds compared to mechanical instruments in mice with and without application of BMP-7. Lasers Surg. Med. 2007, 39, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Yuan, F.; Zhang, Z.; Yan, L.; Li, X.; Shi, X. High-Precision Implant Cavity Fabrication Using Femtosecond Lasers. Photobiomodulation Photomed. Laser Surg. 2024, 42, 541–549. [Google Scholar] [CrossRef]
- Lyukshin, V.; Shatko, D.; Strelnikov, P. Methods and approaches to the surface roughness assessment. Mater. Today Proc. 2021, 38, 1441–1444. [Google Scholar] [CrossRef]
- Eriksson, A.R.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107. [Google Scholar] [CrossRef]
- Dubey, A.K.; Yadava, V. Optimization of kerf quality during pulsed laser cutting of aluminium alloy sheet. J. Mater. Process. Technol. 2008, 204, 412–418. [Google Scholar] [CrossRef]
- Banerjee, S.P.; Chen, Z.; Fedosejevs, R. Femtosecond laser plasma plume characteristics in the nanojoule ablation regime. J. Appl. Phys. 2013, 113, 183101. [Google Scholar] [CrossRef]
- Maggiano, I.S.; Maggiano, C.M.; Cooper, D.M. Osteon circularity and longitudinal morphology: Quantitative and qualitative three-dimensional perspectives on human Haversian systems. Micron 2021, 140, 102955. [Google Scholar] [CrossRef]
- Lin, L.; Huang, X.; Li, Z.; Zhang, G.; Yu, H.; Wan, Y.; Zhou, C.; Zhou, L. Freeze-drying platforms design for batch fabrication of Haversian system mimicking scaffolds with enhanced osteogenesis. Front. Bioeng. Biotechnol. 2022, 10, 1013528. [Google Scholar] [CrossRef]
- Feldmann, A.; Wandel, J.; Zysset, P. Reducing temperature elevation of robotic bone drilling. Med. Eng. Phys. 2016, 38, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, A.C.; Tai, B.L.; Belmont, B.; Irwin, T.A.; Shih, A.; Holmes, J.R. Heat accumulation during sequential cortical bone drilling. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2016, 34, 463–470. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Bone Type | Wavelength | Repetitive Rate | Pulse Width | Scan Rate | Energy Density | Ablation Threshold (Pulse) | Ablation Rate |
|---|---|---|---|---|---|---|---|---|
| In vitro studies | ||||||||
| Liang et al., 2022 [36] | Rabbit femur | 1030 nm | 200 kHz | 500 fs | 4000 mm/s | NA | NA | 36 μm/ 5 scans |
| Gemini et al., 2021 [34] | Porcine femur | 515 nm | 250 kHz | 350 fs | 4000 mm/s | NA | NA | 0.66 mm3/s |
| Zhang et al., 2020 [32] | Sheepshank | 1030 nm | 200 kHz | 230 fs | 2000 mm/s | 14.15 J/cm2 | NA | 0.99 mm3/s |
| Rico et al., 2019 [38] | NA | 1030 nm | 60 kHz | 240 fs | 100 mm/s | 6.1 J/cm2 | NA | 0.053 mm3/s |
| Su et al., 2014 [30] | Bovine articular cartilage | 1700 nm | 5 kHz | NA | NA | NA | NA | 0.8 × 10−4 mm3/s |
| Emigh et al., 2012 [39] | Porcine scapulae | 800 nm | 1 kHz | 170 fs | NA | NA | 1.75 J/cm2 (1000) | NA |
| Cangueiro et al., 2012 [40] | Bovine femur | 1030 nm | 10 Hz | 500 fs | NA | NA | 0.79 J/cm2 (1) | NA |
| Lim et al., 2009 [41] | Bovine femur | 775 nm | 3 kHz | 150 fs | NA | NA | 2.70 J/cm2 (1) | NA |
| McCaughey et al., 2009 [29] | Otic capsule | 1053 nm | 10 kHz | 700 fs | NA | NA | 8.5 J/cm2 (1) | NA |
| Liu et al., 2007 [42] | Porcine femur | 1030 nm | 10 kHz | Below 900 fs | NA | NA | NA | 0.02 mm3/s |
| Girard et al., 2007 [28] | Porcine mandible | 775 nm | 1 kHz | 200 fs | NA | NA | 0.69 J/cm2 (1000) | NA |
| Wieger et al., 2007 [18] | Bovine spongiosa, compacta, and cartilage | 1040 nm | 1 kHz | 330 fs | NA | NA | 0.54–0.82 J/cm2 (1) | NA |
| Armstrong et al., 2002 [43] | Human incus and stapes | 1053 nm | 10 Hz | 350 fs | NA | 2.0 J/cm2 | NA | 1.26 mm/pulse |
| In vivo studies | ||||||||
| Lo et al., 2012 [31] | Mouse calvaria | 800 nm | 1 kHz | 150 fs | 4 mm/s | NA | NA | NA |
| Cloutier et al., 2010 [44] | Mouse calcaria | 775 nm | 1 kHz | <200 fs | NA | 8.0 J/cm2 | NA | NA |
| Girard et al., 2007 [45] | Mouse calcaria | 775 nm | 1 kHz | <200 fs | 200 mm/s | NA | NA | NA |
| Laser Set | Energy Density (J/cm2) | Maximum Temperature (°C) | Maximum Temperature Increase (°C) |
|---|---|---|---|
| Set 1 | 0.58 | 26.4 ± 0.2 | 5.8 ± 0.2 |
| Set 2 | 0.81 | 33.1 ± 0.1 | 12.2 ± 0.1 |
| Set 3 | 1.05 | 42.7 ± 0.1 | 22.4 ± 0.1 |
| Set 4 | 1.28 | 53.2 ± 0.3 | 32.1 ± 0.3 |
| Laser Set | Elemental Mass Percentage (%) | ||
|---|---|---|---|
| O | Ca | P | |
| Set 1 | 40.46 ± 1.84 | 30.58 ± 4.51 | 6.57 ± 1.24 |
| Set 2 | 29.51 ± 2.09 | 29.64 ± 0.37 | 8.33 ± 2.20 |
| Set 3 | 34.29 ± 7.28 | 33.29 ± 6.50 | 10.42 ± 3.67 |
| Set 4 | 37.08 ± 7.09 | 30.25 ± 1.27 | 9.39 ± 2.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Liang, S.; Zhou, Y.; Yuan, F.; Ye, H. Parameter Optimization, Morphological and Histological Characteristics of Accurate Bone Ablation by Femtosecond Laser: An In Vitro Study. Bioengineering 2025, 12, 217. https://doi.org/10.3390/bioengineering12030217
Wang Y, Liang S, Zhou Y, Yuan F, Ye H. Parameter Optimization, Morphological and Histological Characteristics of Accurate Bone Ablation by Femtosecond Laser: An In Vitro Study. Bioengineering. 2025; 12(3):217. https://doi.org/10.3390/bioengineering12030217
Chicago/Turabian StyleWang, Yiyang, Shanshan Liang, Yongsheng Zhou, Fusong Yuan, and Hongqiang Ye. 2025. "Parameter Optimization, Morphological and Histological Characteristics of Accurate Bone Ablation by Femtosecond Laser: An In Vitro Study" Bioengineering 12, no. 3: 217. https://doi.org/10.3390/bioengineering12030217
APA StyleWang, Y., Liang, S., Zhou, Y., Yuan, F., & Ye, H. (2025). Parameter Optimization, Morphological and Histological Characteristics of Accurate Bone Ablation by Femtosecond Laser: An In Vitro Study. Bioengineering, 12(3), 217. https://doi.org/10.3390/bioengineering12030217